Correspondence 225 Figure 3 Long TE (144 ms) monovoxel spectroscopy shows that the N-acetyl-aspartate (NAA) peak is absent and an elevated choline peak at 3.2 ppm. Note the absence of an alanine peak at 1.5 ppm. References [1] Caroli E, Salvati M, Orlando ER, et al. Solitary fibrous tumors of the meninges: report of four cases and literature review. Neurosurg Rev 2004;27:246—51. [2] Weon YC, Kim EY, Kim HJ, Byun HS, Park K, Kim JH. Intracranial solitary fibrous tumors: imaging findings in 6 consecutive patients. AJNR Am J Neuroradiol 2007;28(8): 1466—9. [3] Clarenc ¸on F, Bonneville F, Rousseau A, Galanaud D, Kujas M, Naggara O, et al. Intracranial solitary fibrous tumor: Imaging findings. Eur J Radiol 2011;80(2): 387—94. [4] Cho YD, Choi GH, Lee SP, Kim JK. H-MRS metabolic patterns for distinguishing between meningiomas and other brain tumor. Magn Reson Imaging 2003;21:663—72. [5] Kim KA, Gonzalez I, McComb JG, Giannotta SL. Unusual presen- tations of cerebral solitary fibrous tumors: report of four cases. Neurosurgery 2004;54(4):1004—9. Nivaldo Adolfo Da Silva Jr Fabiano Reis ∗ Department of Radiology, Universidade Estadual de Campinas (UNICAMP), 251, Rua Vital-Brazil, Cidade Universitária Zeferino Vaz., 13083-888, Campinas, São Paulo, Brazil Luciano De Souza Queiroz Department of Pathology, Universidade Estadual de Campinas (UNICAMP), Campinas, São Paulo, Brazil Delphine Sanmartin Fabrice Bonneville Service de neuroradiologie diagnostique et thérapeutique, hôpital Purpan, CHU de Toulouse, Toulouse, France ∗ Corresponding author. Tel.: +55 19 3521 7029/+55 19 3521 7280. E-mail address: [email protected](F. Reis) http://dx.doi.org/10.1016/j.neurad.2012.05.011 Dentate nuclei and Wernicke’s encephalopathy A 64-year-old woman was admitted to the emergency department because of static cerebellar syndrome. She had multiple cardiovascular risk factors and child class C cirrhosis of alcoholic origin, with an estimated alcohol con- sumption of 30 to 50g/day. Brain computed tomography (CT) showed no significant abnormality and magnetic resonance imaging (MRI) was per- formed to exclude posterior circulation stroke. MRI showed focal hyperintense anomalies of the dentate nuclei on fluid- attenuated inversion recovery (FLAIR), T2-weighted and diffusion-weighted sequences (Fig. 1a, b, c), with no con- trast enhancement on T1-weighted imaging. The diagnosis of atypical Wernicke’s encephalopathy was suspected. For this reason, it was suggested to perform an MRI control 2weeks after vitamin B1 therapy. The patient received treatment with vitamin B1 intra- venously for 3 days, and oral administration of B1 at 600 mg/day thereafter. MR imaging 2 weeks later showed complete regression of the abnormalities (Fig. 2a, b). The patient improved clinically with partial regression of her symptoms. Wernicke’s encephalopathy (WE), first described by Wernicke in 1881 [1], is related to vitamin B1 (thiamine) deficiency. The disease is characterized by a classical triad of symptoms [2] found in 30% of cases, including mental dis- orders such as confusion, apathy and hypersomnia (80% of cases), oculomotor disturbances such as nystagmus and ocu- lomotor palsy (93% of cases), and balance disorders (76% of cases). Vitamin B1 deficiency arises most often in alcoholic patients, but can also be seen in other situations such as prolonged intravenous feeding, anorexia, malnutrition, prolonged fasting (hunger strike), chronic vomiting and recovery (recharging) without vitamin therapy [2].
Transcript
Correspondence 225
Figure 3 Long TE (144 ms) monovoxel spectroscopy shows that the N-acetyl-aspartate (NAA) peak is absent and an elevatedt 1.5
D
dhcs
affadt
sM
v6cps
Wdooclc
patients, but can also be seen in other situations such
choline peak at 3.2 ppm. Note the absence of an alanine peak a
References
[1] Caroli E, Salvati M, Orlando ER, et al. Solitary fibrous tumorsof the meninges: report of four cases and literature review.Neurosurg Rev 2004;27:246—51.
[2] Weon YC, Kim EY, Kim HJ, Byun HS, Park K, Kim JH.Intracranial solitary fibrous tumors: imaging findings in 6consecutive patients. AJNR Am J Neuroradiol 2007;28(8):1466—9.
[3] Clarencon F, Bonneville F, Rousseau A, Galanaud D,Kujas M, Naggara O, et al. Intracranial solitary fibroustumor: Imaging findings. Eur J Radiol 2011;80(2):387—94.
[4] Cho YD, Choi GH, Lee SP, Kim JK. H-MRS metabolic patternsfor distinguishing between meningiomas and other brain tumor.Magn Reson Imaging 2003;21:663—72.
[5] Kim KA, Gonzalez I, McComb JG, Giannotta SL. Unusual presen-tations of cerebral solitary fibrous tumors: report of four cases.Neurosurgery 2004;54(4):1004—9.
Nivaldo Adolfo Da Silva JrFabiano Reis ∗
Department of Radiology, Universidade Estadual deCampinas (UNICAMP), 251, Rua Vital-Brazil, Cidade
Universitária Zeferino Vaz., 13083-888, Campinas, SãoPaulo, Brazil
Luciano De Souza QueirozDepartment of Pathology, Universidade Estadual de
Campinas (UNICAMP), Campinas, São Paulo, BrazilDelphine SanmartinFabrice Bonneville
Service de neuroradiologie diagnostique et thérapeutique,hôpital Purpan, CHU de Toulouse, Toulouse, France
E-mail address: [email protected] (F. Reis)http://dx.doi.org/10.1016/j.neurad.2012.05.011
apr
ppm.
entate nuclei and Wernicke’s encephalopathy
A 64-year-old woman was admitted to the emergencyepartment because of static cerebellar syndrome. Shead multiple cardiovascular risk factors and child class Cirrhosis of alcoholic origin, with an estimated alcohol con-umption of 30 to 50 g/day.
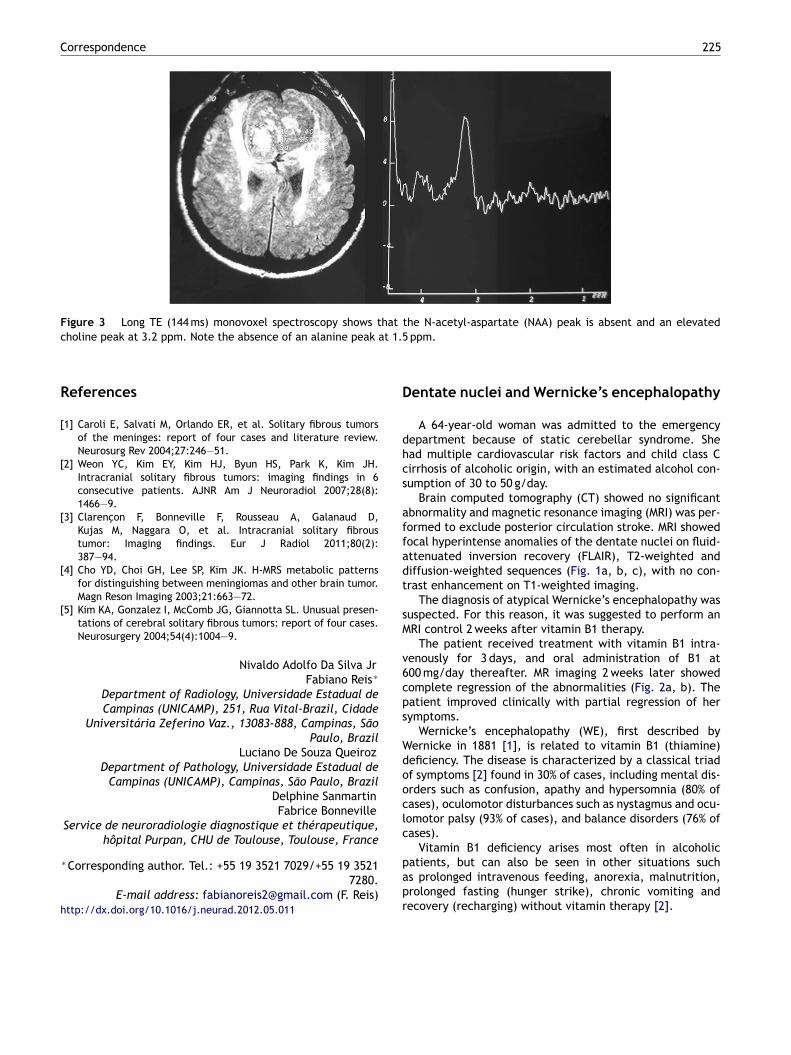
Brain computed tomography (CT) showed no significantbnormality and magnetic resonance imaging (MRI) was per-ormed to exclude posterior circulation stroke. MRI showedocal hyperintense anomalies of the dentate nuclei on fluid-ttenuated inversion recovery (FLAIR), T2-weighted andiffusion-weighted sequences (Fig. 1a, b, c), with no con-rast enhancement on T1-weighted imaging.
The diagnosis of atypical Wernicke’s encephalopathy wasuspected. For this reason, it was suggested to perform anRI control 2 weeks after vitamin B1 therapy.
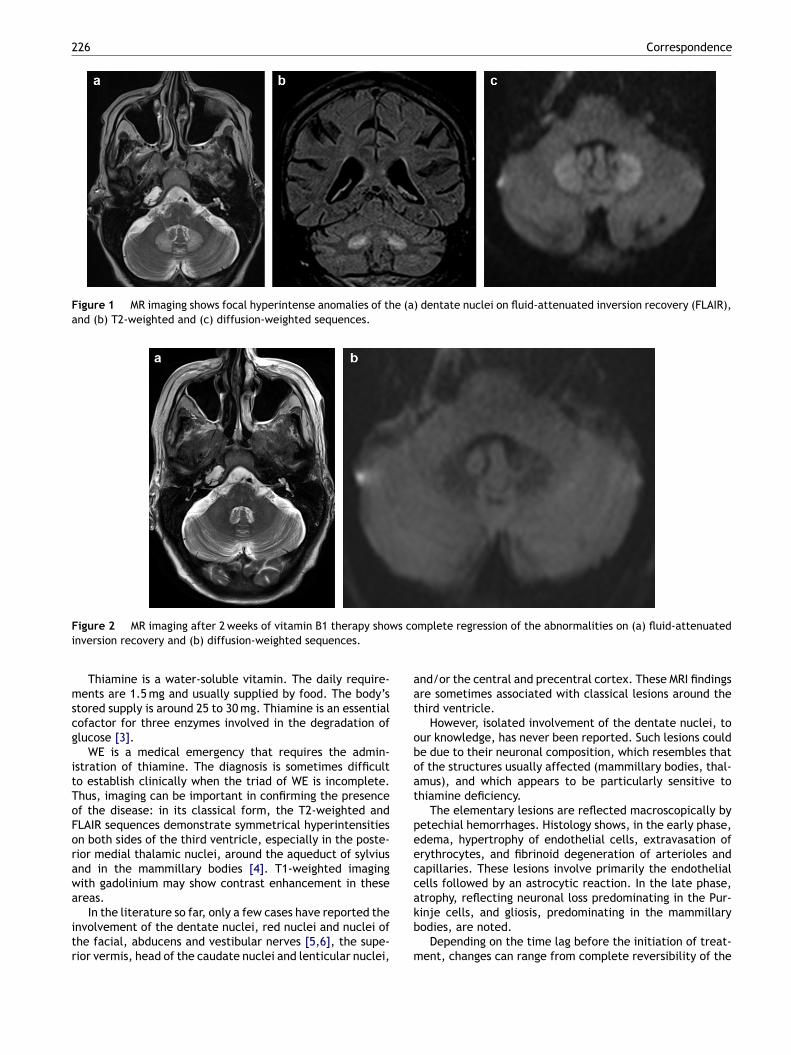
The patient received treatment with vitamin B1 intra-enously for 3 days, and oral administration of B1 at00 mg/day thereafter. MR imaging 2 weeks later showedomplete regression of the abnormalities (Fig. 2a, b). Theatient improved clinically with partial regression of herymptoms.
Wernicke’s encephalopathy (WE), first described byernicke in 1881 [1], is related to vitamin B1 (thiamine)eficiency. The disease is characterized by a classical triadf symptoms [2] found in 30% of cases, including mental dis-rders such as confusion, apathy and hypersomnia (80% ofases), oculomotor disturbances such as nystagmus and ocu-omotor palsy (93% of cases), and balance disorders (76% ofases).
Vitamin B1 deficiency arises most often in alcoholic
s prolonged intravenous feeding, anorexia, malnutrition,rolonged fasting (hunger strike), chronic vomiting andecovery (recharging) without vitamin therapy [2].
Figure 1 MR imaging shows focal hyperintense anomalies of the (a) dentate nuclei on fluid-attenuated inversion recovery (FLAIR),and (b) T2-weighted and (c) diffusion-weighted sequences.
F ws coi
mscg
itToForawa
itr
aat
oboat
peeccak
igure 2 MR imaging after 2 weeks of vitamin B1 therapy shonversion recovery and (b) diffusion-weighted sequences.
Thiamine is a water-soluble vitamin. The daily require-ents are 1.5 mg and usually supplied by food. The body’s
tored supply is around 25 to 30 mg. Thiamine is an essentialofactor for three enzymes involved in the degradation oflucose [3].
WE is a medical emergency that requires the admin-stration of thiamine. The diagnosis is sometimes difficulto establish clinically when the triad of WE is incomplete.hus, imaging can be important in confirming the presencef the disease: in its classical form, the T2-weighted andLAIR sequences demonstrate symmetrical hyperintensitiesn both sides of the third ventricle, especially in the poste-ior medial thalamic nuclei, around the aqueduct of sylviusnd in the mammillary bodies [4]. T1-weighted imagingith gadolinium may show contrast enhancement in thesereas.
In the literature so far, only a few cases have reported the
nvolvement of the dentate nuclei, red nuclei and nuclei ofhe facial, abducens and vestibular nerves [5,6], the supe-ior vermis, head of the caudate nuclei and lenticular nuclei,
b
m
mplete regression of the abnormalities on (a) fluid-attenuated
nd/or the central and precentral cortex. These MRI findingsre sometimes associated with classical lesions around thehird ventricle.
However, isolated involvement of the dentate nuclei, tour knowledge, has never been reported. Such lesions coulde due to their neuronal composition, which resembles thatf the structures usually affected (mammillary bodies, thal-mus), and which appears to be particularly sensitive tohiamine deficiency.
The elementary lesions are reflected macroscopically byetechial hemorrhages. Histology shows, in the early phase,dema, hypertrophy of endothelial cells, extravasation ofrythrocytes, and fibrinoid degeneration of arterioles andapillaries. These lesions involve primarily the endothelialells followed by an astrocytic reaction. In the late phase,trophy, reflecting neuronal loss predominating in the Pur-inje cells, and gliosis, predominating in the mammillary
odies, are noted.
Depending on the time lag before the initiation of treat-ent, changes can range from complete reversibility of the
[
[
Correspondence
disorders to motor sequelae, Korsakoff’s syndrome, comaand death.
Knowing the MRI signs of WE, even the atypicalones, can help to make the diagnosis and prompt treat-ment with vitamin B1, thereby avoiding any emergencycomplications.
Disclosure of interest
The authors declare that they have no conflicts of interestconcerning this article.
References
[1] Wernicke C. Lehrbuch der Gehirnkrankheiten für Aerzete undStudierende. 2 Berlin: Theodor Fischer; 1881.
[2] Vargas MI, Lenz V, Bin JF, Bogorin A, Abu Eid M, Jacques C, et al.Brain MR imaging of chronic alcoholism. J Radiol 2003;84(4 Pt1):369—79.
[3] Gardian G, Voros E, Jardanhazy T, Ungrean A, Vescsei L.Wernicke’s encephalopathy induced by hyperemesis gravi-
darum. Acta Neurol Scand 1999;99:19—98.
[4] Ohara N, Narita F, Kayama C, Goto Y. Wernicke’s encepha-lopathy associated with hyperemesis gravidarum. Hosp Med2003;64:371.
h
227
5] Kuang-Chung L, Shu-Fan K, Lu-An C. Wernicke’s encephalopathywith atypical magnetic resonance imaging: case report. Am JEmerg Med, in press.
6] Bae SJ, Lee HK, Choi CG, Suh DC. Wernicke’s encephalopathy:atypical manifestation at MR imaging. AJNR Am J Neuroradiol2001;22(8):1480—2.
Hakim Zourdania
Ibtihal Hamyaa
Victor Cuvinciucb
Karl Lovbladb
Maria Isabel Vargasb,∗a Service de radiologie, Hôpitaux Universitaires et
Université de Genève, 1211 Genève 14, Switzerlandb Service de neuroradiologie, Hôpitaux Universitaires etUniversité de Genève, 4, Gabrielle-Perret-Gentil, 1211