Patient Name --;------,C7C----------------- Last Name
First Name Middle Initial
Address _
E-mail _
City _
State _ Zip _
Sex D M D F Age _
Birthdate _
D Married DWidowed D Single D Minor
D Separated D Divorced D Partnered for years
Patient Employer/School _
Occupation _
Employer/School Address _
Employer/School Phone (__) _
Spouse's Name _
Birthdate _
SS# _
Spouse's Employer _
Whom may we thank for referring you? _
~ - DENTAL INSURANCE
Who is responsible for this account? _
Relationship to Patient _
Insurance Co. _
Group # _
Is patient covered by additional insurance? DYes D No
Subscriber's Name _
Birthdate _ SS# _
Relationship to Patient _
Insurance Co. _
Group # _
ASSIGNMENT AND RELEASE I certify that I, and/or my dependent(s}, have insurance coverage with
___~,_____---,-,----=---_,,_____,___---and assign directly to Name of Insurance Company(ies)
Dr. all insurance benefits, if any, otherwise payable to me for services rendered. I understand that I am financially responsible for all charges whether or not paid by insurance, I authorize the use of my signature on all insurance submissions.
The above-named dentist may use my health care information and may disclose such information to the above-named Insurance Company(ies} and their agents for the purpose of obtaining payment for services and determining insurance benefits or the benefits payable for related services. This consent will end when my current treatment pian is completed or one year from the date signed below.
Signature of Patient, Parent, Guardian or Personal Representative
Please print name of Patient, Parent, Guardian or Personal Representative
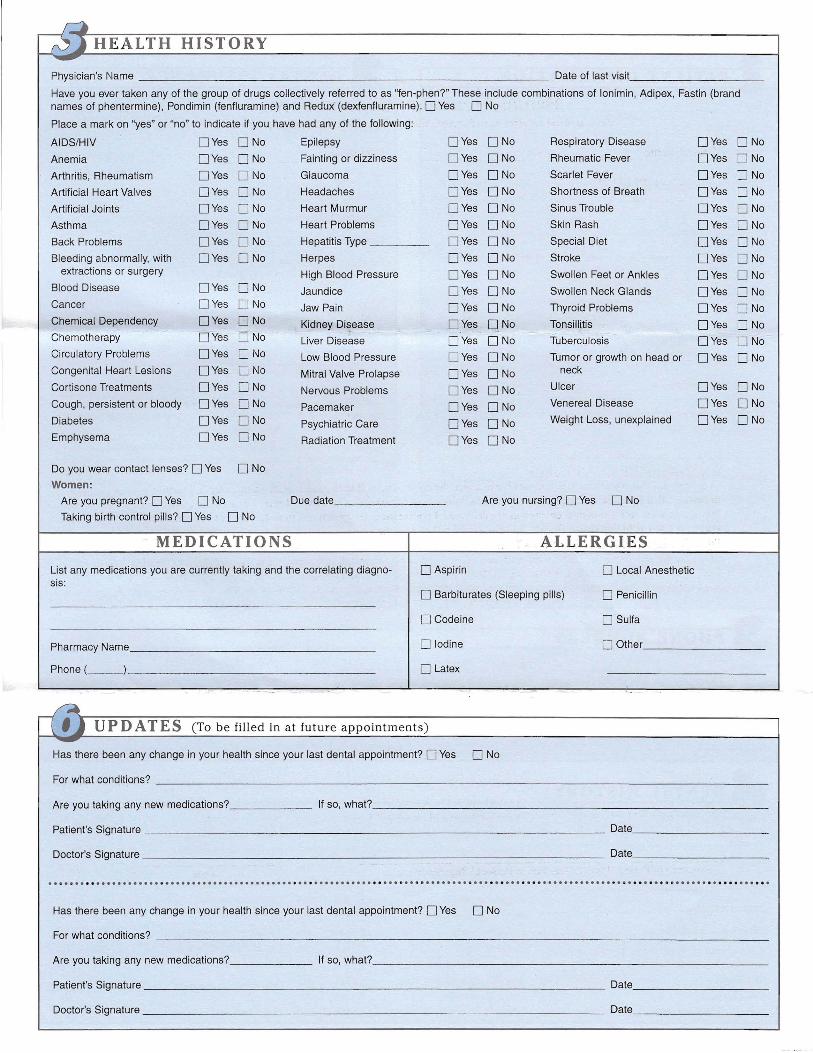
~HEALTH HISTORY-Physician's Name Date of last visit
Have you ever taken any of the group of drugs collectively referred to as ''fen-phen?'' These include combinations of lonimin, Adipex, Fastin (brand names of phentermine), Pondimin (fenfluramine) and ReduX (dexfenfluramine).D Yes DNa
Place a mark on "yes" or "no" to indicate if you have had any of the following:
AIDS/HIV DYes DNa Epilepsy DYes DNa Respiratory Disease DYes DNa
Anemia DYes DNa Fainting or dizziness DYes DNa Rheumatic Fever DYes DNa
Arthritis, Rheumatism DYes DNa Glaucoma DYes DNa Scarlet Fever DYes DNa
Artificial Heart Valves DYes DNa Headaches DYes DNa Shortness of Breath DYes DNa
Artificial Joints DYes DNa Heart Murmur DYes DNa Sinus Trouble DYes DNa
Asthma DYes DNa Heart Problems DYes DNa Skin Rash DYes DNa
Back Problems DYes DNa Hepatitis Type DYes DNa Special Diet DYes DNa
Bleeding abnormally, with DYes DNa Herpes DYes DNa Stroke DYes DNa extractions or surgery High Blood Pressure DYes DNa Swollen Feet or Ankles DYes DNa
Blood Disease DYes DNa Jaundice DYes DNa Swollen Neck Glands DYes DNa Cancer DYes DNa Jaw Pain DYes DNa Thyroid Problems DYes DNa Chemical Dependency DYes DNa Kidney Disease DYes DNa Tonsillitis DYes DNa Chemotherapy DYes DNa Liver Disease DYes DNa Tuberculosis DYes DNa Circulatory Problems DYes DNa Low Blood Pressure DYes DNa Tumor or growth on head or DYes DNa Congenital Heart Lesions DYes DNa Mitral Valve Prolapse DYes DNa neck
Cortisone Treatments DYes DNa Nervous Problems DYes DNa Ulcer DYes DNa
Cough, persistent or bloody DYes DNa Pacemaker DYes DNa Venereal Disease DYes DNa
Diabetes DYes DNa Psychiatric Care DYes DNa Weight Loss, unexplained DYes DNa
Emphysema DYes DNa Radiation Treatment DYes DNa
Do you wear contact lenses? DYes DNa
Women:
Are you pregnant? DYes DNa Due date Are you nursing? DYes DNa
Taking birth control pills? DYes DNa
MEDICATIONS ALLERGIES
List any medications you are currently taking and the correlating diagno- D Aspirin D Local Anesthetic sis:
D Barbiturates (Sleeping pills) D Penicillin
D Codeine D Sulfa
D Iodine D Other Pharmacy Name
Phone (__) D Latex
~ - -.
[(Ij UPDATES (To be filled in at future appointments)-Has there been any change in your health since your last dental appointment? DYes D No
For what conditions? _
Are you taking any new medications? If so, what? _
Has there been any change in your health since your last dental appointment? DYes D No
For what conditions? _
Are you taking any new medications? If so, what? _
Patient's Signature Date _
Doctor's Signature _ Date _
---------------
Dental Treatment Consent Form Please read and initial the items that apply below. Then read and sign the bottom of the form.
Patient Name Birthdate _
WORK TO BE DONE ) understand that I am having the following work done: FiJlings Bridges.,----_--,--_
Crowns Extractions Impacted teeth removed General Anesthesia,__c:---:--,--,
Root Canals Cleanings X-rays___ (initials) _ DRUGS AND MEDICATIONS
I understand that antibiotics and analgesics and other medications can cause allergic reactions causing redness and swclling oftissucs, pain, itching, vomiting, and/or anaphylactic shuck (severe allergic reaction) (initials) _ CHANGES IN TREATMENT PLAN
I understand that during treatment it may be necessary to change or add procedures because of conditions found while working on the teeth that were not discovered during examination, the most common being root canal therapy following routine procedures. I give my permission to the Dentist to make any/all changes and additions as necessary.
(initials) _ REMOV AL OF TEETH
AJternatives to removal have been explained to me (root canal therapy, crowns, and periodontal surgery, etc.) and 1 authorize the Dentist to remove the following teeth And any others necessary for reasons in paragraph #3. I understand removing teeth does not always remove all the infection, if present, and it may be necessary to have ['urther lrealment. I understand the risks involved in having teeth removed, some of which are pain, swelling, spread of infection, dry socket, loss offeeling, lips, tongue, and surrounding tissue (Paresthesia) that can last for an indefinite period of time (days or months) or fractured jaw. I understand I may need further treatment by a specialist or even hospitalization if complications arise during or following treatment, the cost of which is my responsibility. (initials) _ CROWNS, BRIDGES AND CAPS
I understand that sometimes it is not possible to match the color ofnatural teeth exactly with artificial teeth, I further understand that I may be wearing temporary crowns, which may come off easily and that I must be careful to ensure that they are kept on until the permanent crowns are delivered. 1 realize the final opportunity to make changes in my new crown, bridge, or cap (including shape, fit, size, and color) will be before cementation. (inilials) _ DENTURES. COMPLETE OR PARTIAL
[ realize that full or partial dentures are artificial, constructed of plastic, metal, and/or porcelain. The problems of wearing these appliances have been explained to me, including looseness, soreness, and possible breakage. I realize tha final opportunity to make changes in my new denture (including shape, fit, size, placement, and color) will be the "teeth in wax" try-in visit. [ understand that most dentures require relining approximately three to twelve months after initial placement. The cost for this procedure is not included in the initial denture fee. (initials) _ ENDODONTIC TREATMENT (ROOT CANAL)
I realize there is no guarantee that root canal treatment will save my tooth, and that complications can occur from the treatment, and that occasionally metal objects are cemented in the tooth or extent through the root, which does not necessari ly affect the success of the treatment, J understand that occasionally additional surgical procedures may be necessary following root canal treatment (apicoectomy). (initials) _ PERIODONTAL LOSS (TISSUE AND BONE)
[ understand that J have a serious condition, causing gum and bone infection or loss and that it can lead to the loss of my teeth. Alternative treatment plans have been explained to me, including gum surgery, replacement and/or extractions. J understand that undertaking any dental procedures may have a future adverse effect on my periodontal condition.
(initials) _ 1understand that dentistry is not an exact science and that, therefore, reputable practitioners cannot guarantee results, I acknowledge that no guarantee or assurance has been made to me by anyone regarding the dental treatment that I have requested and authorized for my self or my minor child. [ have had full opportunity to discuss and ask questions regarding the dental treatment, and all questions have been answered to my satisfaction.
Signature of Patient, Parent, Guardian or Personal Representative Date
Please print name of Patient, Parent, Guardian or Personal Representative Relationship to Patient
FINANCIAL POLICY
This statement is to inform you of our financial policy. We are committed to providing you with the highest quality dental care using only the best material and teclmology available in the market today. We are also committed to providing you with up-to-date information and educational tools so that you may fully participate in maintaining optimum oral health. Our financial policy is intended to facilitate excellent service to you while minimizing our administrative costs.
All charges you incur are your responsibility regardless of your insurance coverage. We must emphasize that as your dental care provider, our relationship is with you, our patient, not with your insurance company. Your insurance policy is a contract between you, your employer, and the insurance company. Our office is nOt. a third party to that contract.
As a courtesy to you we will help you process all your insurance claims. You may direct your insurance company to pay your benefits directly to our office by signing the authorization on the Assignment and Release section of the Dental Registration and History form. In order for our office to file your insurance claim, you must bring completed dental insurance or proof or insurance at each appointment.
If you have dual insurance, we will also assist you in processing these claims. We will first submit your claim to your primary insurance company. After they make payment, we will submit your claim to your secondary insurance company. Your financial responsibility will be based off of your benefits with your primary insurance, unless preauthorization's have been made.
Payment is due at time service is provided. Our office accepts cash, personal checks, MasterCard, and Visa. Outside financing is available through CareCredit upon request and approval.
Balances older than 30 days may be subject to finance charges at the rate of 10%, billed monthly. Balances older than 60 days may be subject to finance charges and collection fees. Returned checks will be subject to a $25.00 fee. Additionally, our office will charge you for broken appointments cancelled without 48 hour (2 days) advance notice.
If you have any questions regarding our financial policy, please ask. We are committed to providing you with the most positive experience in dental care.
Print Name
Signature Date
------------- -------
--
----
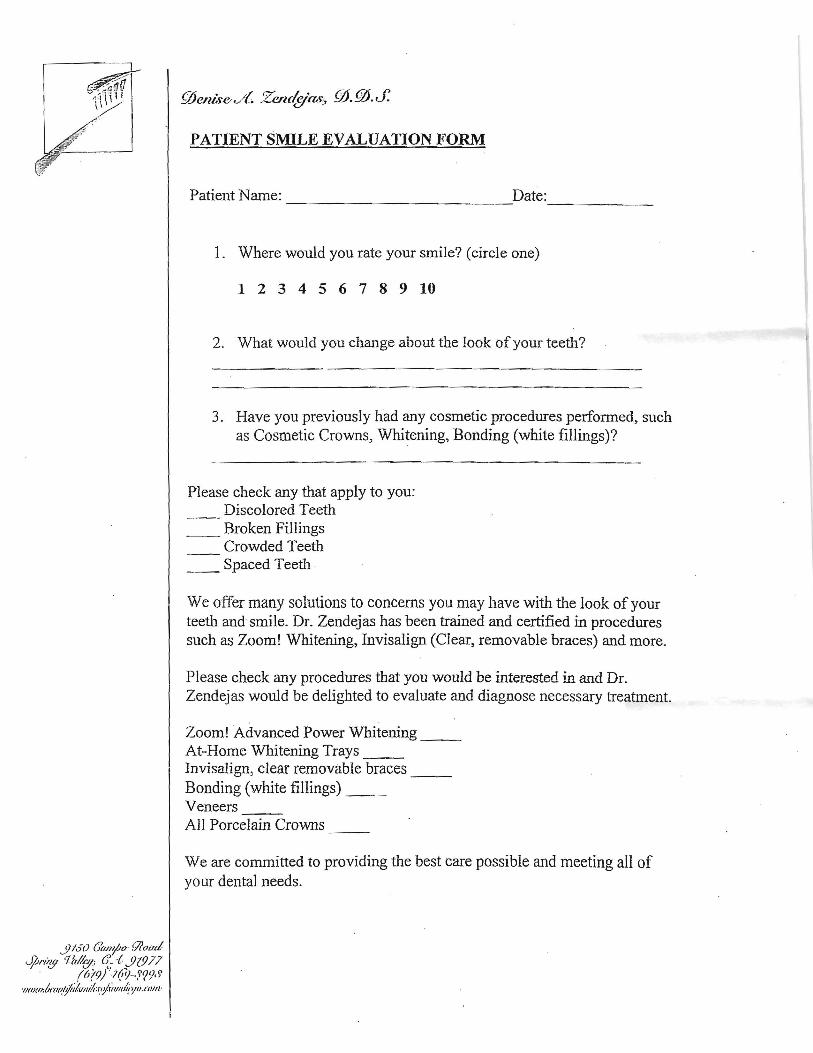
PATIENT SMILE EVALUATION FORM
Patient Name: Date:
1. Where would you rate your smile? (circle one)
1 2 3 4 5 6 7 8 9 10
2. What would you change about the look ofyour teeth?
3. Have you previously had any cosmetic procedures performed, such as Cosmetic Crowns, Whitening, Bonding (white fillings)?
Please check any that apply to you: Discolored Teeth
__ Broken Fillings Crowded Teeth
__ Spaced Teeth .
We offer many solutions to conCerns you may have with the look ofyour teeth and smile. Dr. Zendejas has been trained and certified in procedures such as Zoom! Whitening, Invisalign (Clear, removable braces) and more.
Please check any procedures that you would be interested in and Dr. Zendejas would be delighted to evaluate and diagnose necessary treatment.