1/12/2017 1 Stephen Humphrey, MD Assistant Professor Pediatric Dermatology Feb. 2 nd , 2017 Thursday, January 12, 2017 1 I have no financial relationships to disclose Thursday, January 12, 2017 2 Objectives Describe and discuss clinical presentations of several dangerous dermatologic rashes Understand clinical clues that can aid in diagnosis and treatment Explain current work‐up and treatments for several eruptions Expand differential diagnosis of dangerous rashes based on clinical exams Thursday, January 12, 2017 3 Eruptions Stevens‐Johnson Syndrome (SJS)/Toxic Epidermal Necrolysis (TEN) Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) Meningococcemia Eczema Herpeticum Staph Scalded Skin Syndrome Serum Sickness‐Like Reaction *Not covered: Kawasaki disease, vasculitides Thursday, January 12, 2017 4
Transcript
1/12/2017
1
Stephen Humphrey, MD
Assistant Professor
Pediatric Dermatology
Feb. 2nd, 2017
Thursday, January 12, 2017 1
I have no financial relationships to disclose
Thursday, January 12, 2017 2
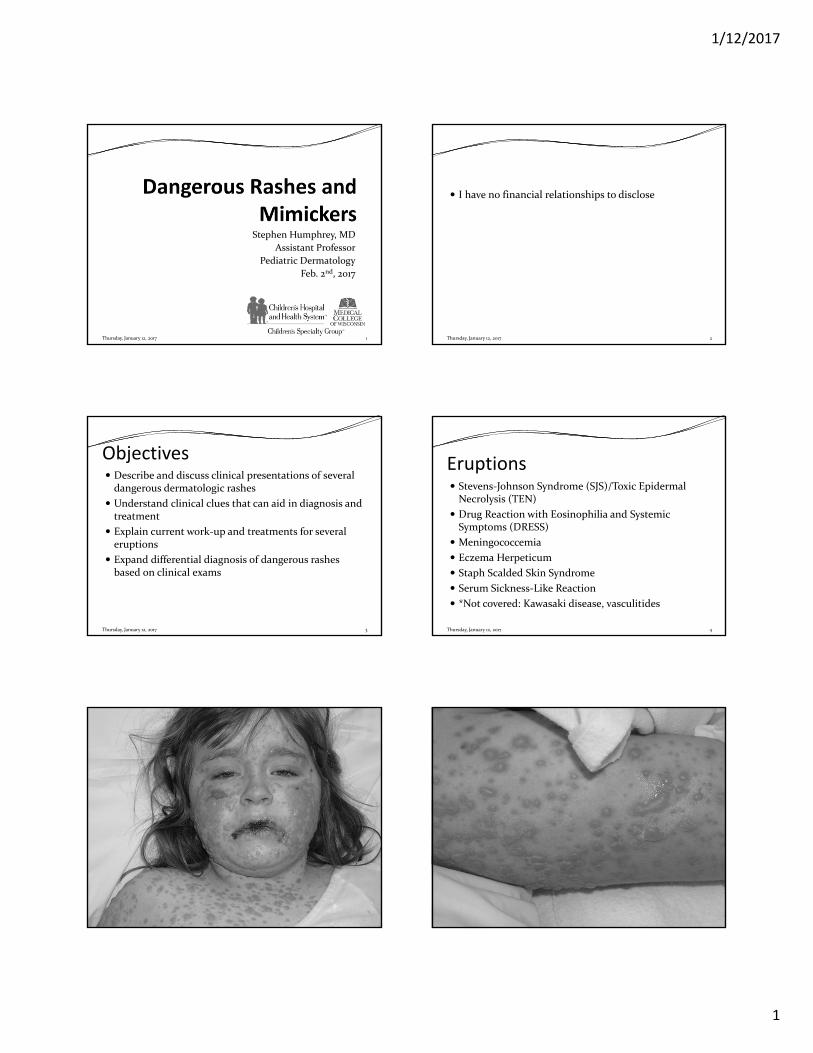
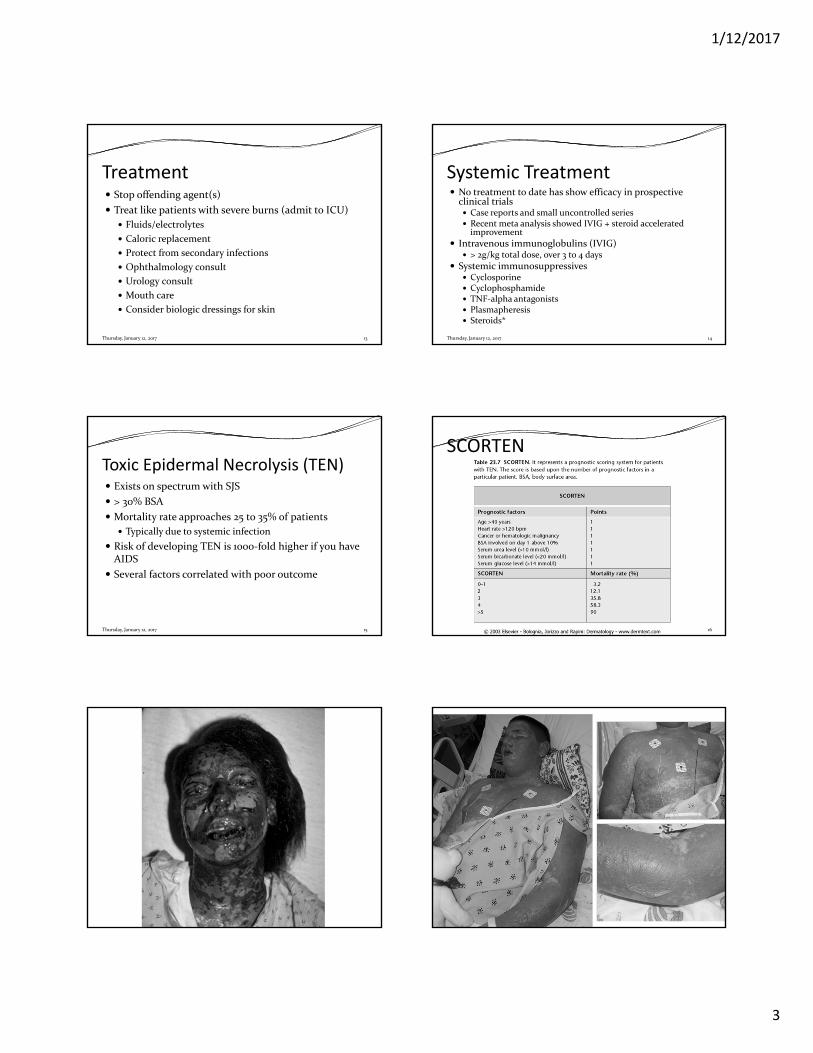
Objectives Describe and discuss clinical presentations of several dangerous dermatologic rashes
Understand clinical clues that can aid in diagnosis and treatment
Explain current work‐up and treatments for several eruptions
Expand differential diagnosis of dangerous rashes based on clinical exams
Treat like patients with severe burns (admit to ICU)
Fluids/electrolytes
Caloric replacement
Protect from secondary infections
Ophthalmology consult
Urology consult
Mouth care
Consider biologic dressings for skin
Thursday, January 12, 2017 13
Systemic Treatment No treatment to date has show efficacy in prospective clinical trials Case reports and small uncontrolled series Recent meta analysis showed IVIG + steroid accelerated improvement
Intravenous immunoglobulins (IVIG) > 2g/kg total dose, over 3 to 4 days
Bibliography Bolognia, J., Jorizzo, J. L., & Schaffer, J. V. (2012). Dermatology. Philadelphia: Elsevier
Saunders. Paller, A., Mancini, A. J., & Hurwitz, S. (2011). Hurwitz clinical pediatric dermatology: A
textbook of skin disorders of childhood and adolescence. New York: Elsevier/Saunders. Mishra AK, Yadav P , Mishra A. A Systemic Review on Staphylococcal Scalded Skin
Syndrome (SSSS): A Rare and Critical Disease of Neonates. Open Microbiol J 2016;10:150‐9.
Olson D, Watkins LK, Demirjian A, Lin X, Robinson CC, Pretty K et al. Outbreak of Mycoplasma pneumoniae‐Associated Stevens‐Johnson Syndrome. Pediatrics 2015;136:e386‐94.
Roujeau JC , Bastuji‐Garin S. Systematic review of treatments for Stevens‐Johnson syndrome and toxic epidermal necrolysis using the SCORTEN score as a tool for evaluating mortality. Ther Adv Drug Saf 2011;2:87‐94.
Stephens DS, Greenwood B , Brandtzaeg P. Epidemic meningitis, meningococcaemia, and Neisseria meningitidis. Lancet 2007;369:2196‐210.
Varghese C, Sharain K, Skalski J , Ramar K. Mycoplasma pneumonia‐associated mucositis. BMJ Case Rep 2014;2014.
Ye LP, Zhang C , Zhu QX. The Effect of Intravenous Immunoglobulin Combined with Corticosteroid on the Progression of Stevens‐Johnson Syndrome and Toxic Epidermal Necrolysis: A Meta‐Analysis. PLoS One 2016;11:e0167120.