Delta Dental of Kentucky Individual and Family Plans Nobody has a smile like yours, and nobody keeps it healthy like us. Your smile creates a lasting impression on everyone you meet. Delta Dental of Kentucky is here to protect your smile and overall health. Individual and Family Plan Options Happy Smiles • Perfect Smiles • Bright Smiles Individual and Family Plan Features • No enrollment fees, waiting periods, or age restrictions • Benefits increase after first year • Annual maximums increase after first year • Delta Dental Mobile App comes with cost estimators and appointment scheduling features • Three plan options • Easy online enrollment
Transcript
Delta Dental of KentuckyIndividual and Family Plans
Nobody has a smile like yours, and nobody keeps it healthy like us.
Your smile creates a lasting impression on everyone you meet. Delta Dental of Kentucky is here to protect your smile and overall health.
Individual and Family Plan OptionsHappy Smiles • Perfect Smiles • Bright Smiles
Individual and Family Plan Features• No enrollment fees, waiting periods,
or age restrictions• Benefits increase after first year• Annual maximums increase after
first year
• Delta Dental Mobile App comes with cost estimators and appointment scheduling features
• Three plan options• Easy online enrollment
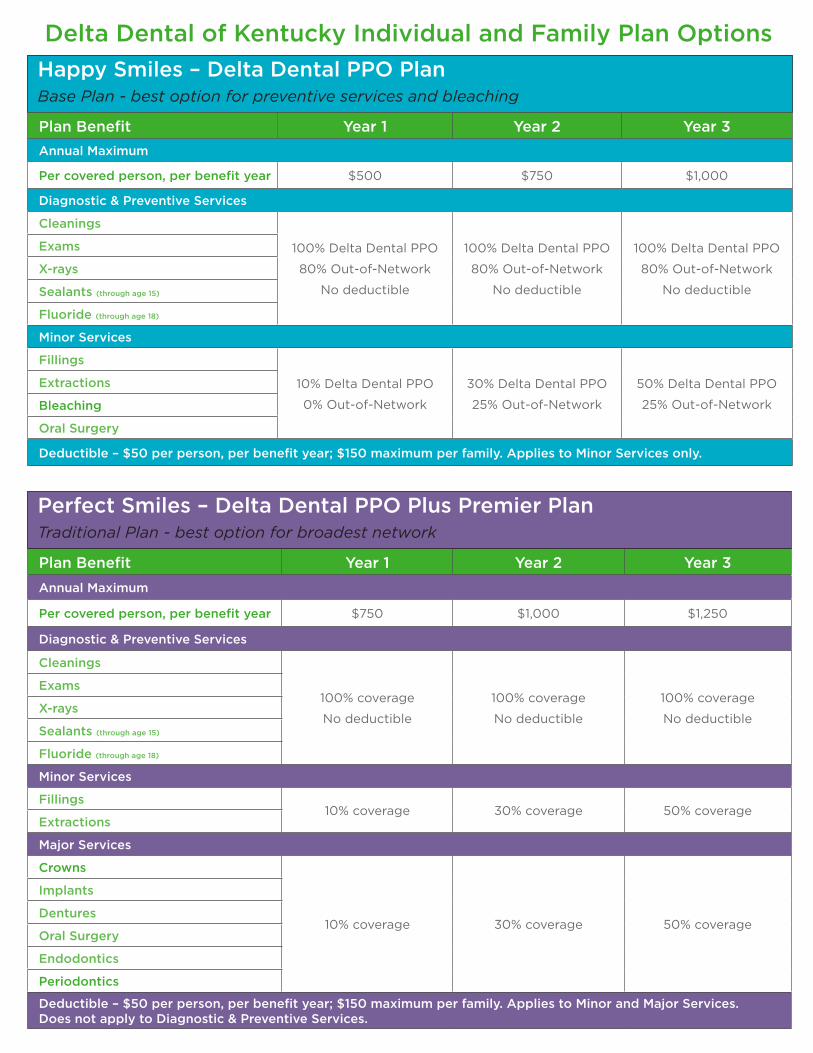
Delta Dental of Kentucky Individual and Family Plan Options
Plan Benefit Year 1 Year 2 Year 3Annual Maximum
Per covered person, per benefit year $500 $750 $1,000
Diagnostic & Preventive Services
Cleanings
100% Delta Dental PPO
80% Out-of-Network
No deductible
100% Delta Dental PPO
80% Out-of-Network
No deductible
100% Delta Dental PPO
80% Out-of-Network
No deductible
Exams
X-rays
Sealants (through age 15)
Fluoride (through age 18)
Minor Services
Fillings
10% Delta Dental PPO
0% Out-of-Network
30% Delta Dental PPO
25% Out-of-Network
50% Delta Dental PPO
25% Out-of-Network
Extractions
Bleaching
Oral Surgery
Deductible – $50 per person, per benefit year; $150 maximum per family. Applies to Minor Services only.
Plan Benefit Year 1 Year 2 Year 3Annual Maximum
Per covered person, per benefit year $750 $1,000 $1,250
Diagnostic & Preventive Services
Cleanings
100% coverage
No deductible
100% coverage
No deductible
100% coverage
No deductible
Exams
X-rays
Sealants (through age 15)
Fluoride (through age 18)
Minor Services
Fillings10% coverage 30% coverage 50% coverage
Extractions
Major Services
Crowns
10% coverage 30% coverage 50% coverage
Implants
Dentures
Oral Surgery
Endodontics
Periodontics
Deductible – $50 per person, per benefit year; $150 maximum per family. Applies to Minor and Major Services. Does not apply to Diagnostic & Preventive Services.
Happy Smiles – Delta Dental PPO PlanBase Plan - best option for preventive services and bleaching
Perfect Smiles – Delta Dental PPO Plus Premier PlanTraditional Plan - best option for broadest network
Monthly Rates for effective dates through 12/2018Happy Smiles
Subscriber only: $17.69Subscriber plus one: $32.12
Family: $48.74
Perfect SmilesSubscriber only: $27.15
Subscriber plus one: $50.60Family: $79.10
Bright SmilesSubscriber only: $33.64
Subscriber plus one: $63.71Family: $109.03
Happy Smiles, Perfect Smiles, and Bright Smiles plans are available to all Kentucky residents.
Plan Benefit Year 1 Year 2 Year 3 Year 4Annual Maximum
Per covered person, per benefit year $500 $1,000 $1,250 $1,500
Diagnostic & Preventive Services
Cleanings
100% Delta Dental PPO
80% Out-of-Network
No deductible
100% Delta Dental PPO
80% Out-of-Network
No deductible
Exams
X-rays
Sealants (through age 15)
Fluoride (through age 18)
Minor Services
Fillings 50% Delta Dental PPO
40% Out-of-Network
80% Delta Dental PPO
60% Out-of-NetworkExtractions
Major Services
Bleaching
25% Delta Dental PPO
10% Out-of-Network
50% Delta Dental PPO
40% Out-of-Network
Crowns
Veneers
Implants
Dentures
Oral Surgery
Endodontics
Periodontics
Orthodontics
Orthodontic Services available to all covered persons. No maximum age. Not covered in Year 1
50% Delta Dental PPO and Out-of-Network
$1,000 Lifetime Maximum
Deductible – $50 per person, per benefit year; $150 maximum per family. Applies to Minor, Major and Orthodontic Services. Does not apply to Diagnostic & Preventive Services.
Bright Smiles – Delta Dental PPO PlanEnhanced Plan - best option for braces and veneers
Delta Dental of Kentucky Individual and Family Plan Options
Enroll your smile today by contacting:AgentLink
1-800-960-1371www.agent-link.net
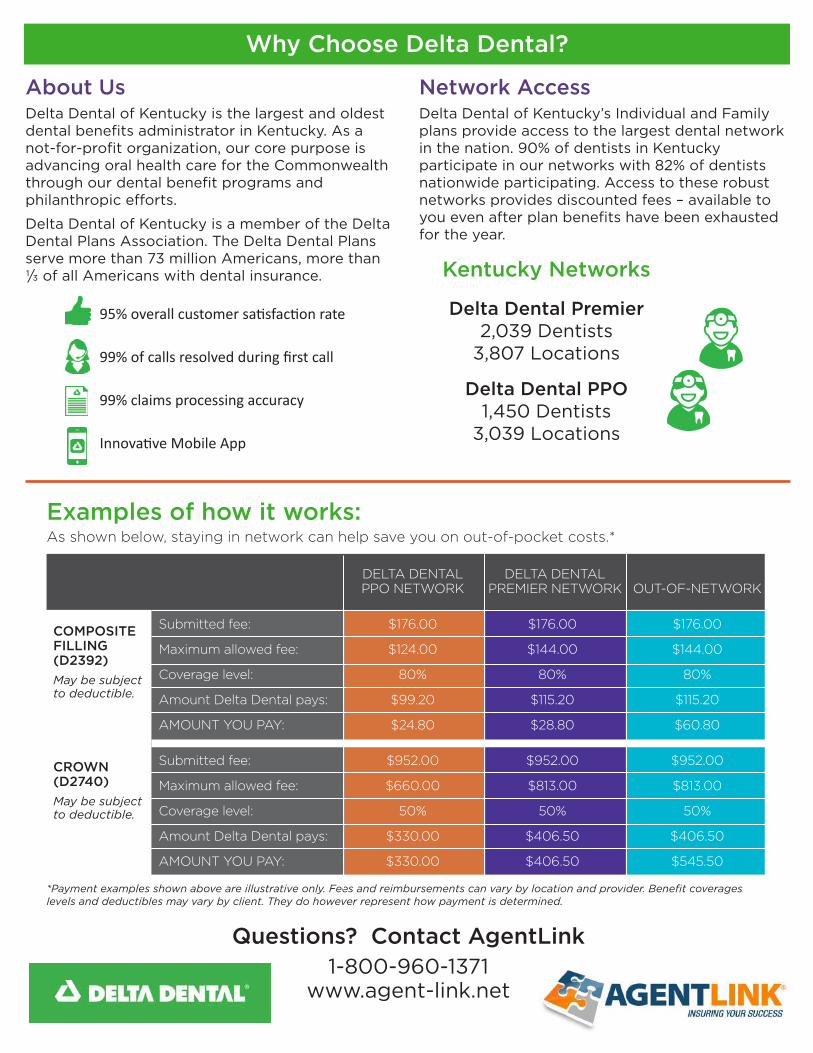
Kentucky Networks
Delta Dental Premier2,039 Dentists
3,807 Locations
Delta Dental PPO1,450 Dentists
3,039 Locations
Questions? Contact AgentLink1-800-960-1371
www.agent-link.net
Why Choose Delta Dental?
About UsDelta Dental of Kentucky is the largest and oldest dental benefits administrator in Kentucky. As a not-for-profit organization, our core purpose is advancing oral health care for the Commonwealth through our dental benefit programs and philanthropic efforts.
Delta Dental of Kentucky is a member of the Delta Dental Plans Association. The Delta Dental Plans serve more than 73 million Americans, more than 1/3 of all Americans with dental insurance.
Network AccessDelta Dental of Kentucky’s Individual and Family plans provide access to the largest dental network in the nation. 90% of dentists in Kentucky participate in our networks with 82% of dentists nationwide participating. Access to these robust networks provides discounted fees – available to you even after plan benefits have been exhausted for the year.
95% overall customer satisfaction rate
99% of calls resolved during first call
99% claims processing accuracy
Innovative Mobile App
*Payment examples shown above are illustrative only. Fees and reimbursements can vary by location and provider. Benefit coverages levels and deductibles may vary by client. They do however represent how payment is determined.
Examples of how it works:As shown below, staying in network can help save you on out-of-pocket costs.*
DELTA DENTAL DELTA DENTAL PPO NETWORK PREMIER NETWORK OUT-OF-NETWORK
Submitted fee: $176.00 $176.00 $176.00
Maximum allowed fee: $124.00 $144.00 $144.00
Coverage level: 80% 80% 80%
Amount Delta Dental pays: $99.20 $115.20 $115.20
AMOUNT YOU PAY: $24.80 $28.80 $60.80
Submitted fee: $952.00 $952.00 $952.00
Maximum allowed fee: $660.00 $813.00 $813.00
Coverage level: 50% 50% 50%
Amount Delta Dental pays: $330.00 $406.50 $406.50
AMOUNT YOU PAY: $330.00 $406.50 $545.50
COMPOSITEFILLING(D2392)May be subject to deductible.
CROWN(D2740)May be subject to deductible.
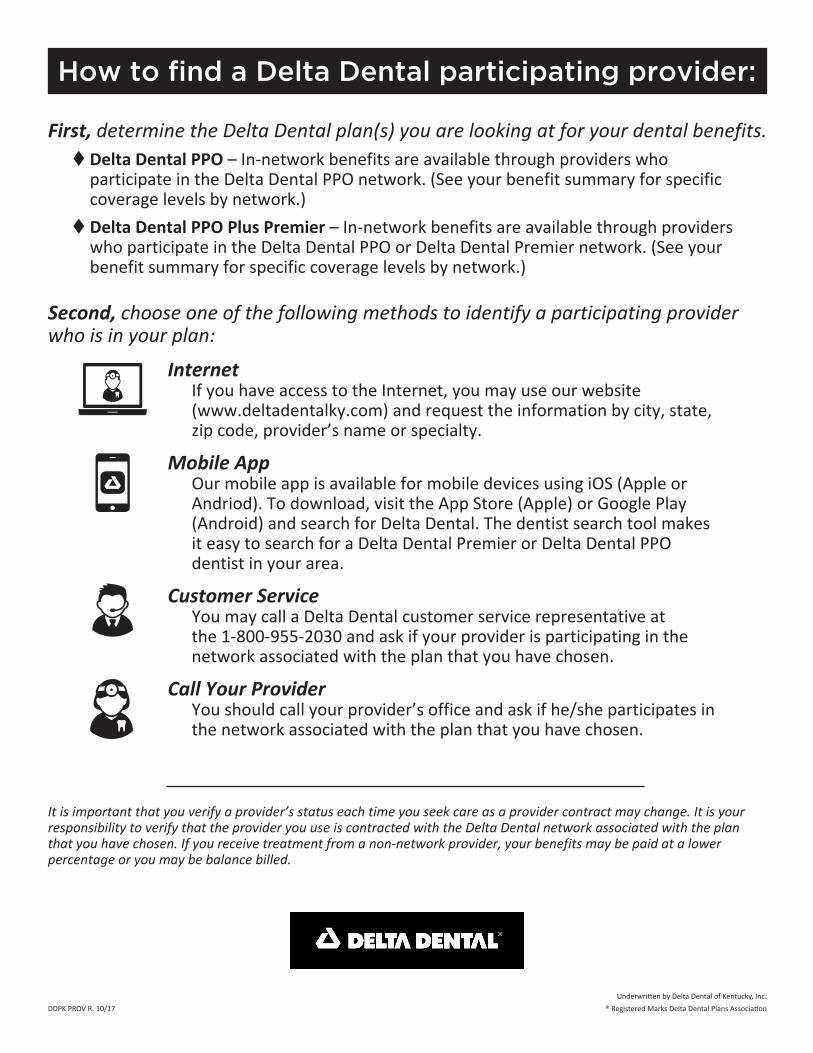
How to find a Delta Dental participating provider:
First, determine the Delta Dental plan(s) you are looking at for your dental benefits. t Delta Dental PPO – In-network benefits are available through providers who
participate in the Delta Dental PPO network. (See your benefit summary for specific coverage levels by network.)
t Delta Dental PPO Plus Premier – In-network benefits are available through providers who participate in the Delta Dental PPO or Delta Dental Premier network. (See your benefit summary for specific coverage levels by network.)
Second, choose one of the following methods to identify a participating provider who is in your plan:
Internet If you have access to the Internet, you may use our website (www.deltadentalky.com) and request the information by city, state,
zip code, provider’s name or specialty.
Mobile App Our mobile app is available for mobile devices using iOS (Apple or
Andriod). To download, visit the App Store (Apple) or Google Play (Android) and search for Delta Dental. The dentist search tool makes it easy to search for a Delta Dental Premier or Delta Dental PPO dentist in your area.
Customer Service You may call a Delta Dental customer service representative at
the 1-800-955-2030 and ask if your provider is participating in the network associated with the plan that you have chosen.
Call Your Provider You should call your provider’s office and ask if he/she participates in
the network associated with the plan that you have chosen.
It is important that you verify a provider’s status each time you seek care as a provider contract may change. It is your responsibility to verify that the provider you use is contracted with the Delta Dental network associated with the plan that you have chosen. If you receive treatment from a non-network provider, your benefits may be paid at a lower percentage or you may be balance billed.
DDPK PROV R. 10/17 ® Registered Marks Delta Dental Plans AssociationUnderwritten by Delta Dental of Kentucky, Inc.
Delta Dental of KentuckyIndividual and Family Plans
Questions? Call us at 1-800-960-1371www.agent-link.net
Frequently Asked Questions
Dental Benefits are offered by Delta Dental of Kentucky, Inc.*Registered Mark of Delta Dental Plans Association, Inc.
If I have current dental coverage, can I move up to the fully mature benefits?Yes, if you or your dependents have current dental coverage that has been in force a minimum of 12 months, we will move you to the fully mature benefits. You will need to provide evidence of this coverage (a certificate of credible coverage from your prior carrier) to Delta Dental of Kentucky.
I have had prior dental coverage for 12 months, but my dependent has not, do we both get to move to the fully mature benefit level? No, each enrollee is treated separately. So you (the subscriber) would be placed in the fully mature benefits while your dependent (who did not have 12 months of prior coverage) will start with year one benefits.
Will I be able to cancel the dental plan after I have enrolled?No, unless there is a qualifying event (proof required). These policies are 12 month contracts that will renew annually upon your benefit anniversary date. If you choose to cancel coverage upon the expiration of your policy, you must provide a written notice of termination 30 days prior to the anniversary date.
What should I expect to see on my Bank/Credit Card Statement for my premium payments?8888593795 Insurance will appear on your statement as the charge for your premiums.
When will my first payment be taken? Your first month’s premium is due at time of enrollment. Banking/Saving account – Please allow up to 3 business days. Credit/Debit Card - Will be taken immediately.
What is the deadline for enrollments?Applications submitted by the 20th of the month can become effective on the 1st of the following month. Any applications received after the 20th can become effective on the 1st of the second month.
What are my options for selecting an Effective Date?Plan effective dates are always the 1st of the month. Incomplete enrollment or failure to submit the required initial premium amount may cause an initial delay in issuance of insurance. We advise you not to cancel any other insurance or assume you are insured under this insurance policy until you receive your confirmation of coverage.
When will I receive my enrollment package and what will it include?You will receive your enrollment package upon completion of enrollment and payment of applicable premiums, or a few days prior to the effective date. The enrollment package will include your welcome letter and ID cards.
What if I need to make changes to my coverage (example: add or remove a dependent/spouse)?You can call Morgan-White at 1-877-877-1497. This plan is a 12-month contract and you will be unable to make any changes until the next open enrollment.
Who is eligible for coverage under this plan?Coverage is offered to all ages. The primary subscriber may also cover dependents (spouse or domestic partner and unmarried children from birth to the end of the benefit year in which they turn age 26).
Will I receive a renewal notice? Once enrolled, the plan will continue to automatically renew unless you send a cancellation notice. All cancellations require a 30 day notice via email to [email protected] or by fax to 601-956-3795. If there is a premium change, you will receive a notice 60 days prior to your anniversary date.
Do I need to obtain claim forms?One of the advantages of visiting Delta Dental network dentists is that they will file all claims on your behalf. If services are provided by an out-of-network dentist, you may be required to file a claim yourself.
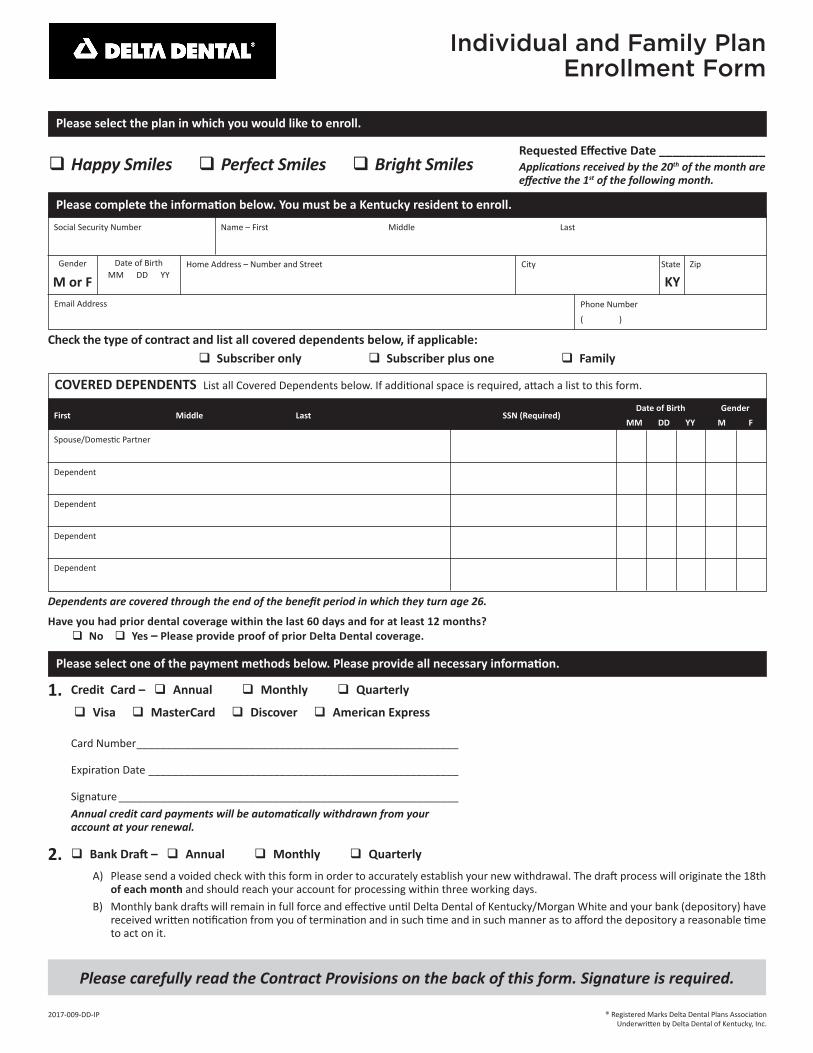
Individual and Family PlanEnrollment Form
Card Number ______________________________________________________
Expiration Date ____________________________________________________
Signature _________________________________________________________Annual credit card payments will be automatically withdrawn from your account at your renewal.
Credit Card – q Annual q Monthly q Quarterly
q Visa q MasterCard q Discover q American Express
Please select one of the payment methods below. Please provide all necessary information.
2017-009-DD-IP
Dependents are covered through the end of the benefit period in which they turn age 26.
Please carefully read the Contract Provisions on the back of this form. Signature is required.
A) Please send a voided check with this form in order to accurately establish your new withdrawal. The draft process will originate the 18th of each month and should reach your account for processing within three working days.
B) Monthly bank drafts will remain in full force and effective until Delta Dental of Kentucky/Morgan White and your bank (depository) have received written notification from you of termination and in such time and in such manner as to afford the depository a reasonable time to act on it.
q Bank Draft – q Annual q Monthly q Quarterly
q Happy Smiles q Perfect Smiles q Bright Smiles
Please select the plan in which you would like to enroll.
1.
2.
® Registered Marks Delta Dental Plans AssociationUnderwritten by Delta Dental of Kentucky, Inc.
Have you had prior dental coverage within the last 60 days and for at least 12 months? q No q Yes – Please provide proof of prior Delta Dental coverage.
Requested Effective Date ________________Applications received by the 20th of the month are effective the 1st of the following month.
Check the type of contract and list all covered dependents below, if applicable:q Subscriber only q Subscriber plus one q Family
COVERED DEPENDENTS List all Covered Dependents below. If additional space is required, attach a list to this form.
First Middle Last SSN (Required)
Spouse/Domestic Partner
Date of BirthMM DD YY
GenderM F
Dependent
Dependent
Dependent
Dependent
Please complete the information below. You must be a Kentucky resident to enroll.
Social Security Number Name – First Middle Last
Phone Number
( )
Home Address – Number and Street City State Zip
KYDate of Birth
MM DD YYGender
M or FEmail Address
Effective Date Process Date Processed By
SHADED AREA BELOW FOR OFFICE USE ONLY
IMPORTANT: If you do not want the contract for any reason, you may return it to us within 10 days after you receive it. Upon return, the contract will be deemed void, and any money you have paid will be refunded.This is an annual contract. If you have elected the annual payment option, you may not terminate this contract prior to the end of the term. If you have elected the monthly payment option and we do not receive your premium within 30 days of the date the premium is due, your contract will be cancelled effective the due date of your premium, whether or not a specific condition was incurred prior to the termination date. Your Covered Dependents will terminate on your termination date. Covered Services are eligible for payment only if your contract is in effect at the time such services are provided.
I acknowledge that I have read the provisions of this enrollment form and I expressly accept such provisions as a condition of coverage. I understand that my membership is for a 12-month period and on my anniversary date I can renew or cancel or change how I pay my premium. I represent the answers given to all questions on this form are true and accurate to the best of my knowledge and I understand they are being relied on by Delta Dental of Kentucky, Inc. in accepting this form. Any material misrepresentation found in this application may result in denial of benefits or cancellation of my coverage(s). Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime. If accepted, this form, the dental contract, and the identification card will constitute the contract.
Applicant Signature_________________________________________________________ Date _____________________________
If Applicant is under the age of 18 at the time of enrollment, a parent or guardian must agree to the above conditions on behalf of Applicant and must agree to assume financial responsibility for Applicant.
Agreed___________________________________________________________________ Date _____________________________
Relationship to Applicant ___________________________________
You can enroll online at www.agent-link.net or by phone at 1-800-960-1371or
You can mail your original application to:AgentLink
2001 Lake Point WayLouisville, KY 40223
Contract Provisions
Please carefully read the Contract Provisions below. Signature required.
Delta Dental of Kentucky reserves the right to assign effective dates.
Agent Name (printed)
FOR AGENT USE ONLY (IF YOU DO NOT HAVE AN AGENT REPRESENTING YOU, PLEASE LEAVE BLANK.)
Agent Email
Agent Signature
Agent Phone Number
Date
Underwritten by Delta Dental of Kentucky, Inc.
DID YOU KNOW?Delta Dental can automatically debit your monthly payment from a checking or savings account.
If you would like to be set up for the automatic debit process, please fill out the form below, attach a copy of your blank voided check and mail it with your enrollment form.
Bank Name: ________________________________________________________________________________
THIS PLAN IS NOT INSURANCE and is not intended to replace health insurance. This plan is not a Qualified Health Plan under the Affordable Care Act. THIS IS NOT A MEDICARE PRESCRIPTION DRUG PLAN. There is no cost to join this discount program. The plan provides discounts at certain health care providers for services. The range of discounts will vary depending on the type of provider and service. Plan members are obligated to pay for all health care services but will receive a discount from those health care providers who have agreed to provide discounts. The plan and its administrators have no liability for providing or guaranteeing service by providers or the quality of service rendered by providers. This plan is not available in Washington. Void where prohibited.
VSP and WellVision Exam are registered trademarks, and Vision Savings Pass is a trademark of Vision Service Plan. Flexon is a registered trademark of Marchon Eyewear, Inc. ®Registered Marks Delta Dental Plans Association. All other brands are trademarks or registered trademarks of their respective owners. JOB#2823-16-VCCM 2/16
Service Reduced prices and savings
Wellvision Exam®• $50 with purchase of a complete pair of prescription glasses. • 20% off without purchase.• Once every calendar year.
Retinal Screening • Guaranteed pricing with Wellvision Exam, not to exceed $39.
LensesWith purchase of a complete pair of prescription glasses:• Single vision $40 • Lined trifocals $75• Lined bifocals $60 • Polycarbonate for children $0
Lens Enhancements • Average savings of 20-25% on lens enhancements such as progressive, scratch-resistant, and anti-reflective coatings.
Frames • 25% savings when a complete pair of prescription glasses is purchased.
Sunglasses • 20% savings on unlimited non-prescription sunglasses from any VSP doctor within 12 months of your last Wellvision Exam.
Contact Lenses • 15% savings on contact lens exam (fitting and evaluation).
Laser Vision Correction • Average 15% off the regular price or 5% off the promotional price; discounts only available from contracted facilities.
VSP Vision Savings Pass is a discount vision program that offers immediate savings on eye care and eyewear. This is not an insurance plan.
See the Savings • Access to discounts through a trusted, private-practice VSP doctor• One rate of $50 for an eye exam1
• Special pricing on complete pairs of glasses and sunglasses• 15% savings on a contact lens exam2
• Unlimited use on materials throughout the year• Exclusive Member Extras, like rebates and special offers
Unlimited Annual Material Use3
Your VSP Vision Savings Pass can be used as often as you like throughout the year. With the best choices in eyewear, we make it easy to find the perfect frame that’s right for you, your family, and your budget. Choose from great brands like Anne Klein, bebe®, Calvin Klein, Flexon®, Lacoste, Nike, Nine West, and more.4
How to Use Your VSP Vision Savings Pass
1. Find a VSP doctor at vsp.com or call 800.877.7195.
2. Save immediately on an eye exam1 and eyewear at the time of service.
3. Take advantage of your VSP Vision Savings Pass over and over—use is unlimited on materials.3
1. This cost is only available with the purchase of a complete pair of prescription glasses; otherwise, you’ll receive 20% off an eye exam only. 2. Applies only to contact lens exam, not materials. You are responsible for 100% of the contact lens material cost.3. Unlimited use is for materials only. An eye exam is limited to once a year per member.4. Brands subject to change.5. Blueocean Market Intelligence National Vision Plan Member Research, 2014.
Hearing aid low price guarantee - if you find the same product at a lower price, bring us the local quote and we’ll not only match it, we’ll beat it by 5%!
Custom hearing solutions - we find the solution that best fits your lifestyle and your budget from one of our 10 manufacturers.
Discount Card● Discounted hearing testing● Low price guarantee● 60-day risk-free trial period● 2 years batteries with purchase
To activate your discount, call 1-877-703-3505 today!
Brought to you by Delta Dental of Kentucky
Continuous Care - one year free follow-up care, two years free batteries, and a three-year warranty.
Accessing your discount is as easy as...
Call Amplifon at 1-877-703-3505 and we’ll find a provider
near you.
We’ll explain the Amplifon process and help you schedule an
appointment.
We’ll send information to you and the provider, ensuring your discount