DEFENSE MECHANISM INTRODUCTION Healthy people desire, work towards and function best when they think positively & feel good about themselves & their accomplishments, goal &relationships. They want to be content with the environment, accepting of self & accepted & loved by others. At same time, they also desire & work toward avoidance of anxiety, discomfort distress & mental or physical pain. All of these at one time or another are an inevitable part of the human condition. People use numerous ways to avoid anxiety & contend with stress. Some of these are conscious methods or techniques that may be learned & may be adaptive or maladaptive, where another are unconscious & operate automatically. The unconscious mechanisms are sometimes referred to as protective ego defenses. DEFINITION Acc. to FREUD, in 1904 used the term “defense mechanism” to refer to the unconscious process that defends the person against anxiety. THEORY OF SIGMUND FREUD Sigmund Freud (1856 – 1939), an Austrian psychiatrist & founder of psychoanalysis, develop a complex theoretical formulation of the nature of the human personality. The following major components of this theory: 1) Levels of awareness 2) Personality structures 3) The concept of anxiety & defense mechanism 4) Psychosexual stages of development LEVELS OF AWARENESS Essentially, Freud’s level of awareness provides a mental typography that is divided into three parts. 1) the conscious 2) the preconscious 3)the unconscious CONCIOUS - the conscious includes all experiences that are within a person’s awareness at any given time. For 1
Transcript
DEFENSE MECHANISM
INTRODUCTIONHealthy people desire, work towards and function best when they think positively & feel good about themselves & their accomplishments, goal &relationships. They want to be content with the environment, accepting of self & accepted & loved by others. At same time, they also desire & work toward avoidance of anxiety, discomfort distress & mental or physical pain. All of these at one time or another are an inevitable part of the human condition.
People use numerous ways to avoid anxiety & contend with stress. Some of these are conscious methods or techniques that may be learned & may be adaptive or maladaptive, where another are unconscious & operate automatically. The unconscious mechanisms are sometimes referred to as protective ego defenses.
DEFINITION Acc. to FREUD, in 1904 used the term “defense mechanism” to refer to the unconscious process that defends the person against anxiety.
THEORY OF SIGMUND FREUDSigmund Freud (1856 – 1939), an Austrian psychiatrist & founder of psychoanalysis, develop a complex theoretical formulation of the nature of the human personality. The following major components of this theory:
1) Levels of awareness2) Personality structures3) The concept of anxiety & defense mechanism4) Psychosexual stages of development
LEVELS OF AWARENESSEssentially, Freud’s level of awareness provides a mental typography that is divided into three parts.1) the conscious 2) the preconscious 3)the unconscious CONCIOUS - the conscious includes all experiences that are within a person’s awareness at any given time. For example all intellectual, emotional & interpersonal aspects of a person’s behavior that a person is aware of & is able to control & within conscious awareness. All information that is easily remembered & immediately available to an individual is in the conscious mind. PRECONCIOUS – The preconscious includes experiences, thoughts, feelings, or desires that might not be in immediate awareness but can be recalled to consciousness. The preconscious (sometimes called subconscious) can help screen out extraneous information & can enhance concentration. The preconscious can censor certain wishes & thinking & helps repress unpleasant thoughts or feelings.
UNCONCIOUS- Freud described the mind as iceberg to convey the relationship between the conscious & the unconscious .The water’s surface represents the boundary between the conscious & the unconscious.
1
The unconscious refers to all the memories, feelings, thoughts or wishes that are not available to the conscious mind. Often these repressed memories, thoughts, feelings or wishes could if made prematurely conscious, trigger enormous anxiety.However, unconscious material often does become manifest in dreams, slips of the tongue or jokes or thought the use of hypnosis, therapy or certain drugs.
PERSONALITY STRUCTURESFREUD organized the structure of personality into three major components: the id, ego & superego. They are distinguish by their unique functions & different characteristics.
ID- The id the locus of instinctual drives – the “pleasure principle”. Present at birth, it endows the infant with instinctual drives that seek to satisfy needs & achieve immediate gratification.Id- driven behaviors are impulsive & may be irrational.
EGO-the ego, also called the rational self or the “reality principle” begins to develop between the ages of 4&6 months. The ego experiences the reality of he external world, adapts to it, & responds to it. As the ego develops & gain strength, it seeks to bring the influences of the external world to bear upon the id & to substitute the reality principle. A primary function of the ego is one of mediator, that is, to maintain harmony among the external world, the id & the superego.
SUPEREGO-If the id is identified as the pleasure principle & the ego the reality principle, the superego might be referred to as the “perfection principle”. The superego which develops between ages 3&6 years, internalizes the values & morals set forth by the primary care givers. Derived out of a system of rewards & punishments, the superego is composed of 2 major components: the egoideal & the coscience.When a child is consistently rewarded for “good” behavior, the self-esteem is enhanced & the behavior becomes part of the egoideal; that is, it is internalized as part of child’s value system. The conscience is formed when the child is punished consistently for “bad” behaviors. The child learns what is considered morally right or wrong from feedback received from parental figures &from society or culture. When moral or ethical principles or even internalized ideals & values are disregarded, the conscience generates a feeling of guilt within the individual. The superego is important in the socialization of the individual because it assists the ego in the control of id impulses. When the superego becomes rigid & punitive problems with low self – confidence & low self esteem arise.
DEFENSE MECHANISM Defense mechanisms are unconscious responses used by person to protect themselves from internal conflicts and external stressors. There are many situations when we fail in our attempts & get frustrated. Our failures and frustrations may bring injury to our ego and causes anxiety & feeling of inferiority. Some methods of developing a compromise & relieving that tension & anxiety in needed. The human being is usually able to relieve the conflict by utilizing
2
certain forms of adaptations which are called ego defense mechanisms, adjustment mechanisms or mental mechanisms,
Defense mechanisms enable a person to “resolve the conflict” and reduce the “stress & anxiety” associated with it.
All of us use defense mechanisms some time or the other in our normal behavior .when use moderately, they are harmless & help us face conflicts & frustrations easily &protect our ego. However, excessive & persistent use of these mechanisms is harmful as they do not solve conflicts & frustrations basically, but only help the individual to make adaptations to distressing experiences.
Ego defense mechanisms are meant to maintain psychological integration & to protect our self concept from devaluation. If they are used beyond certain limits, they become the symptoms of abnormality & interfere with the resolution of adjustive demands. Some of the ego defense mechanisms are:-
1) REPRESSIONS - Acc.to Freud, repression is basic to all other forms of defense mechanisms. Repression refers to the process by which an individual strives to keep unacceptable, painful, unpalatable & anxiety provoking needs, urges & feelings associated with them in the unconscious layer of the mind.
Repression is the sort of “burying alive” mechanism. Therepressed material is always active in the unconscious memories or urges continue to seek expression & may emerge in the form of accidents such as slips of the pen or tongue, dreams, sleep walking & sleep talking, unconscious mannerisms, phobias & psychosomatic illness. Many painful experiences are repressed during early childhood & become unconscious sources of emotional conflict in later life.The repressed material forms part of the unconscious level of the mind & may affect behavior without the person being aware (unconscious motivation) for example a child may feel angry with his mother because she had punished him. If he feels too guilty about his anger, he may repress it & may still be unconsciously angry. This may be shown by accidental breaking of his mother’s favorite things or in his bed wetting or refusal of food or in stubborn behavior.
2) REACTION FORMATION- It is acting opposite of what one thinks or feels.It is sometimes possible to conceal a motive from ourselves by giving strong expression to its opposite. Such a tendency is called reaction formation.EXAMPLE-the mother of unwanted child may feel guilty & so becomes over indulged & over protective of the child to assure herself that she is a good mother.People who are extremely friendly, overtly polite & very socially correct frequently have unconscious feelings of anger & hatred towards many people.
3) PROJECTION- Projection is a frequently used unconscious mechanism that relieves tension & anxiety by transferring the relieves tension & anxiety by transferring the thoughts to another person. It is an attempt to deal with our own short comings, by seeing them in others & denying them in ourselves.
EXAMPLE-the student who believes that everybody cheats in examinations may also cheat in same way. People who are dishonest often attribute dishonesty to others.
3
The boy fails in a test says that the teacher has not been teaching properly. A doctor who has done a mistake in the operation may insist that it happens
because the nurse & ward boy did their task poorly.
4) RATIOALISATION- Here we “MAKE EXCUSES” giving a reason different from the real one for what we are doing. Excusing on behavior to avoid guilt responsibility, conflict, anxiety or loss of self respect. It operates in two forms :A) sour grapes b) sweet lemon Sour grapes- the individual gives the demerits example
A young man who fails to get a beautiful wife may remark that a beautiful wife is a liability.
A doctor without a vehicle does not want to risk his life by driving a scooter or a car.
An unskilled worker always quarrels about tools.
Sweet lemon- the individual justifies his lower achievements by pointing out their merits.
Example -A poor ideal man “does not want to earn more money because” Money is the root cause of many evils”. People living in small houses due to limited financial resources may point out
many virtues of small houses.
5) INTELLECTULAISATIO N- It is similar to a rationalization. Intellectualization is the distancing from an emotional or threatening situation by talking or thinking about it in intellectual terms. A nurse, doctor or paramedical worker cannot afford to become emotionally attached to each patient. So they speak calmly & intelligently rather than emotionally with patients & their families.Example- if there is a patient who is actually ill, calmly tell the family members rather than saying “I am sorry”.
6) DISPLACEMENT - Ventilation of intense feelings towards persons less threatening than the one who aroused those feelings.
EXAMPLE- A person who is angry with his boss, but cannot show it for fear of losing the job may fight with his wife & children on return from the job may fight with his wife & children on return from the office or kick his dog. When a new baby is the centre of attraction, an older child may become jealous,
prevented from harming the baby; the child may damage a doll or a toy.
7) REGRESSION- Moving back to a previous developmental stage in order to feel safe or have needs met. An adult behaving like a child is particular regression. When faced with difficulties of life, the individual reverts a less mature from of behavior, where he finds less conflict & hence less anxiety.Regression is manifested in several ways such as crying on someone’s shoulder, baby talk, nail biting, thumb sucking, crying etc.
8) SUBLIMATION –Channeling of socially acceptable activities.
4
EXAMPLE-A young men who has lost his lover may turn to write poetry about love.
A person who has aggressive feelings may not be able to express these in society but can become a boxer or solider.
One positive result of sublimation is personal satisfaction experienced by the individual. Society also profits as activities like creative writing, music, painting results of sublimation.
9) IDENTIFICATION - Incorporation of the image of an emulated person than acting, thinking & feeling like that person (unconscious mental mimicry)EXAMPLE-Thus, the little boy takes the masculine attributes that he admires in his father. Girls identify with their mother, later perhaps with their teacher & later still perhaps with a film star.
10) COMPENSATION- Compensation is counter balance for deficiency in one area by excelling in another area. Just as nature compensate for diseases in our bodies (as when a blind person develops extra ordinarily keen hearing), so we develop personality trade to compensate favors inadequacies. Example:- A student who fails in his study may compensate becoming the college champion in athletes. A not a beautiful girl can compensate by studying hard and coming first in her
class.
11) Denial:- Denial of reality is when we refuse to accept or believe the existence of some thing that is very unpleasant to us. We use denial most often when faced with death, serious illness or something painful and threatening.Example: Non acceptance of fatal diagnosis such as AIDS. -When some near or dear one die in the family, some people try to keep up the
pretence that he is still alive.
12) Fantasy or day dreaming:-It is kind of withdrawal when faced with real problems of life. We retire to make belief world, where everything is possible. Where we are victor or conqueror. The tendency to day dream is most pronounced during adolescence. Example:- Patient who are very ill may fantasies that when they recover, many good things will happen to them.
13)Withdrawal:- Whenever an individual suspects that he is likely to be criticized, ridiculed or disgraced on account of some prior unfortunate experience or failure, he restored to withdrawal. Such a person is seen as avoiding all the work saying that he can not do this or he can not do that. It may occur as a temporary pattern. They make no real friends.
14) Conversion:- Hear an emotional conflict is expressed as physical symptom for which there is no organic basis. Example:- A student Nurse, very anxious about her exam, may develop a headache.
5
A woman invited for a party which presents an unsetting situation to her may develop G.I. symptom and may excuse herself from the party. Usually, when party time is over her symptom resolve themselves.
15) Suppression:- Suppression is an intentional pushing away from awareness of certain unwelcome ideas, memories or feeling. We merely push them in to the background, into our subconscious mind. Where they are accessible to us whenever we wish to remember them. EXAMPLE: - A student decides not to think about a parent’s illness in order to study for a test.
A patient may refuse to consider his difficulties by saying that he does not want to talk about it.
. 16) Undoing :- Exhibiting acceptable behavior to make up for negative unacceptable behavior. Apologizing for wrong done to other, repentance and undoing punishment are the difference forms of undoing. This is to resolve the guilt feeling and make a new beginning. EXAMPLE: -The unfaithful husband may bring his wife present.
A man who is ruthless in business donates large amount of money to charity.
17) Introjections: - Introjections is closely related to identification. Accepting another person’s attitude, believe and values as ones own.EXAMPLE: - a person who dislikes guns becomes an avid hunter, just like a best friend.
18) Depersonalization- a destruction of personal identity is depersonalization. It is characterized by the feelings of unreality & estrangement from the self body or surrounding. Some people with depersonalization feels as though they arte become cut off from themselves & are blaming themselves from outside. Some feel that their body is dead.
19) ISOLATION- isolation is the separation of a thought or a memory from the feeling tone or emotions associated with it. EXAMPLE- a young woman describes bring attacked and raped by a street gang. She displays an apathetic expression & no emotional tone. -A physician is able to isolate her feelings about the eventual death of a terminally
ill cancer client by focusing her attention instead on the chemotherapy that will be given
.20) Symbolization- the use of words, ideas or objects to symbolically represent repressed thoughts, feelings & impulses that are relegated to the unconsciousness. EXAMPLE: A Patient has a panic attack when he loses a good luck charm because he believes that he is safe only if the object is in his possession.
6
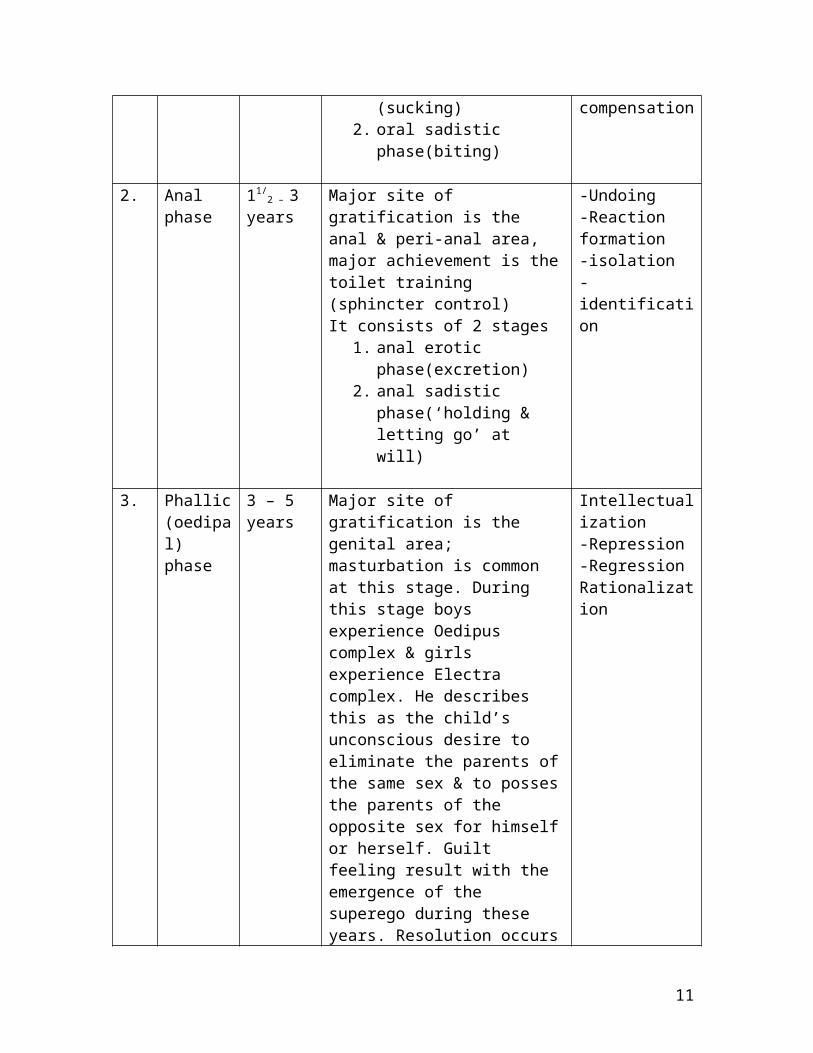
FREUD’S STAGES OF PERSONALITY DEVELOPMENTFREUD described formation of the personality through five stages ofsycho sexual development. He placed much emphasis on first five years of life & believed that characteristics developed during these early years Fixation in an early stage of development almost certainly results in psychopathology..
s.no. Phase Age Normal development Ego defenses1. Oral
phase1-11/
2
yearsmajor site of gratification is the Oral region. It consists of 2 phases:
Major site of gratification is the genital area; masturbation is common at this stage. During this stage boys experience Oedipus complex & girls experience Electra complex. He describes this as the child’s unconscious desire to eliminate the parents of the same sex & to posses the parents of the opposite sex for himself or herself. Guilt feeling result with the emergence of the superego during these years. Resolution occurs by identification with parents of the same sex.
Oedipus complex is usually resolved at the beginning of this stage. This is a stage of relative sexual quiescence.Superego is formed at this stage. Sexual drive is channelized into socially appropriate goals like development of interpersonal relationship, sports, school work, etc.
-Sublimation- projection
7
5. Genitalphase
12 yearsonwards
Adult sexuality develops with capacity for intimacy. Puberty & respect for others. Gradual release from parental controls with more influence of peer group. True self identity develops.
Symbolization
EGO COMPITENCE SKILL
SKILL 1; ESTABLISHING CLOSNESS AND TUSTING RELATIONSHIPS.A basic skill for positive growth and development is the child’s ability to establish close and trusting relationship with others. Children with the medical diagnosis of generalized anxiety disorders may have difficulty establishing trusting relationship because they are very concerned about their perceived competency. The following questions are used to evaluate this skill:
Does the child enjoy making friends? Does the child often feel picked on by other people? Does the child not know what to say when getting to know someone?
To reinforce the skill, nursing staff should encourage interaction and be attentive to the child without being intrusive. Talking with child in a face to face position & offering nurturance are beginning nursing action. Trust can then be demonstrated by the Staff in their interaction with the child. If a child violates trust, a discussion of the issue should take place, allowing trust to be reestablished. In this way children learn about acknowledging mistakes and the importance of forgiveness in developing trusting relationship.
SKILL 2: HANDLING SEPERATION & INDEPENDENT DECISION MAKING.Children who has separation anxiety have great difficulty tolerating separation from their mother or home. Yet individuation is an important mental health process. Being able to identify and express feeling and make independent decisions is critical to becoming a component individual. The following questions are used to evaluate this skill:
Does the child get upset or worry when away from his or her mother? Does the child get upset or worry if he or she thinks someone does not like him or
her? When upset, is there something the child can do to feel better?
Nursing intervention that focus on helping the child identify and clarify the aspects of the self are critical exercises for promoting individuation. This may be done in many ways such as by encouraging children to draw self – portraits, interviewing staff members regarding their opinions on an issue, or identifying personality differences between themselves & others. In the therapeutic milieu, opportunities also can be provided for the child to make choices& decisions, further supporting the child’s growing sense of individuality & ego competency.
SKILL 3: HANDLING JOINT DECSION MAKING AND INTERPERSONAL CONFLICT.Children who have not been allowed to participate in joint decision making or who have not been rewarded for cooperating may be deficient in skill. A child with oppositional
8
defiant disorder may use aggression instead of negotiation to respond to internal conflict. However, learning the skill of joint decision making is critical for success in interpersonal relationships. The following question are used to evaluate the skills:
When the child has a problem, can he or she usually think of several solutions? Does the child get angry if he or she does not get his or her way? Do other people make the child agitated or easily upset?
The therapeutic milieu can provide an opportunity for the child to learn and practice these skills. For example, the nurse can set up opportunities for problem solving. Exercises may be developed for making group decision in which cooperation & collaboration are rewarded. The child should helped to identify fears related to cooperating with others, and assertiveness can be modeled and taught. It is important that the nurse not resolve conflict for the child. Rather, these situations should be used to teach negotiating skills and shape appropriate socialization through the use of reinforcement.
SKILL4:DEALING WITH FRUSTRATION AND UNFAVORABLE EVENTS.Tolerating frustration, although difficult, is critical to becoming a component adult, children with conduct disorders often have difficulty understanding a situation from another’s perspective. The following questions are used to evaluate this skill:
Does the child feel bad if he or she has hurt someone’s feelings? If someone disagrees with the child, does it make him or her angry? Does the child not like playing a game if he or she loses?
Children who have little frustration tolerance become angry easily and are often unable to complete tasks. Children typically learn this skill through cooperation and competition in playing childhood games. However , if the child has not had the opportunities to play games in this way & if the tolerance has not been modulated for child, he or she probably has not developed this skill. The child will face numerous frustration during the course of treatment. The nurse should use this opportunities to think through the process with the child & help increases the child’s frustration tolerance & anger control.
SKIL5: CELEBRATING GOOD FEELING & FEELING PLEASUREHealthy children raised in a nurturing environment naturally experiences good feelings & pleasure. However the children who are depressed or anxious are not able to celebrate good feelings or experiences spontaneous pleasure. Also ,in a maladaptive environment shame is often used to control the children’s behavior, with the result they feel guilty for having angry or unacceptable thoughts. Consequently, they may lose the ability to celebrate the life and feel pleasure. The following questions are used to evaluate this skill:
Does the child worry about the future a lot? Does the child not like it when people say good things about him or her? Does the child feel good about the things he or she does well?
A healthy environment is one in which celebrating the good feelings & feeling pleasure are natural, spontaneous occurrences. Celebrating & have fun are the important nursing interventions. These activities should not be confined to holidays but should be the part of Childs daily activities. Children’s families can be invited to celebrate in these
9
celebrations, where nursing staff model having fun with the children. In this way , children & their families learn the skill of celebrating good feelings & feeling pleasure.
SKILL 6:WORKING FOR DELAYED GRATIFICATIONAs the children grow they are expected to delay needed gratification by following rules & waiting their run. This skill is often difficult for impulsive children with conduct disorder to achieve. The following questions are used to evaluate this skill;
Does the child believe that most rules are responsible & does he or she not mind following them?
Does the child find it difficult to be honest & think that the lying is the only think to do?
Does the child get angry if his or her mother does not give what he or she wants? Delayed gratification can be taught by the nurse through the earning of points for daily expectations, such as tidying one’s room or completing homework assignments. Children’s games, such as red light, in which they respond to “stop” & “wait” commands, are also useful in teaching this skill to younger children. As a child’s behavior improves the reward for the points earned can require the accumulation of many points or tokens. Thus the child is given the opportunity to delay the reinforced for a reward of higher value to be received at a later time. As the child learns greater self control, he or she will be better able to delay gratification for longer periods of time.
SKILL 7: RELAXING AND PLAYINGGiven the stressful environment of current family life, many children may have little opportunity to learn the skill of relaxing and playing. For children with mood , anxiety, or behavior disorders, learning to relax & play is an important skill. The following questions are used to evaluate this skill:
Are there some things the child really enjoys doing? Can the child have lots of fun? Does the child enjoy sitting around & thinking about things?
Time should be devoted to learning skill. Children should be given unstructured play time in which the staff participate with them in playing games. Having spontaneous talent shows or other forms of fun can contribute to a child’s well- being. In this way, relaxing & playing become part of the therapeutic experience & children learn to value & master this skill.
SKILL 8: CONGNITIVE PROCESSING THROUGH WORDS, SYMBOLS, AND IMAGESChildren with psychiatric illnesses may not have developed the important skill of cognitive processing. The following questions are used to evaluate this skill:
Is it difficult for the child to describe how he or she fees? Does the child feel as if he or she never knows how something is going to turn
out? Can the child identify his or her strengths?
A responsive environment should be created to stimulate children’s cognitive development. Furnishings & toys, communications & interactions, and group experiences should all be designed to support the child’s cognitive processing. The nurse can help the
10
child learn this skill by encouraging abstract thinking whenever possible, such as by asking “ what is the moral of the story?” or “what point do you want to think the movie was communicate ?” Children who are encouraged to express themselves in a responsive environment will gain greater competency in this important area of development.
SKILL 9: ADAPTIVE SENSE OF DIRECTION AND PURPOSE Children who experience symptoms of mental illness may feel hopeless about their purpose in life. As they view adult life from watching those around them, they being to draw conclusions about themselves in the world. The following questions are used to evaluate this skill:
Does the child feel that his or her life going to get better? Is the child confused about growing up & doesn’t know what to do about it? Does the child believe that school is important & see it as his or her job in life at
present? Having role models for healthy, meaningful adult experiences is essential to healthy growth & development. Feeling valued as an individual provides the child with an opportunity to learn to value others. Nurses should actively listen to children in their interactions, and even young children should be encouraged to express their needs c& feelings. The child’s importance as a person can be shown through the approach the nurse uses in providing basic care. The nurses should actively help all children realistically assess their & potential to contribute to a better world.
USE OF DEFENSE MECHANISM IN PERSONALITY DISODERS
1. PARANOID: A personality disorder with essential feature of pervasive distrust & suspiciousness of others interpreted as being deliberately demeaning, threatening, or malevolent.
PROJECTION: actively disown undesirable personal traits & motives & attributes them to others; remain blind to one’s own unattractive behaviors & characteristics, yet is over alert to & hypercritical of similar features in others.
2. SCHIZOID: A personality disorder with the essential feature of the lack of enjoyment of close relationships & lack of desire for social or sexual involvement.
INTELLLECTUALIZATION: Describes interpersonal & affective experiences in a matter of fact, abstract, impersonal, or mechanical manner; pays primary attention to formal aspects of social & emotional events.
3. SCHIZOTYPAL: A personality disorder with excessive introversion, pervasive & social interpersonal deficits, cognitive & perceptual distortions & eccentricities in communication & behavior.
11
UNDOING: Bizarre mannerisms & idiosyncratic thoughts appear to represent a retraction or reversal of previous acts or ideas that have stirred feelings of anxiety, conflict, or guilt, ritualistic or “magical” behavior serve to repent for or nullify assumed misdeeds or “evil” thoughts
4. ANTISOCIAL: a personality disorder with the essential feature of a pattern of disregard for & violation of the rights of others beginning at 5 years of age.
ACTING OUT: Rarely constrained inner tensions that might accrue by postponing the expression of offensive thoughts and malevolent actions, socially repugnant impulses are not sublimated , but are discharged directly in perception ways, usually without guilt.
5. BORDELINE: a personality disorder with essential features of a pervasive pattern of unstable interpersonal relationships, self image & moods along with impulsive behavior beginning in early adulthood.
REGRESSION: Retreats under stress to developmentally earlier levels of anxiety tolerance, impulse control, & social adaptation ; among adolescents, is unable to cope with adult demands & conflicts; as evident in immature, if not increasingly infantile, behaviors.
6. HISTRIONIC: a personality disorder with the essential feature of a pervasive & excessive & emotionality & attention seeking behavior beginning in early adulthood.
DISSOCIATION: Regular alerts self presentations to create a succession of socially attractive but changing facades; engages in self- distracting activities to avoid reflecting on and integrating unpleasant thoughts & emotions.
7. NARCIASSISTIC: a personality disorder with exaggerated sense of self importance preoccupation with being admired, & lack of empathy for the feelings of others. RATIONALIZATION: Is self deceptive in devising plausible reasons to justify self centered & socially inconsiderate behaviors; offer alibis to place oneself in the best possible light, despite evident shortcomings or failures.
8. AVOIDANT: A personality disorder with extreme social inhibition & introversion, hypersensitivity to criticism & rejection, limited social relations, & low self esteem FANTASY: Depends excessively on imagination to achieve need gratification & conflict resolution, withdraws into reveries as a means of safely discharging affectionate as well as aggressive impulses.
9. DEPENDENT: a personality disorder with extreme dependence on others, particularly the need to be taken care of, leading to clinging & submissive behavior.INTROJECTION: Is firmly devoted to another, wanting to believe an inseparable bond exist between them; submits any independent views in favor of others to preclude conflicts and threats to the relationship.
12
10. OBSESSIVE COMPULSIVE: A personality disorder with the essential feature of preoccupation with orderliness, perfection & mental & interpersonal control, at the expense of flexibility, openness & efficiency that begins by early adulthood.
REACTION FORMATION: Repeatedly presents positive thoughts & socially commendable behaviors that are diametrically opposite to the deeper, contrary, and forbidden feelings within; displays reasonableness and maturity when faced with circumstances that evoke anger or dismay in others.
11. PASSIVE AGGRESSIVE ( NEGATIVISTIC ): provisional category of personality disorder characterized by a pattern of passive resistance to demands in social or work situations, which may take such forms as simple resistance to fulfilling routine tasks, being submission.
ISOLATION: Can be cold blooded & remarkably detached from the impact of one’s destructive acts; views objects of violation impersonally, as symbols of devalued groups devoid of human sensibilities.
Strained faceRESPIRATORY generalized weaknessRapid breathing wobbly legsShortness of breath clumsy movementPressure on chestShallow breathing URINARY TRACTLump in throat pressure to urinateChoking sensation frequent urinationGasping
GASTROINTESTINAL SKINLoss of appetite flushed faceRevulsion toward food localized sweatingAbdominal discomfort itchingAbdominal pain hot and cold spellsNausea pale faceHeartburn generalized sweatingDiarrhea
13
BEHAVIORLRestlessnessTremorsStartle reactionRapid speech Blocking of thoughtInterpersonal withdrawalInhibitionFlightAvoidanceHyper ventilationAccident proneness
COGNITIVE AFFECTIVE Impaired attention ImpatienceForgetfulness uneasiness Errors in judgment tension Preoccupation nervousness Blocking of thoughts fear Decreased perceptional fright
Field frustrationReduced creativity helplessnessDiminished production alarmConfusion terrorSelf consciousness jitterinessLoss of objectivity jumpinessFear of losing control numbingFrightening visual images guilt Flash back shame Nightmare frustration Injury or death helplessness
NURSING STRATEGIES TO REDUCE PATIENTS ANXIEY Active listening to show acceptance Honesty, answering all questions at the client’s level of understanding. Clearly explaining procedures, surgery & policies & giving appropriate reassurance
based on data. Acting in calm, unhurried manner Speaking clearly, firmly (but not loudly) Giving information about laboratory test, medication, treatments, and rationale for
restrictions on activity. Setting reasonable limits & providing structure Encouraging patients to explore reasons for the anxiety. Encouraging self affirmation through positive statements such as “I will” “I can”
14
Using play therapy with dolls, puppets, games, drawing for young patients. Using touch, giving warm baths, back rubs Initiating recreational activities such as physical exercise, music, card games, board
games, crafts, readings.
NURSE’S ROLE IN HELPING THE PATIENT TO HANDLE ANXIETY1) Help the patient to recognize his anxiety- In order to do this the nurse should be
observant & should be able to identify the behavior that indicates that the patient is anxious. The patient may show increased psychomotor activity such as agitation, pacing & restlessness.Other behaviors that may be seen are anger or withdrawal demanding, tearfulness or complaining of aches & pains. Each individual may differ in the way he behaves in an anxiety attack.
2) Help the patient to gain insight into his anxiety- the patient himself is unable to do
this at that time but the nurse can help him to examine his feelings & thoughts & any particular incident in the environment or in his life that immediately help him to recognize his own patterns of the behaviors by helping him to observe, describe & analyze the connection between what led to his anxiety& what happened after the attack. Thus he can be helped to understand & verbalize the cause.
3) Help the patient to cope with threat behind his anxiety- once he is able to verbalize that cause of anxiety he will be able to recognize similar situations & formulate the usual incidents or situations that make him anxious. Thus he may be helped to have a realistic feeling about various life situations.
4) Help the patient to develop better coping mechanisms- the nurse should help the patient to identify & label the coping & defense mechanisms & discourage its unhealthy use.
BIBLIOGRAPHY1. Townsend C. Mary “psychiatric mental health nursing” Edition 4th p no. 18 – 22, 34- 362. Boynd Ann Mary “psychiatric nursing” 2nd edition p no. 70-733. Fortinash M. Katherine “psychiatric mental health nursing” Edition 3rd p no. 9-114. Morgan t. Clifford etal “introduction to psychology”
Edition 7th p no. 588-591 5. Stuart W. Gali “Psychiatric Nursing” Edition 7th
P. No. 278, 758-762 6. Varcorolis M. Elizabeth “Foundation of Mental Health Nursing” Edition 2nd P. No. 14