Decision to accredit Arrunga The Aged Care Standards and Accreditation Agency Ltd has decided to accredit Arrunga in accordance with the Accreditation Grant Principles 1999. The Agency has decided that the period of accreditation of Arrunga is three years until 21 January 2013. The Agency has found the home complies with 44 of the 44 expected outcomes of the Accreditation Standards. This is shown in the ‘Agency findings’ column appended to the following executive summary of the assessment team’s site audit report. The Agency is satisfied the home will undertake continuous improvement measured against the Accreditation Standards. The Agency will undertake support contacts to monitor progress with improvements and compliance with the Accreditation Standards. Information considered in making an accreditation decision The Agency has taken into account the following: • the desk audit report and site audit report received from the assessment team; and • information (if any) received from the Secretary of the Department of Health and Ageing; and • other information (if any) received from the approved provider including actions taken since the audit; and • whether the decision-maker is satisfied that the residential care home will undertake continuous improvement measured against the Accreditation Standards, if it is accredited.
Transcript
Decision to accredit
Arrunga
The Aged Care Standards and Accreditation Agency Ltd has decided to accredit Arrunga in accordance with the Accreditation Grant Principles 1999. The Agency has decided that the period of accreditation of Arrunga is three years until 21 January 2013. The Agency has found the home complies with 44 of the 44 expected outcomes of the Accreditation Standards. This is shown in the ‘Agency findings’ column appended to the following executive summary of the assessment team’s site audit report. The Agency is satisfied the home will undertake continuous improvement measured against the Accreditation Standards. The Agency will undertake support contacts to monitor progress with improvements and compliance with the Accreditation Standards. Information considered in making an accreditation decision The Agency has taken into account the following: • the desk audit report and site audit report received from the assessment team; and • information (if any) received from the Secretary of the Department of Health and Ageing;
and • other information (if any) received from the approved provider including actions taken
since the audit; and • whether the decision-maker is satisfied that the residential care home will undertake
continuous improvement measured against the Accreditation Standards, if it is accredited.
Home name: Arrunga Date/s of audit: 27 October 2009 to 28 October 2009 RACS ID: 0838 AS_RP_00851 v2.5
2
Home and approved provider details
Details of the home Home’s name: Arrunga
RACS ID: 0838
Number of beds: 96 Number of high care residents: 29
Special needs group catered for: • Dementia specific unit
Street/PO Box: 334 Kissing Point Road
City: Ermington State: NSW Postcode: 2115
Phone: 02 8878 6456 Facsimile: [Home Fax]
Email address:
Approved provider Approved provider: The Uniting Church in Australia Property Trust (NSW)
Assessment team Team leader: Margaret McCartney
Team member/s: Jill Bicknell
Date/s of audit: 27 October 2009 to 28 October 2009
Home name: Arrunga Date/s of audit: 27 October 2009 to 28 October 2009 RACS ID: 0838 AS_RP_00851 v2.5
3
Executive summary of assessment team’s report Accreditation decision
Standard 1: Management systems, staffing and organisational development
Expected outcome Assessment team recommendations
Agency findings
1.1 Continuous improvement Does comply Does comply 1.2 Regulatory compliance Does comply Does comply 1.3 Education and staff development Does comply Does comply 1.4 Comments and complaints Does comply Does comply 1.5 Planning and leadership Does comply Does comply 1.6 Human resource management Does comply Does comply 1.7 Inventory and equipment Does comply Does comply 1.8 Information systems Does comply Does comply 1.9 External services Does comply Does comply
Standard 2: Health and personal care
Expected outcome Assessment team recommendations
Agency findings
2.1 Continuous improvement Does comply Does comply 2.2 Regulatory compliance Does comply Does comply 2.3 Education and staff development Does comply Does comply 2.4 Clinical care Does comply Does comply 2.5 Specialised nursing care needs Does comply Does comply 2.6 Other health and related services Does comply Does comply 2.7 Medication management Does comply Does comply 2.8 Pain management Does comply Does comply 2.9 Palliative care Does comply Does comply 2.10 Nutrition and hydration Does comply Does comply 2.11 Skin care Does comply Does comply 2.12 Continence management Does comply Does comply 2.13 Behavioural management Does comply Does comply 2.14 Mobility, dexterity and rehabilitation Does comply Does comply 2.15 Oral and dental care Does comply Does comply 2.16 Sensory loss Does comply Does comply 2.17 Sleep Does comply Does comply
Home name: Arrunga Date/s of audit: 27 October 2009 to 28 October 2009 RACS ID: 0838 AS_RP_00851 v2.5
4
Executive summary of assessment team’s report Accreditation decision
Standard 3: Resident lifestyle
Expected outcome Assessment team recommendations
Agency findings
3.1 Continuous improvement Does comply Does comply
3.2 Regulatory compliance Does comply Does comply
3.3 Education and staff development Does comply Does comply
3.4 Emotional support Does comply Does comply
3.5 Independence Does comply Does comply
3.6 Privacy and dignity Does comply Does comply
3.7 Leisure interests and activities Does comply Does comply
3.8 Cultural and spiritual life Does comply Does comply
3.9 Choice and decision-making Does comply Does comply
3.10 Resident security of tenure and responsibilities
Does comply Does comply
Standard 4: Physical environment and safe systems
Expected outcome Assessment team recommendations
Agency findings
4.1 Continuous improvement Does comply Does comply
4.2 Regulatory compliance Does comply Does comply
4.3 Education and staff development Does comply Does comply
4.4 Living environment Does comply Does comply
4.5 Occupational health and safety Does comply Does comply
4.6 Fire, security and other emergencies Does comply Does comply
4.7 Infection control Does comply Does comply
4.8 Catering, cleaning and laundry services
Does comply Does comply
Home name: Arrunga Date/s of audit: 27 October 2009 to 28 October 2009 RACS ID: 0838 AS_RP_00851 v2.5
5
Assessment team’s reasons for recommendations to the Agency The assessment team’s recommendations about the home’s compliance with the Accreditation Standards are set out below. Please note the Agency may have findings different from these recommendations.
SITE AUDIT REPORT
Name of home Arrunga
RACS ID 0838 Executive summary This is the report of a site audit of Arrunga RACS ID 0838, 334 Kissing Point Road Ermington NSW from 27 October 2009 to 28 October 2009 submitted to the Aged Care Standards and Accreditation Agency Ltd. Assessment team’s recommendation regarding compliance The assessment team considers the information obtained through audit of the home indicates that the home complies with: • 44 expected outcomes Assessment team’s recommendation regarding accreditation The assessment team recommends the Aged Care Standards and Accreditation Agency Ltd accredit Arrunga. The assessment team recommends the period of accreditation be three (3) years. Assessment team’s recommendations regarding support contacts The assessment team recommends there be at least one unannounced support contact each year during the period of accreditation.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 6
Site audit report Scope of audit An assessment team appointed by the Aged Care Standards and Accreditation Agency Ltd conducted the audit from 27 October 2009 to 28 October 2009. The audit was conducted in accordance with the Accreditation Grant Principles 1999 and the Accountability Principles 1998. The assessment team consisted of two registered aged care quality assessors. The audit was against the 44 expected outcomes of the Accreditation Standards as set out in the Quality of Care Principles 1997. Assessment team Team leader: Margaret McCartney
Team member/s: Jill Bicknell Approved provider details Approved provider: The Uniting Church in Australia Property Trust (NSW)
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 7
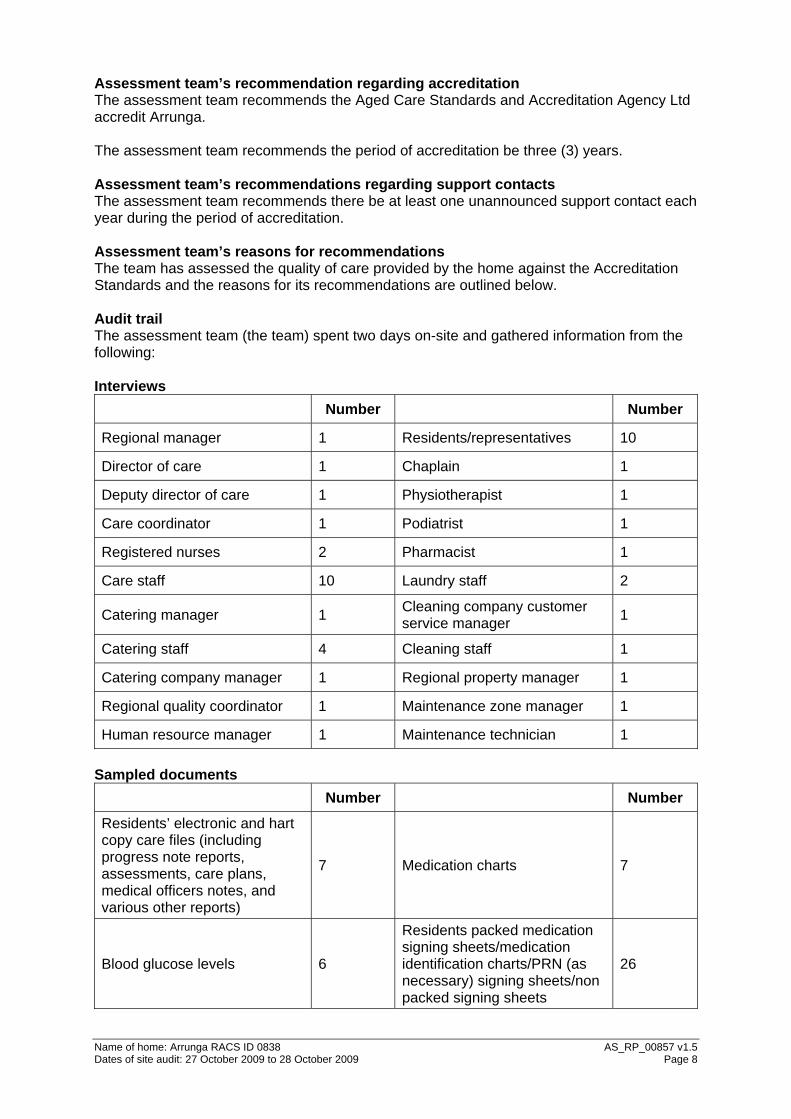
Assessment team’s recommendation regarding accreditation The assessment team recommends the Aged Care Standards and Accreditation Agency Ltd accredit Arrunga. The assessment team recommends the period of accreditation be three (3) years. Assessment team’s recommendations regarding support contacts The assessment team recommends there be at least one unannounced support contact each year during the period of accreditation. Assessment team’s reasons for recommendations The team has assessed the quality of care provided by the home against the Accreditation Standards and the reasons for its recommendations are outlined below. Audit trail The assessment team (the team) spent two days on-site and gathered information from the following: Interviews
Number Number
Regional manager 1 Residents/representatives 10
Director of care 1 Chaplain 1
Deputy director of care 1 Physiotherapist 1
Care coordinator 1 Podiatrist 1
Registered nurses 2 Pharmacist 1
Care staff 10 Laundry staff 2
Catering manager 1 Cleaning company customer service manager 1
Catering staff 4 Cleaning staff 1
Catering company manager 1 Regional property manager 1
Regional quality coordinator 1 Maintenance zone manager 1
Human resource manager 1 Maintenance technician 1 Sampled documents
Number Number
Residents’ electronic and hart copy care files (including progress note reports, assessments, care plans, medical officers notes, and various other reports)
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 8
Bowel charts 23 Pain relieving patch application history sheets 2
Blood pressure charts 5 Wound care plans (hard copy) 7
Resident weight charts 20 Hot and cold pad administration form 1
Clinical observation instructions from local medical officer
3 Personnel files 5
Other documents reviewed The team also reviewed: • Action plan for Arrunga site audit (27/28 October 2009) • Admission checklist • Advanced care directive • Aged care employee and contractors’ police check records • Behavioural monitoring chart (blank) • Care plan review dates lists: high level care and low level care • Chaplaincy resources including, but not limited to: photographs, and advanced directive a
discussion paper for pastoral care and chaplaincy leadership team • Cleaning manual and cleaning schedule • Clinical care handbook • Communication sheet for physiotherapy • Complaints forms • Continence aid extra allocation sheet (blank) • Continuous improvement documentation including: external benchmarking data; audits
and associated results (internal and external); continuous improvement action plan; and continuous improvement summary of achievements
• Doctors’ communication books • Education documentation including: education calendar 2009; handout for administration
of medication in low care facilities; ‘Not just pills’ high care medication administration; and competencies for staff on medication administration
• Electrical test and tagging records 2009 • Emergency procedures manual • External service provider documentation including: contracts, registrations, insurance
agreements • Eyesight assessment • Fire safety records • Fluid balance chart x 1 • Food chart x 1 • Food safety program and manual • Food service questionnaire • Hairdressers notification form • Handover sheets • Incident reporting including: incident reports and graphs with resident incidents each
my story assessments; social, culture and family history assessments; resident consent and social profile assessments; resident care plan; activity program plans; activity participation records; leisure and recreation activity plan; activity description records; activity evaluation by recreational activity officers forms; activity surveys (April 2009); and recreation surveys (August 2009); Catholic resident list; and resident birthday list
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 9
• Low care progress note schedule • Maintenance log records (2009) • Meal choice form (blank) • Medical officers’ contact details • Medication management including: medication signature omission sheets; pharmacy
facsimile order sheets; medication refrigerator temperature records; medication advisory committee terms of reference; monthly audit for medication management (July 2009); medication incident reports; graph with medication incidents; insulin administration instructions; pharmacy newsletter; a guide to using trans dermal medications; policy for medication administration; guidelines for paracetamol use; self medicating assessment (March 2009); nurse initiated medication list; and resources to guide safe and effective administration of non packed medications
• Meeting minutes including: staff meetings; resident meetings, representatives meetings, medication advisory committee meeting, and occupational health and safety/infection control meetings
• Menu • Menu review by dietitian (September 2009) • Newsletters • NSW food authority licence • Occupational health and safety hazard alert control register • Occupational health and safety risk analysis and control plan register • Physiotherapy assessments and care plans • Position descriptions • Privacy statement • Records of education attendance • Recruitment policies and procedures • Resident agreement • Resident dietary information sheets • Resident emergency evacuation list • Resident handbooks (for organisation and for home) • Residents’ information package including: letter of consent for optical, audiology and
podiatry service; residents aged care information sheet; entry and exit criteria for Arrunga; medical emergency consent form; funeral arrangements form; media consent form; declaration of ‘person responsible’; and diet analysis form
• Restraint assessment flow chart • Restraint authorisation (cognitive and mental health domain) • Restraint minimisation policy • Restraint release record x 1 • Safe work practice forms • Schedule eight register • Staff communication books • Staff confidentiality agreement form • Staff orientation information including staff handbook and code of ethical behaviour • Staff roster • Staff signature identification records Observations The team observed the following: • Activities in progress • Activity rooms including shuffle board • Area set aside for coffee shop • Barbecue • Brochures on display in front foyer
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 10
• Car park under building with pedestrian walk way • Charter of residents’ rights and responsibilities on display • Chemical storage and material safety data sheets (MSDS) • Cleaning in progress • Continence aid container in resident room • Daily menu on display • Dining rooms during lunchtimes • Emergency call bell access • Equipment and supply storage areas including continence aids • Fire safety equipment including, fire fighting equipment, fire panel, detectors, sprinklers,
exit signs, smoke doors, correctly orientated evacuation plans and mimic panels • Hair dressing room • Infection control resources including: colour coded equipment in the kitchen and cleaning
areas; first aid kits; spills kits; hand washing signs; sinks; wall mounted soap dispensers; and sanitisation liquid for hand washing
• Interactions between staff/staff and staff/residents and their representatives • Lifts between floor • Living environment (internal living environment including six wings and external living
environment including summer, winter, spring, and autumn courtyards) • Low low beds in use • Medication rounds • Mobility equipment including: mechanical lifters, wheel chairs, and walkers • Notice boards (containing resident/representative information, and staff information) • Nurse call bells in resident rooms and en-suites • Photographs of residents participating in activities • Recreational activity programs on display • Resident sign in and out book • Staff access to computers and information • Staff clinical areas including clinical information resources and computer terminals • Staff work areas (including: kitchen, servery areas, laundry, cleaning room, treatment
rooms, staff room, reception and offices) • Storage of medications • Storage of resident information • Suggestion boxes • Surveillance cameras and screens • Swipe card locks on doors including entrance to dementia specific area • Vision, values, mission and philosophy statements • Visitors/contractors sign in and out book
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 11
Standard 1 – Management systems, staffing and organisational development Principle: Within the philosophy and level of care offered in the residential care service, management systems are responsive to the needs of residents, their representatives, staff and stakeholders, and the changing environment in which the service operates. 1.1 Continuous improvement This expected outcome requires that “the organisation actively pursues continuous improvement”. Team’s recommendation Does comply Arrunga’s continuous improvement is supported through a system that incorporates several avenues for the identification of areas of improvement. The system delivers results through the active identification, implementation and evaluation of improvement opportunities. An internal continuous improvement plan is developed on site and when items are completed they are then moved to a summary of achievements. Self assessments are conducted throughout the year using audits covering all outcomes of the Accreditation Standards, and feedback from residents/resident representatives and staff. Audits are also carried out through a commercial auditing service which is benchmarked with other aged care homes in the organisation. Any adverse benchmarking of the home is then addressed at both site and regional level. Staff interviews demonstrate that staff have opportunities to make suggestions for improvement within the home, which they are confident will be followed up by management. Examples of improvements relating to Accreditation Standard One include, but are not limited to: • Each of the home’s six areas has been given the name of a semi precious stone to help
to differentiate the areas. The areas include Jasper, Amber, Emerald, Sapphire, Topaz, and Jade. Signage has been added throughout the home to facilitate the easy identification and orientation of these areas for residents and representatives.
• The introduction of a pedestrian crossing, reflective mirror and height signs in the undercover car park to reduce the risk/hazard for staff and representatives.
• The introduction of training for the manager as the return to work coordinator. 1.2 Regulatory compliance This expected outcome requires that “the organisation’s management has systems in place to identify and ensure compliance with all relevant legislation, regulatory requirements, professional standards and guidelines”. Team’s recommendation Does comply Systems are in place at an organisational, regional and site level to ensure the identification and implementation of relevant regulatory changes and updates. Notification of regulatory changes and updates is gained through a variety of methods, including subscription to aged care peak industry bodies and an aged care legislative service which provides alerts via emails. Relevant legislation, regulatory requirements, professional standards and guidelines are reviewed by the organisation’s corporate office as well as senior care leadership personnel and other appropriate personnel and changes are sent to the home in the form of information or policy/practice changes. The director of care and/or other appropriate personnel communicate changes to staff via staff meetings, notices, and staff education sessions. Staff also have access to a range of electronic information, and some hard copy resources. Regulatory compliance is monitored through various strategies including audits and staff competency assessments.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 12
Examples of regulatory compliance relating to Accreditation Standard One include: • The organisation conducts reviews of all policy and procedure documentation on a
regular basis to ensure that all relevant legislation, regulatory requirements, professional standards and guidelines are appropriately documented.
• The home has policies and procedures in place regarding the mandatory reporting for alleged or suspected incidents of resident assault and for the reporting of missing residents.
• Procedures for police checks for staff and contractors are in place. Interviews and documentation reviews confirm that these have been completed.
1.3 Education and staff development This expected outcome requires that “management and staff have appropriate knowledge and skills to perform their roles effectively”. Team’s recommendation Does comply Results show that staff education requirements are identified and provided to ensure that staff have the relevant knowledge and skills to perform in their roles effectively. Staff are selected according to the requirements of each role, as documented in job descriptions and a letter of offer of employment. Educational needs are identified though staff requests as well as provision of mandatory education sessions. The education program in the home is overseen by the home’s deputy director of care/education officer. A 12 month education program is developed at the regional level with input from the home’s education officer. The 12 month program covers all four Accreditation Standards. Staff also have access to relevant external educational opportunities. The staff orientation program incorporates a range of topics in relation to management systems, staffing and organisational development and is conducted both for the site and regionally. Staff attendance at education sessions is monitored and skills’ competency assessments are conducted regularly. Records of attendance for individual staff are maintained and feedback is gathered to assess the effectiveness of the training sessions. Staff confirm that adequate education is available to meet their needs. Examples of education and staff development in relation to Accreditation Standard One include: four care staff currently completing a certificate IV in aged care, and the director of care has completed certificate in workplace assessing and training and the WorkCover return to work certificate. 1.4 Comments and complaints This expected outcome requires that "each resident (or his or her representative) and other interested parties have access to internal and external complaints mechanisms". Team’s recommendation Does comply The home has policies, procedures and processes in place to ensure that each resident, representative and other interested parties have access to internal and external complaints mechanisms. Residents and/or their representatives are made aware of internal and external complaints mechanisms through the residents’ handbook, complaint forms, other information displayed in the home and the resident and representative meetings. Avenues are also in place to inform staff of complains mechanisms. Processes for lodging complaints include email access to the director of care. Suggestion boxes are available for the lodging of confidential complaints. The home has a complaints register which documents the actions taken. Documentation reviews demonstrate that all the complaints which have been registered have been actioned in a timely manner. This was also confirmed by feedback from
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 13
residents. Residents/resident representatives interviewed advise that they feel comfortable approaching management about any concerns or suggestions they might have. 1.5 Planning and leadership This expected outcome requires that "the organisation has documented the residential care service’s vision, values, philosophy, objectives and commitment to quality throughout the service". Team’s recommendation Does comply The organisation has developed a mission values statement. This mission values statement is clearly communicated to all stakeholders and posted throughout the home. Management and staff practices and documentation reviews, such as the resident handbook and the staff handbook, confirm the commitment to quality throughout the home. There are a range of mechanisms for planning and reviewing such as regional meetings and staff meetings. 1.6 Human resource management This expected outcome requires that "there are appropriately skilled and qualified staff sufficient to ensure that services are delivered in accordance with these standards and the residential care service’s philosophy and objectives". Team’s recommendation Does comply Results of investigations show that management ensures that appropriate numbers of staff with relevant skills are maintained even though the new home has had a large number of residents entering the home in a short period of time. Management interviews indicate that the home’s staffing has recently increased from 12 to 60 staff over an eight week period. This includes the transfer of a number of staff from a former home within the region. The home is supported by the regional human resource department for the recruitment of skilled staff. All staff receive an orientation, including occupational health and safety, manual handling, fire safety, infection control, and elder abuse. New staff also are ‘buddied’ with more senior staff. Residents/resident representatives interviewed confirm that staff have adequate skills and that there is an emphasis on team work. 1.7 Inventory and equipment This expected outcome requires that "stocks of appropriate goods and equipment for quality service delivery are available". Team’s recommendation Does comply The home has systems in place to ensure that there are adequate supplies of inventory and equipment available for quality service delivery. The home uses a computerised program for purchasing and replacing necessary equipment for use in various functional areas. The team observed storerooms and functional areas, such as staff areas, clinical areas and the kitchen and laundry areas, to be well equipped, well stocked and well maintained. Staff advise that there are adequate supplies of inventory and equipment for them to perform their roles effectively. A routine and preventative maintenance program is in place for the home ensuring that equipment is maintained and ready for use.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 14
1.8 Information systems This expected outcome requires that "effective information management systems are in place". Team’s recommendation Does comply Interviews indicate that residents and staff receive information appropriate to their needs. The resident information system includes, but is not limited to: a variety of documents in the resident information package, administration forms, the resident handbook, the resident agreement, and resident and representative meetings. Staff communication systems include, but are not limited to: meetings; access to computers; the distribution of materials in electronic and/or hard copy such as policies and procedures, and minutes of meetings; staff noticeboards; communication books; and induction and training. A range of both electronic and/or hard copy resident care documentation is maintained. The organisation is currently phasing out all paper based policies and procedures. All computers are secured by password. 1.9 External services This expected outcome requires that "all externally sourced services are provided in a way that meets the residential care service’s needs and service quality goals". Team’s recommendation Does comply The home has a contract management system in place to ensure that externally sourced services are provided in a way that meets the home’s needs and service quality goals. A range of contractors and external service providers operate within contracts and formalised agreements covering resident and care related services, food services, fire systems and various building maintenance and services. Service agreements encompass the organisation’s requirements and expectations for quality service provision, relevant insurances, police checks (where appropriate) and other relevant criteria. Management and staff monitor the performance of external service providers and take appropriate action, including the replacement of services if necessary, to ensure that services are provided at the desired level of quality. For example, a review of one service has resulted in introducing a new service for the residents with positive feedback from residents and representatives. The home also relies on feedback from residents and representatives to assess the quality of service providers. Staff, residents and representatives express their satisfaction with services provided by external providers.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 15
Standard 2 – Health and personal care Principle: Residents’ physical and mental health will be promoted and achieved at the optimum level, in partnership between each resident (or his or her representative) and the health care team. 2.1 Continuous improvement This expected outcome requires that “the organisation actively pursues continuous improvement”. Team’s recommendation Does comply The home has an effective approach to continuous improvement, described in expected outcome 1.1 Continuous improvement, which operates across the four Accreditation Standards, including this Accreditation Standard. Examples of specific improvements relating to Accreditation Standard Two include, but are not limited to: • The introduction of cranberry juice to residents to reduce the incidence of urinary tract
infections. • Alert notifications have been introduced for medications that are required to be
administered outside of normal hours of administration. This is to improve the processes to ensure medications are received by the resident at the correct time.
• The introduction of a weekly gentle exercise group based on a specific program to promote residents’ well being, eye hand coordination, and to maintain and sustain current levels of mobility.
2.2 Regulatory compliance This expected outcome requires that “the organisation’s management has systems in place to identify and ensure compliance with all relevant legislation, regulatory requirements, professional standards and guidelines about health and personal care”. Team’s recommendation Does comply The home’s systems for ensuring regulatory compliance, outlined in expected outcome 1.2 Regulatory compliance, encompass all four Accreditation Standards, including this Accreditation Standard. An example of regulatory compliance relating to Accreditation Standard Two includes: • The home has appropriate arrangements in place to ensure the monitoring of
professional registrations for registered nurses and enrolled nurses. 2.3 Education and staff development This expected outcome requires that “management and staff have appropriate knowledge and skills to perform their roles effectively”. Team’s recommendation Does comply The home’s approach to education and staff development, outlined in expected outcome 1.3 Educational staff development, encompasses all four Accreditation Standards including this Accreditation Standard. Examples of education and staff development in relation to Accreditation Standard Two include: the introduction of training for four personal care assistants in certificate IV aged
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 16
care to meet the needs of the residents. External education sessions on dementia care have been attended by staff from the home including the maintenance technician. Training has been provided for staff on the use of the home’s electronic care documentation system. 2.4 Clinical care This expected outcome requires that “residents receive appropriate clinical care”. Team’s recommendation Does comply The home provides residents with appropriate clinical care through the provision of medical officers’ reviews. The home has an electronic care documentation system for the assessment of residents’ care needs, and for care planning. Management reports that residents’ care planning processes include case conferencing between staff. The home is divided into six areas which each have a nurses’ station and maintain a range of care documentation for residents. One area is designated as a high level care area and provides registered nurse coverage at all times. Many of the residents in this area have been transferred from another home within the region along with the staff from that home. Residents and/or their representatives have a choice of medical officers from those visiting the home. Doctors’ folders are maintained to communicate requests to residents’ medical officers and the home has after hours contact details for medical officers. The home has verbal and written handovers and communication books to inform nursing staff of residents care needs. Residents’ weights and various vital signs are monitored monthly and blood glucose levels are monitored according to residents’ individual identified needs. Clinical observation instructions from medical officers are maintained to guide staff on the ranges of blood pressures and blood glucose levels for residents to be reported to the medical officers. An incident reporting system is in place for the reporting of resident incidents, such as, falls, skin tears, and behaviours of concern. Incident data is collated monthly and monitored through an external benchmarking service. Resident/resident representative interviews indicate they are satisfied with the care provided by the home and the medical treatment given. Interviews also confirm residents/resident representatives have opportunities for input into the care provided. 2.5 Specialised nursing care needs This expected outcome requires that “residents’ specialised nursing care needs are identified and met by appropriately qualified nursing staff”. Team’s recommendation Does comply Residents’ specialised nursing care needs are identified and met by appropriately qualified nursing staff, with medical officers and specialists’ input when required. The home provides ageing in place as well as a 16 bed high level care area which has registered nurse coverage 24 hours a day seven days a week. The home currently provides specialised nursing care for residents including: oxygen therapy and diabetic insulin management. Registered nurses administer residents’ insulin in the high level care area. Care staff advise that they have been provided with training and competency assessments for the administration of residents’ insulin in the low level care areas. The home has a clinical care handbook and access to electronic resources to provide staff with guidelines on procedures for residents’ specialised nursing care if required. A member of the management team is a member of the region’s wound care committee through which wound care policies and protocols are developed. Interviews demonstrate the home accesses supplies of equipment to support residents’ specialised nursing care needs as required. Resident/resident representative interviews indicate satisfaction with the nursing care provided.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 17
2.6 Other health and related services This expected outcome requires that “residents are referred to appropriate health specialists in accordance with the resident’s needs and preferences”. Team’s recommendation Does comply The home has systems to identify residents’ needs and preferences in relation to other health and related services and for making appropriate referrals as required. Interviews and documentation reviews demonstrate examples of residents being seen by health services visiting the home including: physiotherapy, podiatry, optometry, pharmacy, a mobile X-ray, and pathology services. Documentation reviews demonstrate that one resident has had a speech pathology review during a hospital stay. Interviews indicate that one resident has been seen by a dietician. Management advise that an audiology service is available to visit the residents. The home is currently sourcing a dentist to provide a dental service for residents in the home. Residents can choose to visit external health services of their choice, with assistance provided for their transportation by resident representatives. Resident/resident representative interviews demonstrate that residents can choose to see the other health and related services which visit the home or to have external appointments. 2.7 Medication management This expected outcome requires that “residents’ medication is managed safely and correctly”. Team’s recommendation Does comply The home has processes to ensure residents’ medications are managed safely and correctly through: documented policies and guidelines; the use of a prepacked medication administration system; the secure storage of medications; medication management competency assessments completed by care staff; and individual residents’ medication reviews completed by an accredited pharmacist. The pharmacist advises that they are available to provide training and resources for staff including a pharmacy newsletter. Interviews and documentation reviews demonstrate that medication audits are also completed. Residents’ medications are administered by registered nurses in the high level care area and by care staff in the low level care areas. The team observed a registered nurse and a care staff member administering residents’ medications following safe procedures. Care staff advise that they must consult with a registered nurse prior to giving a resident a PRN (as necessary) medication. Residents’ medication signing sheets are filed with medication identification charts with photographic images of residents to assist with the safe delivery of their medications. A self medicating assessment is available for completion by medical officers for residents who choose to self administer their medications. Medications observed by the team are within the expiry dates recorded and eye drop containers are labelled with the dates of opening. The home maintains a schedule eight register in the high level care area. The electronic care documentation system includes medication incident reports. The home participates in a medication advisory committee. Residents/resident representatives interviewed are satisfied with the medication management the home provides. 2.8 Pain management This expected outcome requires that “all residents are as free as possible from pain”. Team’s recommendation Does comply The home ensures residents are as free as possible from pain through initial pain assessments, care planning, and accessing advice on pain management from medical officers and/or the physiotherapist when required. Provision is made for the assessment of Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 18
residents’ verbal and non-verbal pain. Interviews and documentation reviews demonstrate pain management strategies currently in use for residents including: the administration of pain relieving medications such as pain relieving patches and schedule eight medications; the application of heat packs; the provision of pressure relieving equipment; repositioning; gentle exercises; and gentle massage. The physiotherapist advises that they can apply a transcutaneous electronic nerve stimulator to assist with residents’ pain management if required. Resident/resident representative interviews demonstrate that residents are comfortable. 2.9 Palliative care This expected outcome requires that “the comfort and dignity of terminally ill residents is maintained”. Team’s recommendation Does comply The new home has not had any terminally ill residents requiring palliative care at this stage. Management and staff interviews demonstrate that practices would be undertaken to support the comfort and dignity of terminally ill residents. The executive director of care reports that the region has an end of life directive assessment which the home can provide for new residents/resident representatives to start their consideration of end of life care. Management interviews indicate that residents’ palliative care needs would also be discussed at a time when identified to be appropriate. Management interviews indicate that residents’ advanced care directives completed prior to entry to the home are kept on file appropriately for residents. The home has access to advice on residents’ palliative care through local palliative care teams as well as from medical officers. The home’s chaplain and/or local clergy are available to provide spiritual support for terminally ill residents and their representatives as required. The chaplain advises that they are planning to provide staff with training on palliative care. Resident/resident representative interviews indicate they are satisfied that the home would provide appropriate care for residents if they are unwell. 2.10 Nutrition and hydration This expected outcome requires that “residents receive adequate nourishment and hydration”. Team’s recommendation Does comply The home has systems in place to provide residents with adequate nourishment and hydration through the assessment and documentation of residents’ dietary needs and the communication of these needs to catering staff. Meals are provided following a rotating menu which was reviewed by a dietitian in September 2009. Provision is made for residents who require diabetic diets, pureed meals, thickened fluids, assistance with meals, and dietary assistive devices. Management advise that fresh fruit is available in the dining rooms each day for residents. Residents are also provided with fluids at regular intervals as well as water jugs in their rooms unless otherwise indicated. The home monitors residents’ nutrition and hydration status through staff observing the fluids consumed and weighing residents each month. The home has food intake charts and fluid balance charts for completion when indicated. Medication signing sheet reviews demonstrate that several residents currently have dietary supplements provided. Residents/resident representatives express satisfaction with the quantity and quality of the meals and drinks the home provides.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 19
2.11 Skin care This expected outcome requires that “residents’ skin integrity is consistent with their general health”. Team’s recommendation Does comply The home has systems for maintaining residents’ skin integrity consistent with their general health. The electronic care documentation system includes assessments and care plans for residents’ pressure area risk and skin care needs. Interviews and documentation reviews indicate that services including podiatry, hairdressing, and nail care are available for residents. The team observed a podiatrist visiting the home who advises they visit six weekly. Management advise that a beautician and recreational activity officers are available to attend to residents’ finger nail care when required. Care staff interviews demonstrate that residents’ skin integrity is maintained through the application of emollient creams, repositioning of residents, and the provision of pressure relieving equipment. Care staff advise the home has equipment in use to maintain residents’ skin integrity such as airflow mattresses, concave mattresses, and sheep skin booties. The team observed the home has specialised chairs. Residents with skin integrity breakdown have either electronic or hard copy wound care charts completed outlining the wound care provided. The region has a wound care committee to standardise the wound care provided for residents throughout the region. Resident/resident representative interviews indicate satisfaction with the care provided to maintain residents’ skin integrity including wound care. 2.12 Continence management This expected outcome requires that “residents’ continence is managed effectively”. Team’s recommendation Does comply Residents’ continence is managed effectively through the initial assessment of residents’ continence management needs, toileting programs, and support for residents’ continence aid needs. The home has two continence nurses to organise the distribution of residents’ continence aids. This includes the placement of continence aids in containers in residents’ rooms. Management advise that a representative from a continence aid supply company is available to provide staff with training and guidance on the best products to meet residents’ continence aid needs if required. Care staff interviews demonstrate they have access to adequate supplies of continence aids and they provide regular toileting for residents when required. En-suite bathrooms in the dementia specific area are designed so that residents can see their toilet from their bed, to improve their accessibility. The home has strategies for residents’ bowel management including: fibre in residents’ diets; provision of fluids; and the regular administration of aperients for some residents. The home provides cranberry juice with residents’ suppers to help prevent urinary tract infections when necessary. Residents/resident representatives do not identify any issues with residents’ continence management. 2.13 Behavioural management This expected outcome requires that “the needs of residents with challenging behaviours are managed effectively”. Team’s recommendation Does comply The needs of residents with behaviours of concern are identified through the home’s assessment processes. The home provides a 17 bed dementia specific area with a secure living environment for the safety of residents with wandering/absconding behaviours. Care Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 20
staff interviewed described strategies to effectively support residents with behaviours of concern including keeping the residents involved in activities and diversion. The home’s activity programs include activities to support residents with dementia and related behaviours. This includes a visiting music therapist who provides groups and one-to-one support for residents from which, the chaplain advises, good results have been identified to have been achieved. Gardening is also available to help settle residents in the dementia specific area. Documentation reviews demonstrate that the home has a restraint minimisation policy and that alternative strategies to restraint are used when possible. The home has a restraint authorisation and a restraint release record in place for when physical restraint is applied. Management interviews indicate that the home screens residents to ensure their suitability to be accommodated safely in the home. Resident/resident representative interviews demonstrate that staff effectively interact and provide care for residents. 2.14 Mobility, dexterity and rehabilitation This expected outcome requires that “optimum levels of mobility and dexterity are achieved for all residents”. Team’s recommendation Does comply Management interviews indicate examples of residents being supported to achieve optimum levels of mobility and dexterity. A physiotherapist visits the home four hours per week, to complete assessments and care plans for residents as well as providing treatments. The home provides regular exercise groups through the activity program. The team observed residents mobilising with mobility aids, independently and/or with assistance from staff. Strategies for residents’ falls prevention include: the completion of falls’ risk assessments; the availability of a physiotherapist to complete reviews; lowering of beds to the floor when necessary; and incident reporting. The dementia specific area is fitted with sensors which can be used to monitor when residents are out of bed and moving in their bathrooms or rooms. The home provides grab rails in bathrooms to support residents. Residents/resident representatives interviewed do not identify any issues with the support for residents’ mobility and dexterity and confirm that exercise groups are available should residents choose to attend. 2.15 Oral and dental care This expected outcome requires that “residents’ oral and dental health is maintained”. Team’s recommendation Does comply Residents’ oral and dental health care needs are identified and recorded through oral hygiene assessments, and processes are in place for this to be recorded in care plans completed. Residents’ ongoing oral and dental care needs are monitored through staff observations and resident/resident representative feedback. Management advise that the home is currently in the process of sourcing a dentist to visit the home. Residents can also choose to continue to visit external dentists of their choice with assistance in transport provided by their representatives. Care staff interviewed report they provide residents with assistance with denture care, and teeth cleaning. This includes soaking residents’ dentures when indicated. Care staff also advise that some residents in the high level care area have their dentures labelled. Management reports that mouth swabs are available for resident use when needed. Resident/resident representative interviews do not identify any issues with the maintenance of residents’ oral and dental health.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 21
2.16 Sensory loss This expected outcome requires that “residents’ sensory losses are identified and managed effectively”. Team’s recommendation Does comply Residents’ vision and hearing sensory loss needs are identified through initial assessments, and care planning processes. Optometry and/or audiology services can be arranged to visit the home if required or residents can choose to access them externally. The team was shown an example of a resident’s eyesight test completed by the visiting optometry service. Care staff interviews indicate they implement strategies to assist residents with vision impairment and/or hearing loss. This includes escorting residents with vision impairment to the dining rooms and hearing aid care such as battery changes. The home provides large television screens in each lounge area. The chaplain reports that residents in the dementia specific area have access to a garden in which fragrant herbs have been grown. Resident/resident representative interviews indicate satisfaction with the support provided for residents’ sensory loss needs. 2.17 Sleep This expected outcome requires that “residents are able to achieve natural sleep patterns”. Team’s recommendation Does comply The home assists residents to achieve natural sleep patterns through assessments, care planning, and choices of sleeping and waking times. The home is fitted with call bells in residents’ rooms and bathrooms to enable them to call for staff assistance at night. The director of care advises that the home is staffed with one registered nurse and four care staff at night. This includes a care staff member located in the dementia specific area throughout the night. Sensors in residents’ rooms in the dementia specific area also enable staff to monitor residents’ movements at night. A range of strategies are used to support residents to achieve natural sleep patterns including: the availability of warm drinks and snacks at night if required; allowing residents to watch television until late if this is their preference; provision of pressure relieving equipment; continence care; and night sedation as per medical officers’ orders if necessary. All residents have single rooms to assist with providing a quiet living environment conducive to sleep. Residents advise that the home is generally quiet at night and conducive to sleep. Resident representatives interviewed do not identify any problems with residents achieving natural sleep patterns.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 22
Standard 3 – Resident lifestyle Principle: Residents retain their personal, civic, legal and consumer rights, and are assisted to achieve control of their own lives within the residential care service and in the community. 3.1 Continuous improvement This expected outcome requires that “the organisation actively pursues continuous improvement”. Team’s recommendation Does comply The home has an effective approach to continuous improvement, described in expected outcome 1.1 Continuous improvement, which operates across the four Accreditation Standards, including this Accreditation Standard. Examples of improvements relating to Accreditation Standard Three include, but are not limited to: • Translation of the menu into another language to enable choice of menu for a resident
from a culturally and linguistically diverse background. The activity program has also been translated into another language to support residents who do not speak English.
• The appointment of an on site hairdresser for the convenience of the residents. 3.2 Regulatory compliance This expected outcome requires that “the organisation’s management has systems in place to identify and ensure compliance with all relevant legislation, regulatory requirements, professional standards and guidelines, about resident lifestyle”. Team’s recommendation Does comply The home’s systems for ensuring regulatory compliance, outlined in expected outcome 1.2 Regulatory compliance, encompass all four Accreditation Standards, including this Accreditation Standard. Examples of regulatory compliance relating to Accreditation Standard Three include: • Information on residents’ rights is communicated to residents through the home’s
residents’ information package as well as in the resident handbook and the charter of residents’ rights and responsibilities documented in various sources and on display throughout the home.
• The resident agreement outlines a range of information based on the applicable legislation.
3.3 Education and staff development This expected outcome requires that “management and staff have appropriate knowledge and skills to perform their roles effectively”. Team’s recommendation Does comply The home’s approach to education and staff development, outlined in expected outcome 1.3 Educational staff development, encompasses all four Accreditation Standards including this Accreditation Standard. Examples of education and staff development in relation to Accreditation Standard Three include: the staff orientation and in-service sessions canvass issues relating to resident lifestyle such as dementia care, cultural and spiritual care and elder abuse. In addition,
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 23
various aspects of resident lifestyle are covered in the certificate IV in aged care. The chaplain advises that they have provided staff with a spirituality and culture inservice session. 3.4 Emotional support This expected outcome requires that "each resident receives support in adjusting to life in the new environment and on an ongoing basis". Team’s recommendation Does comply The home has systems to ensure each resident receives support in adjusting to life on entry to the home and on an ongoing basis. Systems include providing potential residents and/or their representatives with information on the services available to assist them to identify that the home will meet their needs. Management and staff interviews indicate that new residents/resident representatives are provided with an orientation to the home and that residents are also assisted to settle into the home through the identification and support for their physical and emotional needs. Other mechanisms available to support residents include: introducing new residents to other residents; assisting residents to make their living environment look familiar with personal items on display; and one-to-one support. A chaplain and a pastoral assistant working in the home are available to provide residents with support as required. Resident/resident representative interviews demonstrate they are satisfied with the way the home assists residents to adjust to life in their new home and with the ongoing support and care provided. 3.5 Independence This expected outcome requires that "residents are assisted to achieve maximum independence, maintain friendships and participate in the life of the community within and outside the residential care service". Team’s recommendation Does comply Residents are assisted to achieve maximum independence, maintain friendships and participate in the life of the community within and outside the home as their condition allows. The home provides an environment in which residents’ representatives and visitors are welcome to visit. Review of the visitors sign in and out book demonstrates that a number of people visited the home each day of the Accreditation site audit. The home provides various indoor and outdoor areas in which residents can meet with their guests. Recreational activity officers report that a local school group has visited the home to provide a performance. Residents’ independence is also fostered through ways including: residents having personal items in their rooms; newspaper deliveries on request; and encouragement to maintain independence in attending to the activities of daily living. Several residents are reported to continue to participate in external community groups. The recreational activity program includes bus outings each month. Residents are welcome to attend a mens’ community shed held in the home. The home has plans to open a coffee shop located next to the front foyer. Resident/resident representative interviews indicate satisfaction with the support provided for residents to maintain their independence.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 24
3.6 Privacy and dignity This expected outcome requires that "each resident’s right to privacy, dignity and confidentiality is recognised and respected". Team’s recommendation Does comply The home recognises and respects each resident’s right to privacy and dignity through the identification of residents’ care needs, and the supervision of staff practices. New residents and/or their representatives are provided with information on the home’s policy for the protection of residents’ personal information through the resident agreement. A privacy policy for the Uniting Care Ageing Northern Sydney Region is also on display in the front foyer and includes information on the collection and use of personal information. Residents and/or their representatives are requested to sign a media consent form. Staff interviews demonstrate they understand the need to maintain the confidentiality of resident information and have signed confidentiality agreements on commencement of employment. Care staff advise of strategies applied for maintaining respect for residents’ privacy and dignity including: knocking on the door before entering residents’ rooms and closing doors when providing treatments in residents’ rooms. Observations demonstrate that residents’ care documentation is stored securely. Computerised information is password protected. Residents/resident representatives interviewed express satisfaction with the way staff respect and maintain residents’ privacy and dignity. 3.7 Leisure interests and activities This expected outcome requires that "residents are encouraged and supported to participate in a wide range of interests and activities of interest to them". Team’s recommendation Does comply The home has systems to encourage and support residents to participate in leisure interests and activities of interest to them. This includes completing a range of assessments to identify residents’ interests. Recreational activity officers are employed to provide activity programs five days a week and plans are underway to increase this to seven days per week. The recreational activity programs cater for residents’ various levels of physical and cognitive capabilities. Recreational activity programs record activities available including, but are not limited to: exercises, craft, newspaper readings, falls prevention, bingo, walks, music appreciation, hat making, and happy hours. Photograph reviews show residents participating in various activities. Residents’ individual participation record sheets also demonstrate that residents have attended a range of activities. Documentation is completed to describe the activities available and evaluations of these activities have been completed. Residents/resident representatives are informed of the recreational activities available through activity programs on display, staff prompting, and verbal announcements over a public address system. Residents’ birthdays are included in newsletters and a barbecue is held to celebrate residents’ birthdays each month. Observations demonstrate that the home has a shuffle board for resident use and various rooms in which activities are held. Residents/resident representatives report they are satisfied with the activities the home provides.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 25
3.8 Cultural and spiritual life This expected outcome requires that "individual interests, customs, beliefs and cultural and ethnic backgrounds are valued and fostered". Team’s recommendation Does comply The home has systems in place through which residents’ cultural and spiritual needs are valued including the identification and documentation of residents’ interests, customs, religion and cultural backgrounds. Recreational activity officer interviews indicate that cultural days and religious celebrations are acknowledged and celebrated such as Christmas, Easter, St Patrick’s Day and ANZAC day and Melbourne Cup. The chaplain for the region advises that they are currently working in the home four days a week and have been establishing the new home’s chaplaincy program. A pastoral assistant is also reported to work in the home one day per week. The chaplain and clergy from various denominations hold regular church services to which all residents are welcome to attend. A Roman Catholic mass is held in the home each month. Recreational activity officers advise that a Roman Catholic representative also visits the home to provide Roman Catholic residents with the Eucharist. Interviews indicate that visits from other religious representatives would be organised for residents if requested. The home has processes to support residents for whom English is not their first language including using staff to interpret when available. Staff interviews also indicate that cue cards are available for use to help communicate with residents when necessary. Interviews with the chaplain demonstrate that they plan to hold memorial services to remember deceased residents when applicable. Resident/resident representative interviews do not identify any issues with the spiritual and cultural support the home provides. 3.9 Choice and decision-making This expected outcome requires that "each resident (or his or her representative) participates in decisions about the services the resident receives, and is enabled to exercise choice and control over his or her lifestyle while not infringing on the rights of other people". Team’s recommendation Does comply Residents and/or their representatives are enabled and encouraged to participate in decisions about the care and services provided through information they receive before and at the time of entry to the home. The home informs residents/resident representatives of choices available and their rights through the resident agreement, the organisation’s resident handbook, the home’s resident handbook, and the charter of residents’ rights and responsibilities on display. Examples of residents’ choices for care and services include: personalising of rooms; choice of participation in activities; choice of medical officer; input into care delivery; choice to have telephones in rooms; and choice of bed times. Resident/resident representative input into care and services is also facilitated through resident meetings, comments and complaints’ mechanisms, and management’s ‘open door’ policy. Management advise that resident satisfaction surveys are held by the region each three years. Resident/resident representative interviews confirm that processes are in place to support them to exercise choice and control over the care and services provided within the home.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 26
3.10 Resident security of tenure and responsibilities This expected outcome requires that "residents have secure tenure within the residential care service, and understand their rights and responsibilities". Team’s recommendation Does comply Processes are in place to explain security of tenure to new residents prior to and/or on entry to the home. Management interviews indicate that residents would not be transferred to alternative rooms unless consulted. Management advise that an admissions officer explains the resident agreement and discusses fees and services available with residents and/or their representatives prior to entry to the home. Management reports that residents and/or their representatives are encouraged to seek legal and financial advice on the terms of the resident agreement prior to signing. The resident agreement provides information on residents’ rights and responsibilities including: ending the agreement; transfers; complaints resolution mechanisms; care and services entitlements; an initial 14 day cooling off period; and the charter of residents’ rights and responsibilities. The organisation’s resident handbook also provides information on security of tenure and complaints mechanisms. A range of brochures are on display in the front foyer including brochures on an aged care advocacy service. The home has entry and exit criteria for Arrunga documented. Management interviews indicate that the home has pre 1997 bed allocations which allows for residents to enter at either high level care or low level care with ageing in place. Resident/resident representative interviews generally indicate they have an understanding of residents’ rights and that residents feel secure in their residency in the home. Residents interviewed express satisfaction with the rooms they or their representatives have chosen.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 27
Standard 4 – Physical environment and safe systems Principle: Residents live in a safe and comfortable environment that ensures the quality of life and welfare of residents, staff and visitors. 4.1 Continuous improvement This expected outcome requires that “the organisation actively pursues continuous improvement”. Team’s recommendation Does comply The home has an effective approach to continuous improvement, described in expected outcome 1.1 Continuous improvement, which operates across the four Accreditation Standards, including this Accreditation Standard. Examples of improvements relating to Accreditation Standard Four include, but are not limited to: • The introduction of a new computerised system for recording maintenance requirements
has improved response times and ensures a log is kept to identify equipment with problems.
• The installation of the home’s closed circuit camera has made it easier for the identification of people entering and exiting the building.
• The installation of mimic fire panels has allowed for easier and more accurate identification and monitoring in the event of a fire.
4.2 Regulatory compliance This expected outcome requires that “the organisation’s management has systems in place to identify and ensure compliance with all relevant legislation, regulatory requirements, professional standards and guidelines, about physical environment and safe systems”. Team’s recommendation Does comply The home’s systems for ensuring regulatory compliance, outlined in expected outcome 1.2 Regulatory compliance, encompass all four Accreditation Standards, including this Accreditation Standard. Examples of regulatory compliance relating to Accreditation Standard Four include: • Observations demonstrate the home has relevant regulatory information concerning
occupational health and safety, fire safety and other relevant matters. • Fire safety and other mandatory training takes place. • An annual fire safety statement and records are maintained in accordance with legislative
requirements. • The home has a current food safety licence. 4.3 Education and staff development This expected outcome requires that “management and staff have appropriate knowledge and skills to perform their roles effectively”. Team’s recommendation Does comply The home’s approach to education and staff development, outlined in expected outcome 1.3 Educational staff development, encompasses all four Accreditation Standards including this Accreditation Standard.
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 28
Examples of education and staff development in relation to Accreditation Standard Four include: staff having undertaken compulsory training in fire safety, manual handling, hand washing and other facets of occupational health and safety, as well as training in various aspects of infection control. Evidence was sighted of the catering contractors having completed food safety and handling training. The contracted cleaners have a comprehensive education program including, but not limited to: outbreak procedures, manual handling, swine flu, chemical handling, and safe work practices. 4.4 Living environment This expected outcome requires that "management of the residential care service is actively working to provide a safe and comfortable environment consistent with residents’ care needs". Team’s recommendation Does comply The home has mechanisms in place that demonstrate that they are actively working to provide a safe and comfortable environment consistent with residents’ care needs. These mechanisms include regular environmental safety inspections, cleaning, maintenance and other safety related checks, warm water systems, electrical equipment checks, fire safety systems, hazard assessments, and accident and incident reporting. There is also resident and representative feedback, such as residents meetings and direct discussions with management, in relation to the comfort and safety of the living environment. Resident accommodation is on three levels and all rooms provide one bedded accommodation with en-suite bathroom facilities. The home is divided into six areas made up of either 15 or 16 beds. This includes a secure dementia specific area. Each area provides a lounge area for residents as well as access to a variety of outdoor courtyards and/or garden areas. Four resident dining rooms, some of which are shared between the areas, are currently functioning. Residents/resident representatives express satisfaction with the home’s living environment. 4.5 Occupational health and safety This expected outcome requires that "management is actively working to provide a safe working environment that meets regulatory requirements". Team’s recommendation Does comply There are effective mechanisms in place to ensure that management is actively working to provide a safe working environment that meets regulatory requirements. The home’s safety system is overseen by an occupational health and safety committee, whose membership includes a representative from all departments. The director of care has completed certification in occupational health and safety (OHS) and is a member of the OHS committee for the home and region. The home’s safety system includes: regular staff training (including manual handling); regular safety related audits and inspections; electrical equipment checks; safe operating procedures for chemicals and dangerous goods; access to material safety data sheets; use of personal protective equipment; hazard reporting; and accident and incident reporting. The team’s review of data and discussion with management indicates that accidents and incidents are reported and effectively managed. 4.6 Fire, security and other emergencies This expected outcome requires that "management and staff are actively working to provide an environment and safe systems of work that minimise fire, security and emergency risks". Team’s recommendation Does comply Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 29
Name of home: Arrunga RACS ID 0838 AS_RP_00857 v1.5 Dates of site audit: 27 October 2009 to 28 October 2009 Page 30
The home’s management and staff are actively working to provide an environment and safe systems of work that minimise fire, security and emergency risks. There are documented emergency procedures in place. Fire safety systems in the home include, but are not limited to, fire alarms, a fire panel, mimic panels, smoke/fire doors, the installation of fire fighting equipment, exit signs, regular system and equipment checks, and evacuation plans. The home has formal, external contractual arrangements for the monitoring and maintenance of all fire safety equipment and systems on the site. The team sighted the current fire safety checks. Staff training records confirm that staff participate in regular fire safety training and staff interviewed are aware of fire safety and emergency procedures. The team observed that the home provides a secure living environment including swipe card door locking mechanisms, and the use of security camera surveillance. 4.7 Infection control This expected outcome requires that there is "an effective infection control program". Team’s recommendation Does comply The home has systems for an effective infection control program. The infection control coordinator is responsible for collecting and collating infection data, reviewing causes, supporting early interventions, analysing trends and reporting in the combined OHS and infection control committee meetings. The home has an outbreak policy which has been adopted by all homes within the organisation. Staff are provided with infection control education at orientation and through compulsory training. Staff practices are monitored to ensure an effective infection control program. All staff are offered relevant immunisations and records are kept of these at a regional level. The team observed practices that embrace infection control requirements including the use of personal protective equipment and clothing and the use of colour coded equipment in all areas. Staff interviewed demonstrate an understanding of infection control procedures and resident/resident representatives report satisfaction with the actions taken by staff to minimise infections within the home. Infection control audits are carried out within the home. Legionella testing is carried out on the warm water system every three months. 4.8 Catering, cleaning and laundry services This expected outcome requires that "hospitality services are provided in a way that enhances residents’ quality of life and the staff’s working environment". Team’s recommendation Does comply The home contracts the catering to an external company. Food is cooked fresh on site and a dietician has recently reviewed the home’s four weekly rotating menu. The home’s menu addresses the dietary needs of residents. Residents have input into menus and food quality through the completion of a dietary requirements form on entry to the home, ongoing feedback directly to staff, and resident meetings. The organisation contracts the cleaning to an external company. The team reviewed the safe work procedures and safe work method statement for the cleaners. The cleaning contractor has policies, procedures and appropriate arrangements to ensure that the cleaning services are provided in a way that enhances residents’ quality of life. The external cleaning contractor conducts regular audits and surveys to ensure that they are operating at desired levels. Results are discussed with management and the OHS committee. The contracted cleaner is a representative on the home’s OHS committee. The common areas and residents’ rooms are cleaned regularly with high level care residents’ rooms being cleaned daily. The home has an on site laundry. The home’s laundry system ensures that linen is appropriately laundered and residents’ personal items are washed and returned to their owner, within a reasonable turnaround time. Residents/resident representatives interviewed express satisfaction with the home’s catering, cleaning and laundry services.