11.5.18 1 Inpatient Delirium Management: A Quality Improvement Project for Hospitalized Veterans November 5, 2018 IIndiana Nursing Summit Veteran Health Indiana At the conclusion of this presentation, participants will be able to: ‣ Identify impact of delirium on hospitalized patients. ‣ Discuss screening for delirium ‣ Identify treatment modalities for acute care. ‣ Discuss impact of delirium management. Increased calls (Rapid Response and Code Orange) r/t delirium on Med-Surg units (7N & 7S) Providers met to discuss interventions and medical management Delirium Team convened There is no consistent process for proactively identifying and addressing delirium in the Medical-Surgical areas. Led by Evidence-Based Practice (EBP) APNs Anna Bober Rebecca Parks Earlie Hale Sara Clay Alex Radovanovich Shelly Keiser Candace Whittler-Ducre Tamra Pierce Jo Lee Coleman Dr. Cathy Schubert Jason McClara Dr. Eric Boss Heather Nixon Dr. Maria Poor Celine Alba-Patino
Providers had ordered PRN medication but very few doses were ever administered (despite the fact that most of the doses were charted as “effective” when given)
Medications were potentially underutilized in some patients that were severely agitated.
*Haldol IV Push not approved for use on medical surgical units at the time
19 out of 25 incidents involved physical and verbally disruptive behavior
Area # of Incidents
7 North 10
7 South 10
8 North 2
8 South 1
ED 1
Other 1
11.5.18
4
Lack of protocol
Inconsistent
follow-up
Communication
Inconsistent
nursing care
interventions
Inconsistent
medical
management by
Providers
Gaps Action Purpose/Outcome
Development of a protocol to standardize the process (screening and order set)
Standardize identification of patients with delirium and management of symptoms
Vet trial plan to Nursing Documentation, Acute Care, Nurse Executive and Clinical Practice Committees
Approval and additional feedback from all disciplines
Provider, Pharmacy and Nursing Staff education about the trial
Consistent information provided to promote successful trial
Trial the process on 7N & 7S Test and identify additional improvements on the protocol before full implementation
Request report that shows patients with positive screen
Efficient way to track patients for “just in time” review during trial
Delirium Screening and Order Set
• Literature review
• Query to other VA hospitals and local area hospitals
• Review of MICU Delirium Protocol
• Development of Medical-Surgical Delirium Protocol
Mirror MICU except Haldol PO or IM instead of IV
• Obtaining permission from the author to use Short CAM
(Confusion Assessment Method) screening tool
• Development of the Short CAM into a CPRS template note
(Delirium Screening Note)
Face-to-face training (2 weeks) CPRS documentation of nursing screening and assessment
Order set
Nurses were slotted into 30-minute scheduled blocks with nurse manager input
Pre and post-test administered 6-item questionnaire
Assess knowledge of common signs & symptoms of delirium, risk factors, interventions, and nurse comfort level related to assessing patients for delirium
11.5.18
5
Delirium Protocol Trial Education
Delirium Protocol trial on 7N & 7S is from April 11-May 11, 2017.
Background: Increased calls (code oranges, rapid response calls) related to patients experiencing delirium on medical surgical units.
Goal: Early identification of delirium and implementation of interventions. “An ounce of prevention is worth a pound of cure.”
Protocol includes Order Set, screening for delirium, and appropriate interventions
Order Set:
Built in CPRS – very similar to MICU order set pathway: Same medications, different route.
Differences: 1) Order for Inpatient Geriatric Consult for (Age 65 or Older) link included on menu, 2) Different routes (PO or IM). IV Haldol for
MICU/SICU only 3) note to contact pharmacy for medication review
Screening: Nurses will use the Short CAM to screen patients for delirium
RN will screen patient on admission and every shift and as needed when there is a change in pt. mental status using the Delirium Screening Note
Provider will be notified of 1st positive screen so that the Delirium Order Set can be ordered. Changes in status will be reported to provider.
Nursing staff will implement appropriate interventions to manage symptoms
1
2
PO OR IM
Haloperidol
3
RN will screen patient on admission and every shift and as needed when there is a change in mental status using the Delirium screening Note.
Provider will be notified of a positive screen so that the Delirium Order Set can be initiated.
Nursing staff will implement appropriate interventions to manage symptoms.
Delirium Screening: Types: ICUs use ICU CAM in Essentris while Med-Surg use the Short CAM in CPRS Who completes and when: by RN on admission and every shift and as needed when there is a change in
pt. mental status. Location of note: Essentris, Nursing Admission, Nursing 24 Hour Flow Sheet & stand alone note. Includes documentation of patient behaviors
11.5.18
6
In CPRS, use the care plan titled, Cognitive Function Altered for any disease or condition with
altered cognitive function (e.g. delirium, dementia, TBI, electrolyte imbalance, etc.)
Care Plan Documentation
Definition of Delirium
Types of Delirium
Possible Causes of Delirium
Negative Impact of Delirium
Importance of Recognizing Delirium
Managing Behavioral and Psychological Symptoms and Communication Techniques
‣ Focus on:
Awareness of risk factors for delirium (alcohol withdrawal, pain, post-procedure, delirium superimposed on dementia, etc.)
Considering restraint alternatives prior to restraints
Least restrictive restraint
Encouraging consults (Geriatric, Pharmacy review of medications, etc.)
Importance of reassessment
Questionnaires completed from
7/24/17 -8/3/17
Multiple Choice and Tor F questions:◦ Pre-test average score (N=46) was 72%
◦ Post-test average score (N=46) was 82%
11.5.18
7
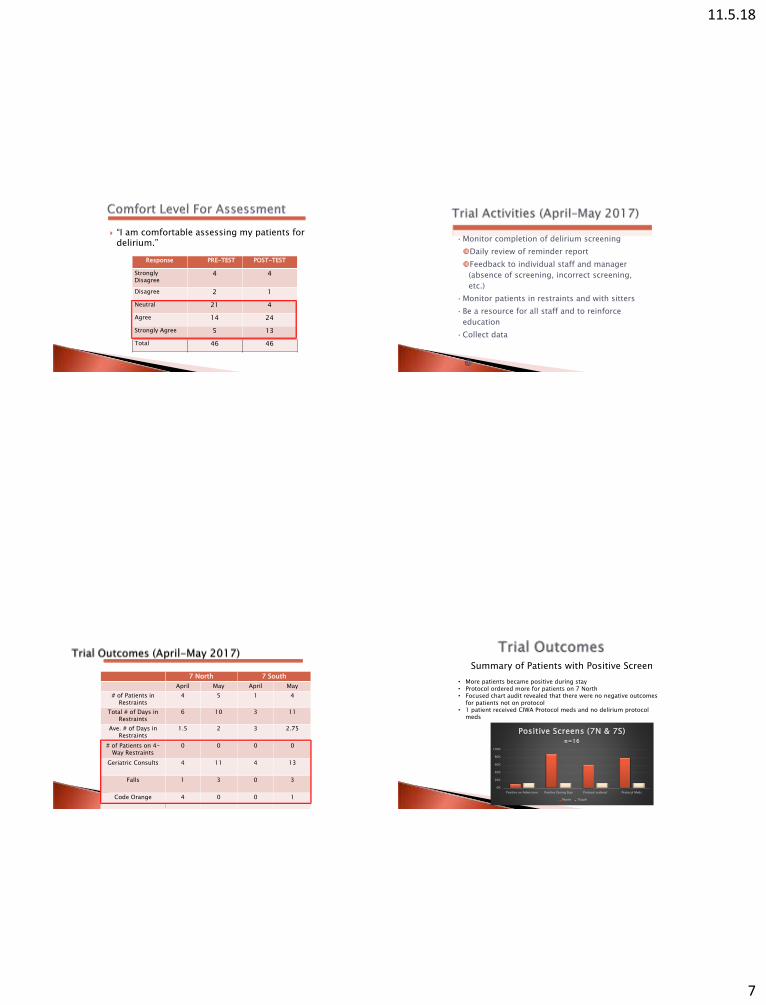
“I am comfortable assessing my patients for delirium.”
Response PRE-TEST POST-TEST
Strongly Disagree
4 4
Disagree 2 1
Neutral 21 4
Agree 14 24
Strongly Agree 5 13
Total 46 46
•Monitor completion of delirium screening
Daily review of reminder report
Feedback to individual staff and manager
(absence of screening, incorrect screening,
etc.)
•Monitor patients in restraints and with sitters
•Be a resource for all staff and to reinforce
education
•Collect data
7 North 7 South
April May April May
# of Patients in Restraints
4 5 1 4
Total # of Days in Restraints
6 10 3 11
Ave. # of Days in Restraints
1.5 2 3 2.75
# of Patients on 4-Way Restraints
0 0 0 0
Geriatric Consults 4 11 4 13
Falls 1 3 0 3
Code Orange 4 0 0 1
0%
20%
40%
60%
80%
100%
Positive on Admission Positive During Stay Protocol ordered Protocol Meds
Positive Screens (7N & 7S)n=16
7North 7South
• More patients became positive during stay• Protocol ordered more for patients on 7 North• Focused chart audit revealed that there were no negative outcomes
for patients not on protocol • 1 patient received CIWA Protocol meds and no delirium protocol
meds
Summary of Patients with Positive Screen
11.5.18
8
‣ Medication Use During Trial
Medications ordered for all patients who screened positive
except 1 patient.
Quetiapine and Trazadone ordered most often.
Haldol 1 time only doses noted.
1 patient did not receive scheduled medications. Pt. escalated
and code orange called. Restraints for short period of time
‣ Barriers that were addressed: Providers (Moonlighters) not aware of the protocol, some
reluctant to order protocol
Protocol not ordered with positive screen
Pts. Transferred with ICU Delirium Protocol – delay in order
reconciliation
Delay in re-screening patients with a change in patient condition
Inconsistent completion of the screening.
‣ Positive Outcomes Nurses empowered to advocate for patients
Increased effective communication with providers
Increased use in restraint alternatives and fall prevention interventions.
Delirium care education elevated the practice level of the nurses