Denver Public Health Center for Public Health Preparedness Public Health Services Research, Moving to the Mainstream Public health performance and quality improvement, one state’s experience A. Davidson, MD, MSPH AcademyHealth, Annual Research Meeting Hynes Convention Center Boston, MA June 26, 2005
Transcript
Denver Public Health Center for Public Health Preparedness
Public Health Services Research, Moving to the Mainstream
Public health performance and quality improvement, one state’s experience
A. Davidson, MD, MSPH AcademyHealth, Annual Research Meeting
Hynes Convention CenterBoston, MA
June 26, 2005
• Historical context• Current efforts
Outline
• Historical context
• CO Health Data Advisory Committee (CoHDAC)• Colorado PH Education Committee• CO PH Capacity Building Steering Committee• Denver Center for Public Health Preparedness• Public Health Performance Improvement Collaborative
(PH-PIC)
Outline
Colorado Health Data Advisory Committee (CoHDAC)
Vision: Access to health data on as needed basis with an analytic toolset to generate information.
Result• [1994-present] created a competent, committed,
collaborative (local/state) problem-solving group• [1995] Colorado Health Information Dataset
(CoHID) CD-version, Weld County
• [1998 – present] Colorado Health Information Dataset (CoHID) on-line SAS IntrNet query tool (CDPHE), GIS capacities
Colorado PH Education CommitteeCharge: Create a strategy for improving education and training of
Colorado’s PH workforce.
Results• [April 2001] Colorado PH Professional Education Plan: Life-long
survey) to set training priorities by gauging: • How important a skill area was to job,• How prepared staff felt in each skill area, and• What interest existed around training
• [2004] Implementation CO-TRAIN, (PHF)
CO PH Capacity Building Steering Committee
Charge: Workforce development was only a part of PH essential services delivery capacity; convened committee to create a strategy for enhancing Colorado’s capacity to do PH work.
Result• [2001] The committee recommended the use of the
NPHPS. – Post Sept 11, 2001, enabled NPHPS assessment
funding.
– OLL coordinated implementation of NPHPS assessment
• [February 2003]. NPHPS study completed for Colorado
Denver Center for Public Health Preparedness (CDC-funded Advanced Practice Center )
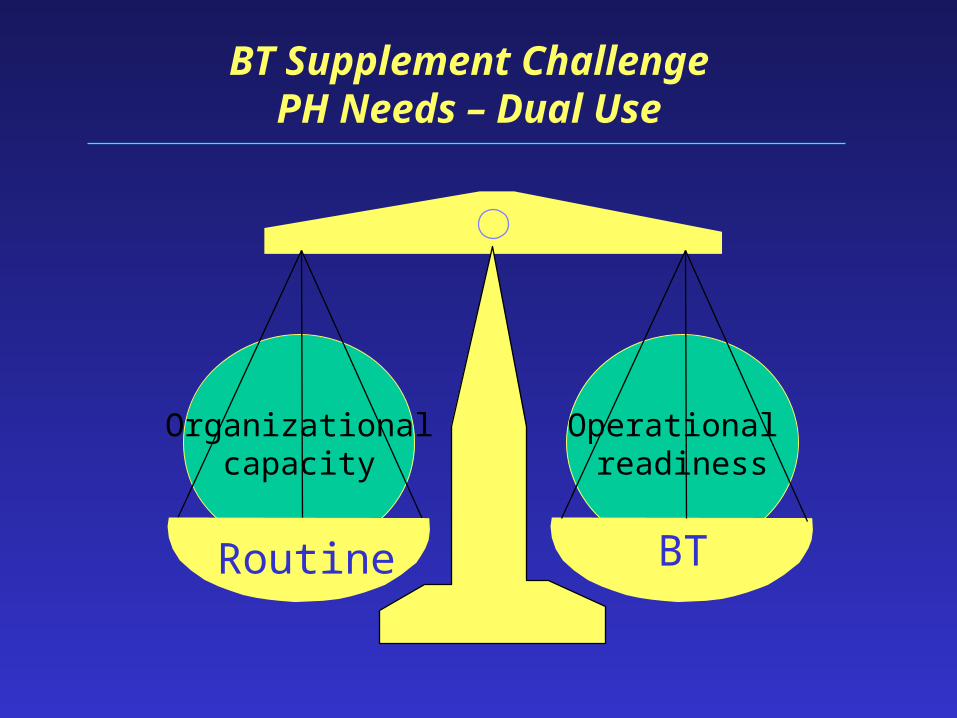
Mission: to…enhance operational readiness…• dual use perspective, operational readiness related to organizational capacity
• parallel skills for BT readiness and routine ES capacities
• operates at organizational or system level– PH community had individual readiness competencies (Columbia SON)
Issues:• Have we defined organizational competencies? How are they measured? Are they
being used? How would combined (individual and organizational) competency measures better evaluate our essential services delivery or BT readiness capacities?
Operational readiness
Organizationalcapacity
BT Supplement ChallengePH Needs – Dual Use
Routine BT
Denver Center for Public Health Preparedness (cont.)
Result: [June 2003, Conference ] Started the QI Collaborative
Goals:• Cultivate within Colorado’s PH community a culture of learning and QI• Facilitate PH quality improvement, capacity building and all hazards
preparedness in CO
Members: representatives of local/state public health departments (e.g., OLL, data, QI, academics)
Merger: QI Collaborative & the Capacity Building Steering Committee (2003).
• Articulated a new group identity (mission, vision and new name: PH-PIC).
Public Health Performance Improvement
Collaborative (PH-PIC)
• What is PH-PIC?: A workgroup from local/state health departments which adapts national initiatives to expand and improve local public health performance and all-hazards preparation and capacity.
• PH-PIC Premise: The process of setting priorities for performance improvement and all-hazards preparation should be driven by current Colorado data.
Merger: QI Collaborative & the Capacity Building Steering Committee (2003).
• Articulated a new group identity (mission, vision and new Articulated a new group identity (mission, vision and new name: name: PH-PICPH-PIC).).
• Analyzed and distributed the NPHPS Colorado results and other assessment data.
NPHPS Opportunities for Colorado
• To use results to improve public health practice and the public health system performance as a whole
• To provide a foundation for continuous quality improvement activities
• Encourages stakeholder communication and collaboration
– Promotes greater understanding of the available capacity and resources within a region
– Promotes the development of new and/or stronger partnerships
Very importantProportion being metQI in next 12 months
Workforce Proficiency (SON Survey)
Office of Local Liaison Colorado DPHE2
6872
50
70
48
68
5450
54
37
31
45
30
46
25
41 40
22
0
20
40
60
80
Pe
rce
nt
Proportion being met Proficiency
NPHPS Priority Matrix
Mon
itor
Dia
gnos
is
Ed
uca
te
Par
tner
shi
p
Pol
icy
En
forc
e
Lin
k
Wor
kfo
rce
Eva
luat
ion
Res
earc
h
< 50% of model (locally) X X X X < 50% of model (state) X X X X X Rated most important X X X > 50% intend QI in 1 year X X X X Greatest discrepancy: importance vs. model
X X X X
Indicators < 50% (locally) X X X X X X Indicators < 50% (state) X X X X X X X X < 30% of local work force highly proficient
X X X
Merger: QI Collaborative & the Capacity Building Steering Committee (2003).
• Articulated a new group identity (mission, vision and new Articulated a new group identity (mission, vision and new name: name: PH-PICPH-PIC).).
• Analyzed and distributed the NPHPS Colorado results and Analyzed and distributed the NPHPS Colorado results and other assessment data.other assessment data.
• Created a BT-focused training opportunity in Feb 2004 to learn QI/PI process and use the NPHPS data.
Denver Public Health Department
Performance topics: • Emergency notification system
• System to divert workforce to function in specific emergency response roles, while maintaining core public health functions
• Selection of sites for dispensing mass vaccinations/prophylaxis
Denver Public Health Department
Performance topic: • Emergency notification system
How decided is important:• Contractual obligation (BT preparedness)• No current system
Specific aim or purpose:• Develop an alert/notification system• Inform PH workforce of roles/responsibilities• Insure a functioning system
Desired outcome or target improvement:• 100% of employees aware of emergency number• 98% of employees contacted within 24 hours• 100% of contacted employees follow emergency
notification procedures• Quarterly test of efficiency system
Denver Public Health Department: 2/11/04
Number:149
101 (68)98 (97)48 (32)
34 (23)1.2
2.2 hrs3.1 hrs.
3723
Results: • Total employees
• Employees contacted• Performed action
• Employees not contacted
• Employees beneath 1 caller • Mean contacts per employee• Mean time to contact• Mean time to return call• No. corrected phone numbers• No. of alternative numbers
Merger: QI Collaborative & the Capacity Building Steering Committee (2003).
• Articulated a new group identity (mission, vision and new Articulated a new group identity (mission, vision and new name: name: PH-PICPH-PIC).).
• Analyzed and distributed the NPHPS Colorado results and Analyzed and distributed the NPHPS Colorado results and other assessment data.other assessment data.
• Created a BT-focused training opportunity in Feb 2004 to Created a BT-focused training opportunity in Feb 2004 to learn QI/PI process and use the NPHPS data. learn QI/PI process and use the NPHPS data.
• Presented PH-PIC methods, activities & the “Primer on PH-PI” at CPHA (September 2004).
Quality Improvement
• What are we trying to accomplish?
• How will we know that a change is an improvement?
• What changes can we make that will result in an improvement?
Four Steps of Improvement (IHI Model)
• Plan
• Do
• Study
• Act
Plan
Study Do
Act
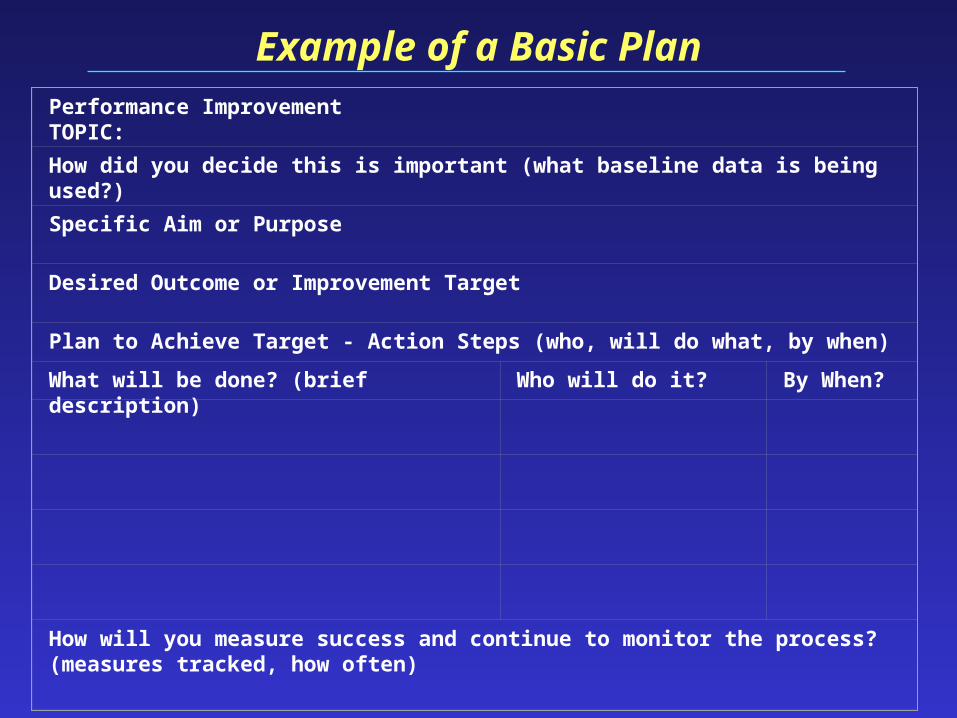
Performance Improvement TOPIC:
How did you decide this is important (what baseline data is being used?)
Specific Aim or Purpose
Desired Outcome or Improvement Target
Plan to Achieve Target - Action Steps (who, will do what, by when)
What will be done? (brief description) Who will do it? By When?
How will you measure success and continue to monitor the process? (measures tracked, how often)
Example of a Basic Plan
Repeated Use of the Cycle
Pla
n
Stu
dy
Do
Act
Plan
StudyDo
Act
Plan
Stud
yD
o
Act
Plan
Study Do
Act
DATA
Hunches, theories, ideas
Changes that result in
improvement
Denver Public Health Department: 6/24/04
Number:11
11 (100)--0
--1
NA4.1 hrs.
----
Results: • Total employees
• Employees contacted• Performed action
• Employees not contacted
• Employees beneath 1 caller • Mean contacts per employee• Mean time to contact• Mean time to return call• No. corrected phone numbers• No. of alternative numbers
Merger: QI Collaborative & the Capacity Building Steering Committee (2003).
• Articulated a new group identity (mission, vision and new Articulated a new group identity (mission, vision and new name: name: PH-PICPH-PIC).).
• Analyzed and distributed the NPHPS Colorado results and Analyzed and distributed the NPHPS Colorado results and other assessment data. other assessment data.
• Created a BT-focused training opportunity in Feb 2004 to Created a BT-focused training opportunity in Feb 2004 to learn QI/PI process and use the NPHPS data. learn QI/PI process and use the NPHPS data.
• Presented PH-PIC methods, activities & the “Primer on PH-Presented PH-PIC methods, activities & the “Primer on PH-PI” at CPHA (September 2004).PI” at CPHA (September 2004).
• Created the “Colorado Public Health Performance Improvement Plan”. http://www.cdphe.state.co.us/as/ollhom.asp
• Diagnosing– 29 local system plans– 5 state system plans
• Evaluating– 12 state system plans– 5 local system plans
• 39 local and state plans targeted All-Hazards
PH-PIC Assessment (Fall 2004/Winter 2005)
• Clustering of PI priorities • Results of NPHPS matrix
Should Learning Communities be developed to support quality improvement/ performance improvement in Colorado’s Public Health systems?
• Current efforts• Learning communities• Regional Health Information Organization
(RHIO)
Outline
• Hear and log our stories• Recognize common statewide issues• Work to define and solve problems • Assure dual purpose/use of our efforts• Consider developing a learning community • Use as opportunity to guide new BT supplemental
planning process
What might we accomplish today?
June 2, 2003
Learning Community
“Learning communities are developed where groups of people, linked geographically or by shared interest, collaborate and work in partnership to address their members’ learning needs… Learning communities facilitated through adult and community education are a powerful tool for social cohesion, community capacity building and social, cultural and economic development.”
Department of Education, 2003, p 12.
Barriers to Organizational Learning
• Silo style of work and work groups• Unsupportive leadership• Lack of legitimacy• Failure to build in time and structures for
learning• Defensive communication patterns• Limited ability for reflection and generative
learning• Lack of the 6 “C’s” in group members
What It Takes to Create and Sustain A Learning Community
• Capability: have the skills, knowledge and personal qualities to renew themselves and reinvent a future through skillful discussion
• Commitment: people are an integral part of creating a community they value together
• Contribution: members must see how their work contributes to community; provide opportunities for diversity of talents and contributions
(Brown and Isaacs, Fifth Discipline Fieldbook, 1994, p 508-517)
Creating and Sustaining Learning Communities (cont.)
• Continuity: develop an institutional memory, careful orientation of new members
• Collaboration: develop interdependence, share vision and strategy, free flow of information, able to act autonomously to achieve common goals
(Brown and Isaacs, Fifth Discipline Fieldbook, 1994, p 508-517)
PUBLIC HEALTH PERFORMANCE IMPROVEMENT COLLABORATIVE
Title: Demonstrating success: User-friendly evaluation for public health programs
Learning objectives• Increase familiarity with useful evaluation terminology.• Identify evaluation resources.• Practice using basic evaluation skills
Short DescriptionThis user-friendly, interactive workshop will allow participants to gain
knowledge and skills to demonstrate the success of their programs. Commonly used evaluation processes and resources will be presented with opportunities for practice.
EVALUATION LEARNING COMMUNITY
CPHA Abstract Draft – June 3, 2005
• Initiating work around cataloguing available data sources and identifying data gaps.
• Adjunct work by Colorado Health Information Exchange
MONITORING LEARNING COMMUNITY
Goal: Create a local health information infrastructure for clinicians to access patient information across individual health care institutions
Colorado Health Information Exchange 2 Complementary Initiatives
Build upon what exists• Denver Health (DH)
• 150,000 residents (25% of population)
• Kaiser Permanente of Colorado (KPC)• 3rd largest CO HMO (350,000 members)
• The Children’s Hospital (TCH)• Largest pediatric specialty care provider
• University of Colorado Hospital (UCH)• Largest Metro area teaching hospital
COHIE to CORHIO
COHIE
Learning
Laboratory
Steering Committee
Working groups:• Technical• Clinical• Evaluation• Legal• Organizational
Community Advisory Council
Colorado Regional Health Information Organization
A sharing, self-sustaining non-profit structure that:
Promotes legal
agreements for
participation and access
Maintains a robust
technical environment
Defines clinical value
through policy and procedures
Manages the budget and
sustainable business
model
Supports national
standards and public
health interfaces
PROJECT
(10/2004)
VISION
(10/2009)
COHIE: 2005 plan
COHIE: Linking independent clinical data into a “virtual” patient-centered view
1. Accountable and OPEN participation
2. Clinical data sharing between different platforms
3. Data sharing and degree of participation remains under local control
Mesa County
The Children’s Hospital
Boulder
Larimer
Weld
Denver Health
El Paso County
MedSouth IPA University Hospital
Kaiser Permanente
Exempla
Rose Medical Group
Colorado Care Collaborative (RMD)
Payor # 1 – RMHP ???
RxHub ???
COHIE:
“Community” patient index
common (standard) messaging
Vendor independent (neutral)
Rural small MD access ?
CHCN - Health Center?
Clinical Data Contributor TBD ?
CORHIO Process
• Colorado Health Institute (neutral convener)• Legal support • Explore/define relationship COHIE ⇔ CORHIO• Working Group
• Business plan
• Articles of incorporation (501c3)
• Defining the board
• Education/public relations
• Community Advisory Council (greater than 40 members, most HIT projects going on in Colorado
Future activities/use cases
• Public Health • Registries and evaluation of care quality• Active surveillance due to recent events• Immunization tracking and reminder/recall• Others ??
• Use of global-level decision support• Continuity of care record (CCR) for effective
care transitions (acute -> treatment centers -> home)
• Patients controlling EHR access
Conceptual Framework
State/Local Partnerships
Leadership Development
Performance Improvement
If the conceptual work is successful,
we should focus on….
And if true leaders emerge,
we should generate ….
Then partners will agree to emphasize…
And then tools/methods and measures will evolve to
support/revise the…
COLORADO TEAM - VISUAL MODELNational Public Health Leadership Institute
Draft V1.1, June 20, 2005
• 10 Essential Services• Clear PH message
• Systems thinking• Change management
• Respectful relations• Inclusive planning
• Accountability targets• Unified measurement process