69
Dementia and Confusion in Older Women OB GYN Grand Rounds 9/15/12 Teresa McCarthy MD,MS [email protected]
Dementia and Confusion in Older Women
OB GYN Grand Rounds 9/15/12
Teresa McCarthy MD,MS [email protected]
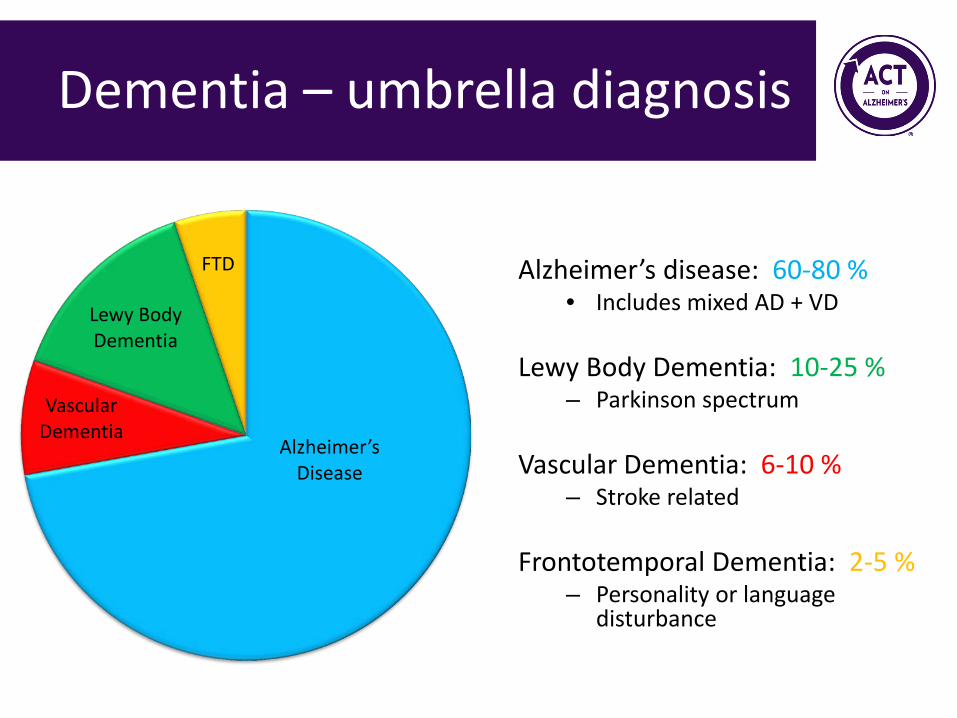
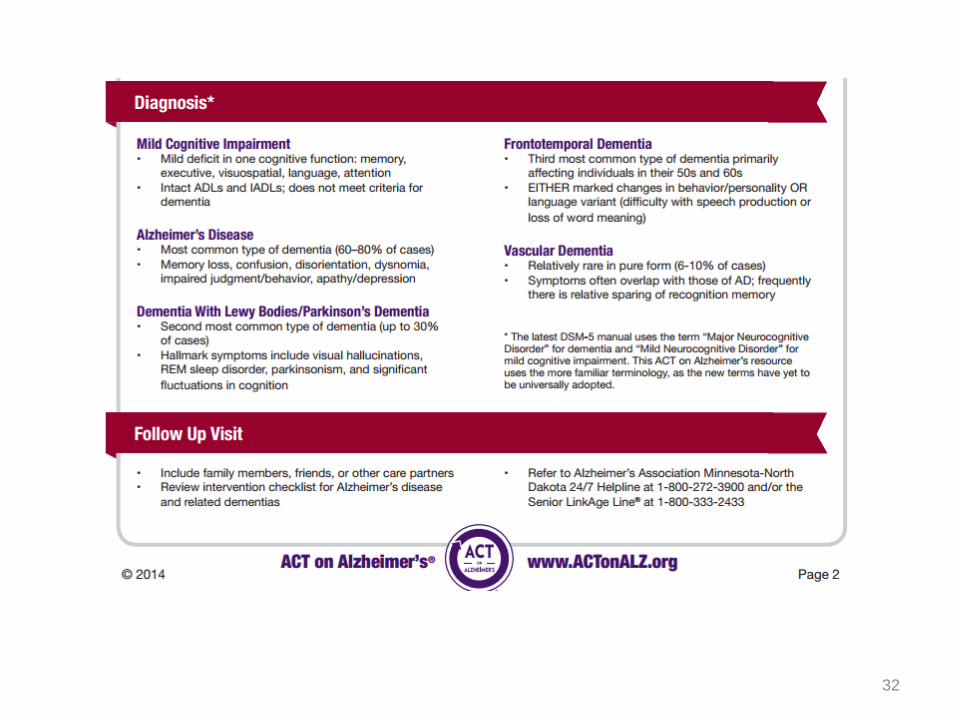
Dementia – umbrella diagnosis
Alzheimer’s Disease
Vascular Dementia
Lewy Body Dementia
FTD
Alzheimer’s disease: 60-80 % • Includes mixed AD + VD
Lewy Body Dementia: 10-25 %
– Parkinson spectrum
Vascular Dementia: 6-10 % – Stroke related
Frontotemporal Dementia: 2-5 %
– Personality or language disturbance
DSM – 5 Dementia = Neurocognitive disorders • Major Cognitive Impairment
– Substantial cognitive decline from previous level of performance based on history
– Formal testing (>2 SD from norm)
• Minor Cognitive Impairment – Modest decline from previous – Formal testing (1-2 SD from norm)
3
Alzheimer’s Disease
• Chronic progressive decline in 2 or more areas of
cognition: – Memory* – Executive function – Ability to recognize objects - agnosia – Motor ability -apraxia – Language – aphasia
• Severe enough to interfere with occupational or social life
4
Alzheimer’s disease
– Deficits are not due to DELRIUM – Deficits are not due to another mental
disorder
5
Alzheimer’s: A Public Health Crisis
• Scope of the problem – 5.3M Americans with AD in 2015 – Growing epidemic expected to impact 13.8M Americans by
2050 and consume 1.1 trillion in healthcare spending – Almost 2/3 are women (longer life expectancy) – If disease could be detected earlier incidence would be
much higher • Pre-clinical stage 1-2 decades
• Some populations at higher risk – Older African Americans (2x as whites) – Older Hispanics (1.5x as whites)
6 Alzheimer’s Association Facts
and Figures 2015

Base Rates
• 1 in 9 people 65+ (11%) • 1 in 3 people 85+ (32%)
7
Alzheimer’s Association Facts and Figures 2014
Challenges & Opportunities
• AD under-recognized by providers – Only 50% of patients receive formal diagnosis
• Millions unaware they have dementia
– Diagnosis often delayed on average by 6+ years after symptom onset
8 Boise et al., 2004; Boustani et al., 2003; Boustani et al., 2005; Silverstein & Maslow, 2006
Introduction to
ACT on Alzheimer’s
What is ACT on Alzheimer’s?
statewide
collaborative
volunteer driven
60+ O R G A N I Z A T I O N S
500+ I N D I V I D U A L S
I M P A C T S O F A L Z H E I M E R ’ S
BUDGETARY SOCIAL PERSONAL

Collaborative Goals/Common Agenda – www.actonalz.org
Five shared goals with a Health Equity perspective
11
ACT Tool Kit
• Evidence and consensus-based, best practice standards for Alzheimer’s care
• Tools and resources for: – Primary care providers – Care coordinators – Community agencies – Patients and families
12

ACT Tools – www.actonalz.org
13
Evaluation of memory concerns
14
Case Study: Colleen
• 66 y/o retired accountant for family business • Presents to primary care with memory complaints • Daughter agrees that short-term memory is poor • Began 2 years ago, seems to be worsening • Frequent medication changes, managing
independently • Lives with husband who is still running the family
business
Signs and Symptoms of AD – should prompt an evaluation/”screen”
• Memory loss • Confusion • Disorientation to time or place • Getting lost in familiar locations • Impairment in speech/language • Trouble with time/sequence relationships • Diminished insight
16 Alzheimer’s Association, 2009
Signs and Symptoms of AD – should prompt an evaluation/”screen
• Poor judgment/problem solving • Changes in sleep and appetite • Mood/personality/behavior changes • Wandering • Deterioration of self care, hygiene • Difficulty performing familiar tasks, functional
decline
17
Practice Tips
• Clinical interview – Let patient answer questions without help – Remember: Social skills remain intact until
late stage dementia • Easy to be fooled by a sense of humor, reliance on old
memories, or quiet/affable demeanor
Practice Tips
• Red flags
– Repetition (not normal in 7-10 min conversation) – Tangential, circumstantial responses – Losing track of conversation – Frequently deferring answers to family member – Over reliance on old information/memories – Inattentive to appearance – Unexplained weight loss or “failure to thrive”
Practice Tips
• Family observations:
– ANY instances of getting lost while driving, trouble following a recipe, asking same questions repeatedly, mistakes paying bills
– Take these concerns seriously: by the time family report problems, symptoms have typically been present for quite a while and are getting worse
Cognitive “Screening”/Assessment
21
Screening Measures
• Wide range of options
– Mini-Cog™ (MC) – Mini-Mental State Exam© (MMSE) – St. Louis University Mental Status Exam™ (SLUMS) – Montreal Cognitive Assessment™ (MoCA)
• All but MMSE free, in public domain, and online
Borson et al., 2000; Folstein et al., 1975; Nasreddine 2005; Tariq et al., 2006
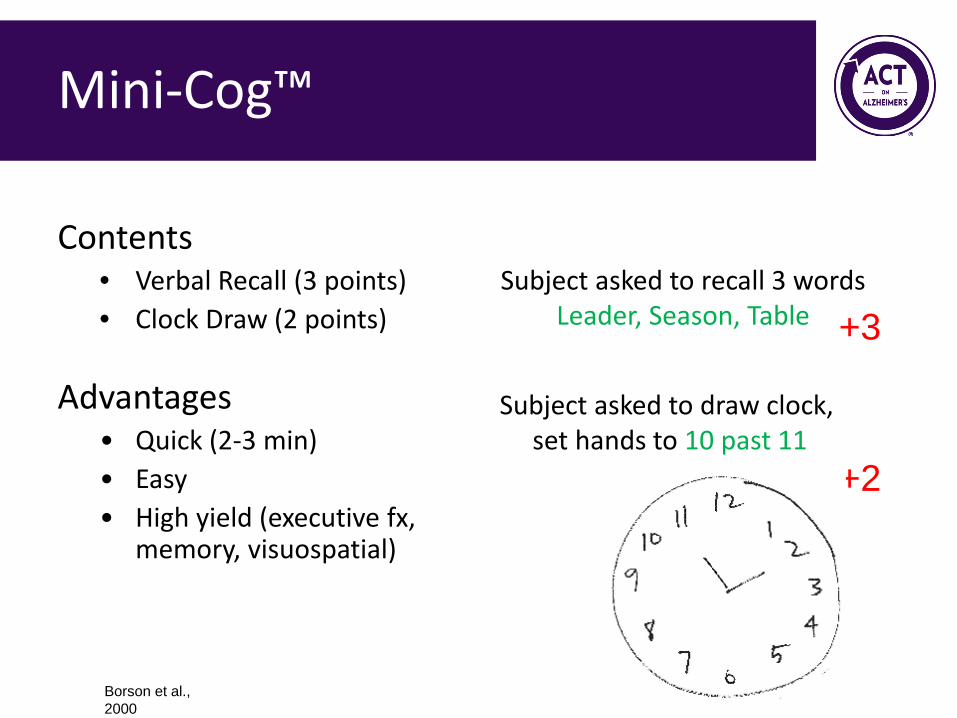
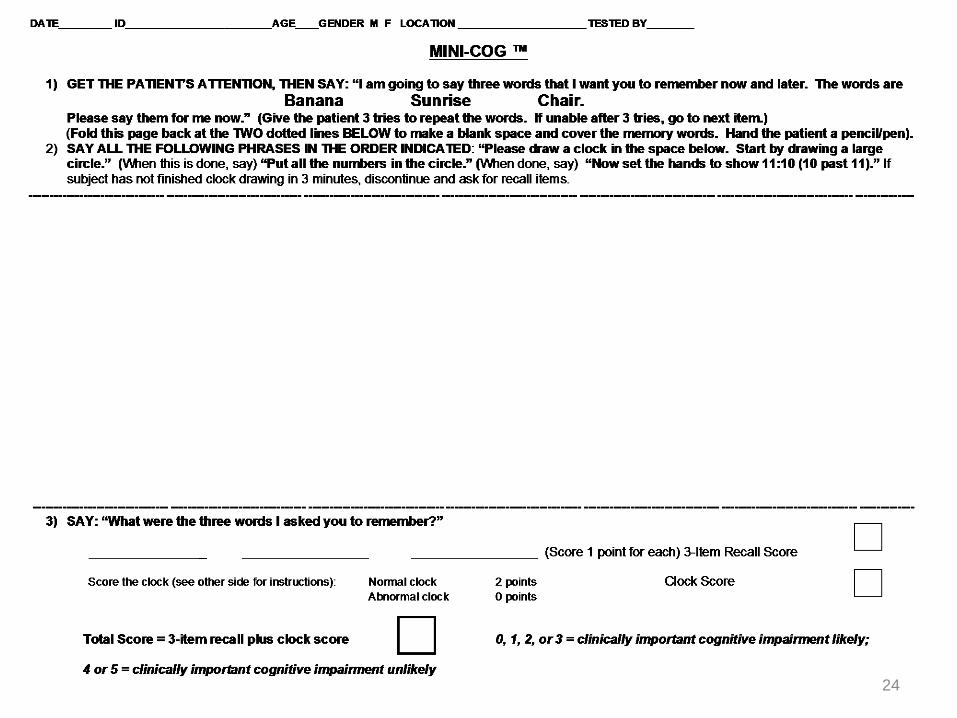
Mini-Cog™
Contents • Verbal Recall (3 points) • Clock Draw (2 points)
Advantages • Quick (2-3 min) • Easy • High yield (executive fx,
memory, visuospatial)
Subject asked to recall 3 words Leader, Season, Table
Subject asked to draw clock, set hands to 10 past 11
+3
+2
Borson et al., 2000
24
Mini-Cog
Pass • > 4
Fail • 3 or less
Borson et al., 2000
Mini-Cog Research
• Performance unaffected by education or language
• Borson Int J Geriatr Psychiatry 2000
• Sensitivity and specificity similar to MMSE (76% vs. 79%; 89% vs. 88%)
• Borson JAGS 2003
• Does not disrupt workflow & increases rate of diagnosis in primary care
• Borson JGIM 2007
• Failure associated with inability to fill pillbox • Anderson et al Am Soc Consult Pharmacists 2008
Mini-Cog: Colleen
27
http://youtu.be/DeCFtuD41WY
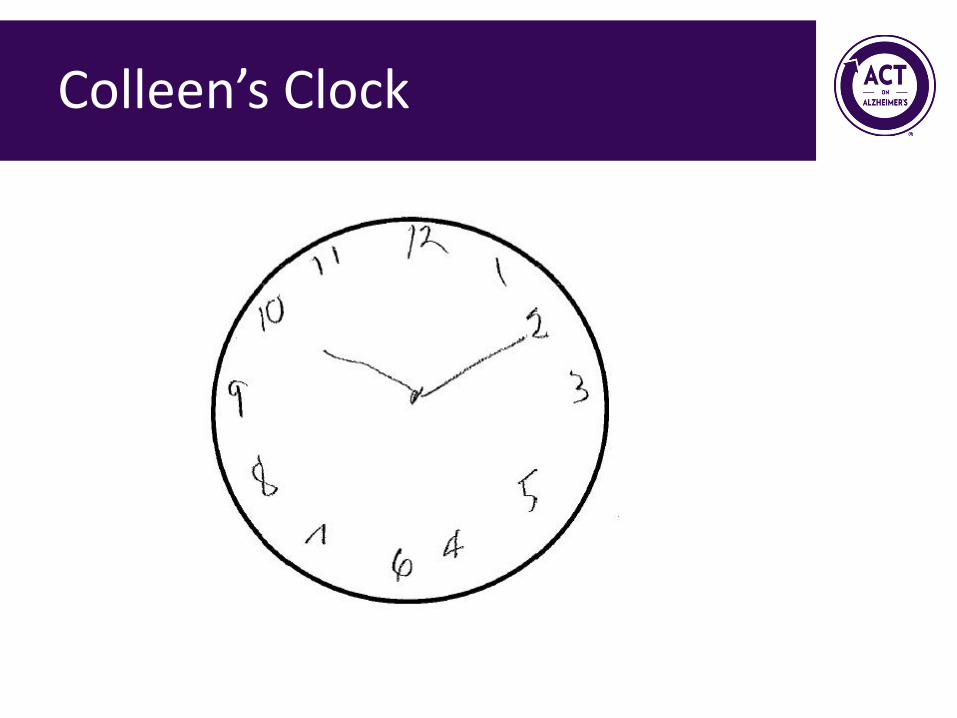
Colleen’s Clock
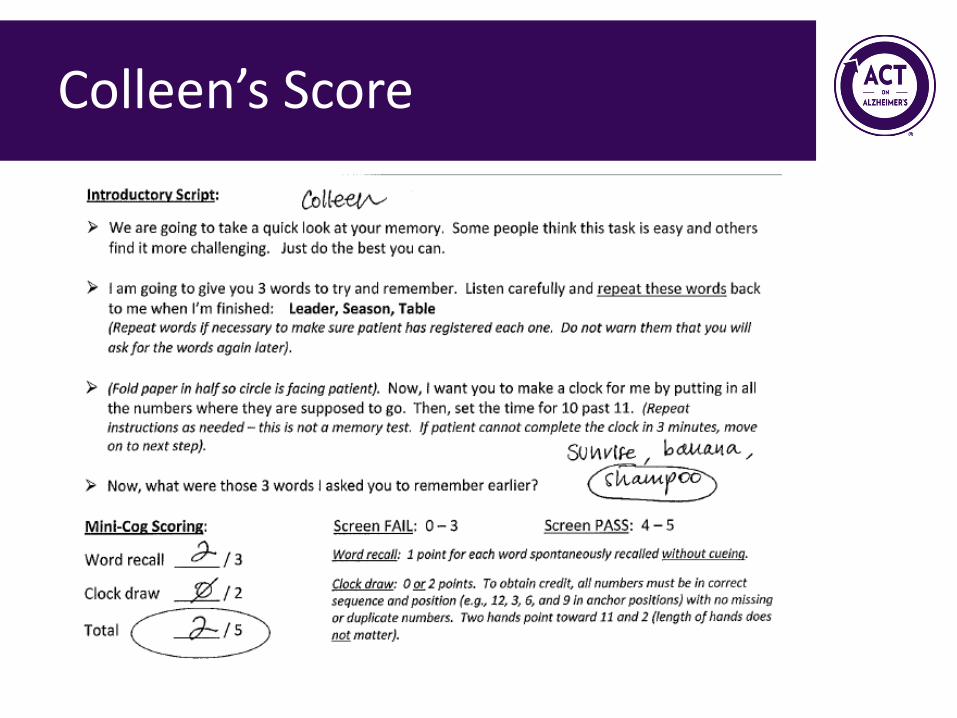
Colleen’s Score
Dementia Work-up and Diagnosis
30
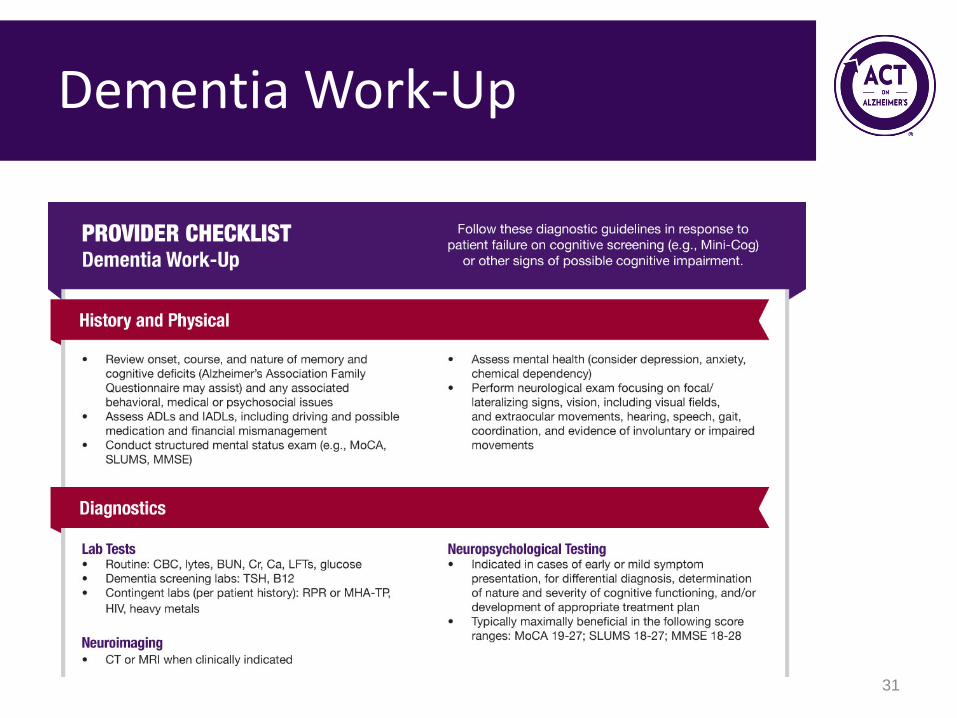
Dementia Work-Up
31
32
Dementia Work-Up
• H&P • Diagnostics
– Labs – Imaging ?
• Objective cognitive measurement – More specific testing (e.g., neuropsychometric)
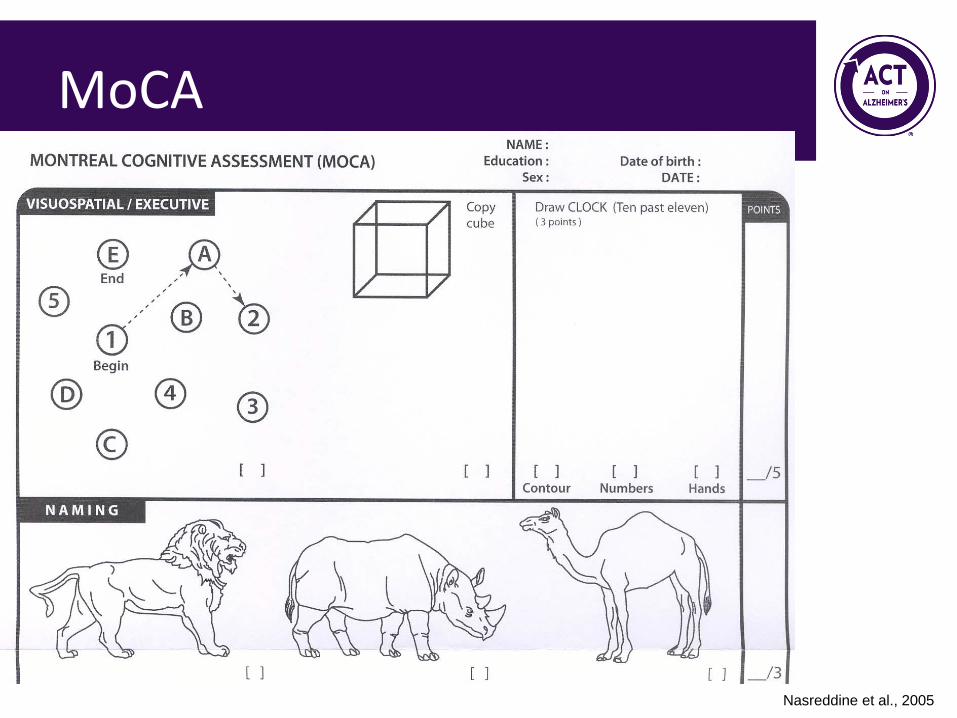
MoCA
Nasreddine et al., 2005
MoCA
Pass • > 26
Fail • 25 or less
35 Nasreddine 2005
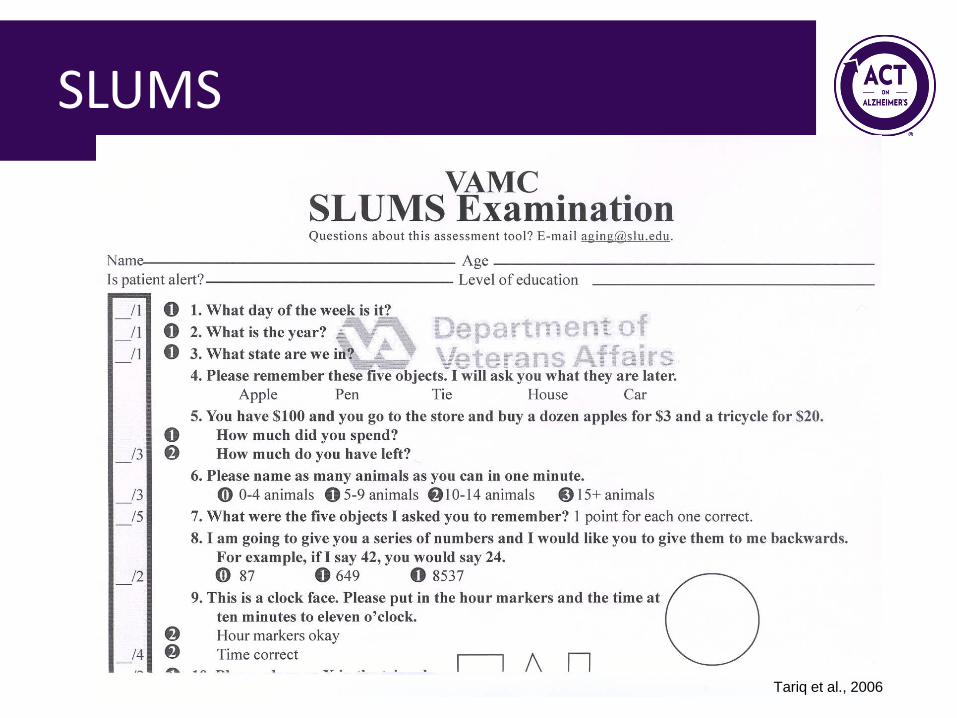
SLUMS
Tariq et al., 2006
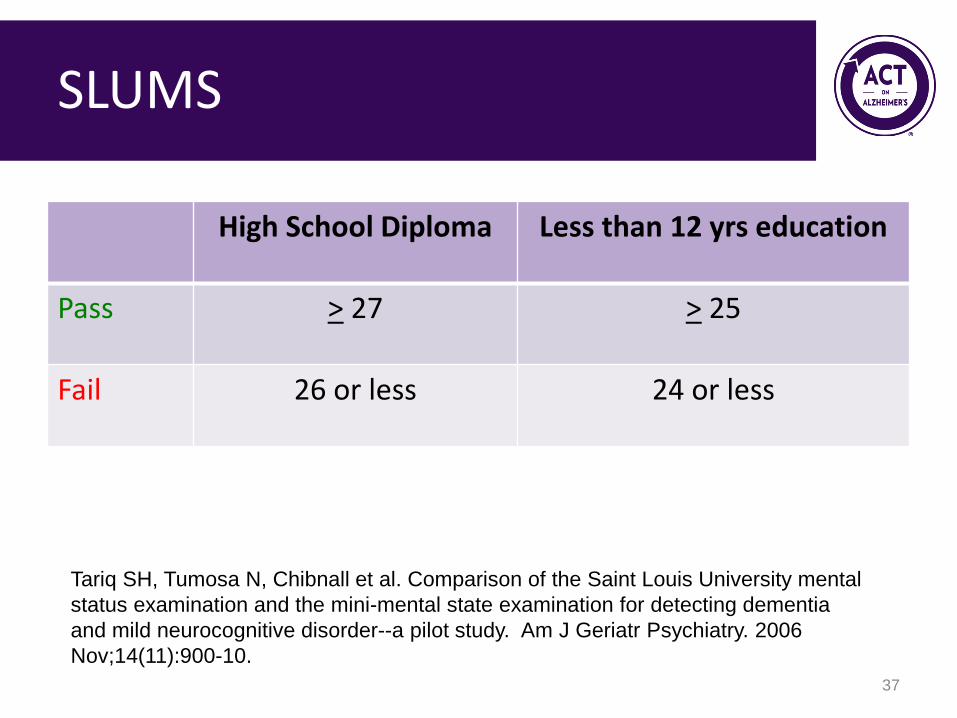
SLUMS
High School Diploma Less than 12 yrs education
Pass > 27 > 25
Fail 26 or less 24 or less
37
Tariq SH, Tumosa N, Chibnall et al. Comparison of the Saint Louis University mental status examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder--a pilot study. Am J Geriatr Psychiatry. 2006 Nov;14(11):900-10.
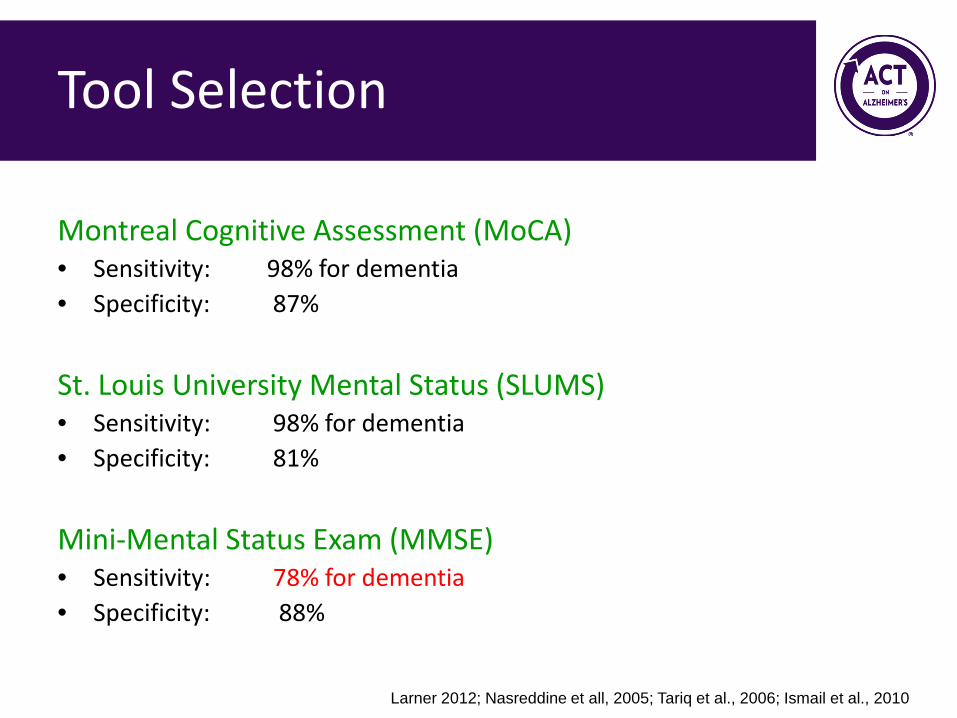
Tool Selection Montreal Cognitive Assessment (MoCA) • Sensitivity: 98% for dementia • Specificity: 87% St. Louis University Mental Status (SLUMS) • Sensitivity: 98% for dementia • Specificity: 81% Mini-Mental Status Exam (MMSE) • Sensitivity: 78% for dementia • Specificity: 88%
Larner 2012; Nasreddine et all, 2005; Tariq et al., 2006; Ismail et al., 2010
CPT- Cognitive performance test
• Fairview Occupational Therapist – Identify level of functional impairment associated
with cognitive deficit
• Formal neuropsychiatric testing
39
Delivering the Diagnosis
• GIVE the diagnosis • Connect patient/family to community
resources – Examples: Senior linkage line, Alzheimer’s
Association
• Discuss follow-up – regular intervals (e.g., q 6 months) for proactive
care
• Provide written summary of visit 40
Delivering the Diagnosis
• Address immediate problems: – Management of medications, finances, meals – Home safety – Caregiver burnout – Need care supporter to track and come to
appointments
41
Delivering the Diagnosis: Sam
42
https://www.youtube.com/watch?v=vy2ZC5ZSZL8

Dementia Care and Treatment
43
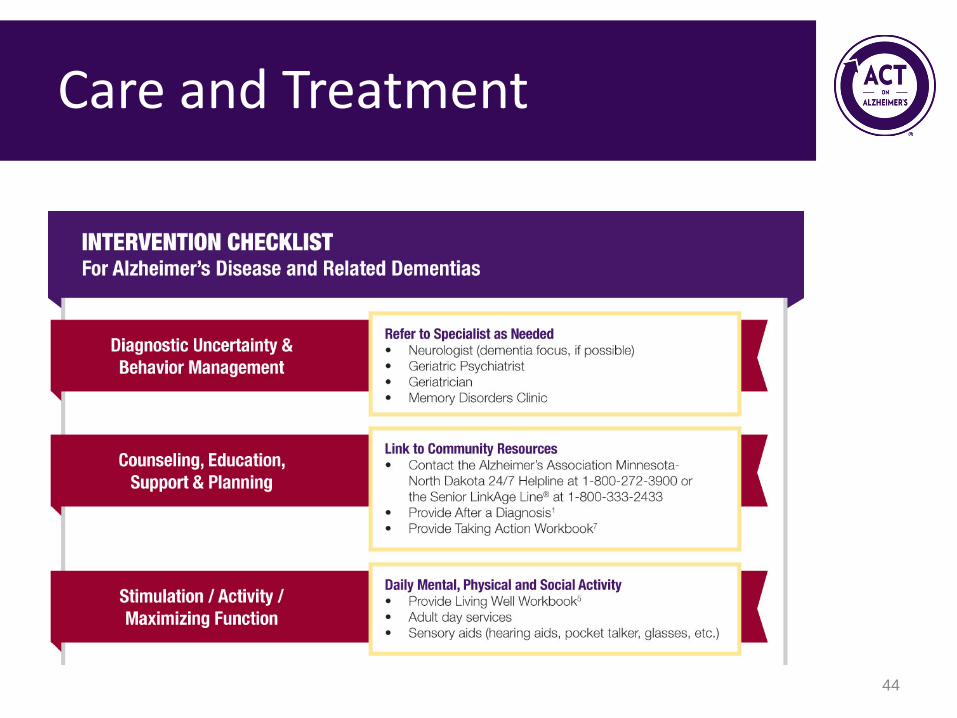
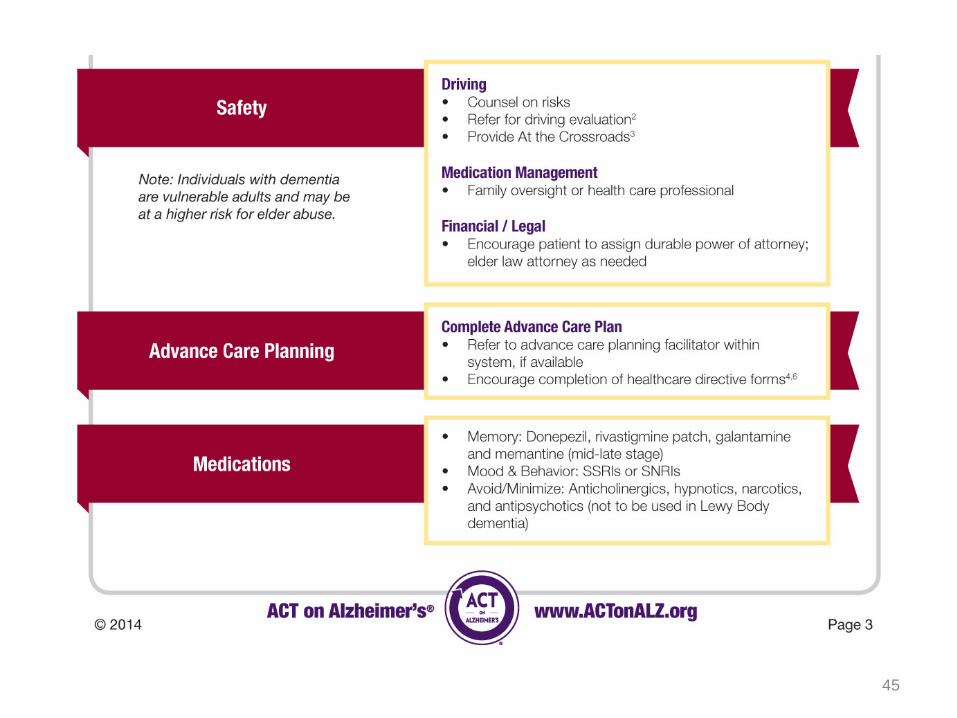
Care and Treatment
44
45
Care and Treatment
Treatment: Medications
• Cholinesterase inhibitors
– Donepezil, Rivastigmine, Galantamine, Cognex – Possible side effects: nausea, vomiting, syncope,
dizziness, anorexia
• NMDA receptor antagonist – Memantine – Possible side effects: tiredness, body aches,
dizziness, constipation, headache 46
Care and Treatment
• The care for patients with Alzheimer’s has very little to do with pharmacology and more to do with psychosocial interventions
• Connect patient and family to experts in the community – Alzheimer’s Association, care coordinator – Stress this is part of their treatment plan and you
expect to hear about their progress at next visit
47
Confusion in older adults - beyond dementia Dementia • Chronic, progressive
decline in cognitive function
Delirium • Acute onset of
confusion with lack of attention
48
What is delirium? DSM 5
• Impaired attention • Acute disturbance of consciousness • Fluctuating course
• Disorganized thinking • Perceptual disturbances • Psychomotor changes • Sleep disturbance • Evidence that there is an underlying physiologic or
medical condition causing the disorder
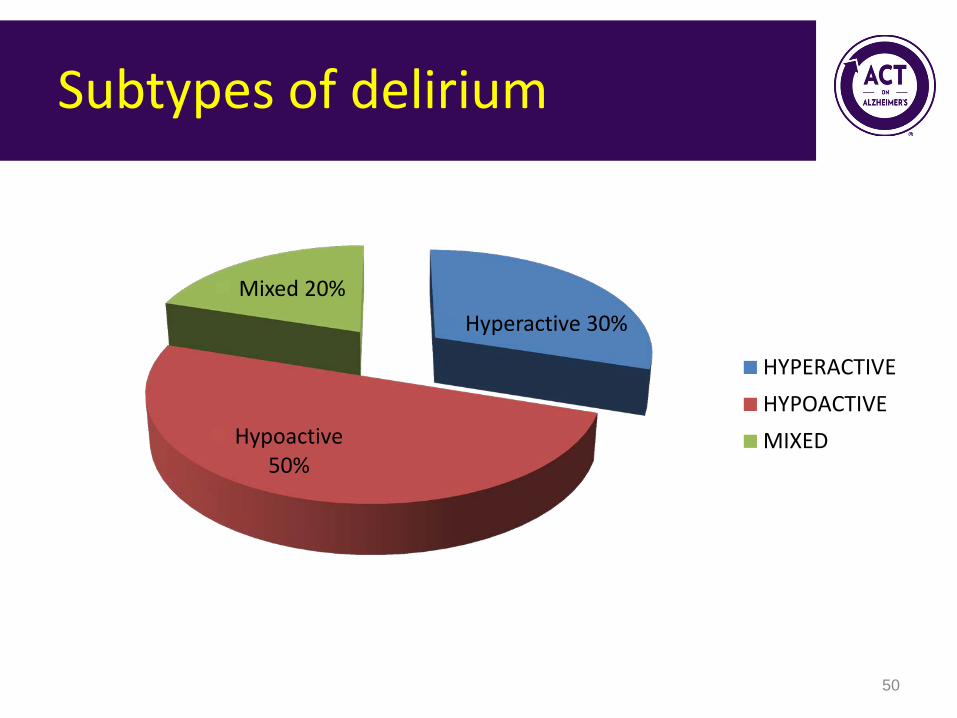
Subtypes of delirium
Hyperactive 30%
Hypoactive 50%
Mixed 20%
HYPERACTIVEHYPOACTIVEMIXED
50
• Anyone with underlying physiologic or medical instability
= Those stressed and with limited reserve* *This is the frail geriatric population
Who is at risk for delirium?
• “Anything” that can acutely disrupt normal brain function – Medications – Brain trauma – Blood chemistry abnormalities – Infection – Pain – Myocardial ischemia
Causes of Delirium usually multiple causes!
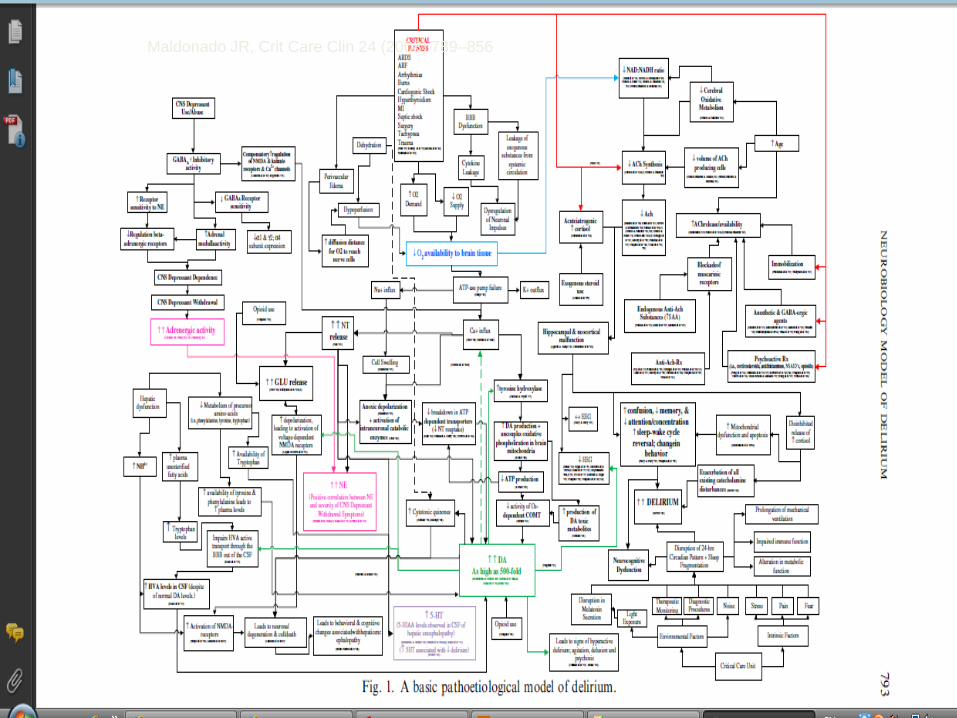
Maldonado JR, Crit Care Clin 24 (2008) 789–856
ANY change in drug therapy
– New – Discontinued – Dose change – Time change
Medications – common contributor to delirium
• Most common offenders:
ANTICHOLINERGIC medications
Benadryl Urinary incontinence drugs Antidepressants Antipsychotics
Medications
• 1. Acute onset and fluctuating course • 2. Inattention
• 3. Disorganized thinking • 4. Altered level of consciousness
• Probable delirium requires (1 and 2) + (3 or 4)
Identifying delirium tool
CAM – Confusion Assessment Method
Delirium
• Evidence that there is an underlying physiologic or medical condition causing the disorder
57
Causes of Delirium
• Mnemonic Drugs Electrolyte disturbances Lack of drugs Infection Reduced sensory input Intracranial Urinary, fecal Myocardial, pulmonary
Summary
• Confusion in older women can be confusing
– Dementia is a chronic progressive decline in
cognitive function
– Delirium is an acute decline in cognition with lack of attention and should be reversible
59
Objectives
1. Be aware of the updated DSM5 criteria for “dementia” 2. Identify indications for "screening" for dementia in older women 3. Know the components of a diagnostic evaluation – www.actonalz.org 4. Recognize delirium in older women
60
Top 5 Resources for Patients and Families
61

#1 Promoting Wellness & Function
62
#2 Addressing Behavioral Challenges
63

#3 Caregiver Support
Alzheimer’s Association
800.272.3900 | www.alz.org/mnnd
One stop shop for: – Care Consultation – Support Groups (Memory Club) – 24/7 Helpline
64
References & Resources • Alzheimer’s Association (2014). Alzheimer’s Disease Facts and Figures, Alzheimer’s & Dementia, Volume 10, Issue 2. • Anderson K, Jue S & Madaras-Kelly K 2008. Identifying Patients at Risk for Medication Mismanagement: Using Cognitive
Screens to Predict a Patient's Accuracy in Filling a Pillbox. The Consultant Pharmacist, 6(14), 459-72. • Barry PJ, Gallagher P, Ryan C, & O‘mahony D. (2007). START (screening tool to alert doctors to the right treatment)--an
evidence-based screening tool to detect prescribing omissions in elderly patients. Age and Ageing, 36(6): 632-8. • Blendon RJ, Benson JM, Wikler, EM, Weldon, KJ, Georges, J, Baumgart, M, Kallmyer B. (2012). The impact of experience
with a family member with Alzheimer’s disease on views about the disease across five countries. International Journal of Alzheimer’s Disease, 1-9.
• Boise L, Neal MB, & Kaye J (2004). Dementia assessment in primary care: Results from a study in three managed care systems. Journals of Gerontology: Series A; Vol 59(6), M621-26.
• Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. (2000). The mini-cog: a cognitive “vital signs” measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry, 15(11):1021-1027.
• Borson S, Scanlan JM, Chen P, Ganguli M. (2003). The Mini-Cog as a screen for dementia: validation in a population-based sample. J Am Geriatr Soc;51(10):1451-1454.
• Borson S, Scanlan J, Hummel J, Gibbs K, Lessig M, & Zuhr E (2007). Implementing Routine Cognitive Screening of Older Adults in Primary Care: Process and Impact on Physician Behavior. J Gen Intern Med; 22(6): 811–817.
• Boustani M, Peterson B, Hanson L, et al. (2003). Systematic evidence review. Agency for Healthcare Research and Quality; Rockville, MD: Screening for dementia.
• Boustani M, Callahan CM, Unverzagt FW, Austrom MG, Perkins AJ, Fultz BA, Hui SL, Hendrie HC (2005). Implementing a screening and diagnosis program for dementia in primary care. J Gen Intern Med. Jul; 20(7):572-7.
• Ferri CP, Prince M, Brayne C, et al. (2005). Alzheimer’s Disease International Global prevalence of dementia: A Delphi consensus study. Lancet, 366: 2112–2117.
65
References & Resources • Finkel, SI (Ed.) (1996). Behavioral and Psychological Signs of Dementia: Implications for Research and Treatment.
International Psychogeriatrics, 8(3). • Folstein MF, Folstein SE, & McHugh PR (1975). "Mini-mental state". A practical method for grading the cognitive state of
patients for the clinician. J Psychiatr Res, Nov 12(3):189-98. • Gallagher P & O’Mahony D (2008). STOPP (Screening Tool of Older Persons’ potentially inappropriate Prescriptions):
Application to acutely ill elderly patients and comparison with Beers’ criteria. Age and Ageing, 37(6): 673-9. • Gitlin LN, Kales HC, Lyketsos CG, & Plank Althouse E (2012). Managing Behavioral Symptoms in Dementia Using
Nonpharmacologic Approaches: An Overview. JAMA, 308(19): 2020-29. • Holroyd S, Turnbull Q, & Wolf AM (2002). What are patients and their families told about the diagnosis of dementia?
Results of a family survey. Int J Geriatr Psychiatry, Mar;17(3):218-21. • Ismail Z, Rajji TK, & Shulman KI (2010). Brief cognitive screening instruments: An update. Int J Geriatr Psychiatry, 25:111–20. • Jeste DV, Blazer D, Casey D et al. (2008). ACNP White Paper: Update on Use of Antipsychotic Drugs in Elderly Persons with
Dementia. Neuropsychopharmacology, 33(5): 957-70. • Larner AJ (2012). Screening utility of the Montreal Cognitive Assessment (MoCA): In place of – or as well as – the MMSE?
Intern Psychogeriatrics, 24, 391–396. • Lin JS, O’Connor E, Rossom RC, Perdue LA, Burda BU, Thompson M, & Eckstrom E (2014). Screening for Cognitive
Impairment in Older Adults: An Evidence Update for the U.S. Preventive Services Task Force. Agency for Healthcare Research and Quality, Evidence Syntheses, 107.
• Long KH, Moriarty JP, Mittelman MS, & Foldes SS (2014). Estimating The Potential Cost Savings From The New York University Caregiver Intervention In Minnesota. Health Affairs, 33(4), 596-604.
• McCarten JR, Anderson P Kuskowski MA et al. (2012). Finding dementia in primary care: The results of a clinical demonstration project. J Am Geritr Soc;60(2):210-217.
66
• Mittelman MS, Haley WE, Clay OJ, & Roth DL (2006). Improving caregiver well-being delays nursing home placement of
patients with Alzheimer disease. Neurology, November 14(67 no. 9), 1592-1599. • Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, Cummings JL, & Chertkow H. (2005). The
Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J Amer Ger Soc, 53(4), 695-99.
• National Chronic Care Consortium and the Alzheimer’s Association. 1998. Family Questionnaire. Revised 2003. • Silverstein NM & Maslow K (Eds.) (2006). Improving Hospital Care for Persons with Dementia. New York: Springer Publishing
CO. • Tariq SH, Tumosa N, Chibnall JT, Perry MH, & Morley E. (2006). Comparison of the Saint Louis University mental status
examination and the mini-mental state examination for detecting dementia and mild neurocognitive disorder: A pilot study. Am J Geriatr Psychiatry, Nov;14(11):900-10.
• Turnbull Q, Wolf AM, & Holroyd S (2003). Attitudes of elderly subjects toward “truth telling” for the diagnosis of Alzheimer’s disease. J Geriatr Psychiatry Neurol, Jun;16(2):90-3.
• Zaleta AK & Carpenter BD (2010). Patient-Centered Communication During the Disclosure of a Dementia Diagnosis. Am J Alzheimers Dis Other Demen, 25, 513.
67
References & Resources
References & Resources
• 2012 Updated AGS Beers Criteria: http://www.americangeriatrics.org/files/documents/beers/2012BeersCriteria_JAGS.pdf
• After a Diagnosis (ACT): http://www.actonalz.org/sites/default/files/documents/ACT-AfterDiagnosis.pdf Alzheimer’s Association • Basics of Alzheimer’s Disease: https://www.alz.org/national/documents/brochure_basicsofalz_low.pdf • Caregiver Notebook - http://www.alz.org/care/alzheimers-dementia-caregiver-notebook.asp • Driving Center: www.alz.org/care/alzheimers-dementia-and-driving.asp • Facts & Figures video: http://youtu.be/waeuks1-3Z4 • Facts & Figures Report: https://www.alz.org/facts/downloads/facts_figures_2015.pdf • Family Questionnaire: http://www.alz.org/mnnd/documents/Family_Questionnaire.pdf • Know the 10 Signs. http://www.alz.org/national/documents/checklist_10signs.pdf • Living with Alzheimer’s – Mid Stage: https://www.alz.org/documents_custom/middle-stage-caregiver-tips.pdf • Living with Alzheimer’s – Late Stage: https://www.alz.org/documents_custom/late-stage-caregiver-tips.pdf • Living Well workbook:http://www.alz.org/documents/mndak/alz_living_well_workbook_2011v2_web.pdf • Taking Action Workbook: http://www.alz.org/mnnd/documents/2010_taking_action_e-book(1).pdf • Trial Match: http://www.alz.org/research/clinical_trials/find_clinical_trials_trialmatch.asp
68
References & Resources
• AD8 Dementia Screening Interview: http://knightadrc.wustl.edu/About_Us/PDFs/AD8form2005.pdf • At the Crossroads: http://www.thehartford.com/sites/thehartford/files/at-the-crossroads-2012.pdf • Caring for a Person with Alzheimer’s Disease:
http://www.nia.nih.gov/sites/default/files/caring_for_a_person_with_alzheimers_disease_0.pdf • Coach Broyles Playbook on Alzheimer’s: http://www.caregiversunited.com • Honoring Choices Minnesota:http://www.honoringchoices.org • Hospitalization Happens: http://www.nia.nih.gov/sites/default/files/hospitalization_happens_0.pdf • Medicare Annual Wellness Visit: http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-
MLN/MLNMattersArticles/downloads/MM7079.pdf • MiniCog™ http://www.alz.org/documents_custom/minicog.pdf • MN Health Care Home Care Coordination Tool Kit:
http://www.health.state.mn.us/healthreform/homes/collaborative/lcdocs/cliniccarecoordtoolkit.pdf • Montreal Cognitive Assessment (MoCA)http://www.mocatest.org • National Alzheimer’s Project Act: http://aspe.hhs.gov/daltcp/napa/NatlPlan.pdf • Next Step in Care: http://www.nextstepincare.org • Physician Orders for Life Sustaining Treatment (POLST): http://www.polst.org • St. Louis University Mental Status (SLUMS) examination
http://medschool.slu.edu/agingsuccessfully/pdfsurveys/slumsexam_05.pdf
69

















