Damage Control Surgery: What’s New? Muhammad S Niam Divisi Bedah Digestif, Lab/SMF Bedah RSU Dr Saiful Anwar/FK Universitas Brawijaya Malang Acute Care Surgery: February 23-24 th , 2018 Crown Plaza Hotel, Bandung
Transcript
Damage Control Surgery: What’s New?Muhammad S Niam
Divisi Bedah Digestif, Lab/SMF Bedah
RSU Dr Saiful Anwar/FK Universitas Brawijaya Malang
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
New AdditionDamage control surgery in the era of damage controlresuscitationC. M. Lamb, P. MacGoey, A. P. Navarro and A. J. Brooks*East Midlands Major Trauma Centre, Queen’s Medical Centre Campus, Nottingham University Hospitals, Derby Road, Nottingham NG5 2UH, UK
† Damage control strategies prioritizephysiological and biochemicalstabilization over the full anatomicalrepair of all injuries.
† Damage control strategies are useful fora subset of trauma patients and are notappropriate in all cases.
† Selection criteria for damage controlmanagement include the mechanismof injuryand the degree of physiologicalderangement.
Damage control surgery (DCS) is aconcept of abbreviated laparotomy,designed toprioritize short-term physiological recovery over anatomical reconstruction in theseriously injured and compromised patient. Over the last 10 yr, a new addition tothe damage control paradigm has emerged, referred to as damage controlresuscitation (DCR). This focuses on initial hypotensive resuscitation and earlyuse of blood products to prevent the lethal triad of acidosis, coagulopathy, andhypothermia. This review aims to present the evidence behind DCR and itscurrent application, and also to present a strategy of overall damage control toinclude DCR and DCS in conjunction. The use of DCR and DCS have beenassociated with improved outcomes for the severely injured and wider adoptionof these principles where appropriate may allow this trend of improved survivalto continue. In particular, DCR may allow borderline patients, who wouldpreviously have required DCS, to undergo early definitive surgery as theirphysiological derangement is corrected earlier.
Keywords: resuscitation; surgery, abdominal; trauma; wounds and injuries
Over the last two decades, public health measures and betterpre-hospital care have led to an increasing number of seriouslyinjured patients surviving their initial accident and arriving inhospital.1 These injured patients often have injuries to multiplebody cavities, massive haemorrhage, and near exhaustedphysiological reserve. Management of these cases haschanged significantly in the last decade with the emergenceof a new paradigm termed damage control.
A combination of acidosis, hypothermia, and coagulopathy(the so-called lethal triad) may preclude definitive surgicalrepair of all injuries in one sitting and it is in this subset ofpatients that ‘damage control surgery’ (DCS) is advocated.DCS is a treatment strategy of temporization; prioritizing physio-logical recovery over anatomical repair. Its use is associatedwith dramatically increased survival of the most seriouslyinjured patients.2 Damage control resuscitation (DCR) is a newerdevelopment within the damage control paradigm, and des-cribes novel resuscitation strategies aimed to limit the physio-logical derangement of trauma patients. This review will discussthe principles and application of DCS in the current era of DCR.
Damage controlStone and colleagues were the first to describe a technique of‘truncated laparotomy’ for patients with clinically evident co-agulopathy and retrospectively reviewed its efficacy in 1983.3
A decade later, Rotondo and colleagues popularized theterm ‘damage control laparotomy’, retrospectively reviewingthe management of patients undergoing laparotomy for
exsanguinating penetrating injuries [requiring urgent transfu-sion of .10 units of packed red blood cells (PRBC)]. They iden-tified a subset of maximally injured patients (major vascularinjury with two or more visceral injuries) in which survival wasmarkedly improved in the DCS group.2 DCS limits the goals ofthe initial operation to control of haemorrhage and limitationof contamination rather than definitive repair of all injuries; pri-oritizing physiology over anatomy.
In modern trauma practice, it is inconceivable that DCSshould be practiced separately from DCR; the two strategiesare integral to each other and DCS should be the endpoint ofDCR with surgical control of haemorrhage. DCS was originallydescribed by Rotondo and colleagues in 1993 as a three-phasetechnique. This was later modified by Johnson and Schwab4 toinclude a fourth, pre-theatre phase:
† Part zero (DC 0) emphasizes injury pattern recognition forpotential damage control beneficiaries and manifests intruncated scene times for the emergency services andabbreviated emergency department DCR by the traumateam. Rapid-sequence induction (RSI) of anaesthesiaand intubation, early rewarming, and expedient trans-port to the operating theatre are the key elements.
† Part one (DC I) occurs once the patient has arrived intheatre and consists of immediate exploratory laparot-omy with rapid control of bleeding and contamination,abdominal packing, and temporary wound closure.
† Part two (DC II) is the intensive care unit (ICU) resuscita-tive phase where physiological and biochemical
& The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
British Journal of Anaesthesia 113 (2): 242–9 (2014)doi:10.1093/bja/aeu233
Downloaded from https://academic.oup.com/bja/article-abstract/113/2/242/1746165by gueston 04 February 2018
Damage control surgery in the era of damage controlresuscitationC. M. Lamb, P. MacGoey, A. P. Navarro and A. J. Brooks*East Midlands Major Trauma Centre, Queen’s Medical Centre Campus, Nottingham University Hospitals, Derby Road, Nottingham NG5 2UH, UK
† Damage control strategies prioritizephysiological and biochemicalstabilization over the full anatomicalrepair of all injuries.
† Damage control strategies are useful fora subset of trauma patients and are notappropriate in all cases.
† Selection criteria for damage controlmanagement include the mechanismof injuryand the degree of physiologicalderangement.
Damage control surgery (DCS) is aconcept of abbreviated laparotomy,designed toprioritize short-term physiological recovery over anatomical reconstruction in theseriously injured and compromised patient. Over the last 10 yr, a new addition tothe damage control paradigm has emerged, referred to as damage controlresuscitation (DCR). This focuses on initial hypotensive resuscitation and earlyuse of blood products to prevent the lethal triad of acidosis, coagulopathy, andhypothermia. This review aims to present the evidence behind DCR and itscurrent application, and also to present a strategy of overall damage control toinclude DCR and DCS in conjunction. The use of DCR and DCS have beenassociated with improved outcomes for the severely injured and wider adoptionof these principles where appropriate may allow this trend of improved survivalto continue. In particular, DCR may allow borderline patients, who wouldpreviously have required DCS, to undergo early definitive surgery as theirphysiological derangement is corrected earlier.
Keywords: resuscitation; surgery, abdominal; trauma; wounds and injuries
Over the last two decades, public health measures and betterpre-hospital care have led to an increasing number of seriouslyinjured patients surviving their initial accident and arriving inhospital.1 These injured patients often have injuries to multiplebody cavities, massive haemorrhage, and near exhaustedphysiological reserve. Management of these cases haschanged significantly in the last decade with the emergenceof a new paradigm termed damage control.
A combination of acidosis, hypothermia, and coagulopathy(the so-called lethal triad) may preclude definitive surgicalrepair of all injuries in one sitting and it is in this subset ofpatients that ‘damage control surgery’ (DCS) is advocated.DCS is a treatment strategy of temporization; prioritizing physio-logical recovery over anatomical repair. Its use is associatedwith dramatically increased survival of the most seriouslyinjured patients.2 Damage control resuscitation (DCR) is a newerdevelopment within the damage control paradigm, and des-cribes novel resuscitation strategies aimed to limit the physio-logical derangement of trauma patients. This review will discussthe principles and application of DCS in the current era of DCR.
Damage controlStone and colleagues were the first to describe a technique of‘truncated laparotomy’ for patients with clinically evident co-agulopathy and retrospectively reviewed its efficacy in 1983.3
A decade later, Rotondo and colleagues popularized theterm ‘damage control laparotomy’, retrospectively reviewingthe management of patients undergoing laparotomy for
exsanguinating penetrating injuries [requiring urgent transfu-sion of .10 units of packed red blood cells (PRBC)]. They iden-tified a subset of maximally injured patients (major vascularinjury with two or more visceral injuries) in which survival wasmarkedly improved in the DCS group.2 DCS limits the goals ofthe initial operation to control of haemorrhage and limitationof contamination rather than definitive repair of all injuries; pri-oritizing physiology over anatomy.
In modern trauma practice, it is inconceivable that DCSshould be practiced separately from DCR; the two strategiesare integral to each other and DCS should be the endpoint ofDCR with surgical control of haemorrhage. DCS was originallydescribed by Rotondo and colleagues in 1993 as a three-phasetechnique. This was later modified by Johnson and Schwab4 toinclude a fourth, pre-theatre phase:
† Part zero (DC 0) emphasizes injury pattern recognition forpotential damage control beneficiaries and manifests intruncated scene times for the emergency services andabbreviated emergency department DCR by the traumateam. Rapid-sequence induction (RSI) of anaesthesiaand intubation, early rewarming, and expedient trans-port to the operating theatre are the key elements.
† Part one (DC I) occurs once the patient has arrived intheatre and consists of immediate exploratory laparot-omy with rapid control of bleeding and contamination,abdominal packing, and temporary wound closure.
† Part two (DC II) is the intensive care unit (ICU) resuscita-tive phase where physiological and biochemical
& The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved.For Permissions, please email: [email protected]
British Journal of Anaesthesia 113 (2): 242–9 (2014)doi:10.1093/bja/aeu233
Downloaded from https://academic.oup.com/bja/article-abstract/113/2/242/1746165by gueston 04 February 2018
British Journal of Anaesthesia 113 (2): 242–9 (2014) doi:10.1093/bja/aeu233
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Key Points• Prioritize physiological and biochemical
stabilisation • Useful for a subset of trauma patients, not
appropriate in all cases • Selection criteria include the mechanism of injury
and the degree of physiological derangement.
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Background• Over the last 2 decades PH measures and better pre-
hospital care ☛ number of seriously injured patients surviving and arriving in hospital
• These injured patients of multiple body cavities, massive haemorrhage, and near exhausted physiological reserve
• Management of these cases has changed significantly in the last decade ☛ a new paradigm termed damage control
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• Lethal triad (acidosis, hypothermia, and coagulopathy) preclude definitive surgical repair ☛‘damage control surgery’ (DCS) recommended
• DCS prioritizing physiological recovery over anatomical repair
• Associated with dramatically increased survival of the most seriously injured patients
• Damage control resuscitation (DCR) is a newer development within the damage control paradigm ☛ novel resuscitation strategies
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Damage Control• Stone et.al were the first to describe a technique of ‘truncated
laparotomy’ for patients with coagulopathy and retrospectively reviewed in 1983
• A decade later, Rotondo et.al popularized the term ‘damage control laparotomy’, retrospectively reviewing the management of patients undergoing laparotomy for exsanguinating penetrating injuries requiring urgent transfusion of .10 units of PRBC ☛ major vascular injury with two or more visceral injuries which survival was markedly improved in the DCS group
• The goals of the initial operation are control of haemorrhage and contamination
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Modified Rotondo’s 3-phase technique to 4 by Johnson & Schwab • DC 0: Injury pattern recognition for potential DC by the
trauma team ☛ Rapid induction and intubation, early rewarming, and transport to OT
• DC I: In OT ☛ immediate exploratory laparotomy for control of bleeding and contamination, abdominal packing, and temporary wound closure
• DC II: In ICU ☛ physiological and biochemical stabilization, identify all injuries
• DC III: Physiology normalized ☛ definitive repair of all injuries
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Indication for DC• Physiological derangement • Bleeding with massive transfusion (>10 units PRBC) • Severe metabolic acidosis (<pH,7.30) • Hypothermia (temperature <35o C) • Operative time >90 min • Coagulopathy (laboratory results or ‘non-surgical’
bleeding • Lactate >5 mmol litre
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Damage Control Steps
DC 0:
Injury pattern recognition for potential DC by the trauma team
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Damage Control Resuscitation• Excessive fluid resuscitation vs delayed fluid resuscitation or
permissive hypotension ☛ endogenous ‘acute traumatic coagulopathy’ with poor outcomes
• Resuscitation strategies ☛ permissive hypotension and early treatment of anticipated coagulopathy with blood products
• The military’s experience of management of major haemorrhage during conflicts in Afghanistan and Iraq
• Holcomb et.al 2007: Proactive early treatment strategy that addresses the lethal triad on admission to a combat hospital’
• Hodgetts et.al: Systematic approach to major trauma combining the ABC paradigm ‘minimize blood loss, maximize tissue oxygenation, and optimize outcome’.
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
The main elements of DCR are: • ABC resuscitation • Permissive hypotension • Limitation of crystalloid with early use of blood and
blood products • Early use of TXA • DCS (DCI)
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• Early use of blood and blood products with attention to the ratio of blood components used are essential ☛ FFP > PRBC
• Protocolized administration of blood products to reduce mortality and morbidity in major trauma patients requiring massive transfusion
• Available an initial pack of non-cross-matched blood for immediate use in the unstable patient
• Once bloods for cross-match have been taken, fully matched components designed to prevent clotting factor depletion and coagulopathy during early massive transfusion
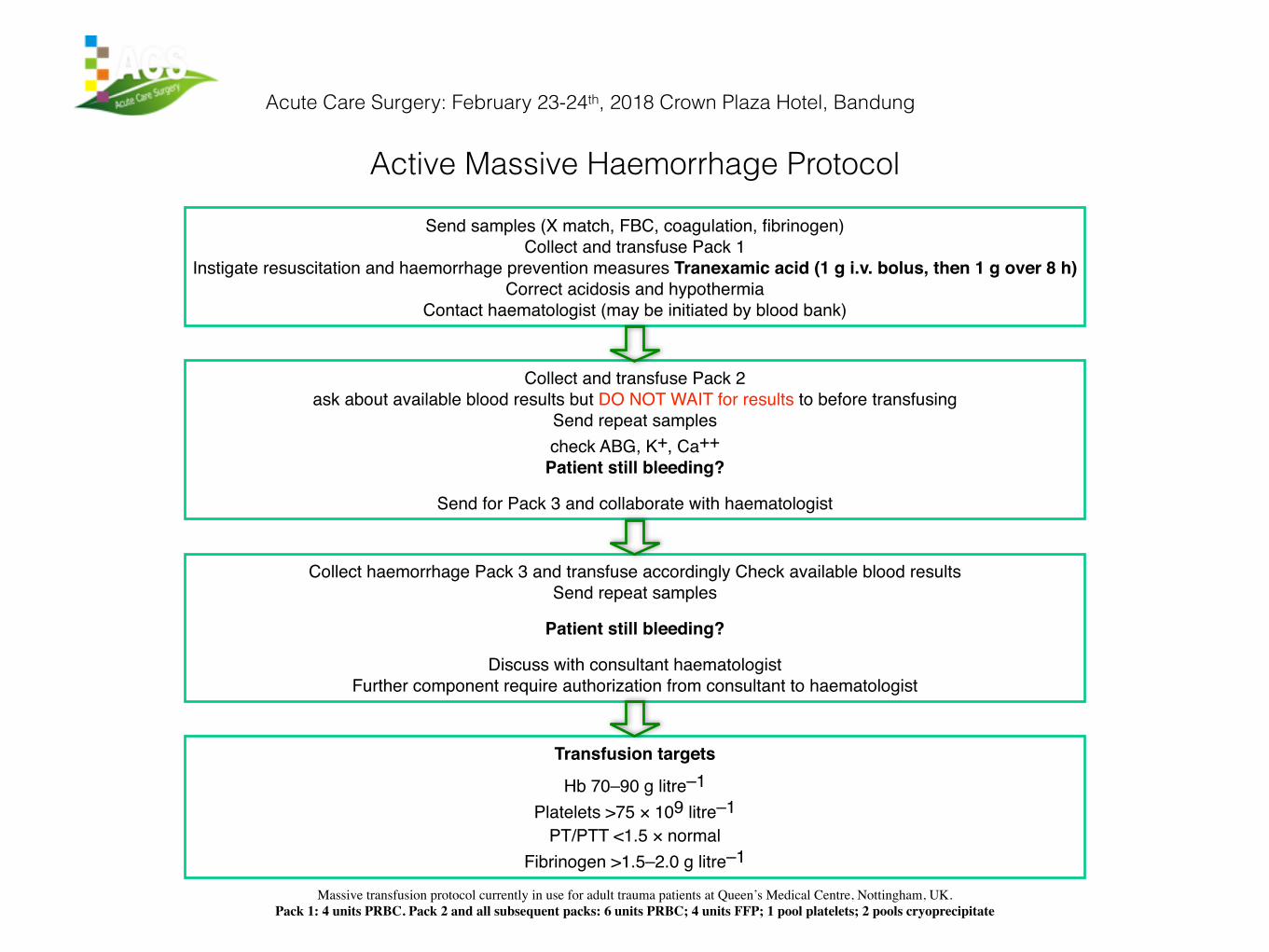
Instigate resuscitation and haemorrhage prevention measures Tranexamic acid (1 g i.v. bolus, then 1 g over 8 h) Correct acidosis and hypothermia
Contact haematologist (may be initiated by blood bank)
Collect and transfuse Pack 2 ask about available blood results but DO NOT WAIT for results to before transfusing
Send repeat samplescheck ABG, K+, Ca++
Patient still bleeding?
Send for Pack 3 and collaborate with haematologist
Collect haemorrhage Pack 3 and transfuse accordingly Check available blood resultsSend repeat samples
Patient still bleeding?
Discuss with consultant haematologist Further component require authorization from consultant to haematologist
Transfusion targets
Hb 70–90 g litre–1 Platelets >75 × 109 litre–1
PT/PTT <1.5 × normal Fibrinogen >1.5–2.0 g litre–1
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Massive transfusion protocol currently in use for adult trauma patients at Queen’s Medical Centre, Nottingham, UK. Pack 1: 4 units PRBC. Pack 2 and all subsequent packs: 6 units PRBC; 4 units FFP; 1 pool platelets; 2 pools cryoprecipitate
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Damage Control Steps
DC I:
In the Operating Theater
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• The primary objectives: haemorrhage control limitation of contamination temporary abdominal wall closure.
• To restore physiology • DCR should be on-going throughout DC 0 and DC I
and is indeed an integral part of the damage control strategy.
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
standard laparotomy set, vascular, and chest instruments (including a sternal saw)
• Laparotomy pads for the initial packing • A trolley stocked with damage control equipment
MaxxLyfe Hospital & Trauma Center
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Preparation• The patient position on the table • No leads or tubing should be
present on the anterior or lateral chest wall for a median or resuscitative left thoracotomy, or bilateral tube thoracostomy
• A urinary catheter and nasogastric/orogastric tube
• CVC line insertion should not delay surgery in unstable patient
DONNERSTAG, 30. MÄRZ 2017
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Incision• The best incision for abdominal exploration is the
vertical midline extending from the xiphoid process to the pubic symphysis
• In a suspected severe pelvic fracture just below the umbilicus initially, allowing for continued tamponade of a potential large pelvic haematoma
• The incision can be easily extended superiorly, laterally, or both to give chest exposure, and laterally in subcostal regions to give better access to the upper abdomen
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Haemorrhage Control• The first step is haemorrhage control • Large clots should be removed • Provide space for the packing of all four quadrants • The cell salvage suction to maximise autologous blood capture
and return • Assessing the degree and location of the most significant
injuries. • Adequate packing of haemorrhage control for most venous or
solid organ bleeding • A significant arterial source ☛ give manual occlusion of the
aorta at the diaphragmatic hiatus to augment cerebral and myocardial perfusion
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Haemorrhage Control• For prolonged occlusion a vascular clamp can be
placed on the supra-coeliac aorta after minimal dissection in the abdomen or the descending thoracic aorta if a thoracotomy is performed.
• Time should be noted to prevent severe visceral ischaemia
• It is desirable to move the clamp down the aorta sequentially as access and haemorrhage control is gained distally.
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Haemorrhage Control• Once haemorrhage has been stopped, packs are
removed in sequentially • For major vascular injuries ☛ vessel ligation or
placement of temporary intravascular shunts to improve arterial flow
and normalize haemodynamics • The exact monitoring methods: trans-oesophageal
Doppler, transthoracic echocardiography, lithium dilution, pulmonary artery catheters, etc to measure or estimate the cardiac output and its response to fluid challenges
Physiological and Biochemical Restoration
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• Abramson et.al., serum lactate clearance correlates well with patient survival and ability to clear lactate to normal levels within 24 h essential to ensure patient survival
• Immediate and aggressive core rewarming ☛ improves perfusion and reverse coagulopathy
• Gentilello showed that failure to correct a patient’s hypothermia result of inadequate resuscitation or irreversible shock.
• Administration of FFP, which is rich in Factors V and VIII until laboratory of coagulation are normal
• Platelet also corrected, fibrinogen levels corrected by cryoprecipitate • Bedside testing of the coagulation system (e.g. with rotational
thromboelastometry) and protocolized massive transfusion policies
Correct Hypothermia and Coagulopathy
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• Tertiary survey complete physical examination include relevant imaging studies
• CT scan to detect occult injuries if stable enough • In blunt trauma, completion of the spinal survey is imperative • Peripheral wounds are addressed and vascular integrity of all
injured limbs is assessed frequently • Recruitment of consultants for all definitive repairs • The exact timing of reconstruction and abdominal closure (DC III)
is dependent on the individual patient (12-36 hrs) • Patient does not normalize haemodynamically, lactic acid or base
deficit fail to improve ☛ back to the OT earlier for re-exploration
Tertiary Survey
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• The first is the group: • ongoing transfusion requirements or persistent acidosis
despite normalized clotting and core temperature • ongoing surgical bleeding or a missed visceral injury • very high mortality rate.
• The second group: • IAH (prolonged IAP >12 mm Hg) ☛ organ dysfunction • ACS (sustained or repeated IAP >20 mm Hg) ☛ 1/>
organ failure • Normal IAP 2–7 mm Hg
Unplanned Re-operation
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• Clinical appearance: • tensely distended abdomen • elevated peak airway pressure and impaired ventilation with hypoxia
and hypercarbia • decreased urine output • increased systemic vascular resistance • and decreased cardiac output.
• 6% of patients with severe abdominal and/or pelvic trauma • Incidence reduced by the use of DCR strategies • Management of the open abdomen with vacuum pack closure does not
prevent the development of ACS • Best treatment of ACS is prevention
Abdominal Compartment Syndrome
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• Medical and anaesthetic measures to reduce intraabdominal volume • colloid rather than crystalloid resuscitation to decrease gut oedema • nasogastric drainage • bowel cleansing
• Increase abdominal wall compliance (optimal analgesia and sedation including complete neuromuscular block if necessary)
• Continuous haemofiltration ☛ reduce circulating cytokine load in patients with significant SIRS, and reduce IAH and mortality
• Opening the patient’s abdomen to relieve the pressure • Ongoing blood loss best performed in the OT when transportable • Alternative, open the abdomen in the ICU under sterile conditions • Adequate decompression by incising the external drape of the vacuum pack
Abdominal Compartment Syndrome
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
Damage Control Steps
DC III:
Definitive care
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• Impact on achieving traditional measures of ‘successful outcomes’ (e.g. LOS, SSI, anastomotic leaks, etc.)
• Adequate resuscitation and physiological optimization has been achieved: • normothermic • normal coagulation studies • normal pH and lactate
• Early progression to DC III may be: • to salvage an ischaemic limb because of shunt occlusion • Interrupted bowel at several sites, resulting in a closed-
loop obstruction.
Timing is Critical
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• All packs are irrigated copiously and removed carefully to avoid clot disruption or further visceral damage
• If bleeding is encountered on pack removal and local haemostatic measures fail ☛ immediate repacking is the safest course
• Alternatively, the packs may be wrapped in a non-adherent material such as IobanTM during initial exploration
• Complete re-examination of the abdominal contents • Control additional sites of bleeding, vascular repairs
performed, and intestinal continuity restored
Operative Game Plan
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
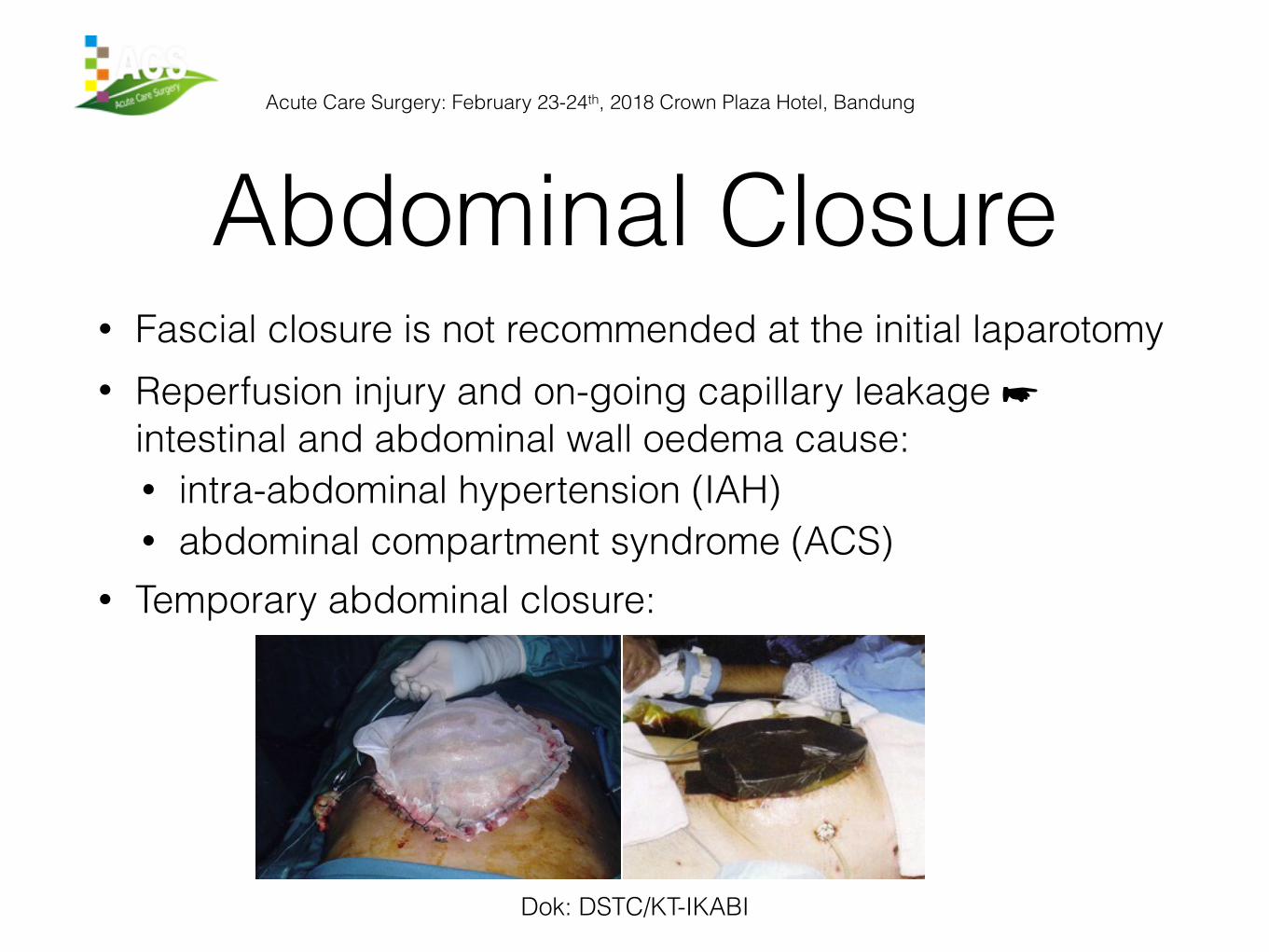
• Abdominal closure without tension is the challenging • Gentle adduction allows the fascial edges to approximate ☛ a
standard fascial closure • Persistent oedema within retroperitoneum, bowel & abdominal wall,
peak airway pressure >10 cm H2O ☛ left opened and TACD replaced • Aggressive diuresis should be considered in ICU • Frequent and regular abdominal washouts • Re-inspection, and careful replacement of TACD to prevent fistula
formation • Majority of DC open abdomens can be closed primarily within 1 week • Fascial closure not achieved after 7 days, leave patient with a large
ventral hernia that may repaired at a later date.
Abdominal Closure
Acute Care Surgery: February 23-24th, 2018 Crown Plaza Hotel, Bandung
• DCS and DCR associated with improvements in survival for the severely injured trauma patient
• Abbreviated operation to control of haemorrhage and enteral contamination
• Aggressive resuscitation allows one to improve the patients’ physiology
• DCR used during the initial phases result in improved mortality rates and reduced incidence of complications in major trauma patients
• Better physiological condition after DCR reduce the requirement for DCS