Decrease in mortality rate and hospital admissions for acute myocardial infarction after the enactment of the smoking ban law in São Paulo city, Brazil Tania M O Abe, 1 Jaqueline Scholz, 1 Eduardo de Masi, 2 Moacyr R C Nobre, 1 Roberto Kalil Filho 1 1 Medicine Faculty, Heart Institute, University of São Paulo, São Paulo, São Paulo, Brazil 2 Municipal Health Secretary, Municipality of São Paulo, São Paulo, São Paulo, Brazil Correspondence to Tania M O Abe, Heart Institute, Medicine Faculty, University of São Paulo, Rua Dr Eneas de Carvalho Aguiar 44 —1 andar Bloco 2–São Paulo, SP CEP 05403-000, Brazil; [email protected]Received 20 June 2016 Revised 26 September 2016 Accepted 3 October 2016 To cite: Abe TMO, Scholz J, de Masi E, et al. Tob Control Published Online First: [ please include Day Month Year] doi:10.1136/ tobaccocontrol-2016- 053261 ABSTRACT Background Smoking restriction laws have spread worldwide during the last decade. Previous studies have shown a decline in the community rates of myocardial infarction after enactment of these laws. However, data are scarce about the Latin American population. In the first phase of this study, we reported the successful implementation of the law in São Paulo city, with a decrease in carbon monoxide rates in hospitality venues. Objective To evaluate whether the 2009 implementation of a comprehensive smoking ban law in São Paulo city was associated with a reduction in rates of mortality and hospital admissions for myocardial infarction. Methods We performed a time-series study of monthly rates of mortality and hospital admissions for acute myocardial infarction from January 2005 to December 2010. The data were derived from DATASUS, the primary public health information system available in Brazil and from Mortality Information System (SIM). Adjustments and analyses were performed using the Autoregressive Integrated Moving Average with exogenous variables (ARIMAX) method modelled by environmental variables and atmospheric pollutants to evaluate the effect of smoking ban law in mortality and hospital admission rate. We also used Interrupted Time Series Analysis (ITSA) to make a comparison between the period pre and post smoking ban law. Results We observed a reduction in mortality rate (−11.9% in the first 17 months after the law) and in hospital admission rate (−5.4% in the first 3 months after the law) for myocardial infarction after the implementation of the smoking ban law. Conclusions Hospital admissions and mortality rate for myocardial infarction were reduced in the first months after the comprehensive smoking ban law was implemented. INTRODUCTION It is well known that passive smoking increases the risk of heart attacks. In the last 2 decades, many cities and some countries, motivated by the WHO Framework Convention on Tobacco Control, approved partial or total smoking ban laws, con- tributing to the decline in passive smoking. The main benefit of smoking ban laws is the reduction of passive smoking, which is associated with an increase in the risk of myocardial infarction of 30–60%. 1–5 Although this risk might seem dispro- portionately high, it is consistent with laboratory evidence of increasing platelet aggregation and changing endothelial function (observed within 30 min of exposure to tobacco smoke), which can increase the risk of coronary heart disease and trigger acute coronary events. 4–8 Concerning current smoking, previous studies showed benefits of smoking ban laws and other tobacco control policies in reducing current smoking. 9–12 In most of the world, a decline has been observed in rates of hospitalisation for myocardial infarction. The decline prior to the smoking ban laws was attributed to improvements in the treat- ment of risk factors for myocardial infarction and implementation of other preventive measures. After the laws, the pre-existing trend of a decline in rates of hospitalisation for myocardial infarction became more evident, especially in small cities and local- ities; 13–15 in larger cities and countries, 16 17 the reduction of the rates was less significant—other factors such as migration make population control more difficult, which may have influenced these rates. In this scenario, Uruguay, which has ∼3.5 million inhabitants, was the first Latin American country to implement a comprehensive smoking ban law, in 2006, and to corroborate these data. They observed a decrease of 22% in the admissions for acute myo- cardial infarction in the first 2 years after the enact- ment of the law. 18 In Brazil, in 1965, the obligation of having warn- ings about the dangers of smoking on the cigarette packs was introduced. In 1996, some restrictions to cigarette advertising were created and a partial restriction law to not smoking in hospitals, public repartition and some public places were established. Since 2000, the restrictions became more severe. São Paulo is a city of more than 12 million inha- bitants. It is the most populated city in the southern hemisphere and the 14th most global city in the world. It was the first city in Brazil to enact a com- prehensive smoking ban law. The Sao Paulo smoking ban law prohibited the use of cigarettes and other tobacco products in closed and semiclosed places, public and private, with the exception of residences, places of religious worship where smoking is part of the ceremony and sites designated for the consumption of tobacco products. To evaluate the consequences of this law, we con- ducted this study in two parts. The first part was published in 2010, 19 when we analysed the close effect of the implementation of the smoking ban law in São Paulo. We reported a significant reduc- tion in the indoor levels of carbon monoxide (CO) after the law in collective environments, such as Abe TMO, et al. Tob Control 2016;0:1–7. doi:10.1136/tobaccocontrol-2016-053261 1 Research paper TC Online First, published on October 28, 2016 as 10.1136/tobaccocontrol-2016-053261 Copyright Article author (or their employer) 2016. Produced by BMJ Publishing Group Ltd under licence.
Transcript
Decrease in mortality rate and hospital admissionsfor acute myocardial infarction after the enactmentof the smoking ban law in São Paulo city, BrazilTania M O Abe,1 Jaqueline Scholz,1 Eduardo de Masi,2 Moacyr R C Nobre,1
Roberto Kalil Filho1
1Medicine Faculty, HeartInstitute, University ofSão Paulo, São Paulo,São Paulo, Brazil2Municipal Health Secretary,Municipality of São Paulo,São Paulo, São Paulo, Brazil
Correspondence toTania M O Abe, HeartInstitute, Medicine Faculty,University of São Paulo, Rua DrEneas de Carvalho Aguiar 44—1 andar Bloco 2–São Paulo,SP CEP 05403-000, Brazil;[email protected]
Received 20 June 2016Revised 26 September 2016Accepted 3 October 2016
To cite: Abe TMO, Scholz J,de Masi E, et al. Tob ControlPublished Online First:[please include Day MonthYear] doi:10.1136/tobaccocontrol-2016-053261
ABSTRACTBackground Smoking restriction laws have spreadworldwide during the last decade. Previous studies haveshown a decline in the community rates of myocardialinfarction after enactment of these laws. However, dataare scarce about the Latin American population. In thefirst phase of this study, we reported the successfulimplementation of the law in São Paulo city, with adecrease in carbon monoxide rates in hospitality venues.Objective To evaluate whether the 2009implementation of a comprehensive smoking ban law inSão Paulo city was associated with a reduction in ratesof mortality and hospital admissions for myocardialinfarction.Methods We performed a time-series study of monthlyrates of mortality and hospital admissions for acutemyocardial infarction from January 2005 to December2010. The data were derived from DATASUS, the primarypublic health information system available in Brazil andfrom Mortality Information System (SIM). Adjustmentsand analyses were performed using the AutoregressiveIntegrated Moving Average with exogenous variables(ARIMAX) method modelled by environmental variablesand atmospheric pollutants to evaluate the effect ofsmoking ban law in mortality and hospital admissionrate. We also used Interrupted Time Series Analysis(ITSA) to make a comparison between the period preand post smoking ban law.Results We observed a reduction in mortality rate(−11.9% in the first 17 months after the law) and inhospital admission rate (−5.4% in the first 3 monthsafter the law) for myocardial infarction after theimplementation of the smoking ban law.Conclusions Hospital admissions and mortality rate formyocardial infarction were reduced in the first monthsafter the comprehensive smoking ban law wasimplemented.
INTRODUCTIONIt is well known that passive smoking increases therisk of heart attacks. In the last 2 decades, manycities and some countries, motivated by the WHOFramework Convention on Tobacco Control,approved partial or total smoking ban laws, con-tributing to the decline in passive smoking. Themain benefit of smoking ban laws is the reductionof passive smoking, which is associated with anincrease in the risk of myocardial infarction of30–60%.1–5 Although this risk might seem dispro-portionately high, it is consistent with laboratoryevidence of increasing platelet aggregation andchanging endothelial function (observed within
30 min of exposure to tobacco smoke), which canincrease the risk of coronary heart disease andtrigger acute coronary events.4–8 Concerningcurrent smoking, previous studies showed benefitsof smoking ban laws and other tobacco controlpolicies in reducing current smoking.9–12
In most of the world, a decline has beenobserved in rates of hospitalisation for myocardialinfarction. The decline prior to the smoking banlaws was attributed to improvements in the treat-ment of risk factors for myocardial infarction andimplementation of other preventive measures. Afterthe laws, the pre-existing trend of a decline in ratesof hospitalisation for myocardial infarction becamemore evident, especially in small cities and local-ities;13–15 in larger cities and countries,16 17 thereduction of the rates was less significant—otherfactors such as migration make population controlmore difficult, which may have influenced theserates.In this scenario, Uruguay, which has ∼3.5 million
inhabitants, was the first Latin American country toimplement a comprehensive smoking ban law, in2006, and to corroborate these data. They observeda decrease of 22% in the admissions for acute myo-cardial infarction in the first 2 years after the enact-ment of the law.18
In Brazil, in 1965, the obligation of having warn-ings about the dangers of smoking on the cigarettepacks was introduced. In 1996, some restrictions tocigarette advertising were created and a partialrestriction law to not smoking in hospitals, publicrepartition and some public places were established.Since 2000, the restrictions became more severe.São Paulo is a city of more than 12 million inha-
bitants. It is the most populated city in the southernhemisphere and the 14th most global city in theworld. It was the first city in Brazil to enact a com-prehensive smoking ban law.The Sao Paulo smoking ban law prohibited the
use of cigarettes and other tobacco products inclosed and semiclosed places, public and private,with the exception of residences, places of religiousworship where smoking is part of the ceremonyand sites designated for the consumption oftobacco products.To evaluate the consequences of this law, we con-
ducted this study in two parts. The first part waspublished in 2010,19 when we analysed the closeeffect of the implementation of the smoking banlaw in São Paulo. We reported a significant reduc-tion in the indoor levels of carbon monoxide (CO)after the law in collective environments, such as
Abe TMO, et al. Tob Control 2016;0:1–7. doi:10.1136/tobaccocontrol-2016-053261 1
Research paper TC Online First, published on October 28, 2016 as 10.1136/tobaccocontrol-2016-053261
Copyright Article author (or their employer) 2016. Produced by BMJ Publishing Group Ltd under licence.
restaurants, bars and nightclubs, without any significant changein the level of CO in the atmospheric air (outdoor), provingthat the law was working. The same occurred with the level ofCO in the exhaled air of workers in these same places. Thesemeasures were made before and 3 months after the enactmentof the law.19
In this second phase of the study, we analysed the rates ofhospitalisation and mortality for acute myocardial infarctionbefore and after enactment of the law, in August 2009, in SãoPaulo city. We also analysed data for air pollutants, temperatureand humidity of the air and other factors that could contributeto changes in these rates.
METHODSThe Ethics Committee for Research Project Evaluation(CAPPesq) of the Hospital das Clinicas—School of Medicine,University of São Paulo approved this study. It is a time-seriesstudy, and we acquired data from January 2005 to December2010. The law is dated from August 2009, and we acquireddata 4 years before the law went into effect to estimate thebehaviour of myocardial infarction time series, for hospitaladmission rate and for mortality rate.
Study sampleData concerning hospital admissions for acute myocardialinfarction were collected from DATASUS, the administrativedatabase of the Sistema Único de Saúde (SUS; Brazilian PublicHealth System). It includes data from all SUS hospitals of thecity, but not includes data from private hospitals. SUS system isresponsible for about 55% of the medical coverage in Sao Paulocity, according to 2010 Report of Sao Paulo Municipal HealthDepartment.
Mortality data were collected from Mortality InformationSystem (SIM). It includes data from all the city, including publicand private hospitals and deaths occurred out of the hospital.
We used the hospital admission diagnosis or death diagnosis,according to International Classification of Disease, 10thRevision (ICD-10), coded I21 (acute myocardial infarction), I22(subsequent ST elevation (STEMI) and non-ST elevation(NSTEMI) myocardial infarction, I23 (current complicationsfollowing STEMI and NSTEMI myocardial infarction) and I24(other acute ischaemic heart diseases). The data were collectedin a monthly basis from January 2005 to December 2010, andincluded residents of São Paulo city.
The total hospital admission for all diseases in SUS hospitalswas also collected and called ‘total hospital admission’.
Data concerning the total population of São Paulo city wereprovided by the Data Analyses State System (SEADE)Foundation, which is based on the Geography and StatisticsBrazilian Institute (IBGE) decennial census. We estimated thepopulation between the two decennial censuses using geometricprogression analyses.
Pollutant dataData related to environmental variables and atmospheric pollu-tants—maximum and minimum temperature, air relative humid-ity, maximum CO concentration, nitrogen dioxide (NO2),sulfur dioxide (SO2), ozone (O3) and particulate matter (MP10)—were provided by CETESB (Environmental Company of SãoPaulo State) database. The data were acquired from January2005 to December 2010, on a monthly basis.
These data were used to estimate models and to control con-founding. Because of multicolinearity among the variables andthe biologic plausibility of them related to acute coronary
disease, the variables used in the models were CO, minimumtemperature and air relative humidity.
Statistical analysisThe Autoregressive Integrated Moving Average with exogenousvariables (ARIMAX) method was used to analyse the effect ofthe smoking ban law, modelled as a dummy variable, in themortality rate and hospital admission rate data for myocardialinfarction. The ARIMAX models were also adjusted to otherparameters, including ‘total hospital admission’, CO, minimumtemperature and air relative humidity. The ARIMAX methodallows to estimate lag effects of input series and to forecastoutput series, as a function of a linear filter of the input series(transfer function) and of the noise (ARIMA filter) and by con-trolling for the autocorrelations. It enables us to compare thepredicted rate of hospital admission and mortality with the realobserved rate.
Transfer function models were estimated using the ARIMAcommand for ‘Data Analysis and Statistical Software’ Stata/LP,StataCorp, V.10.1.
We also applied Interrupted Time Series Analysis (ITSA) inte-grated into ARIMAX to compare the series trend before andafter the law and to verify changes in the level in the moment ofthe law. The time-series intervention models were conductedusing the ITSA command in Stata/MP, StataCorp, V.14.20
Construction of the ARIMAX modelsThe modelling process followed the Box-Jenkins methodology.First, identification of the best model was performed based onautocorrelations and the presence of unit roots. The autoregres-sive orders p, moving average q and their corresponding sea-sonal orders P and Q were identified by the observation of theautocorrelation and partial autocorrelation functions. The pres-ence of unit roots was tested using the augmented Dickey-Fullertest and Phillips-Perron test. Prewhitening and the cross-correlation function were performed to identify lag correlationorder between input and output series.
Thereafter, transfer function models were constructed. InARIMAX modelling process, environmental series (minimumtemperature, air relative humidity) were inserted first. Thus,atmospheric pollutant series (CO) were input, followed by theintervention series. During the entire process, the model wasadjusted to identify the series and their lags that could better
Table 1 Monthly number of hospital admissions for myocardialinfarction, SUS, city of São Paulo, Brazil, January 2005 to December2010
2 Abe TMO, et al. Tob Control 2016;0:1–7. doi:10.1136/tobaccocontrol-2016-053261
Research paper
explain the rates of mortality and hospital admission for myo-cardial infarction. Because of the multicollinearity among thepollutant series, we chose the series that provided the best
prediction of the event under study and which have biologicalplausibility.
Two models were estimated in this process. First, a completemodel was estimated for the entire period of the study, to evalu-ate the effect of the intervention (smoking ban) in the behaviorof the series. Then, a second model was estimated using onlythe pre intervention data, and creating a forecast model for“future events”. Then, it was possible to compare the real eventrate with the forecasted event rate.
Construction of ITSA-ARIMA modelsIn the ITSA analysis, the Prais-Winsten and Cochrane-Orcuttmethod was used. This method uses the generalisedleast-squares method to estimate the parameters in a linearregression model in which errors are assumed to follow a first-order autoregressive process.
At the end, a more complex ARIMA model was incorporatedto ITSA procedure.20 The model’s accuracy was verified byresidue correlogram analysis, which has autocorrelation andpartial autocorrelation functions, and by the Q test ofLjung-Box. The residue normality was tested by theShapiro-Wilk test. The best model was chosen based on theAkaike Criterion Information, the mean prediction error per-centage and the residual SD. In the entire analysis, 5% signifi-cance level was adopted.
RESULTSThe number of monthly hospital admissions and deaths formyocardial infarction is shown in tables 1 and 2.
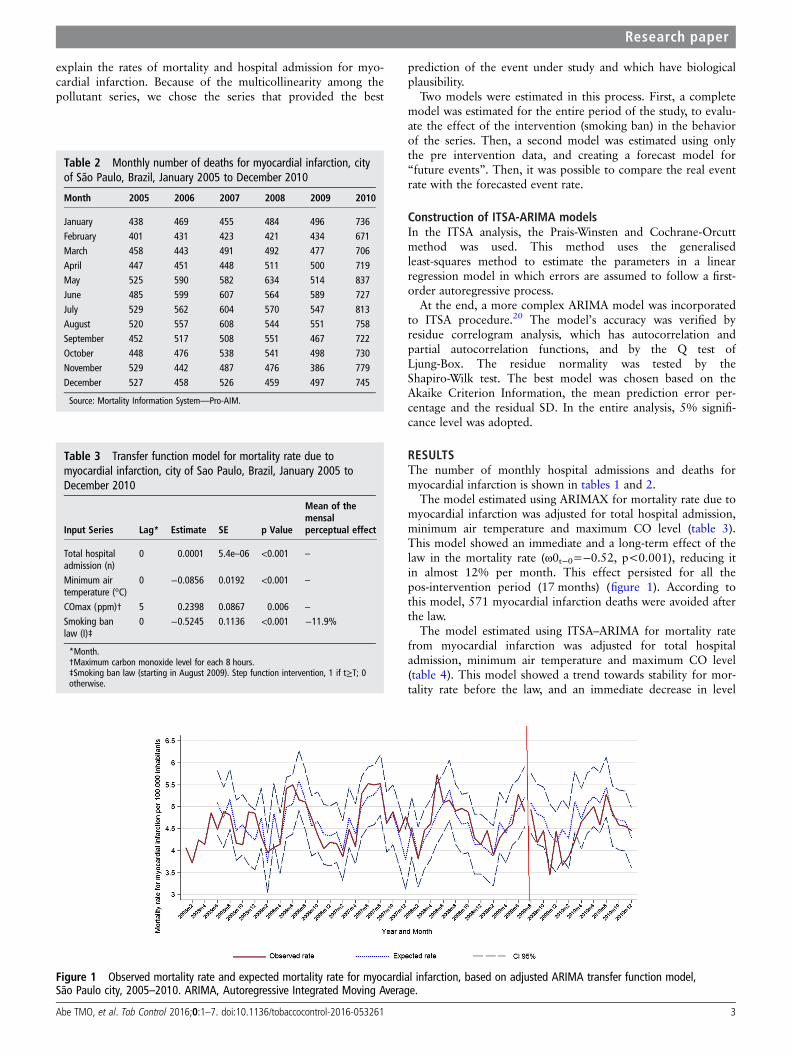
The model estimated using ARIMAX for mortality rate due tomyocardial infarction was adjusted for total hospital admission,minimum air temperature and maximum CO level (table 3).This model showed an immediate and a long-term effect of thelaw in the mortality rate (ω0t−0=−0.52, p<0.001), reducing itin almost 12% per month. This effect persisted for all thepos-intervention period (17 months) (figure 1). According tothis model, 571 myocardial infarction deaths were avoided afterthe law.
The model estimated using ITSA–ARIMA for mortality ratefrom myocardial infarction was adjusted for total hospitaladmission, minimum air temperature and maximum CO level(table 4). This model showed a trend towards stability for mor-tality rate before the law, and an immediate decrease in level
Table 3 Transfer function model for mortality rate due tomyocardial infarction, city of Sao Paulo, Brazil, January 2005 toDecember 2010
Input Series Lag* Estimate SE p Value
Mean of themensalperceptual effect
Total hospitaladmission (n)
0 0.0001 5.4e–06 <0.001 –
Minimum airtemperature (°C)
0 −0.0856 0.0192 <0.001 –
COmax (ppm)† 5 0.2398 0.0867 0.006 –
Smoking banlaw (I)‡
0 −0.5245 0.1136 <0.001 −11.9%
*Month.†Maximum carbon monoxide level for each 8 hours.‡Smoking ban law (starting in August 2009). Step function intervention, 1 if t≥T; 0otherwise.
Table 2 Monthly number of deaths for myocardial infarction, cityof São Paulo, Brazil, January 2005 to December 2010
Figure 1 Observed mortality rate and expected mortality rate for myocardial infarction, based on adjusted ARIMA transfer function model,São Paulo city, 2005–2010. ARIMA, Autoregressive Integrated Moving Average.
Abe TMO, et al. Tob Control 2016;0:1–7. doi:10.1136/tobaccocontrol-2016-053261 3
Research paper
(compared with the counterfactual in the period immediatelypos-intervention) (β2 −0.89; p<0.001). There was no trendtowards change after the intervention (figure 2).
The model estimated using ARIMAX for SUS hospital admis-sion rate for myocardial infarction was adjusted to total hospitaladmission, air relative humidity, minimum air temperature andmaximum CO level (table 5). This model showed an immediateeffect of the smoking ban law (ω0t−0=−0.78, p=0.022), redu-cing monthly myocardial infarction rate in 5.4%. This effectpersisted for 3 months after the smoking ban law (ω1t−3=0.83,p=0.036) (figure 3). According to this model, 142 myocardialinfarction were avoided in the first 3 months after the ban.
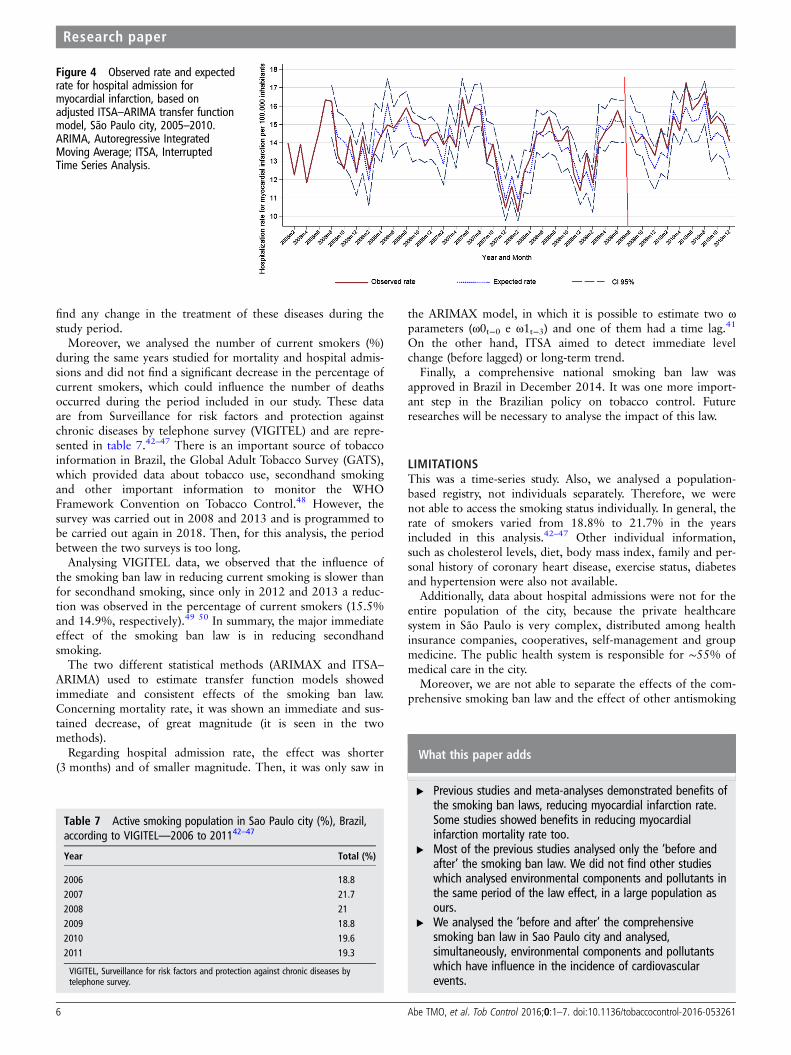
The model estimated using ITSA–ARIMA for SUS hospitaladmission rates for myocardial infarction was adjusted for totalhospital admission, air relative humidity, minimum air tempera-ture and maximum CO levels (table 6). This model showed atrend towards a decrease in the hospital admission rate beforethe law. After the law, it was not observed any significant long-term effect in time series (figure 4).
DISCUSSIONIn this study, a monthly decrease of almost 12% was observedin mortality rate for myocardial infarction in the first 17 monthsafter the enactment of the comprehensive smoking ban law inSão Paulo city.
Additionally, a monthly decrease of 5.4% was found in SUShospital admissions for myocardial infarction during the first3 months after the law. After this period, no additional reduc-tion was observed and the hospital admission rate returned tothe level before the law.
In comparison with previous studies, most of the evidence inthe literature for rates of hospital admission is based on hospitaladmission data,21–25 whereas studies analysing population-basedregistries are limited.26–28 Concerning these previous data, mostof the studies showed a decrease in hospital admission for acutemyocardial infarction after smoking ban laws.
Regarding studies of cardiovascular mortality, only fewstudies examined the effect of smoking ban laws, and the resultswere divergent. Shetty did not find a significant decline in mor-tality for acute myocardial infarction in the USA when compar-ing areas of smoking restrictions with control regions, althoughthere are some questions about the methodology concerningcoverage of local smoking ban laws.29 Rodu studied the behav-iour of myocardial infarction mortality in six states of the USA
Table 4 Interrupted time-series analysis with ARIMA error modelfor mortality rate due to myocardial infarction, city of Sao Paulo,Brazil, January 2005 to December 2010
Input Series Lag* Estimate SE p Value
Total hospital admission (n) 0 0.0001 5.6e–06 >0.001Minimum air temperature (°C) 0 −0.0915 0.0189 >0.001COmax (ppm)† 5 0.2761 0.0863 0.001Preintervention trend 0 0.0067 0.0037 0.070Smoking ban law (I)‡ 0 −0.8889 0.2018 <0.001Postintervention trend 0 0.0196 0.0187 0.294
*Month.†Maximum carbon monoxide level for each 8 hours.‡Smoking ban law (starting in August 2009). Step function intervention, 1 if t≥T; 0otherwise.
Figure 2 Observed mortality rate and expected mortality rate for myocardial infarction, based on adjusted ITSA–ARIMA transfer function model,São Paulo city, 2005–2010. ARIMA, Autoregressive Integrated Moving Average; ITSA, Interrupted Time Series Analysis.
Table 5 Transfer function model for SUS hospital admission ratefor myocardial infarction, city of Sao Paulo, Brazil, January 2005 toDecember 2010
*Month.†Maximum carbon monoxide level for each 8 hours.‡Smoking ban law (starting in August 2009). Step function intervention, 1 if t≥T; 0otherwise.
4 Abe TMO, et al. Tob Control 2016;0:1–7. doi:10.1136/tobaccocontrol-2016-053261
Research paper
where smoking ban laws started and his conclusion was thatlocal smoke-free ordinances had no immediate effect on myo-cardial infarction mortality.30
On the other hand, Villalbi showed a decrease in the mortal-ity rate for acute myocardial infarction in Spain, in apopulation-based registry,31 and the magnitude of the reductionwas similar to ours. Stallings-Smith studied an Irish populationand showed a larger reduction in mortality rate for ischaemicheart disease.32 These two studies have a similarity to ours—they used a population-based registry. Villabi analysed popula-tion separated by sex and age. Stallings-Smith analysed othercauses of mortality. In contrast, none of them analysed theenvironmental influence on these rates as we did.
In the present study, the mortality rate shown is representativeof the entire population of the city (11 million people), and wefound a mean decrease of 11.9% in the mortality rate duringthe 17 months after the law was enacted. Moreover, we analysedpopulation data and environmental components together,looking for the influence of temperature, humidity and air com-ponents and pollutants in cardiovascular diseases. It is knownthat very high temperatures and very low temperatures increasethe rate of cardiovascular events. Some pollutants, such as CO
and particulate matter, have been previously described as causa-tive of cardiovascular diseases.33–36 In this context, we consid-ered it very important to analyse the influence of variations inthese components in the behaviour of the rates of events, whichwas possible using ARIMAX models.
Concerning hospital admissions, most of the studies showed areduction in hospital admission rates in the period of 1–2 yearsafter the law was enacted. One of the reasons that could explainthe fleetingness of the effect for hospital admissions is a peculi-arity of the health system in São Paulo city: it is composed ofthe public health system (SUS), which is responsible for ∼55%of the medical coverage in the city, and a private health system,which is responsible for ∼45% of the medical care in the city.Moreover, Sao Paulo had a previous law with partial restrictionto smoking in some closed places, like public repartitions andhospitals.
Then, we imagine that the population with the highest benefitafter the comprehensive law is the patrons of bars, restaurantsand other establishments not included in previous partial laws,including workers of these places. Most of this population arecovered by private health system and is not included in thisanalysis.
The data described in this paper for hospital admission comefrom the public health system, and we believe the result couldbe more impactful if we had the entire population data, as wehad for mortality rate. Concerning private hospitals, until 2010there was not a standardised data acquisition system of hospitaladmissions for private health system and, because of this, it wasnot possible to acquire these data.
Considering pollutant data, some previous studies conductedin Sao Paulo and in other places, including a meta-analysis,showed a significant association among CO level and particulatematter with cardiovascular diseases.34 37 38 Regarding environ-mental variables, temperature variations are implicated with theoccurrence of myocardial infarction.39 40 In our study, we usedthe pollutant and environmental data to estimate models usingARIMAX method and since the variations of air pollutants arerelated themselves, we opted for using that one which providedthe best prediction of events and that has biological plausibilitywith cardiovascular diseases.
Changes in the treatment of myocardial infarction and strokecould interfere with the mortality and admission rates for thesediseases. We looked for advances in medical care and did not
Figure 3 Observed rate and expectedrate for hospital admission formyocardial infarction, based onadjusted ARIMA transfer functionmodel, São Paulo city, 2005–2010.ARIMA, Autoregressive IntegratedMoving Average.
Table 6 Interrupted time-series analysis with ARIMA error modelfor SUS hospital admission rate for myocardial infarction, city of SaoPaulo, Brazil, January 2005 to December 2010
Input series Lag* Estimate SE p Value
Total hospital admission (n) 0 0.0003 0.00014 <0.001Minimum air temperature (°C) 0 −0.1488 0.02660 <0.001Air relative humidity (%) 7 0.0409 0.0118 0.001COmax (ppm)† 5 0.1953 0.1286 0.118Pre-intervention trend 0 −0.1633 0.0055 0.003Smoking ban law (I)‡ 0 0.0807 0.3460 0.815Pos-intervention trend 0 −0.0425 0.0340 0.211ARIMA error structureAutorregressive 14 −0.5241 0.1096 <0.001
*Month.†Maximum carbon monoxide level for each 8 hours.‡Smoking ban law (starting in August 2009). Step function intervention, 1 if t≥T; 0otherwise.
Abe TMO, et al. Tob Control 2016;0:1–7. doi:10.1136/tobaccocontrol-2016-053261 5
Research paper
find any change in the treatment of these diseases during thestudy period.
Moreover, we analysed the number of current smokers (%)during the same years studied for mortality and hospital admis-sions and did not find a significant decrease in the percentage ofcurrent smokers, which could influence the number of deathsoccurred during the period included in our study. These dataare from Surveillance for risk factors and protection againstchronic diseases by telephone survey (VIGITEL) and are repre-sented in table 7.42–47 There is an important source of tobaccoinformation in Brazil, the Global Adult Tobacco Survey (GATS),which provided data about tobacco use, secondhand smokingand other important information to monitor the WHOFramework Convention on Tobacco Control.48 However, thesurvey was carried out in 2008 and 2013 and is programmed tobe carried out again in 2018. Then, for this analysis, the periodbetween the two surveys is too long.
Analysing VIGITEL data, we observed that the influence ofthe smoking ban law in reducing current smoking is slower thanfor secondhand smoking, since only in 2012 and 2013 a reduc-tion was observed in the percentage of current smokers (15.5%and 14.9%, respectively).49 50 In summary, the major immediateeffect of the smoking ban law is in reducing secondhandsmoking.
The two different statistical methods (ARIMAX and ITSA–ARIMA) used to estimate transfer function models showedimmediate and consistent effects of the smoking ban law.Concerning mortality rate, it was shown an immediate and sus-tained decrease, of great magnitude (it is seen in the twomethods).
Regarding hospital admission rate, the effect was shorter(3 months) and of smaller magnitude. Then, it was only saw in
the ARIMAX model, in which it is possible to estimate two ωparameters (ω0t−0 e ω1t−3) and one of them had a time lag.41
On the other hand, ITSA aimed to detect immediate levelchange (before lagged) or long-term trend.
Finally, a comprehensive national smoking ban law wasapproved in Brazil in December 2014. It was one more import-ant step in the Brazilian policy on tobacco control. Futureresearches will be necessary to analyse the impact of this law.
LIMITATIONSThis was a time-series study. Also, we analysed a population-based registry, not individuals separately. Therefore, we werenot able to access the smoking status individually. In general, therate of smokers varied from 18.8% to 21.7% in the yearsincluded in this analysis.42–47 Other individual information,such as cholesterol levels, diet, body mass index, family and per-sonal history of coronary heart disease, exercise status, diabetesand hypertension were also not available.
Additionally, data about hospital admissions were not for theentire population of the city, because the private healthcaresystem in São Paulo is very complex, distributed among healthinsurance companies, cooperatives, self-management and groupmedicine. The public health system is responsible for ∼55% ofmedical care in the city.
Moreover, we are not able to separate the effects of the com-prehensive smoking ban law and the effect of other antismoking
Figure 4 Observed rate and expectedrate for hospital admission formyocardial infarction, based onadjusted ITSA–ARIMA transfer functionmodel, São Paulo city, 2005–2010.ARIMA, Autoregressive IntegratedMoving Average; ITSA, InterruptedTime Series Analysis.
Table 7 Active smoking population in Sao Paulo city (%), Brazil,according to VIGITEL—2006 to 201142–47
VIGITEL, Surveillance for risk factors and protection against chronic diseases bytelephone survey.
What this paper adds
▸ Previous studies and meta-analyses demonstrated benefits ofthe smoking ban laws, reducing myocardial infarction rate.Some studies showed benefits in reducing myocardialinfarction mortality rate too.
▸ Most of the previous studies analysed only the ‘before andafter’ the smoking ban law. We did not find other studieswhich analysed environmental components and pollutants inthe same period of the law effect, in a large population asours.
▸ We analysed the ‘before and after’ the comprehensivesmoking ban law in Sao Paulo city and analysed,simultaneously, environmental components and pollutantswhich have influence in the incidence of cardiovascularevents.
6 Abe TMO, et al. Tob Control 2016;0:1–7. doi:10.1136/tobaccocontrol-2016-053261
Research paper
policy changes, like increase in tobacco tax rates, implementedalong the years, and especially in 2009.
CONCLUSIONMortality rate and hospital admission rate for myocardial infarc-tion decreased after the comprehensive smoking ban law inSão Paulo city.
Contributors TMOA conducted the study and submitted the article. JS planned thestudy and reviewed the article. EdM made the statistical analysis and help in thearticle writing. MRCN and RKF planned the study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Glantz SA, Parmley WW. Passive smoking and heart disease. Epidemiology,
physiology, and biochemistry. Circulation 1991;83:1–12.2 Glantz SA, Parmley WW. Passive smoking and heart disease. Mechanisms and risk.
JAMA 1995;273:1047–53.3 He J, Vupputuri S, Allen K, et al. Passive smoking and the risk of coronary heart
disease—a meta-analysis of epidemiologic studies. N Engl J Med 1999;340:920–6.4 Barnoya J, Glantz SA. Cardiovascular effects of secondhand smoke: nearly as large
as smoking. Circulation 2005;111:2684–98.5 Whincup PH, Gilg JA, Emberson JR, et al. Passive smoking and risk of coronary
heart disease and stroke: prospective study with cotinine measurement. BMJ2004;329:200–5.
6 Otsuka R, Watanabe H, Hirata K, et al. Acute effects of passive smoking on thecoronary circulation in healthy young adults. JAMA 2001;286:436–41.
7 Pechacek TF, Babb S. How acute and reversible are the cardiovascular risks ofsecondhand smoke? BMJ 2004;328:980–3.
8 Raupach T, Schäfer K, Konstantinides S, et al. Secondhand smoke as an acutethreat for the cardiovascular system: a change in paradigm. Eur Heart J2006;27:386–92.
9 Levy DT, Benjakul S, Ross H, et al. The role of tobacco control policies in reducingsmoking and deaths in a middle income nation: results from the ThailandSimSmoke simulation model. Tob Control 2008;17:53–9.
10 Levy DT, Hyland A, Higbee C, et al. The role of public policies in reducing smokingprevalence in California: results from the California tobacco policy simulation model.Health Policy 2007;82:167–85.
11 Currie LM, Blackman K, Clancy L, et al. The effect of tobacco control policies onsmoking prevalence and smoking-attributable deaths in Ireland using the IrelandSSsimulation model. Tob Control 2013;22:e25–32.
12 Levy D, de Almeida LM, Szklo A. The Brazil SimSmoke policy simulation model:the effect of strong tobacco control policies on smoking prevalence andsmoking-attributable deaths in a middle income nation. PLoS Med 2012;9:e1001336.
13 Sargent RP, Shepard RM, Glantz SA. Reduced incidence of admissions formyocardial infarction associated with public smoking ban: before and after study.BMJ 2004;328:977–80.
14 Centers for Disease Control and Prevention (CDC). Reduced hospitalizations foracute myocardial infarction after implementation of a smoke-free ordinance—City ofPueblo, Colorado, 2002–2006. MMWR Morb Mortal Wkly Rep 2009;57:1373–7.
15 Seo DC, Torabi MR. Reduced admissions for acute myocardial infarction associatedwith a public smoking ban: matched controlled study. J Drug Educ2007;37:217–26.
16 Sims M, Maxwell R, Bauld L, et al. Short term impact of smoke-free legislation inEngland: retrospective analysis of hospital admissions for myocardial infarction. BMJ2010;340:c2161.
17 Juster HR, Loomis BR, Hinman TM, et al. Declines in hospital admissions for acutemyocardial infarction in New York state after implementation of a comprehensivesmoking ban. Am J Public Health 2007;97:2035–9.
18 Sebrié EM, Sandoya E, Hyland A, et al. Hospital admissions for acute myocardialinfarction before and after implementation of a comprehensive smoke-free policy inUruguay. Tob Control 2013;22:e16–20.
19 Issa JS, Abe TM, Pereira AC, et al. The effect of Sao Paulo’s smoke-free legislationon carbon monoxide concentration in hospitality venues and their workers. TobControl 2011;20:156–62.
20 Linden A. Conducting interrupted time series analysis for single and multiple groupcomparisons. Stata J 2015;15:480–500.
21 Lightwood JM, Glantz SA. Declines in acute myocardial infarction after smoke-freelaws and individual risk attributable to secondhand smoke. Circulation2009;120:1373–9.
22 Mackay DF, Irfan MO, Haw S, et al. Meta-analysis of the effect of comprehensivesmoke-free legislation on acute coronary events. Heart 2010;96:1525–30.
23 Meyers DG, Neuberger JS, He J. Cardiovascular effect of bans on smoking in publicplaces: a systematic review and meta-analysis. J Am Coll Cardiol 2009;54:1249–55.
24 Tan CE, Glantz SA. Association between smoke-free legislation and hospitalizationsfor cardiac, cerebrovascular, and respiratory diseases: a meta-analysis. Circulation2012;126:2177–83.
25 Vander Weg MW, Rosenthal GE, Vaughan Sarrazin M. Smoking bans linked tolower hospitalizations for heart attacks and lung disease among medicarebeneficiaries. Health Aff (Millwood) 2012;31:2699–707.
26 Cesaroni G, Forastiere F, Agabiti N, et al. Effect of the Italian smoking ban onpopulation rates of acute coronary events. Circulation 2008;117:1183–8.
27 Cox B, Vangronsveld J, Nawrot TS. Impact of stepwise introduction of smoke-freelegislation on population rates of acute myocardial infarction deaths in Flanders,Belgium. Heart 2014;100:1430–5.
28 Christensen TM, Møller L, Jørgensen T, et al. The impact of the Danish smokingban on hospital admissions for acute myocardial infarction. Eur J Prev Cardiol2014;21:65–73.
29 Shetty KD, DeLeire T, White C, et al. Changes in U.S. hospitalization and mortalityrates following smoking bans. J Policy Anal Manage 2010;30:6–28.
30 Rodu B, Peiper N, Cole P. Acute myocardial infarction mortality before and afterstate-wide smoking bans. J Community Health 2012;37:468–72.
31 Villalbí JR, Sánchez E, Benet J, et al., Barcelona Group for Smoking RegulationPolicies Evaluation. The extension of smoke-free areas and acute myocardialinfarction mortality: before and after study. BMJ Open 2011;1:e000067.
32 Stallings-Smith S, Zeka A, Goodman P, et al. Reductions in cardiovascular,cerebrovascular, and respiratory mortality following The National Irish smoking ban:interrupted time-series analysis. PLoS One 2013;8:e62063.
33 Lee WH, Choo JY, Son JY, et al. Association between long-term exposure to airpollutants and prevalence of cardiovascular disease in 108 South Koreancommunities in 2008–2010: A cross-sectional study. Sci Total Environ2016;565:271–8.
34 Wang XD, Zhang XM, Zhuang SW, et al. Short-term effects of air pollution on acutemyocardial infarctions in Shanghai, China, 2013–2014. J Geriatr Cardiol2016;13:132–7.
35 Luo C, Zhu X, Yao C, et al. Short-term exposure to particulate air pollution and riskof myocardial infarction: a systematic review and meta-analysis. Environ Sci PollutRes Int 2015;22:14651–62.
36 Meo SA, Suraya F. Effect of environmental air pollution on cardiovascular diseases.Eur Rev Med Pharmacol Sci 2015;19:4890–7.
37 Gouveia N, de Freitas CU, Martins LC, et al. [Respiratory and cardiovascularhospitalizations associated with air pollution in the city of Sao Paulo, Brazil].Cad Saude Publica 2006;22:2669–77.
38 Mustafic H, Jabre P, Caussin C, et al. Main air pollutants and myocardial infarction:a systematic review and meta-analysis. JAMA 2012;307:713–21.
39 Lin S, Soim A, Gleason KA, et al. Association Between Low Temperature DuringWinter Season and Hospitalizations for Ischemic Heart Diseases in New York State.J Environ Health 2016;78:66–74.
40 Kwon BY, Lee E, Lee S, et al. Vulnerabilities to Temperature Effects on AcuteMyocardial Infarction Hospital Admissions in South Korea. Int J Environ Res PublicHealth 2015;12:14571–88.
41 Helfenstein U. Box-Jenkins modelling in medical research. Stat Methods Med Res1996;5:3–22.
48 Almeida L, Szklo A, Sampaio M, et al. Global Adult Tobacco Survey data as a toolto monitor the WHO Framework Convention on Tobacco Control (WHO FCTC)implementation: the Brazilian case. Int J Environ Res Public Health2012;9:2520–36.