62
Deep Vein Thrombosis A Case for Early Intervention Hiranya A. Rajasinghe MD Vascular and Endovascular Surgery Naples, Florida
| Date post: | 11-Aug-2015 |
| Category: |
Health & Medicine |
| Upload: | dr-hiranya-rajasinghe |
| View: | 198 times |
| Download: | 0 times |

Deep Vein ThrombosisA Case for Early Intervention
Hiranya A. Rajasinghe MD
Vascular and Endovascular Surgery
Naples, Florida

Mainstream RxClot removal is not a part of recommendation for care
Clot removal is not a part of recommendation for care
2004
Acute Venous ThromboembolismAcute Venous Thromboembolism

AnticoagulationAnticoagulation
Calf DVT Calf DVT
…. for everyone! …. for everyone!
Femoral-popliteal Femoral-popliteal Iliofemoral Iliofemoral
Do not recognize iliofemoral DVT as a unique conditionDo not recognize iliofemoral DVT as a unique condition
……Change occurred in the 2008 guidelines…Change occurred in the 2008 guidelines…
Acute DVTAcute DVT

Where are We Going…
• Surgeon General’s “Call to Action”– Joint Commission/NQF Mandates
• DVT/PE Risk Assessment Protocols 2008– Prevention– Intervention
• ACCP Recommendations Changing 2008– Thrombolytic Therapy
• Iliofemoral
• SIR Recommendations– Thrombolytic Therapy
• Iliofemoral

• This joint effort elevates the awareness of DVT to a National healthcare level.
• This joint effort recognizes the need to standardize the care of DVT patients and measure outcomes.
• The American College of Chest Physicians (ACCP) will publish the physician consensus on patient treatment.– It is changing its 2004 DVT treatment guidelines
• 2007 guidelines will include a thrombolysis recommendation• 2007 guidelines will include a recommendation for
specifically treating iliofemoral DVT (CDT, PMT) (Comerota)
Why is this Information Important ?

6
PE600,00
0
Silent PE1
Million
DVT2
Million
Death
200,000Estimated Cost of VTE Care $1.5 Billion/yearEstimated Cost of VTE Care $1.5 Billion/year
VTE: A Public Health ProblemEstimated Annual Incidence
Post-Thromboti
c Syndrome800,000
Pulmonary Hypertensi
on30,000
Goldhaber. . LancetLancet 1999;353:1386-1389 1999;353:1386-1389

What is a DVT?
• Blood clot in a deep vein• Blocks blood from returning
to heart• Damages the valves and
vein wall• Potentially grow or travel
VEIN

Virchow’s Triad
StasisStasisAir Travel, Obesity, Air Travel, Obesity,
ImmobilityImmobility
Endothelial InjuryEndothelial InjuryLimb Trauma, Major SurgeryLimb Trauma, Major Surgery
HypercoagulabilityHypercoagulabilityBCP, Cancer, HereditaryBCP, Cancer, Hereditary

DVT Risk Factors and Symptoms
Risk Factors
• Immobility, such as bed rest or sitting for long periods
• Previous DVT or family history of DVT
• Recent surgery • Above the age of 40 • Hormone therapy or oral
contraceptives • Pregnancy or post-partum • Previous or current cancer • Limb trauma and/or orthopedic
procedures • Coagulation abnormalities • Obesity
Symptoms
• Pain
• Discoloration of the legs
• Calf or leg pain or tenderness
• Swelling of the leg or lower limb
• Warm skin
• Surface veins become more visible
• Leg fatigue

Economy Class Syndrome
• Flights over 4 hours
• Any prolonged trip in cramped conditions
• Immobility and dehydration
• Prevention:– aspirin, fluids, avoid alcohol, frequent walks,
support stockings

Symptoms
• Commonly no symptoms!• Pain• Swelling• Redness• Palpable clot
Diagnosis• Clinical: exam and
symptoms
• Venous duplex
• Magnetic resonance venography
• Blood test:
Elevated D-dimer

DVT treatments
• MEDICAL – Anticoagulation (blood thinning medications)
• IV Heparin (in hospital only)• Low molecular weight heparin (given at home)• Coumadin (by mouth)
– Support Stockings– Elevation

Therapeutic Goals of DVT Treatment
• Relieve Patient Symptoms• Prevent Pulmonary Embolism• Prevent Further Thrombus Propagation• Prevent DVT Recurrence• Maintain Valve Competence• Prevent Postthrombotic Syndrome

Complications of DVT
• Pulmonary Embolus
• Post-DVT syndrome
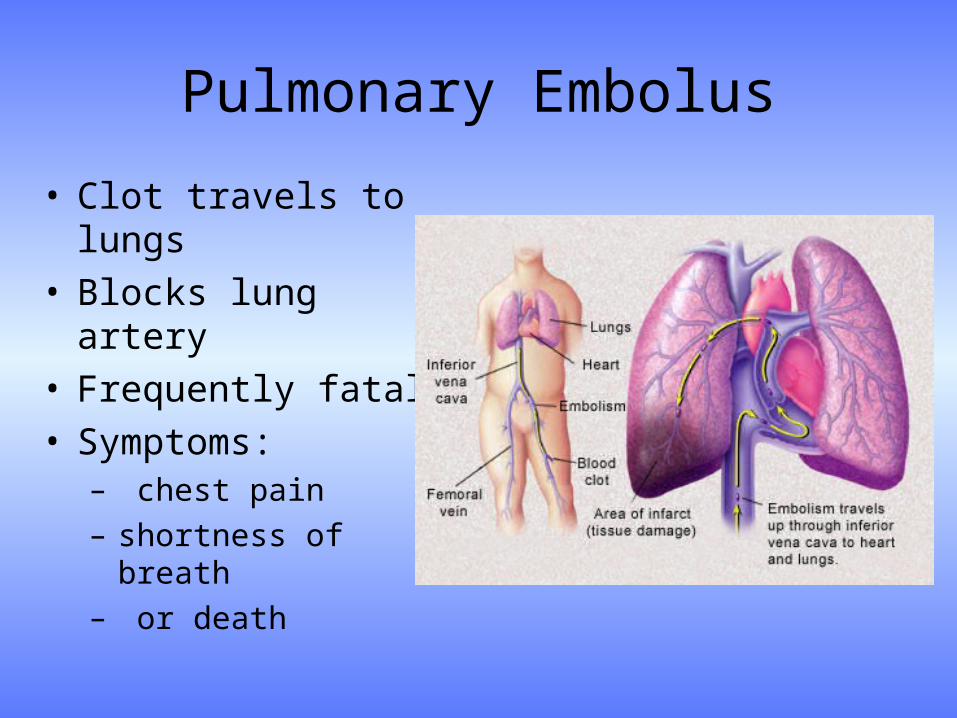
Pulmonary Embolus
• Clot travels to lungs• Blocks lung artery• Frequently fatal• Symptoms:
– chest pain – shortness of breath– or death

Vena Cava Interruption: IVC Filters
Indications:
Prevent large emboli from reaching the lungs
Contraindication for anticoagulation therapy
Complications while receiving anticoagulation therapy
High risk of mortality from recurrent PE
Placement:
Below renal veins
Inserted via jugular or femoral vein
May be easily removed

Caval Filters
• PERMANENT• RETRIEVABLE

What We Know…
• Gold Standard –Anticoagulation
• Heparin, Lovenox, Coumadin
–Compression Hose
• Long Term Results–Anticoagulation
• Prevents Clot from Propagating – Does not dissolve thrombus
• PE Prevention
– May Lead to Post Thrombotic Syndrome

Current Standard Therapy for DVT:Anticoagulation Therapy
• Relies on the patient’s fibrinolytic system for thrombolysis– Veins have limited capacity to dissolve thrombus– Only 6% of patients with acute proximal DVT show complete lysis of
thrombus within 10 days– Recurrent thrombosis and postthrombotic syndrome have been highly
correlated to residual thrombus
• Anticoagulation does not directly resolve symptoms– Leg edema, pain and difficulty ambulating associated with DVT usually
subside over days to weeks as collateral venous channels develop– Many patients continue to experience some degree of venous
obstructive symptoms, especially during exercise
Breddin HK et al. Effects of LMWH on thrombus regression and recurrent thomboembolsim in patients with DVT. N Engl J Med. 2001
Sherry S. Thrombolytic Therapy for Deep venous thrombosis. Semin Intervent Radiol 1985

Post-DVT Syndrome
• Reversed flow of blood in veins
• Symptoms:
pain, swelling, ulceration
• 6-7 million patients with venous stasis changes
• 500,000 patients with leg ulcers yearly

Valvular Damage

Venous Blood Flow• The Low pressure of the venous system
requires special adaptations to help return blood to the heart.
• A complex system of venous valves, the calf muscle pump, and the respiratory pump all assist in returning blood to the heart.
• Venous valves are one way valves of hinge-like flaps formed by the Tunica Intima– Most abundant in the lower limbs where gravity
opposes flow.– Prevent backflow as blood travels toward the
heart.
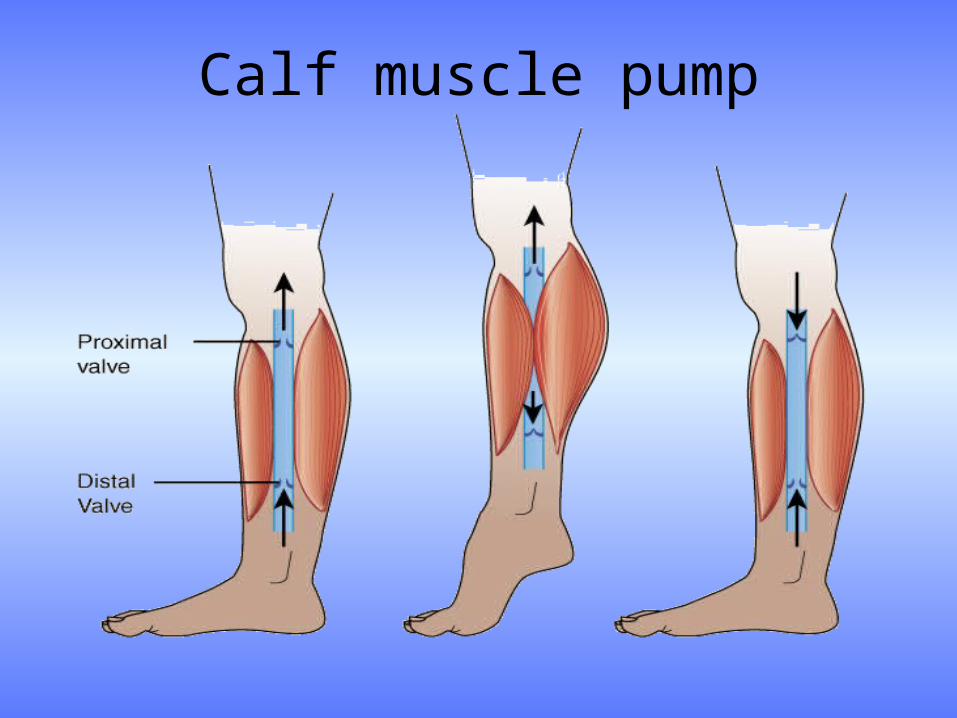
Calf muscle pump

Pathophysiology of Postthrombotic Syndrome
• Acute thrombus, inflammation, and the process of vein recanalization cause valvular reflux
• Reflux and/or chronic obstruction causes venous hypertension which leads to edema, tissue hypoxia, or ulceration
• Clinical studies suggest that reflux in proximal veins is associated with the manifestation of Postthrombotic Syndrome
Kahn et al. Relationship between deep venous thrombosis and the
postthrombotic syndrome. Arch Intern Med. 2004


Postthrombotic Syndrome (PTS)
• 29-47% of DVT patients eventually develop PTS (Prandoni, Brandjes, Kahn)*
• 25-33% of Patients with PTS will develop severe symptoms such as ulcers and skin deterioration (Kahn)
• 75% of the cost of Treating DVT is related to PTS (Kahn, Berqvist)
• 6% of home care clientele and 18% of expenditures are related to PTS (Kahn)
Frequency of PTS with symptomatic DVT (Prandoni)
Follow up Incidence
1 Year 17%
2 Years 23%
5 Years 28%
8 Years 29%
Frequency of PTS with symptomatic DVT (Brandjes)
5 years 47%
Frequency of PTS with symptomatic DVT (Ginsberg)
1 Year 27%

Postthrombotic SyndromeSigns & Symptoms
Signs• Edema• Stasis • Dermatitis• Redness• Dependent Cyanosis• Varicose Veins• Venous dilation• Open Ulcer• Hyperpigmentation• Healed Ulcer
Symptoms• Heaviness• Cramps• Pain• Paresthesia• Swelling• Bursting Pain• Itching

Long-Term Follow-Up• 59 patients with iliofemoral DVT• Conventional anticoagulation• Followed 5 years
Long-Term Follow-Up• 59 patients with iliofemoral DVT• Conventional anticoagulation• Followed 5 years
Anticoagulation
Iliofemoral DVTIliofemoral DVT
Akesson H, Eur J Vasc Surg 1990
Delis K T et alAnn Surg 2004;239(1):116
Akesson H, Eur J Vasc Surg 1990
Delis K T et alAnn Surg 2004;239(1):116

Parameter @ 5 yrs %Calf muscle dysfunction 50%
Ambulatory venous hypertension 95%
Venous insufficiency 90%
Venous claudication 15% -45%
Venous ulceration 15%
Limited ambulation 15%
Reduced QOL nearly all
Parameter @ 5 yrs %Calf muscle dysfunction 50%
Ambulatory venous hypertension 95%
Venous insufficiency 90%
Venous claudication 15% -45%
Venous ulceration 15%
Limited ambulation 15%
Reduced QOL nearly all
Anticoagulation
Iliofemoral DVTIliofemoral DVT
Akesson H, Eur J Vasc Surg 1990
Delis K T et alAnn Surg 2004;239(1):116
Akesson H, Eur J Vasc Surg 1990
Delis K T et alAnn Surg 2004;239(1):116
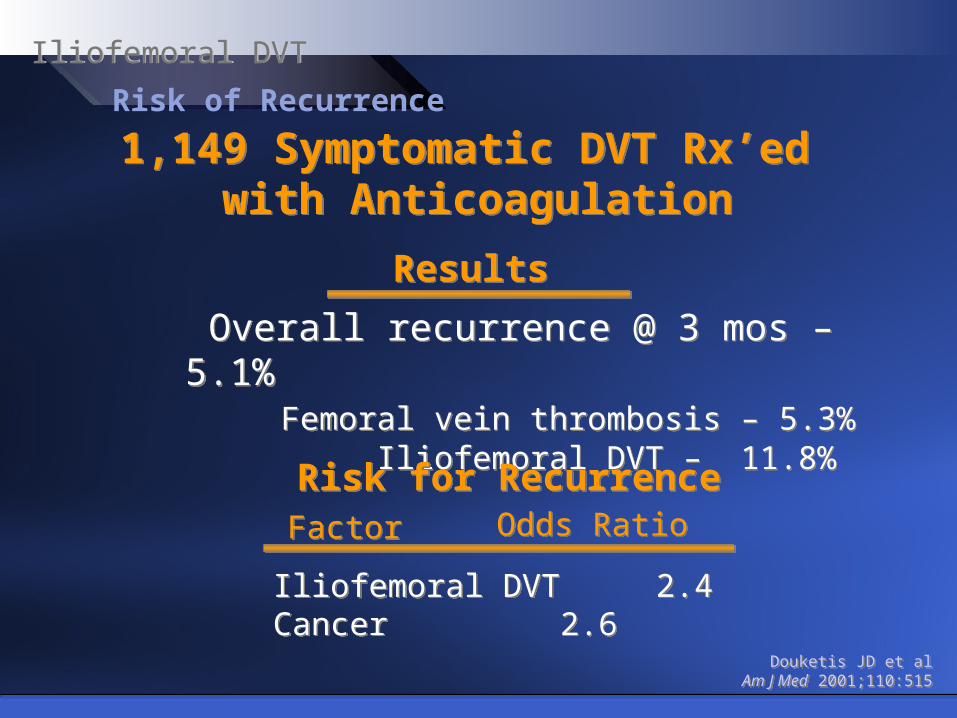
Risk of Recurrence
1,149 Symptomatic DVT Rx’ed with Anticoagulation
1,149 Symptomatic DVT Rx’ed with Anticoagulation
Iliofemoral DVTIliofemoral DVT
Overall recurrence @ 3 mos – 5.1%Femoral vein thrombosis – 5.3%
Iliofemoral DVT – 11.8%
Overall recurrence @ 3 mos – 5.1%Femoral vein thrombosis – 5.3%
Iliofemoral DVT – 11.8%
Douketis JD et alAm J Med 2001;110:515
Douketis JD et alAm J Med 2001;110:515
ResultsResults
Risk for RecurrenceRisk for RecurrenceFactorFactor Odds RatioOdds Ratio
Iliofemoral DVT 2.4Cancer 2.6Iliofemoral DVT 2.4Cancer 2.6

Time after Initial DVT, moTime after Initial DVT, mo
Cu
mu
lativ
e P
rop
ort
ion
of
Pa
tient
s w
ith R
ecu
rre
nt V
TE
Cu
mu
lativ
e P
rop
ort
ion
of
Pa
tient
s w
ith R
ecu
rre
nt V
TE Hazard ratio 2.9 with
residual thrombus P = 0.001
Hazard ratio 2.9 with residual thrombus P = 0.001
Residual Venous Thrombus
Recurrent DVTRecurrent DVT
Prandoni, P et alAnn Intern Med 2002;137:955
Prandoni, P et alAnn Intern Med 2002;137:955
Residual thrombus predictive of recurrent DVTResidual thrombus predictive of recurrent DVT

Increasing evidence…
• Early thrombus resolution is associated with improved outcome!
Increasing evidence…
• Early thrombus resolution is associated with improved outcome!
(especially iliofemoral DVT)(especially iliofemoral DVT)
…and…
• Without thrombus removal, risk of recurrence is increased
…and…
• Without thrombus removal, risk of recurrence is increased
Acute DVTAcute DVT

Early Intervention = Reduction of Postthrombotic
Syndrome• Early thrombus removal may decrease the risk of valvular insufficiency, thereby
decreasing the risk developing postthrombotic syndrome. 1–4
– Rapidly remove clot– Restore venous flow– Preserve valvular function– Identify and treat the cause of the thrombosis
• Valve function is preserved with rapid successful lytic therapy3
• Venous thrombectomy shows significant benefit vs anticoagulation in randomized trials1,4
1. Plate et al. J Vasc Surg. 1984;1:867–876. 2. Meissner et al. J Vasc Surg. 1993;18:596–602.3. Jeffrey et al. Proc 2nd Intl Vasc Sympos. 1989; London Abstract S20–3.4. Plate et al. Eur J Vasc Surg. 1990;4:483–489.
Thrombolytic Therapy for DVT
• Thrombolytic agent is delivered into thrombus using a drug infusion catheter
• Immediate restoration of Vein Patency
• Immediate Resolution of Patient Symptoms
• Preservation of Valve Function– Reduction in Recurrent DVT – Lower Likelihood of Postthrombotic Syndrome
Thrombolytic therapy is an adjunctive therapy to
anticoagulation, not a replacement



1100 Patency @ 1 yr Patency @ 1 yrIliacIliacFemoralFemoral
1100 Patency @ 1 yr Patency @ 1 yrIliacIliacFemoralFemoral
63%63%40%40%
63%63%40%40%
64%64%47%47%
64%64%47%47%
78%78%------------
78%78%------------
Iliac Stent: Patency @ 1 yr Iliac Stent: Patency @ 1 yr ++ StentStent-- StentStent
Iliac Stent: Patency @ 1 yr Iliac Stent: Patency @ 1 yr ++ StentStent-- StentStent
54%54%75%75%
54%54%75%75%
74%74%53%53%
74%74%53%53%
89%89%71%71%
89%89%71%71%
Initial SuccessInitial SuccessIliacIliacFemoralFemoral
Initial SuccessInitial SuccessIliacIliacFemoralFemoral
79%79% 63%63%40%40%
79%79% 63%63%40%40%
83%83% 64%64%47%47%
83%83% 64%64%47%47%
84%84% 78%78%------------
84%84% 78%78%------------
Bjarnason ‘97Bjarnason ‘97Bjarnason ‘97Bjarnason ‘97(n=77)(n=77)(n=77)(n=77)
Mewissen ‘99Mewissen ‘99Mewissen ‘99Mewissen ‘99(n=287)(n=287)(n=287)(n=287)
Comerota ‘01Comerota ‘01Comerota ‘01Comerota ‘01(n=58)(n=58)(n=58)(n=58)
Mewissen et alMewissen et alRadiol Radiol 19991999Mewissen et alMewissen et alRadiol Radiol 19991999
Bjarnason H et alBjarnason H et alJVIRJVIR 1997 1997Bjarnason H et alBjarnason H et alJVIRJVIR 1997 1997
Comerota et alComerota et alPhlebologyPhlebology 2001 2001Comerota et alComerota et alPhlebologyPhlebology 2001 2001
Contemporary Series: Bleeding Complications
Iliofemoral DVT – CD ThrombolysisIliofemoral DVT – CD Thrombolysis

Fatal PEFatal PE
Death 2Death 2°° LysisLysis
Fatal PEFatal PE
Death 2Death 2°° LysisLysis
0%0%
0%0%
0%0%
0%0%
0.2%0.2%
0.4%0.4%
0.2%0.2%
0.4%0.4%
0%0%
0%0%
0%0%
0%0% (? 2%)(? 2%)(? 2%)(? 2%)
Bjarnason ‘97Bjarnason ‘97Bjarnason ‘97Bjarnason ‘97(n=77)(n=77)(n=77)(n=77)
Mewissen ‘99Mewissen ‘99Mewissen ‘99Mewissen ‘99(n=287)(n=287)(n=287)(n=287)
Comerota ‘01Comerota ‘01Comerota ‘01Comerota ‘01(n=58)(n=58)(n=58)(n=58)
Bleeding complications < 5%in reports since 2001
Bleeding complications < 5%in reports since 2001
Contemporary Series: Bleeding Complications
Iliofemoral DVT – CD ThrombolysisIliofemoral DVT – CD Thrombolysis
Mewissen et alMewissen et alRadiol Radiol 19991999Mewissen et alMewissen et alRadiol Radiol 19991999
Bjarnason H et alBjarnason H et alJVIRJVIR 1997 1997Bjarnason H et alBjarnason H et alJVIRJVIR 1997 1997
Comerota et alComerota et alPhlebologyPhlebology 2001 2001Comerota et alComerota et alPhlebologyPhlebology 2001 2001
Pulm EmbPulm EmbPulm EmbPulm Emb 1%1% 1%1% 1%1%1%1% 0%0%0%0%
Major BleedMajor BleedMajor BleedMajor Bleed 5%5%5%5% 11%11%11%11% 9%9%9%9%
IC BleedIC BleedIC BleedIC Bleed 0%0%0%0% <1%<1%<1%<1% 0%0% 0%0%


• Trellis 8 clinical resultsO’Sullivan JVIR 2007; 18:715-724
• 19 Oncology patients with above knee DVT treated with Trellis with one year follow up.
• 96% of limbs showed Grade III and Grade II thrombus removal immediately post procedure
• Primary assisted patency rate of 100% at 30 days post procedure• Valvular function was maintained in 82% of treated lower extremities
(one year follow up) • Systemic thrombolysis was absent in patients tested for serum
fibrinogen levels or fibrin degradation products• All patients had an adjunctive procedure (PTV and/or venous
stenting)



Pharmaco-Mechanical Thrombolysis
• Combines thrombolytic infusion with mechanical energy
• Increases the surface area penetration of thrombolytics
• Dissolves and macerates thrombus
• Reduces the thrombolytic dose
• Reduces the time of thrombolytic infusion
• Reduces or eliminates patient time in the ICU

Patient Selection Patient with an expected long-term survival
Massive DVT or iliofemoral thrombophlebitis
Iliofemoral DVT
Multiple segment DVT
Patients who are symptomatic despite anticoagulation
Acute clot diagnosis: <14 DAYS

Isolated Thrombolysis Catheter –
Design and Components
Balloon Inflation & Thrombolytic Infusion Ports
8Fr Multi-LumenCatheter
Oscillation Drive Unit
Isolated Treatment Zone
Combination of Mechanical Motion & Drug Infusion
• Single-Setting Thrombolysis
• Targeted delivery of thrombolytic agents
• Treatment area isolated within occluding balloons
• Mechanical dispersion of infused thrombolytic agents
• Aspiration following treatment
Aspiration Port

Isolated Thrombolysis Catheter -
Thrombus Removal
Aspiration allows removal of residual vessel content
• Post-Operative Care:– Monitor Puncture Site and Dressings– Begin Standard Anti-Coagulation Therapy– Observe Patient for 4-8 Hours, Depending on Physician Orders
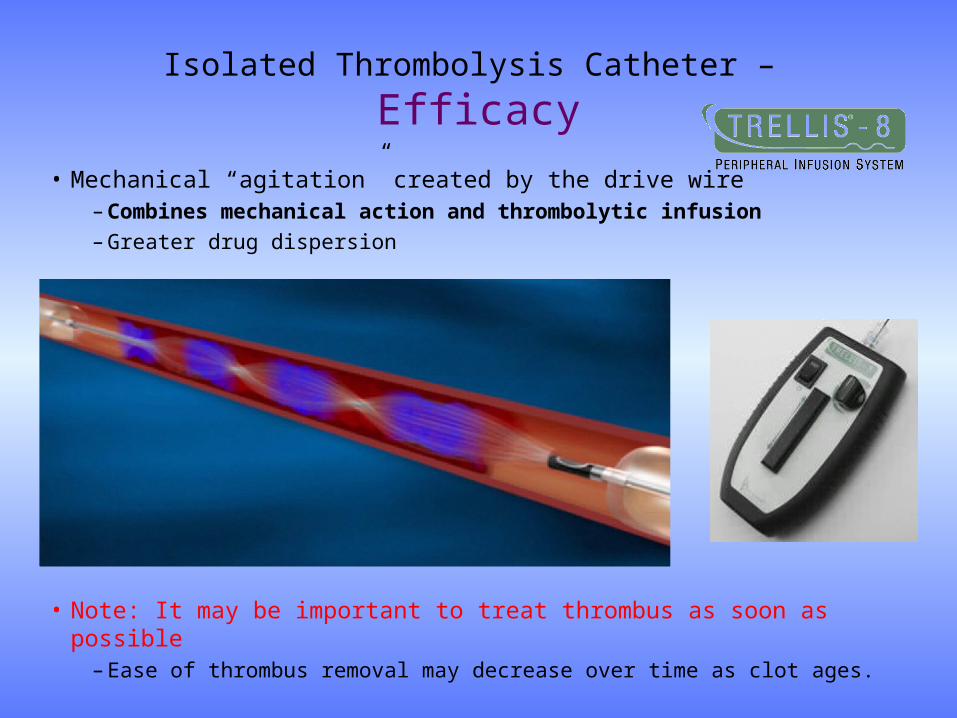
Isolated Thrombolysis Catheter –
Efficacy
• Mechanical “agitation” created by the drive wire– Combines mechanical action and thrombolytic infusion
– Greater drug dispersion
• Note: It may be important to treat thrombus as soon as possible– Ease of thrombus removal may decrease over time as clot ages.

Isolated Thrombolysis Catheter Potential for Improved Safety
Isolated treatment zone: Created by 2 Occlusion Balloons
Potential for lower lytic utilization Reduced treatment time
Procedure TimeDosage
(t-PA)
Catheter Directed
Thrombolysis
2-6 days
0.5mg/hr
(24mg / 2 days)
Isolated Thrombolysis
2 hours3-5mg
(per segment)

Isolated Thrombolysis Catheter –
TRELLIS Venograms
Full occlusion in common femoral through iliac veinsFull occlusion in common femoral through iliac veins
Patency restored throughout treated areasPatency restored throughout treated areas

Isolated Thrombolysis Catheter
Symptom Relief
Pain and swelling caused by iliofemoral DVT
Reduced swelling following Isolated Thrombolysis

May Thurner Syndrome(Iliac Vein Compression)

Iliofemoral Vein ThrombusCase Study
Iliac/Femoral Vein with Iliac/Femoral Vein with Acute on Chronic Acute on Chronic
ThrombusThrombusIliac Vein Subacute ThrombusIliac Vein Subacute Thrombus
Final FilmFinal Film

DVT also occurs in the arm
Thoracic outlet syndromePaget Schroeder syndrome
Chronic catheterizationDialysis access
Trauma

Subclavian DVTCase Study
BeforeBefore AfterAfter

Subclavian Thrombus Removed

Isolated Thrombolysis Catheter -
Benefits For All• Isolated Thrombolysis:
– Pharmaco-Mechanical system aids in rapid thrombus removal – Restores vessel patency– Minimizes drug exposure
• Patient:– More immediate symptomatic relief– Decreased risk of Post-Thrombotic Disease (PTS)– Potential for NO ICU Stay and overall shorter length of stay– Single setting treatment of DVT
• Physician & Staff:– 1.5 to 2 hour procedure– Easier post-up care– Elimination of repeat venograms
• Hospital:– Decreased Procedural Costs:
• $2,000-$3,000 Per DVT Patient
– Decreased ICU Costs• $4,000-12,000 Savings per DVT Patient

The Evolution of DVT Treatment

DVT Management Strategy
Anticoagulation/Lysis Risk Assessment*
PMT
Temporary IVC Filter Anticoagulation
IVC and/or Iliofemoral Femoral/Popliteal Isolated Calf
Symptomatic Asymptomatic
Unstable Thrombus?
Compression HoseAnticoagulation
Follow-up
Compression Hose
Consider Hypercoagulability Work-up
Yes
No
Follow-up
Lytic Contraindications? Isolated PMT*
Correct Underlying Stenosis

Therapeutic Goals of DVT Treatment
Relieve Patient Symptoms
Prevent Pulmonary Embolism
Prevent Further Thrombus Propagation
Prevent DVT Recurrence
Maintain Valve Competence
Prevent Postthrombotic Syndrome

Early Intervention =Quality of Life Improvement

















