KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
i
Inherent Limitations
This report has been prepared as outlined in the Scope Section. The services provided in connection with this engagement comprise an advisory engagement, which is not subject to assurance or other standards issued by the Australian Auditing and Assurance Standards Board and, consequently no opinions or conclusions intended to convey assurance have been expressed.
The findings in this report are based on a qualitative study and the reported results reflect a perception of stakeholders but only to the extent of the sample surveyed, being Defence and Department of Veterans’ Affairs nominated representative sample of stakeholders. Any projection to the wider service provider/ stakeholder community is subject to the level of bias in the method of sample selection.
No warranty of completeness, accuracy or reliability is given in relation to the statements and representations made by, and the information and documentation provided by stakeholders consulted as part of the process.
KPMG have indicated within this report the sources of the information provided. We have not sought to independently verify those sources unless otherwise noted within the report.
KPMG is under no obligation in any circumstance to update this report, in either oral or written form, for events occurring after the report has been issued in final form.
The findings in this report have been formed on the above basis.
Third Party Reliance
This report is solely for the purpose set out in the Scope Section and for Commander Joint Health’s (CJHLTH) information, and is not to be used for any other purpose or distributed to any other party without KPMG’s prior written consent.
This report has been prepared at the request of CJHLTH in accordance with the terms of KPMG’s engagement letter/contract/official order dated 20 July 2010. Other than our responsibility to CJHLTH, neither KPMG nor any member or employee of KPMG undertakes responsibility arising in any way from reliance placed by a third party on this report. Any reliance placed is that party’s sole responsibility.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Document review and approval
Revision history Version Author Date Revision 0.1 N Moore Initial draft 0.2 N Moore 12 Oct 2010 Second draft 0.3 N Moore 8 Nov 2010 Third draft 0.4 N Moore 12 Nov 2010 Forth draft following Working Group feedback 0.5 N Moore 18 Nov 2010 Fifth draft following Working Group feedback 0.6 N Moore 30 Nov 2010 Sixth draft 1.0 N Moore 16 Dec 2010 Final
This document has been reviewed by Reviewer Date reviewed
1 SIIP Working Group 8 Nov 2010 onwards 2 KPMG Partner Review 1 10 Nov 2010 3 KPMG Partner Review 2 12 Nov 2010 onwards 4 SIIP Project Steering Group 12 Nov 2010 onwards 5 KPMG Partner Review 3, SIIP Project Steering Group, SIIP Working Group 29 Nov 2010 onwards
This document has been approved by Subject matter experts Name Signature Date reviewed
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
2 REPORT SUMMARY ...................................................................................................................... 6 2.1 SUPPORT FOR INJURED OR ILL PROJECT ...................................................................................... 6 2.2 SIIP PURPOSE .............................................................................................................................. 6 2.3 SIIP SCOPE .................................................................................................................................. 6 2.4 WORKING WITH THIS DOCUMENT ................................................................................................ 7 2.5 SIIP ENGAGEMENT APPROACH .................................................................................................... 7 2.6 ANALYSIS FRAMEWORK ............................................................................................................ 14 2.7 RECOMMENDATIONS - C: HOW WILL WE GET THERE? ............................................................... 22 2.8 NEXT STEPS - D: WHAT ELSE NEEDS TO BE DONE? .................................................................... 23
3 RECOMMENDATIONS AND SUGGESTED INITIATIVES ................................................... 24 3.1 SIIP RECOMMENDATIONS .......................................................................................................... 24 3.2 REC 1: SYSTEM OWNER AND PROGRAM OF WORK ...................................................................... 30 3.3 REC 2: MEMBER SUPPORT FRAMEWORK .................................................................................... 31 3.4 REC 3: MANAGE INFORMATION. PERSONALISE CONTENT .......................................................... 39 3.5 REC 4: INFORMATION TECHNOLOGY AS AN ENABLER ............................................................... 42 3.6 REC 5: SIIP GOVERNANCE ........................................................................................................ 44 3.7 REC 6: EFFICIENCY .................................................................................................................... 45 3.8 REC 7: POLICY DEVELOPMENT .................................................................................................. 47 3.9 REC 8: AWARENESS .................................................................................................................. 48 3.10 REC 9: GUIDANCE ..................................................................................................................... 49 3.11 REC 10: OTHER GAPS AND ISSUES ............................................................................................. 50
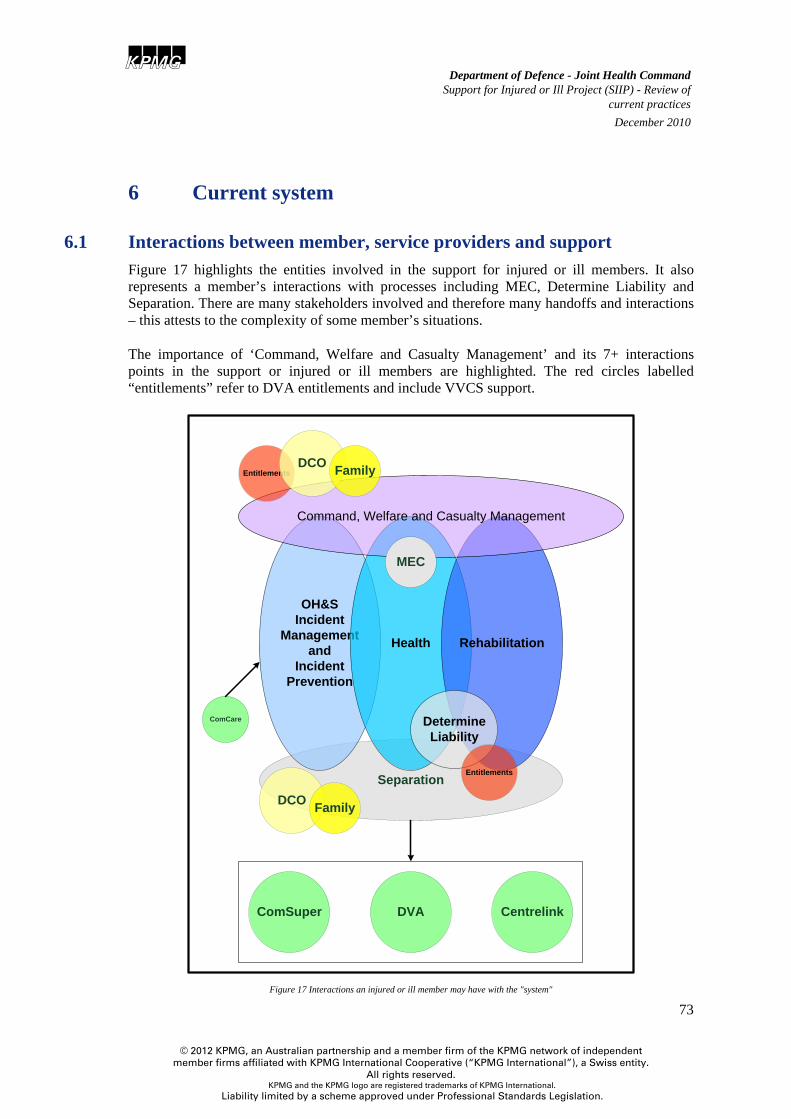
6 CURRENT SYSTEM ...................................................................................................................... 73 6.1 INTERACTIONS BETWEEN MEMBER, SERVICE PROVIDERS AND SUPPORT .................................... 73 6.2 DESCRIPTION OF THE “SYSTEM” ................................................................................................ 74
7 AVAILABLE SUPPORT ............................................................................................................... 76 7.1 GARRISON HEALTH OPERATIONS BRANCH ............................................................................... 78 7.2 DIRECTORATE OF ADF MENTAL HEALTH, PSYCHOLOGY AND REHABILITATION (DMHPR) ... 78 7.3 ADF MENTAL HEALTH STRATEGY (ADFMHS) ....................................................................... 82 7.4 ADF TRANSITION SERVICES ..................................................................................................... 84 7.5 DEFENCE COMMUNITY ORGANISATION (DCO) ......................................................................... 86
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7.6 DEPARTMENT OF VETERANS’ AFFAIRS (DVA) ......................................................................... 87 7.7 TRANSITION MANAGEMENT SERVICE (TMS) (DVA) ................................................................ 91 7.8 VVCS - VETERANS AND VETERANS FAMILY COUNSELLING SERVICE (VVCS) ........................ 91 7.9 DEFENCE HOUSING AUSTRALIA (DHA) .................................................................................... 95 7.10 AUSTRALIAN CENTRE FOR POST-TRAUMATIC MENTAL HEALTH (ACPMH) ............................ 95 7.11 CHAPLAINS/ PADRES ................................................................................................................. 96 7.12 NATIONAL WELFARE COORDINATION CENTRE (NWCC) .......................................................... 96 7.13 ALL-HOURS SUPPORT LINE (ASL) ............................................................................................ 96 7.14 1800 IMSICK ........................................................................................................................... 96 7.15 EMERGENCY SUPPORT FOR FAMILIES SCHEME (ESFS) ............................................................. 96 7.16 OPERATION CARE .................................................................................................................... 96 7.17 AUSDIL ................................................................................................................................... 97 7.18 DEFENCE SCHOOL TRANSITION AIDE (DSTA) AND DEFENCE TRANSITION MENTOR (DTM) ... 97 7.19 TRADE TRANSFER AND RETENTION .......................................................................................... 97
8 LOCAL/ REGIONAL/ SERVICE INITIATIVES ....................................................................... 98 8.1 CASUALTY MANAGEMENT, CLAIMS ASSISTANCE AND COMPLEX CASE MANAGEMENT ........... 98 8.2 ARMY PERSONNEL COORDINATION DETACHMENTS................................................................ 110 8.3 PROJECT AKESA .................................................................................................................... 112 8.4 WOUNDED DIGGERS FORUM ................................................................................................... 112 8.5 TRANSITION CASE MANAGER – SECTION 64 MRCA ................................................................ 113 8.6 PROJECT WARRIOR WELFARE – SOCAUST ........................................................................... 114 8.7 CASE CONFERENCES – LAVARACK BARRACKS ........................................................................ 115 8.8 DEPLOYMENT SUPPORT BOOKLET .......................................................................................... 115 8.9 RE-INTEGRATION BOOKLET .................................................................................................... 115 8.10 FAMILY CARE PLAN (FCP) ..................................................................................................... 115 8.11 GENERATING AC563 - ARMY .................................................................................................. 116 8.12 HOW ARE YOU TRAVELLING? PROJECT .................................................................................... 116
9 PROJECTS AND INITIATIVES WHICH AFFECT OR IMPACT ON SIIP ........................ 117 9.1 CURRENT PROJECTS AND SUB-PROJECTS WITH SIIP IMPACTS .................................................. 117 9.2 COMPLETED PROJECTS WITH SIIP IMPACTS ............................................................................. 137
10 GOVERNANCE, REPORTING AND FEEDBACK ............................................................. 142 10.1 CURRENT GOVERNANCE ARRANGEMENTS .............................................................................. 142 10.2 CURRENT FEEDBACK MECHANISMS ......................................................................................... 144
11 CONTEMPORARY PRACTICE OVERVIEW .................................................................... 148 11.1 COMCARE STRATEGIC PLAN 2010-2015 ................................................................................. 161 11.2 TRANSITION MENTAL HEALTH AND FAMILY COLLABORATIVE (TOWNSVILLE) ...................... 162 11.3 DEFENCE MILITARY REHABILITATION CENTRE (DMRC), HEADLEY COURT UK ................... 162 11.4 VETERANS’ AFFAIRS CANADA (VAC) REHABILITATION PROGRAM (RP) ............................... 163 11.5 PRIMARY CARE PARTNERSHIPS ............................................................................................... 163 11.6 AUSTRALIA POST - REHABILITATION MANAGEMENT SYSTEM ................................................ 164
12 STAKEHOLDER CONSULTATION .................................................................................... 165 12.1 POSITIVES................................................................................................................................ 165 12.2 GAPS AND ISSUES .................................................................................................................... 167 12.3 GAPS AND ISSUES IDENTIFIED - NOT WITHIN SCOPE OF THE SIIP REVIEW ................................ 191
A ENGAGEMENT TERMS OF REFERENCE ............................................................................ 195
B PROCESS MAPS .......................................................................................................................... 198
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
v
C CONTEMPORARY PRACTICE EXAMPLES AND CASE STUDIES .................................. 218
D STAKEHOLDER ENGAGEMENT ............................................................................................ 225
E GLOSSARY AND ACRONYMS ................................................................................................. 230
F FORMS .......................................................................................................................................... 239
G POLICIES, INSTRUCTIONS AND PROCEDURES ............................................................... 241
H LEGISLATION ............................................................................................................................. 245
I TMS ROLES – DEFENCE AND DVA ....................................................................................... 246
J MEC CLASSIFICATION PROJECT – ADDITIONAL INFORMATION ............................ 250
K DUNT RECOMMENDATION – DVA PROGRESS AS AT JUNE 2010 ................................ 252
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Figure 1 Key system interactions - Support for injured or ill members ........................................ 8Figure 2 Initiatives and projects influencing support for injured or ill members ........................ 11Figure 3 Analysis framework – ABCD ....................................................................................... 14Figure 4 Analysis framework - A: Where are we now? .............................................................. 15Figure 5 Analysis framework - B: Where do we want to be? ..................................................... 21Figure 6 Analysis framework - C: How will we get there? ......................................................... 22Figure 7 Analysis framework - D: What else needs to be done? ................................................ 23Figure 8 SIIP recommendations - how they relate to a member, stakeholders and enablers ...... 28Figure 9 Case coordination responsibilities within the Member support framework ................. 33Figure 10 Member Support framework – based on complexity of member’s situation .............. 34Figure 11 Member Support framework for a "complex" member situation ................................ 35Figure 12 Indicative triggers for entry into the Member Support framework ............................. 37Figure 13 Activities required to manage knowledge and personalise content ............................ 40Figure 14 Personalised content is pushed to an injured or ill member ........................................ 41Figure 15 Personalised content pushed to an injured member, family and Command ............. 41Figure 16 Information technology - simple workflow example .................................................. 43Figure 17 Interactions an injured or ill member may have with the "system" ............................ 73Figure 18 Key systems relevant to the support provided to injured or ill members .................... 74Figure 19 Australian Defence Force Rehabilitation Program Service Delivery Framework ...... 80Figure 20 CAS-O Organisation structure .................................................................................. 105Figure 21 Navy Complex Case Management Cell .................................................................... 108Figure 22 RAAF Complex Claims Liaison Office .................................................................... 110Figure 23 Army Personnel Coordination Detachment locations – March 2011 ....................... 112Figure 24 Representation of key projects (and milestones) having the capacity to influence support for injured or ill members ............................................................................................. 119Figure 25 JeHDI core user requirements ................................................................................... 124Figure 26 Support for injured or ill - current Governance arrangements and feedback mechanisms ............................................................................................................................... 146Figure 28 Overview of the key systems and processes in the support of injured or ill ADF members .................................................................................................................................... 149
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
1
Table 1 Mapping between desired end state and recommendations to address gaps and issues . 29Table 2 ADF Average Funded Strength - extracted from Defence Annual Reports ................... 57Table 3 MEC classification of ADF AFS - 30 Jun 2010 ............................................................ 58Table 4 MEC classification of ADF AFS at 30 Jun 2009 ........................................................... 58Table 5 Lodgement of AC563Incident Notification Forms - by entity ....................................... 59Table 6 Average time taken to lodge AC563 Incident Notification - by incident type ............... 60Table 7 Rehabilitation referrals - FY2005-06 to FY 2009-10 ..................................................... 61Table 8 Closed rehabilitation cases – by Service and goal – 2009/10 ........................................ 62Table 9 Closed rehabilitation cases – by Service and ADFRP Closure Outcome – 2009/2010 . 63Table 10 Top 5 injuries – by Service – 2009/10 ......................................................................... 63Table 11 DVA clients by type at 30 Jun 2010 ............................................................................ 64Table 12 VEA beneficiaries by age - as at 30 June 2010 ............................................................ 65Table 13 MRCA and SRCA beneficiaries who received benefits in the two years to Jun 2010 66Table 14 Claim processing times - actual vs. target, for FY 2009/10 ......................................... 67Table 15 Undecided MRCA primary claims by age at 30 Jun 2008, 2009 and 2010 ................. 67Table 16 ADF separation figures, by Service for FY 2005-6 to 2008-09 .................................. 69Table 17 Separation breakdown - by Service .............................................................................. 70Table 18 Separation Reason FY 2009/10 - by Service ............................................................... 71Table 19 Separation Reasons FY 2008/09 - by Service .............................................................. 72Table 20 Support Services available to ADF members and their families ................................. 77Table 21 Service Casualty, Claims and Complex Case Management features ........................ 102Table 22 Services provided through Service casualty management frameworks ..................... 104Table 23 Initiatives which influence and enhance support provided to injured or ill members 118Table 24 SAM Requests for the period Jul to Sep 2010 ........................................................... 132Table 25 Overview of contemporary practice in the management of ill or injured members ... 160Table 26 MECRBs by Service for FY 09/10 ............................................................................ 179Table 27 Duration MSU to action ............................................................................................. 181Table 28 Duration MSU action as percentage .......................................................................... 181Table 29 To MECRB Duration ................................................................................................. 182Table 30 To MECRB Duration as a percentage ........................................................................ 182Table 31 MECRB Determination duration ............................................................................... 182Table 32 MECRB Determination by percentage ...................................................................... 183Table 33 Process: Occupational Health and Safety .................................................................. 200Table 34 Process: Incident, presentation of injury or illness .................................................... 201Table 35 Process: Primary Healthcare and Treatment .............................................................. 203Table 36 Process: Rehabilitation ............................................................................................... 205Table 37 Process: Determine Liability/ Compensation ............................................................. 207Table 38 Process: Return to ADF Duties (MEC1 and MEC2) ................................................. 208Table 39 Process: Medical separation ....................................................................................... 210Table 40 Process: Transition ..................................................................................................... 210Table 41 Process: Superannuation ............................................................................................ 211Table 42: Proposed MEC system .............................................................................................. 251
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
3
1 Executive Summary Background
The Support for Injured or Ill Project (SIIP) Review was conducted between August and December 2010. It included a gap analysis of Defence, single Service and Department of Veterans’ Affairs (DVA) incident reporting, welfare, health care, rehabilitation, compensation and transition policies, processes and services. This was informed by significant stakeholder consultation at Defence locations around Australia, a Project Working Group and Project Steering Committee, a literature review of contemporary practice in Defence, relevant Government Agencies and Private sector entities and consideration of relevant reviews, existing process maps, policies and procedures.
Current support system
The system supporting injured or ill Defence members is generally good and results in a high return to work rate for rehabilitated members. However, this review has confirmed that a more coordinated and integrated approach across welfare, rehabilitation, compensation and transition programs is likely to improve outcomes for ADF members and their families and better support command responsibilities.
There are instances where:
• Some members are falling through gaps and not receiving the support they are entitled to and/ or require.
• Some injured or ill members and their families do not feel supported by Defence.
• The current system does not always enable Defence to effectively and efficiently support its injured or ill members.
• Duplication of some services occurs and results in inefficiencies.
• Unclear roles and responsibilities lead to duplication or service and support gaps.
The need to look beyond incremental improvements
These circumstances and situations underpin the case for change. A number of initiatives are presented within the recommendations of this report that if implemented will provide improvement and contribute to a more effective and efficient member support framework.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
However, the Project Steering Group concludes that to achieve sustained improvement across the programs currently in place to support ill, injured and wounded ADF members and their families, through out their career and through transition to civilian life, these initiatives firstly require organisational commitment to and implementation of more systemic change within Defence and transformational change to a new partnership and understanding between Defence and DVA.
The Project Steering Group has determined that the review to date has delivered valuable insight and suggestions for future directions at a program level and can be considered as Phase One. The recommendations arising from Phase One of SIIP form a framework that will better meet the needs of ADF members and their families, and incorporate commanders’ welfare, personnel management and administrative responsibilities.
Requirements for transformational and system change
As the principal stakeholders, Defence and DVA are committed to ensuring the interfaces, boundaries and barriers with regard to medical separation from the ADF, workplace safety, health care, rehabilitation and compensation are identified and resolved so as ensure the resulting system is both member-centric and responsive to Command requirements.
Key changes necessary to achieve a more integrated and streamlined system will include:
• Identification of a single Defence system owner accountable for governance,
implementation and performance (including measurement of and reporting on performance);
• A member support framework which is member centric, includes a dedicated case coordinator and support tailored to the member’s needs;
• Enabling Command to better undertake its responsibilities for the welfare and management of a member;
• An efficient (shared services) tri-Service system operates where duplication of support and service provision is eliminated;
• Programs delivered within the integrated system are joined up, demonstrate evidence-based practice and are outcomes-focussed;
• Cultural, practice and system change that supports injury prevention and timely incident reporting;
• Appropriate communication and education occurs and roles and responsibilities are defined and understood;
• Improved data and information sharing within and external to Defence;
• Management information and reporting to inform decision making; and
• Technology-based solutions which enables workflow capabilities, content management and “pushing” targeted and personalised information to the member and their family and between Defence and DVA.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
5
Conclusion and next steps Phase One has delivered a gap analysis report of current Defence, single Service and DVA incident reporting, welfare, health care, rehabilitation, compensation and transition policies, processes and services compared with evidence based best practice. Recommendations relating to a framework, process map(s) and improvements that will better meet the needs of ADF members and their families, and incorporate commanders' welfare, personnel management and administrative responsibilities have also been defined during this phase. Phase Two of this project, required to be undertaken during the first 6 months of 2011, will pursue the implementation of a SIIP system (encompassing workplace safety, incident reporting, welfare, ADF health, rehabilitation, liability determination and transition). It will develop a legislative, policy, governance and systems schema within which the recommended initiatives of Phase One can be considered and outline the new partnership requirements between Defence and DVA to effectively support a coordinated and integrated approach.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
2 Report Summary
2.1 Support for Injured or Ill Project Defence has a commitment to managing the health consequences of operational service as well as providing health treatment to ill or injured personnel.
The Defence health care system is designed to prevent and minimise the impact of operational, environmental and occupational health threats and to treat ill or injured members.
The Support for Injured or Ill Project (SIIP) commenced on 2 August 2010, as a result of the Head of People Capability (HPC), Head of Defence Support Operations (HDSO) and Commander Joint Health (CJHLTH) agreeing to conduct a gap analysis against best practice of the elements of service delivery and related policy in the areas of incident reporting, welfare, health care, rehabilitation, compensation and transition.
2.2 SIIP Purpose
“Develop a seamless and integrated support process for injured or ill ADF members throughout their Service career and through transition from Defence”1
2.3 SIIP scope
.
Included in scope are all support mechanisms available to an injured or ill ADF member from the point of, or presentation of, injury or illness right through their rehabilitation and recovery process or from the point of entry to Australia where the injury or illness occurred outside Australia.
Included in scope is primary health/ clinical treatment, rehabilitation, return to ADF duties, medical separation and liability determination for members with compensable and non-compensable injuries or illness.
Whilst the importance of preventing injury or illness is recognised, consideration of this activity was excluded from scope by the SIIP Project Steering Committee during its initial meeting on 5 August 2010 due to the significant activity and reform already occurring in this space and the time limitations of the SIIP review.
Although “family” was not initially included within the SIIP terms of reference it has been included within the review – acknowledging the importance of family in the recovery and rehabilitation of an ill or injured member. The review team did not define “family” and adopted an inclusive view covering member support networks.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
7
The SIIP did not consider support systems available to non-ADF members – so does not address Australian Public Service (APS) Department of Defence employees and Defence contractors.
Also out of scope for this review is the Australian Government Mental Health Lifecycle Package, including the Lifecycle Transition Mental Health and Family Collaborative (Townsville) project and report recommendations, the in-progress mental health consultation program and the Dunt Review(s) recommendations.
2.4 Working with this document Section 1 is an Executive Summary. Section 2 provides a summary of the SIIP project including scope, approach, identified gaps and issues. Section 3 summarises the recommendations for this review. The supporting evidence and background information which informs the recommendations is contained in sections 4 through to 12.
Sections 2 and 3 will provide the reader with an overview of the SIIP project and recommendations. If further detail is required – the reader will find this in sections 4 through to 12 and in the Appendices.
2.5 SIIP engagement approach The approach used by the Review team to manage this engagement included:
• Defining the current state – processes, existing support services including those provided at a local, regional or Service level as well as Joint services, current governance, current initiatives and projects;
• Literature review of contemporary practice in the support of injured or ill members;
• Field analysis – seeking input from stakeholders involved in supporting injured or ill members;
• Using the above to inform a gap analysis and issue identification; and
• Recommendations to address gaps and issues.
2.5.1 Define current state The current state was defined through reviewing existing process maps, developing a revised end to end process map based on existing maps and input from the SIIP Working Group members, identifying existing support services, identifying current governance arrangements within Defence and between Defence and the Department of Veterans’ Affairs (DVA) and understanding current projects which have the ability to influence and/ or affect support for injured or ill members.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
2.5.1.1 Processes and systems
Review of available current system documentation culminated in the Working Group compiling a set of a high-level process maps describing the key processes and interactions, relevant legislation, applicable forms and key stakeholder and service providers involved in each process. Each of the high-level process maps is described in detail in Appendix B. Figure 1 provides a snapshot view of the key “systems’ and interactions.
Occ. Health and Safety
Injury Prevention
Illness Prevention
Incident/ Presentation
Rehabilitation
Return to ADF Duty
(MEC1 and MEC2)
Determine Liability/ Compensation
Medical Separation
Primary Healthcare/ Treatment
Key systems within Support for Injured or Ill Project (SIIP)
Superannuation
Post Separation healthcare Services:
• DVA• External
healthcare providers
• Centrelink• ComSuper
TransitionServices
Figure 1 Key system interactions - Support for injured or ill members
2.5.1.2 Existing support services
Members are able to access many support services which are provided by:
• Garrison Health Operations Branch (JHC) (including Regional Health Services);
• Directorate of ADF Mental Health, Psychology and Rehabilitation;
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
9
• Department of Veterans’ Affairs (DVA);
• Transition Management Service (TMS);
• VVCS – Veterans; and Veterans Families Counselling Service (VVCS);
• Defence Housing Australia (DHA);
• Australian Centre for Post-Traumatic Mental Health (ACPMH);
• Chaplaincy/ Padres;
• National Welfare Coordination Centre (NWCC);
• All-hours Support Line (ASL);
• 1800 IMSICK (Part of Garrison Health Operations);
• Emergency Support to Families Scheme (ESFS);
• Operation CARE (RSL);
• AUSDIL;
• Defence School Transition Aide (DSTA)/ Defence Transition Mentor (DTM); and
• Trade Transfer and Retention.
A more detailed description of the available support services for injured or ill members and their families (including eligibility criteria) is located at section 6 and includes those services provided by Defence and DVA.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
There are also a number of local/ regional and Service specific support initiatives which include:
• Casualty management, claims assistance and complex case management functions – provided through the CAS-A (Casualty Administrative Support – Army), CCM (Navy Complex Case Management) and CCLO (Air Force Compensation Claims Liaison Office) functions;
• Army Personnel Coordination Detachments (APCD);
• Project AKESA – Army;
• Wounded Diggers Forum – Army;
• Transition Case Manager – section 64 MRCA appointment for medically separating members;
• Project Warrior Welfare – SOCAUST; and
• Case conferences, deployment support, re-integration booklets and family care plans (FCP).
2.5.1.3 Current governance A description of the current governance arrangements within Defence and between Defence and DVA is found in section 9. This section includes a discussion on:
• The Defence/ DVA links Steering Committee (DLSC);
• The Interdepartmental Working Group (IWG) for Streamlining Administration of Transitioning and Former ADF members;
• The Australian Defence Force Rehabilitation Program (ADFRP) reporting framework; and
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
11
2.5.1.4 Current initiatives and projects
There are many current projects and initiatives occurring within Defence, DVA and more broadly which have the capacity to influence or inform the support provided to injured or ill members. These are summarised in the timeline below and described in more detail in section 8. The stars on the diagram represent key milestone/dates within the project or program
Dec 10 Mar 12Feb 12Jan 12Dec 11Nov 11Oct 11Sep 11Aug 11Jul 11Jun 11May 11Apr 11Mar 11Feb 11Jan 11
Transition Management Services (TMS) Contract
ADFRP – PCM to APS Roles
Simpson Assistance Package
Medical Employment Classification (MEC) changes
Interdepartmental Working Group Initiatives – Various (ongoing)
Joint eHealth Data and Information System (JeHDI)
Defence Occupational Medicine and Occupational Hygiene Capability
Garrison Health Transition Project
MRCA Review - Ongoing
Military Health Outcomes Program (MilHOP)
JP 2080 Phase 2B1 – HR Shared Service Transition Project
Single Access Mechanism – clear backlog
Occupational Health and Safety Strategy 2007-2012
Figure 2 Initiatives and projects influencing support for injured or ill members
2.5.1.5 Workforce …. at a glance
• The FY2008/09 average funded strength (AFS) of the ADF was 55,091 members. This was represented by Army – 27,833, Navy – 13,182 and Air Force – 14,066 and is an increase of 3.6% from FY 2007/08 (53,167)2
• The Medical Employment Classification (MEC) of the AFS (at 30 Jun 2010) was MEC1 – 71.1%; MEC2 – 19.9%; MEC3 – 7.7% and MEC4 – 1.2%.
.
• 12,906 AC563 Incident Notification forms were recorded for ADF members during FY 2009/10.3
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• There were 4,189 referrals into the Australian Defence Force Rehabilitation Program (ADFRP) during FY 2009/10. This was a slight increase on FY 2008/09 where there were 4,117 referrals into the ADFRP.
• An 84.1% total return to work rate was achieved for the 3,959 rehabilitation programs closed during FY 2009/10.
• For all closed rehabilitation programs - 61.4% (2,430) achieved Rehabilitation Goal 1, 1.8% (72) achieved Goal 2, 13.4% (532) were Goal 3 and 23.4% (925) did not require a rehabilitation program.
• The top 5 injury categories (tri-service) for FY 2009/10 requiring rehabilitation plans were “Other musculo-skeletal (1,172), Mental health disorders (577), Disorders of the knee (558), Disorders of the back (415) and Obesity (167).
• There were 10,789 unique clients receiving intake referrals to VVCS during FY 2009/10 and 4,610 calls were received by the after hours counselling service during the same period.
• There were 9,649 new VEA Veterans’ Income Support and Allowance claims during FY 2009-104, 16,821 primary claims for VEA Veterans’ Disability Support5, 2,589 incapacity payees under SRCA and 3,381 initial liability claims for injury received and 1,254 incapacity payees under MRCA and 3,181 initial liability claims for injury received.6
• The average claims processing times for Veterans’ Income Support and Allowances (VEA) was 43 days (target 32 days), Veterans’ Disability Support (VEA) – 70.3 days (target 75 days), Incapacity payees (SRCA) – 89 days (target 120 days) and Incapacity payees (MRCA) – 123 days (target 120 days) during FY 2009/10.
• As at Aug 2010, the average elapsed time between incident/ injury and the member submitting a claim with DVA was 1.6 years (570 days) for MRCA claims and 16.7 years (6,113) for SCRA claims.7
• There were 5,043 tri-service separations during FY 2008/09 of which 3,012 were voluntary, 825 were involuntary, 2 were age retirement and 1,204 were cadets and trainees.
8
• 13.4% of the FY 2009/10 total separations were medically unfit for further service (MUFS), 12.0% were retention not in the Service interest and 0.7% was as a result of death.
3 Caution should be used in linking OHS AC563 data to actual OHS incidents. The AC563 is principally designed as a ComCare notification form. Every incident is not captured through the AC563 process – including near misses/ dangerous occurrences. In additional, multiple members can be covered by the same AC563 form. 4 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 109 5 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 114 6 Department of Veterans’ Affairs Annual Report 2009/10 pages 135 and 137 7 Information provided by DVA Director Defence Links - MRCA stats excludes all non-primary removed (AAT, Recons, and VRB). SRCA stats exclude Removed claims with no MCRS received date or Date of Effect recorded and excludes all Claims where the TTTC (total days) is less then 0 8 Defence Annual Report 2008-09 Volume 1 Page 196
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
13
2.5.2 Contemporary practice To inform the gap analysis a literature review was undertaken to identify principles of contemporary/ better practice in relation to the management of injured or ill members during their Defence career and in transition from Defence.
The contemporary practice element of the SIIP review considered published and grey literature9
2.5.3 Field analysis phase
, evaluations and guidelines that discuss policies, processes and services. The majority of available literature related to civilian situations. Some literature was provided regarding defence systems and process in Australia, United Kingdom, Canada and the United States. This information was gathered to inform the gap analysis and is summarised in section 10 and in more detail in Appendix C.
The approach included a field analysis phase where input from key stakeholders including Medical Officers, Commanding Officers, Rehabilitation Coordinators, Training establishments, Single Service representatives, Defence Transition Services, Defence Community Organisation (DCO), DVA and VVCS was sought.
Over 70 stakeholders were engaged during this phase. The Review team is appreciative of the time and information contributed to the review and feel strongly that this input has informed many of the review recommendations. Details of stakeholders engagement is found in Appendix D.
Locations where field analysis occurred were:
• RAAF Base Amberley, Enoggera Barracks and Lavarack Barracks in Queensland;
• HMAS Stirling, Leeuwin Barracks and Campbell Barracks in Western Australia;
• HMAS Kuttabul, HMAS Penguin, Defence Plaza Sydney, RAAF Base Wagga, Kapooka and Holsworthy Barracks (2nd Commando Regiment) in New South Wales; and
• HMAS Cerberus in Victoria (via phone hook-up).
2.5.4 Issue identification and gap analysis
The understanding of the current state, (developed through the process mapping, literature review and field analysis), along with the contemporary practice findings informed the gap analysis and issue identification activity for this review.
9 The term ‘grey literature’ refers to research that is either unpublished or has been published in non-commercial form
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
D
C BA
2.6 Analysis framework The focussing question – which is also the ‘purpose’ defined in the SIIP Review Terms of Reference is “How do Defence and related service providers develop a seamless and integrated support process for injured or ill ADF members throughout their Service career and in transition from Defence.”
A model which describes the current situation (A: Where are we now?), the desired end state from the perspective of the ill or injured member and Defence (B: Where do we want to be?), the steps required to move from A to B (C: How will we get there?) and a description of other activities and next steps required to assist in realising C (D: What else needs to be done?) was developed to assist the reader to visualise the change process and underlying drivers and motivations for the recommendations in this review.
Figure 3 Analysis framework – ABCD
A description of the current state (Where are we now?) is contained in Figure 4. Supporting evidence and related information about the current state is contained in sections 5,6,7,8 and 9 of this document.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
15
Where are we now?A
Defence currently …..
Provides support to injured or ill members throughout their service career and in transition from Defence
However there are instances where……
• members fall through the gaps and do not receive the support they are entitled to and/ or require
• Ill or injured members and their families do not feel supported by Defence
• the implementation of the current system (including Policy, Defence Instructions, Legislation, Technology) does not enable Defence, in all cases, to effectively support its injured or ill members
So …….
“How do Defence and related service providers develop a seamless and integrated support process for injured or ill ADF members throughout their Service career and in transition from Defence”
Figure 4 Analysis framework - A: Where are we now?
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
Key features identified by stakeholders during SIIP as worth maintaining in the current support system include:
• The clinical care provided to injured or ill members is generally appropriate to the needs of the member. Good clinical treatment is provided in a timely manner. There are generally no barriers to the provision of treatment – although stigma associated with mental health issues exists.
• The ADFRP framework – the existence of a framework and its flexibility - especially that feedback from the MOs regarding entry triggers was acknowledged and reflected in recent modifications to the framework.
• The conversion of Program Case Manager (PCM) roles to APS positions and integration into Garrison Health Regional Health Services as part of the Garrison Health Transition Project – this will provide greater likelihood of case manager continuity as the APS roles will be committed/ dedicated to a Unit or Health Centre.
• Infrastructure investment in health facilities – Kapooka (Kapooka Health Centre, new RAP, rehabilitation/hydrotherapy facilities and Digger James 2 (Rehabilitation) platoon facilities), Edinburgh (not visited as part of this review) and Amberley (1EHS health facilities) were examples where infrastructure investment was significantly improving the health and rehabilitation of injured or ill members.
• Integration/ co-location – Service providers including counsellors, rehabilitation coordinators, claims assistance and transition service providers felt that the co-location (or close relationships and networks where co-location is not possible due to office space) resulted in better outcomes for members and their families.
• Regional Stakeholder Forums (RSF) – the purpose of the RSF is to enable a regionally based coordinated interdepartmental forum to focus on issues relating to the provision of transition support services. Participants viewed these as very worthwhile communication forums.
• Cultural change – new recruit training – it was felt that newer entrants into the ADF were aware of their requirements with respect to completing OHS incident notification and claim/ compensation paperwork as a result of the entry training they received. It is felt this translates into higher compliance by this demographic.
• Local focus groups/ case conferences – many of the locations visited held regular command meetings (variously called focus group, rehabilitation meeting, case conference etc) where a member’s situation was discussed.
Further details on these features are found in section 12.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
17
A summary of identified gaps and issues include:
• Overall visibility of members on rehabilitation programs - from a Unit and Service level - absence of management reports, performance metrics to inform Command/ Units of available capability, emerging trends etc.
• Support system at times relies on a member to hold up their hand and request assistance - self refer - noting some members are not in a position/ comfortable to do this. It is noted that the member also has obligation s in respect of their personal accountabilities.
• Converse to the above point, a member may self refer outside of Defence - to VVCS, civilian practitioners or to a psychologist and the CO and Defence has no visibility of this.
• Members on long-term convalescence leave or maternity leave who return to family (i.e. posted away from their Unit/ CO) - concern they are not visible to new CO/ structure for the duration of their leave.
• Trainees - medically separate quickly – may be unaware of their entitlements or support services available to them.
• Members who choose to voluntarily separate when a medical separation is more appropriate.
• Members who medically separate but choose not to engage, or are not in a position to engage with Transition Services so are unaware of their full entitlements and may not be linked in to available services.
• Defence services geared towards member not family even though Service related activity has caused or contributed to the family need.
• Governance and ownership - Who owns the system? Who has accountability for ensuring the system works? What quality assurance metrics are utilised to measure if the system is operating efficiently and effectively?
• MOs not referring members for rehabilitation.
Rehabilitation related including:
• Concern that members on rehabilitation programs are transferred to roles that do not provide them with an environment conducive to rehabilitation. This concern also extends to deployment and training waivers being provided to MEC3 members.
• The service provided by some (a minority) PCMs was unsatisfactory.
• Handover between Defence and civilian MOs/ facilities can be improved.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• Absence of appropriate performance metrics to enable rehabilitation referral patterns and PCM individual case manager workloads to be measured and monitored.
• The significant workload of PCMs in some regions results in instances where service provision is prioritised.
• A member may have many “case managers’ including a medical, rehabilitation, compensation claims, transition case manager and possibly even a MRCA section 64 case manager (perhaps a CCM) assigned to them as a legislative obligation of their Rehabilitation Authority.
• Confusion over roles, responsibilities and interactions - especially between case managers, Complex Case Managers, RCASOs and DCO and between APCDs and Transition Services.
Awareness related including:
• Limited understanding of requirement to hold Welfare Boards, in what circumstances they should be held and who should attend.
• Members not maintaining complete NOK, PEC details in PMKeyS - especially pre-deployment.
• Difficulty in encouraging Reservists (on CFTS) to complete RTAPS and POPS when they return to Australia.
• Difficulty in encouraging Reservists to complete the MECRB process for medical separation.
• The available corporate systems have not been/ are not configured to maximise usability and provide users with the information they require to make informed decisions. Non-corporately supported, but business critical, systems have been developed and generally do not interface with other systems, are not maintained and are not audited/verified to ensure they are returning the correct information to users.
Information technology related including:
• The absence of an effective system (including interface/ mechanism as well as procedures and conditions for information/ data exchange – including Privacy considerations) to transfer information and data between Agencies.
• User and business requirements for JeHDI and JP2080 Phase 2B projects: Many of the stakeholders visited during the review were unaware of the aims and functionality of the JeHDI project and have not provided input into the requirement gathering and specification phase of the project.
• Absence of workflow capability to support/ inform users of the IT systems.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
19
• Limitation of IT systems to support Defence personnel in performing their duties. This includes the limited availability of key performance metrics and information to make informed decisions.
• Information is generally not able to be presented/ filtered based on an individual's need to know. For instance, medical-in-confidence information may not always be separated out before a member’s situation is discussed at Welfare Boards, weekly case conferences etc.
• Difficulty extracting required OHS information/ trends from OHSCAR – Stakeholders reported that they have to request information - it does not appear to be readily available or pushed out to them.
• PMKeyS does not track MECRB dates which limits the ability of COs to keep on top of the MECRB process.
• Separated members trying to reach back into the Defence system when they should be relying on the public system for their health needs.
Expectation management related including:
• Expectation that services an injured member and their family are entitled to receive should be in excess of those services available to the general community.
• Member support networks are not always aware of the services DCO can provide.
• Efficiency of the MECRB process - Timeliness and Communication were the key pressure points. Members feel unsupported by Defence due to the time this process takes. The delay may exacerbate underlying mental issues of some members.
• Opportunity cost of members remaining on the rehabilitation program whilst awaiting a determination from the MECRB.
• Perception that submitting a DVA claim will affect career progression.
Liability determination related including:
• Length of time taken for claims determination to occur.
• Trainees – medically separating with a MEC 3 classification - doesn't exclude trainees from receiving entitlements, it just means that they have to prove more and jump through more hoops to access the same entitlements as a member who separates as MEC 4. Separation classifications and access to ComSuper benefits have an interrelationship with DVA benefits.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• There is inconsistency in the frequency, expected outcomes and participants attending Command focus groups/ case conferences by location and Service.
• There are many policy documents which relate to support for injured or ill members however there is no overarching document/ user guide which maps how all the individual health policies interact with each other.
Health policy development and implementation related including:
• Some Health policy is confusing, contradictory or difficult to understand. Limited effort appears to be directed to plain English expression of the health policy.
• Key stakeholders do not feel they are always adequately consulted during the development of health policy.
• Existing health policies do not appear to be updated/ amended in a timely manner to reflect changes to policy.
• Medical vs. administrative separation – guidance where medical conditions may cause, contribute or exacerbate administrative grounds for separation or vice versa.
2.6.1 B: Where do we want to be? Figure 5 defined the aspirational expectations of ill or injured members – as informed by the field analysis phase of this review, and from the member perspective.
Also listed are the Defence and related service provider expectations of a framework for supporting ill or injured members.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
21
Where do we want to be?B
Ill or Injured Member:ü Decisions impacting me are timely – liability determination,
MECRB etcü I know who to ask for assistance and they provide the correct
guidance/ informationü My family and I are guided and supported through the
complete process - based on my needs and entitlementsü I am aware of available supportü I am linked in to, and receiving required supportü There is continuity in the support I receiveü I understand the “system” and processes relevant to meü The system is easy for me to navigate throughü We are kept informed (what’s happening with me, how am I
progressing through system, what are the likely outcomes for me, what are my potential entitlements, what is my role and responsibility in this process etc)
Defence (DVA and other service providers):ü Primarily member centricü Efficient system – remove duplicationü Simple and efficient processes to deal with legislative
complexityü Service providers understand the system and their roles and
responsibilities in supporting injured or ill members ü Shared services (SRP)ü Joined up – integrated system to support decision making
within and between Agenciesü Maintains Defence capability ü Effective Governance – performance indicators identified,
measurable, measured and monitoredü Technology enables effective support of injured or ill –
improved information sharingü System appropriately resourced to be effectiveü Positioned/ co-located to provide timely supportü Enhances Defence’s reputation as Employer of Choiceü Effective communicationü Rehabilitation culture (Goal 1 and 2)
Figure 5 Analysis framework - B: Where do we want to be?
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
2.7 Recommendations - C: How will we get there? This summarises the SIIP recommendations to address identified gaps and issues. A comprehensive description of the recommendations is located in section 3.
How will we get there?C
Program of work including:
Integrated support framework addressing:1: Case coordination for “qualifying” members – single coordination point for the ill or injured member, their family, Command and service providers2: Content Management/ Personalisation - A technology solution to “push” targeted information to an injured or ill member (and/ or family) … based on information Defence already has about a member, triggers and specified business rules ... in a format appropriate to the member – email, MMS, link to web pages, hard copy (mail), through CO/Unit etc. A content/knowledge management solution to better manage Defence’s content and ensure it is accurate, accessible and fit for purpose3: Information Technology - to enable Defence and DVA to support an ill or injured member – information available on need to know basis, workflow, management reports – technology to guide and inform service providers and ensure consistency and compliance. Systematic process for sharing information to enable determination of liability.4: Recommendations addressing gaps and issues identified during SIIP Review including:• Governance and Ownership• Efficiency – MECRB, Compensation claim processing• Policy – Health policy development and implementation• Awareness - roles, responsibilities, functions• Guidance – Administrative vs. medical separation, MEC3
medical separation, Command focus groups• Other gaps - ADFRP
Figure 6 Analysis framework - C: How will we get there?
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
23
2.8 Next steps - D: What else needs to be done? This part of the analysis framework highlights additional activities, which are in general outside of the SIIP Review framework, which need to occur to assist Defence in achieving the desired future state framework for support of ill or injured members.
What else needs to be done?
Includes:1: Can legislative base be simplified? – Defence Act, SRCA, MRCA, VEA, OHS Act, Privacy Act etc2: Defence technology projects > JeHDI, JP20803: Section 64 MRCA – Transition Case Manager4: Single/Consolidated compensation claim form5: Prioritised claims processing 6: Resolve Medical-In-Confidence vs. Command “need to know” issues7: Identify Member Support Officers – Primary role were possible (not secondary activity/ function)8: DVA and ComSuper processes acknowledge Trainee MEC3 (MUFS) as medical separation so trainees are not disadvantaged
D
Figure 7 Analysis framework - D: What else needs to be done?
The recommendations arising from this review must be considered by the SIIP Project Steering Committee. The SIIP Project Steering Committee must advise which recommendations are to be further developed and progressed.
A high-level implementation plan has been developed to support this progression.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
3 Recommendations and suggested initiatives This section contains recommendations and suggested initiatives to better support injured or ill members and deliver an end state solution where:
• A member centric framework exists;
• An effective / joined up system exists;
• An efficient (shared service) tri-service system operates where duplication of support service provision is eliminated;
• Cultural change is occurring (a rehabilitation and timely incident reporting culture); and
• Appropriate communication and education occurs.
3.1 SIIP recommendations
REC 1.1 – It is recommended an owner is appointed to provide oversight to the systems which support injured or ill members. The owner will determine appropriate system performance metrics and report on these. The owner will ensure an effective and appropriate system governance framework is in operation.
REC 1.2 - It is recommended a program of work be established to progress and implement recommendations arising from this review. A dedicated Program Manager should be appointed to provide oversight across the program of work and to monitor and report on progress, dependencies, issues and risks.
REC 2.1 - It is recommended Defence provides qualifying ill or injured members with a Member support framework which, depending on the individual member circumstances could consist of a Member Support Officer (MSO), Rehabilitation Consultant (RC) and Command (always). This framework provides member case coordination across all stakeholders to ensure an injured or ill member and their family are supported throughout their injury, illness and rehabilitation outcome and, possibly, medical separation and transfer to external health care and support services.
REC 2.2 - It is recommended Defence fully defines the role, function and responsibilities of the MSO, RC and Command as they relate to supporting injured or ill members. It is further recommended that Defence defines and documents the triggers, criteria, conditions and circumstances that would “qualify” a member for entry into the Member Support framework.
REC 2.3 - It is recommended Defence uses the role, function and responsibility descriptions developed through REC 2.2 to inform and agree appropriate resourcing of the MSO and RC functions.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
25
REC 2.4 - It is recommended Defence and DVA develop processes and procedures that enable Defence to advise DVA of higher priority claims for liability processing and determination. Agreed service levels and benchmark processing times for these higher priority claims should be developed as part of this recommendation.
REC 2.5 - It is recommended that DVA pursue the development of processes that simplify the acceptance of liability under MRCA/SRCA/VEA.
REC 2.6 – It is recommended DGPERS Air Force and DG Navy People implement a individual member ‘welfare board’ equivalent within their Service for seriously ill or injured members.
REC 3.1 – It is recommended Defence investigates content/ knowledge management solutions to support the effective management of information.
REC 3.2 – It is recommended Defence investigates a technology solution to “push” personalised information to an injured or ill member (and/ or family) based on information.
REC 4.1 – It is recommended Defence utilise information technology to better support injured or ill members. Required information is available on a need to know basis to support effective information exchange, management reporting and enable informed decision-making. Workflow functionality is utilised to educate, guide and encourage compliance from service providers. An audit trail of activity is maintained.
REC 4.2 – It is recommended that a requirements team of subject matter experts is formed to develop and feed SIIP requirements into the JeHDI and JP2080 projects.
REC 5.1 - It is recommended the SIIP Project Steering Committee continues to convene after the conclusion of the SIIP review to provide overarching governance to Defence’s support for injured or ill members. It is further recommended that the title of the Steering Committee incorporates “wounded” to demonstrate an inclusiveness of injuries sustained whilst on Operations, in addition to illness or injury.
REC 5.2 – It is recommended that a joint review, update and redrafting of the overarching memorandum of understanding (MOU) between Defence and DVA occurs – to provide a refreshed/ current framework for implementing SIIP recommendations.
REC 6.1 - It is recommended CJHLTH defines and establishes performance metrics for the MECRB process areas within Joint Health Command control. It is recommended that the Services (including their personnel management agencies) define and establish performance metrics for the MECRB process areas within their influence and control.
REC 6.2 - It is recommended CJHLTH initiate a review of the resourcing requirements for the MECRB process to ensure it is adequately resourced to achieve defined performance metrics and provides greater transparency to people administering the MECRB process as well as members awaiting a determination
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
REC 6.3 – It is recommended DVA and Defence establish mechanisms to improve claims processing times.
REC 6.4 – It is recommended DVA and Defence develop processes and/or technology solutions to enhance sharing of information relating to injury or illness between Defence and DVA with a view to streamlining and simplifying compensation claims handling.
REC 6.5 – It is recommended Defence and DVA (through the DLSC) agree to accelerate and leverage the co-location of injured or ill member support services.
REC 6.6 - It is recommended a ‘visiting’ compensation claims advisory service is established as a high priority. Whilst it is expected this service will mainly be offered through existing Defence locations, a member home/ medical facility visit capability must form part of this service.
REC 7.1 – It is recommended that all areas responsible for the development of health related policy (including CJHLTH, the single Services and Transitions Support) leverage the policy development and reform activity in the Personnel Policy and Employment (PPEC) Branch of People Strategies and Policy Group (PSPG) and Human Resources Shared Services Program (HRSS) to better inform the development, alignment and delivery of Defence health policy.
REC 8.1 – It is recommended the Program Manager assigned in REC 1.2 oversee the development of a comprehensive and interrelated roles and responsibilities framework. This must include the functions each role performs and handoffs between roles.
REC 8.2 - It is recommended that the classification of a member as MEC3 triggers the MO to suggest to the member that they submit claims paperwork with DVA.
REC 8.3 – It is recommended that Defence, following classification of a member as MEC 3, advises DVA of the circumstances surrounding the classification – to enable DVA to commence liability determination. Processes and the mechanism for automated information exchange must be agreed between Defence and DVA.
REC 9.1 - It is recommended that Defence Instructions be reviewed to consider circumstances where a member has health and administrative reasons for separation.
REC 9.2 - It is recommended the Interdepartmental Working Group (IWG) address the interpretation and application of legislation relating to trainees medically separating with a MEC 3 classification (MUFS).
REC 9.3 - It is recommended the three Service DGPERS collectively adopt an outcomes based framework which guides COs in the conduct of command focus groups. There should be sufficient flexibility in the framework to ensure its applicability to each Service (size, location, primary function) and in Tri-Service situations.
REC 9.4 – It is recommended Health Directive 289 – Mental Health Case Management in the ADF and Health Directive 290 – Health Procedures for the Delivery of the ADF Rehabilitation Program are revised to address issues identified during this review – including contradictory
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
27
elements and confusion regarding how these two directives interact. It is further recommended that DI(A)PERS 33-11 and CA Directive 09/10 be reviewed and overlaps removed.
REC 10.1 - It is expected that the conversion of PCM roles into APS positions and integration into Garrison Health Services as part of the Garrison Health Transition Project, will suitably address a number of the gaps in the ADFRP. It is recommended the conversion activity, including appropriate and sufficient resourcing levels, are monitored and reported on to the governance committee (REC 5.1).
REC 10.2 - It is recommended the Services, through their DGPERS, consider whether it is appropriate for members classified as MEC 302 to be posted into Unit pool positions so that their active position can be filled by an able member until the member on rehabilitation is assessed as fit to return to work.
REC 10.3 – It is recommended the ADFRP implement a process to seek member feedback on the efficiency and effectiveness of the rehabilitation and support received through the ADFRP.
3.1.1 Interrelated nature of recommendations Figure 8 is an attempt to demonstrate how the recommendations interrelate and in totality produce enhanced member support outcomes. It maps the SIIP recommendations against an indicative member pathway (from point of injury/illness, primary care, rehabilitation and return to ADF duties or medical separation and related liability determination. and includes the ‘enablers’ – people, process and technology (suggested initiatives) which support/ underpin the recommendations.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
29
Represented another way, Table 1 maps the overarching recommendations against to the desired end state support framework as described in 2.6.1 “Where do we want to be?”.
Table 1 Mapping between desired end state and recommendations to address gaps and issues
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
3.2 Rec 1: System owner and program of work
REC 1.1 – It is recommended an owner is appointed to provide oversight to the systems which support injured or ill members. The owner will determine appropriate system performance metrics and report on these. The owner will ensure an effective and appropriate system governance framework is in operation.
The portfolio owner will provide leadership in the development of a member centric and joined up system which supports ill or injured members.
Preliminary discussions suggest the system owner would likely be:
• Deputy Secretary People Strategies and Policy (DSPSP)
• Vice Chief of the Defence Force (VCDF); or
• Shared ownership between DSPSP and VCDF.
REC 1.2 - It is recommended a program of work be established to progress and implement recommendations arising from this review. A dedicated Program Manager should be appointed to provide oversight across the program of work and to monitor and report on progress, dependencies, issues and risks.
The Program Manager position could be attached to Joint Health Command – possibly reporting to Director General Garrison Health, Director General Mental Health, Psychology and Rehabilitation or Commander Joint Health (CJHLTH) or attached to Head of People Capability (HPC).
The program manager will need to be across interdependent projects having the potential to inform, influence and assist in delivering support for injured or ill members. These projects include, but are not limited to:
• Joint e-Health Data Information System (JeHDI) – refer to 9.1.2;
• Joint Project 2080 Phase 2B1 – Human Resources Shared Services Transformation Project – refer to 9.1.4;
• Review of current Military Rehabilitation and Compensation arrangements – refer to 9.1.9; and
• The next phases of the Rehabilitation and Compensation (R&C) Business Redesign Blueprint Project (DVA) – refer to 9.1.16.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
31
It is suggested the program manager reports back to the SIIP Steering Committee on progress and actions taken in relation to out of SIIP scope issues identified in section 12.3.
3.3 Rec 2: Member support framework
REC 2.1 - It is recommended Defence provides qualifying ill or injured members with a Member support framework which, depending on the individual member circumstances could consist of a Member Support Officer (MSO), Rehabilitation Consultant (RC) and Command (always). This framework provides member case coordination across all stakeholders to ensure an injured or ill member and their family are supported throughout their injury, illness and rehabilitation outcome and, possibly, medical separation and transfer to external health care and support services.
To the extent possible – this should be a tri-Service approach – leveraging a shared services model and aiming to provide a consistent support framework across the Services.
The key features of this Member support framework include:
• The member is central. Any system supporting a ill or injured member must involve the member and the member’s support networks. An individual “welfare board” must actively involve the ill or injured member.
• Specified triggers, criteria, circumstances and conditions will define entry or ‘qualification’. These need to be developed as per REC 2.2.
• Member welfare is a Command responsibility.
• Command has visibility of all members – through defined communication pathways with the member’s case coordinator.
• In providing Member welfare, Command will be supported by health and administration service providers
• Command may seek additional assistance and support in dealing with more complex cases, multiple casualty situations etc.
• Member case coordination will be provided by Command, the RC or the MSO, depending on the complexity of the member’s situation (including injury, support network, rehabilitation gaol, Agencies and service providers involved etc).
• Where the member situation is “not complex” and the injured or ill member does not require a rehabilitation program, member case coordination will be provided by Command.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• If the member circumstances trigger entry into the ADFRP – a Rehabilitation Consultant (RC) will be assigned to the member through the ADFRP.
• Where the member situation is of “moderate complexity”
• Where the member situation is
and a RC has been assigned to the member, the RC will be the principal case co-ordinator for the member. This will require the RC to inform and advise Command on the member.
“complex”,
Figure 11
a MSO will be assigned and they will be the principal case co-ordinator for the member. This is irrespective of whether a RC has also been assigned to the member and noting the RC will assume coordination responsibility for rehabilitation related service providers, as per .
• The Services will assign a MSO to their member – informed by the member’s needs and circumstances.
• Support of ill or injured members is the primary responsibility of the MSO (i.e. it is a dedicated role).
• The MSO must be accessible to the member and the member’s support network.
• The MSO (service specific but not necessarily in uniform) role description contains sufficient flexibility to cater for Service and location specific outcomes whilst delivering a consistent support framework across the ADF.
• It is recommended the Service’s existing casualty management roles and responsibilities will transition into the Member support framework.
• The appointment of either a RC or MSO as the member’s principal case coordinator will satisfy the MRCA s64 obligation on the Rehabilitation Authority (currently the Service Chiefs) to appoint a transition case manager for medically separating members.
Some members may ‘opt out’ of Defence provided/ funded care, treatment and support. Defence needs to be comfortable this is an informed decision and receive documentation from the member to this effect. The member opting out of health care does not rule out the appointment of the MSO as this is a Command decision.
There are instances where a member chooses to engage directly with an external service provider (including but not limited to VVCS, Specialists, and Psychologists etc). In these instances, the member should still be able to easily access available information from within Defence.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
33
This handover of member case coordination, as well as indicative volumes (based on current statistics) is represented as follows:
Figure 9 Case coordination responsibilities within the Member support framework
The three levels of the Member Support framework are represented as follows in Figure 10. Indicative triggers which would “qualify” an ill or injured member into one of these levels have been defined.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
Figure 10 Member Support framework – based on complexity of member’s situation
A representation of the expanded the case coordination responsibility, for a “complex” case might look as follows:
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
35
Figure 11 Member Support framework for a "complex" member situation
Note from this diagram that the primary case coordination is provided by the MSO however the RC maintains responsibility for rehabilitation related services (and other service providers as defined in REC 2.2)
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
REC 2.2 - It is recommended Defence fully defines the role, function and responsibilities of the MSO, RC and Command as they relate to supporting injured or ill members. It is further recommended that Defence defines and documents the triggers, criteria, conditions and circumstances that would “qualify” a member for entry into the Member Support framework.
Responsibilities of the case coordinator should include:
• Primary point of contact between member and all service providers;
• Case coordination of required services;
• Provide and maintain link between member and all identified service providers;
• Review member progress;
• Keep Command informed – including updates at unit/case meetings;
• Engage with member’s support network including family – as appropriate;
• Monitor the efficiency and quality of services being provided by service providers– feedback to Defence;
• Recognise factors impacting on a member’s recovery;
• Monitor member engagement;
• Support member through transition process (as required); and
• Validate member is ‘separation ready’ from an administration perspective (as required).
Performance metrics and service level agreements should be developed as part of this recommendation.
Issues relating to the communication of medical-in-confidence information between providers of health services and clinical rehabilitation will need to be resolved and documented.
The Service approaches are relatively new and are being further defined, modified and adjusted through ongoing process improvement.
Existing Defence Instructions, policies etc will need to be amended to reflect the Member Support framework. It is recommended this opportunity is utilised to address the overuse of “case manager” within Health policy and procedures.
The member support services provided by each Service to their members differ markedly. The Services should collectively review their own and their counterparts offerings and determine
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
37
which elements from the three offerings should be consistently offered across the Services. Duplication of the services being offered to injured or ill members – through their Service and through other service providers should be eliminated.
Efficiencies through shared training opportunities and the ability to network across the three Services should also be considered.
Indicative triggers including MEC and rehabilitation goals that underpin the Member Support framework must be defined but could include triggers represented in the following figure:
Figure 12 Indicative triggers for entry into the Member Support framework
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
REC 2.3 - It is recommended Defence uses the role, function and responsibility descriptions developed through REC 2.2 to inform and agree appropriate resourcing of the MSO and RC functions.
The MSO and RC functions must be appropriately resourced. Experience in the Complex Case Officer (CCO) rollout suggests the introduction of this type of support function will surface existing but hidden demand for services – i.e. it is expected there will be an initial surge in demand for member support services.
There are a number of enabling projects which enhance the efficiency of the MSO and RC roles. It is noted that these projects occurring in isolation (outside the Member support framework) will still result in better support outcomes
REC 2.4 - It is recommended Defence and DVA develop processes and procedures that enable Defence to advise DVA of higher priority claims for liability processing and determination. Agreed service levels and benchmark processing times for these higher priority claims should be developed as part of this recommendation.
for injured or ill members. These projects include the implementation of a single/ consolidated compensation claim form (REC 2.5) and the ability for Defence to advise DVA of higher priority claims for prioritised liability determination (REC 2.4).
Care needs to be taken to ensure every, or even the majority of, cases are not
1. Deaths/Terminal illnesses (not in payment);
classified as high priority. Criteria for determining what constitutes a high priority claim needs to be agreed. A suggested priority follows:
2. Financial necessity;
3. Reservists;
4. Imminent medical separation (termination notice (TN) issued); then
5. Serious injuries (work related) that require DVA services as a priority (e.g. home modifications, home services, significant aids and equipment) to enable a member to leave hospital.
REC 2.5 - It is recommended that DVA pursue the development of processes that simplify the acceptance of liability under MRCA/SRCA/VEA.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
39
Many stakeholders were of the view that a single/ simplified claim form and process should reduce the administration involved in obtaining and photocopying service and medical documents and reduce the member’s requirement to understanding the overarching legislative framework. This should be considered as part of this recommendation.
REC 2.6 – It is recommended DGPERS Air Force and DG Navy People implement a individual member ‘welfare board’ equivalent within their Service for seriously ill or injured members.
The focus of a “welfare board” is to ensure a member’s welfare needs are adequately addressed. It is specific to, and involves the member and enables the Command group to consider all relevant information regarding a member’s care. It has a member focus.
The requirement to hold an individual welfare board is additional to the conduct of command focus groups (REC 9.3) – which have a Unit and capability focus (many members discussed during a single command focus group). As per the key principles described for REC 2.1 – a member (and support personnel) must be invited to attend their welfare board.
REC 3.1 – It is recommended Defence investigates content/ knowledge management solutions to support the effective management of information.
Put simply, a significant amount of information exists but it is not easy to find.
Managing this information (content management activities including review and updating content (and related change control activities), ensuring key messages are easy to understand, ensuring the information can be accessed and found) and personalising it as appropriate to a member’s circumstance will better support injured or ill members, Command and service providers.
This recommendation extends to all available content which Defence owns – not just the content being “pushed” to an ill or injured member. It involves “clean up” and refresh of existing content, the creation of new/ targeted content and indexing and tagging all content to ensure it is discoverable, can be located and accessed by members. Indeed – the application of this would extend more broadly in Defence – but the specific target for this recommendation is that content which is relevant to the support for injured or ill members and their service providers.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
Some of the key project tasks to enable information to be managed and content personalised are described below:
Figure 13 Activities required to manage knowledge and personalise content
REC 3.2 – It is recommended Defence investigates a technology solution to “push” personalised information to an injured or ill member (and/ or family) based on information.
Defence already possesses about the member, information triggers and specified business rules. The information will be pushed to the member in a format preferred (and appropriate to the current location ) by the member but including email, MMS, web pages, hard copy (mail), directed through the member’s Unit or Command etc.
This recommendation has been suggested as a mechanism to enhance member and service provider access to available information and not a mechanism to force unwanted information onto a member.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
41
The concept of personalisation is illustrated in the following diagram – where information is already held by Defence about an injured or ill member. Defence pushes relevant content to a member (and other entities as defined and appropriate) – based on this knowledge/ information.
Figure 14 Personalised content is pushed to an injured or ill member
A simple example to illustrate the concept follows:
Figure 15 Personalised content pushed to an injured member, family and Command
Circle 4 in the above figure acknowledges that it may also be prudent to provide some information, either through this process or the workflow processes described in REC 4.1, to external agencies including DVA, ComCare, and ComSuper etc.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
3.5 Rec 4: Information Technology as an enabler
REC 4.1 – It is recommended Defence utilise information technology to better support injured or ill members. Required information is available on a need to know basis to support effective information exchange, management reporting and enable informed decision-making. Workflow functionality is utilised to educate, guide and encourage compliance from service providers. An audit trail of activity is maintained.
A simple example of a potential workflow capability follows where:
• CAPT John Smith severely injures his back , whilst on duty, on 1 November;
• CAPT Smith has a consultation with a MO on 1 November; and
• During the consultation the MO notes in the “system” that the injury occurred in the workplace.
• The “system” realises no AC563 has been lodged in relation to this incident. This kicks off an AC563 workflow – sending an email to CAPT Smith’s CO informing that an AC563 is outstanding. If the relevant AC563 is lodged within 2 days no further activity occurs in this workflow. If no lodgement has occurred within two days, the workflow sends a follow up email to the CO. If no lodgement occurs within four days from the initial email the workflow escalates the non-lodgement issue up the Command chain.
• A similar situation occurs with the MO noting the injury occurred in the workplace. The liability determination workflow informs DVA of a potential liability (what is notified to be determined based on privacy considerations and information exchange principles) as well as triggering a DVA representative to contact CAPT Smith and offer him assistance in lodging claim paperwork. The liability determination workflow could also send MRCA claim paperwork to CAPT Smith.
It is noted that the AC563 is not the only mechanism through which injury notification occurs – and in some instances such as sporting injuries an AC563 is not a legislative requirement. Any workflow would need to build in these other incident notification mechanisms. The above example was provided for illustrative purposes only and does not describe a complete and entire workflow. There are many workflow possibilities.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
43
Figure 16 Information technology - simple workflow example
REC 4.2 – It is recommended that a requirements team of subject matter experts is formed to develop and feed SIIP requirements into the JeHDI and JP2080 projects.
These requirements include user-defined reports, workflows and related triggers, system modifications and process improvements. This team will also be responsible for defining SIIP related business rules, inform the project teams on process, documentation and workflows and assist in defining appropriate test scripts and cases and perform user acceptance testing on SIIP related functionality.
Membership could be drawn from the current SIIP Working Group and supplemented with relevant subject matter expertise as required.
It would also be prudent to consider representation from other Agencies on the requirements team.
Given both projects require user/business requirements by Feb-Mar 2011, the formation of this team should be a high priority.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
3.6 Rec 5: SIIP Governance
REC 5.1 - It is recommended the SIIP Project Steering Committee continues to convene after the conclusion of the SIIP review to provide overarching governance to Defence’s support for injured or ill members. It is further recommended that the title of the Steering Committee incorporates “wounded” to demonstrate an inclusiveness of injuries sustained whilst on Operations, in addition to illness or injury.
Terms of Reference defining Committee member’s responsibilities will need to be drafted and endorsed. Meeting frequency should be at least every quarter. The current membership should be reviewed to ensure it reflects the revised Terms of Reference.
This Committee will provide guidance to the Program Manager appointed to oversee the implementation of SIIP recommendations (REC 1.1).
This Committee will provide updates on issues and progress to the Defence/DVA Links Steering Committee (DLSC) as appropriate.
REC 5.2 – It is recommended that a joint review, update and redrafting of the overarching memorandum of understanding (MOU) between Defence and DVA occurs – to provide a refreshed/ current framework for implementing SIIP recommendations.
The MOU was set up in 2006 to standardise and draw together common parts of the agreements between Defence and DVA. The MOU is supported by a number of schedules which pertain to individual aspects of particular services including:
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
45
• SLA – Research Support & Development, DVA and SCMA, Nominal Roll of Australian Veteran of the Vietnam War; and
• SLA – Provision of ADF personnel records.
The MOU and schedules have not been reviewed for several years.
3.7 Rec 6: Efficiency
REC 6.1 - It is recommended CJHLTH defines and establishes performance metrics for the MECRB process areas within Joint Health Command control. It is recommended that the Services (including their personnel management agencies) define and establish performance metrics for the MECRB process areas within their influence and control.
These metrics should include agreement of acceptable timeframes for preparation of a medical summary upon receipt of all required documentation, scheduling MECRBs, notification of panelling, length of time between panelling advice and MECRB occurring, and elapsed time between a determination being made and notification to the CO and member.
This should also include guidance on how frequently a MECRB should meet and acceptable panel loads per MECRB.
REC 6.2 - It is recommended CJHLTH initiate a review of the resourcing requirements for the MECRB process to ensure it is adequately resourced to achieve defined performance metrics and provides greater transparency to people administering the MECRB process as well as members awaiting a determination
This resourcing review should consider “possible solutions” detailed in section 11.
REC 6.3 – It is recommended DVA and Defence establish mechanisms to improve claims processing times.
REC 6.4 – It is recommended DVA and Defence develop processes and/or technology solutions to enhance sharing of information relating to injury or illness between Defence and DVA with a view to streamlining and simplifying compensation claims handling.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
This extends to investigating mechanisms to better update and inform the member about their claim’s progress through the liability determination cycle.
Revised key performance indications (KPI) and service level agreements (SLA) must be developed to reflect new efficiencies.
It is expected that member access to liability/ compensation claim determination expertise (REC 6.5) will assist in this regard, as will improvement initiatives in the Single Access Mechanism (SAM) process, the progressing of a single claim form (REC 2.5) and the progression of the Rehabilitation and Compensation Business Redesign Blueprint Project (DVA). Implementation of REC 6.2 and REC 6.4 will further assist in this regard.
It is expected the agreed processing time SLA will reflect the period of time between injury/ incident/ exposure and the submission of a compensation claim. Where the elapsed time between incident and claim is short (to be agreed) then it is expected these claims should be capable of being processed in a more expedient manner than where the elapsed time is significant.
REC 6.5 – It is recommended Defence and DVA (through the DLSC) agree to accelerate and leverage the co-location of injured or ill member support services.
Real estate considerations and the appropriate premises for co-location will need to de addressed (i.e. within medical/ rehabilitation facilities, with the ADF Transition Centres etc). As will the hours of operation of these member support hubs – ensuring the hours of operation are suited to member lifestyles. For instance – some services provided after hours so the member’s support network can attend, availability of temporary childcare facilities etc.
It is noted that other pathways into support services must also be available to cater more fully to member preferences. This would include the ability to receive advice and support from uniformed or non-uniformed (civilian) service providers, off site provision of some services for those members who are unable to, or would prefer not to, return to a Defence location.
Although the focus of this review is supporting injured or ill members, it is expected that the co-location of member support services would be addressed in the context of support services for all ADF member circumstances.
REC 6.6 - It is recommended a ‘visiting’ compensation claims advisory service is established as a high priority. Whilst it is expected this service will mainly be offered through existing Defence locations, a member home/ medical facility visit capability must form part of this service.
This recommendation includes consideration of suitably located premises and required facilities (meeting rooms, photocopiers, computers, telephones etc) on larger Defence premises to facilitate a base visitation schedule.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
47
The main service provider is expected to be DVA, but will also include ESOs and the single service claim assistance specialists such as the Air Force Complex Claims Liaison Officers (CCLO). This should be a shared service.
This is not an advocacy service. It is not envisaged that this will be a form filling service – it is a member advisory service which informs the member about the claims process, liability determination and how to complete the required paperwork.
Funding of this service, including possible changes to DVA’s operating model will need to be addressed.
3.8 Rec 7: Policy development
REC 7.1 – It is recommended that all areas responsible for the development of health related policy (including CJHLTH, the single Services and Transitions Support) leverage the policy development and reform activity in the Personnel Policy and Employment (PPEC) Branch of People Strategies and Policy Group (PSPG) and Human Resources Shared Services Program (HRSS) to better inform the development, alignment and delivery of Defence health policy.
HRSS is one of the reform programs within the Workforce and Shared Services Reform Program (WSSR) – a SRP initiative sponsored by the Deputy Secretary of People Strategies and Policy (PSP). The HRSS has three reform sub-streams – namely Career Management, Education and Training and “Other HR”. Efficiencies are to be gained through:
• Creating leaner, more efficient business support functions including improved or new shared service functions;
• Civilianising military support positions; and
• Converting contractor positions to APS positions.
“Delivery of HR Policy Framework” is one of the projects within the Other HR sub-stream. This project links in to the policy deregulation work presently occurring and aims to improve the policy development cycle areas across the portfolio. Whilst it is early days in terms of delivery – the project is currently designing the future state framework which is expected to consider the stakeholder consultation and improving the feedback loop, to support the existing de-regulation initiative and potential for electronic policy workflow/ decision-making.
Simpler, more concise policies that refer to national benchmarks as appropriate is the desired outcome from this recommendation.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
3.9 Rec 8: Awareness
REC 8.1 – It is recommended the Program Manager assigned in REC 1.2 oversee the development of a comprehensive and interrelated roles and responsibilities framework. This must include the functions each role performs and handoffs between roles.
This activity will be informed by many of the SIIP review recommendations. An outcome of this process must be a clearly defined and easy to follow role description for members, service providers and relevant stakeholders.
REC 2.2 is a subset of this recommendation.
The outcome of this recommendation must clearly acknowledge the obligations and outline the responsibilities of an ADF member within this support system.
REC 8.2 - It is recommended that the classification of a member as MEC3 triggers the MO to suggest to the member that they submit claims paperwork with DVA.
REC 8.3 – It is recommended that Defence, following classification of a member as MEC 3, advises DVA of the circumstances surrounding the classification – to enable DVA to commence liability determination. Processes and the mechanism for automated information exchange must be agreed between Defence and DVA.
These recommendations should be addressed through the communications activities planned for Phase Two of SIIP.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
49
3.10 Rec 9: Guidance
REC 9.1 - It is recommended that Defence Instructions be reviewed to consider circumstances where a member has health and administrative reasons for separation.
This review needs to include the provision of guidance to COs and MOs on the appropriate mode of separation and acknowledgment of the continuum between administrative and health factors.
REC 9.2 - It is recommended the Interdepartmental Working Group (IWG) address the interpretation and application of legislation relating to trainees medically separating with a MEC 3 classification (MUFS).
DVA relies on the MEC classification and the condition that lead to that classification to determine if legislative support exists to support a decision that a person is incapacitated for service because of an accepted condition under MRCA or SRCA. This results in issues where DVA interprets that trainees being separated with a MEC 3 classification are not being medically separated/ discharged. This appears contrary to the intent of DI(G)PERS 16-15 Amdt 2 – Australian Defence Force Medical Employment Classification System . This impacts the entitlements the medically separated trainee receives.
Resolution must include MECRB guidance as to the appropriate MEC classification for Trainees who separate medically from the ADF.
REC 9.3 - It is recommended the three Service DGPERS collectively adopt an outcomes based framework which guides COs in the conduct of command focus groups. There should be sufficient flexibility in the framework to ensure its applicability to each Service (size, location, primary function) and in Tri-Service situations.
REC 9.4 – It is recommended Health Directive 289 – Mental Health Case Management in the ADF and Health Directive 290 – Health Procedures for the Delivery of the ADF Rehabilitation Program are revised to address issues identified during this review – including contradictory elements and confusion regarding how these two directives interact. It is further recommended that DI(A)PERS 33-11 and CA Directive 09/10 be reviewed and overlaps removed.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
3.11 Rec 10: Other gaps and issues
REC 10.1 - It is expected that the conversion of PCM roles into APS positions and integration into Garrison Health Services as part of the Garrison Health Transition Project, will suitably address a number of the gaps in the ADFRP. It is recommended the conversion activity, including appropriate and sufficient resourcing levels, are monitored and reported on to the governance committee (REC 5.1).
REC 10.2 - It is recommended the Services, through their DGPERS, consider whether it is appropriate for members classified as MEC 302 to be posted into Unit pool positions so that their active position can be filled by an able member until the member on rehabilitation is assessed as fit to return to work.
REC 10.3 – It is recommended the ADFRP implement a process to seek member feedback on the efficiency and effectiveness of the rehabilitation and support received through the ADFRP.
The feedback received should be analysed and the findings reported back to the SIIP Steering Committee (REC 5.1) for actioning – as well as Garrison Health Support Branch.
The frequency with which feedback is sought should be sufficiently regular to inform future activity and for any emerging issues to be acted upon in a timely manner. Feedback should be sought from members currently on a rehabilitation program and all members who have completed rehabilitation (closed rehabilitation program).
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
51
4 Engagement overview
4.1 Background Defence is committed to managing the health consequences of operational service as well as providing health treatment to ill or injured personnel.
The Defence occupational health and safety system is designed to prevent and minimise the impact of operational, environmental and occupational health threats.
The Support for Injured or Ill Project (SIIP) commenced on 2 August 2010, as a result of the Head of People Capability (HPC), Head of Defence Support Operations (HDSO) and Commander Joint Health (CJHLTH) agreeing to conduct a gap analysis against best practice of the elements of service delivery and related policy in the areas of incident reporting, welfare, health care, rehabilitation, compensation and transition.
The purpose of SIIP is to develop a seamless and integrated support process for injured or ill ADF members throughout their Service career and in transition from Defence.
The areas of rehabilitation, compensation and transition continue to be the subject of extensive attention within Defence with a view to developing a seamless and integrated support service for injured or ill ADF members. There has been a number of process mapping exercises that have defined the range of services available and how they relate to each other. Most recently these exercises have focused on a developing area of concern, that is, the service responsibility boundaries between Defence and the Department of Veterans’ Affairs (DVA) with regard to medical separations. The issues have also been raised in the context of the Review of Military Compensation Arrangements and in the agenda of the Defence/DVA Links Steering Committee (refer to 10.1.1), the latter focusing on the decommissioning of the Transition Management Service (TMS – refer to 7.7). The opportunity to improve the integration and streamlining of services is also supported by the Defence Strategic Reform Program (SRP).
The SIIP project has been undertaken in a collaborative manner with DVA.
The project’s governance consists of a SIIP Working Group and a SIIP Project Steering Committee.
The complete Terms of Reference for SIIP, including membership of the abovementioned governance entities is located in Appendix A.
4.2 Scope Included in scope is all support mechanisms available to an injured or ill ADF member from the point of, or presentation of, injury or illness right through their rehabilitation and recovery process or from the point of entry back in Australia in instances where the injury or illness occurred outside Australia. This includes primary healthcare/ clinical treatment, rehabilitation, return of the member to ADF duties, medical separation and liability determination and includes members with compensable or non-compensable injuries and illness.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
Whilst the importance of preventing injury or illness is acknowledged, consideration of this activity was excluded from scope by the SIIP Project Steering Committee during its initial meeting on 5 August 2010 due to the significant activity and reform already occurring in this space and the time limitations of the SIIP review.
Although “family” was not initially included within the Terms of Reference it has subsequently been brought into scope for the review – acknowledging the importance of member support networks for the recovery and rehabilitation of an ill or injured member. The review team has not attempted to define “family”. For the purposes of this review, we have assumed family to include the family, friends, acquaintances and other networks the member may acknowledge and rely on for support and assistance.
The SIIP did not consider support systems available to non ADF members – so does not address Australian Public Service (APS) Department of Defence employees, Defence contractors etc.
4.3 Approach
4.3.1 Define current state
Significant documentation (in various formats and degrees of completeness and accuracy) exists to describe the current support system for injured or ill members. This documentation includes process maps, process and procedure guides, legislation, Defence Instructions, Health Directives and Review findings and recommendations.
Workforce analysis statistics are included in section 5.
Review of available current system documentation culminated in the Working Group compiling a set of a high-level process maps describing the key processes and interactions, relevant legislation, applicable forms/ documents and key stakeholder and service providers involved in the following systems:
• Occupational Health and Safety (as per those elements included in scope);
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
53
Each of these high-level process maps are described in more detail in 6.2. These process maps are attached in Appendix B.
Descriptions of the available support services for injured or ill members is located at section 7 and includes those services provided by Defence and other service providers including VVCS and DVA. Local, regional or Service specific support services are described in section 8.
An analysis of other initiatives and projects, external to the SIIP review, which have the capacity to influence or inform the support provided to injured or ill members are described in section 9.
A description of the current governance arrangements within Defence and between Defence and DVA are contained in section 10.
4.3.2 Contemporary practice principles – identify and define To inform the SIIP gap analysis, a literature review was undertaken to develop principles of contemporary practice with regards to the management of injured or ill ADF members both during their Defence career and in transition from Defence.
The contemporary practice element of the SIIP review considered a wide range of published and grey literature10
• OHS Act, Regulations and Legislation.
, evaluations and guidelines that discuss policies, processes and services. The majority of the literature found related to civilian services. Some literature was available regarding defence systems and process in Australia, United Kingdom, Canada and the United States. In undertaking the better practice document review, information was sourced from:
• ComCare Guidelines and State Worker’s Compensation bodies.
• The Heads of Worker’s Compensation Authorities (HWCA).
• Productivity Commission Inquiry Report.
• Published and grey literature regarding RTW and worker’s compensation.
• Websites from the United Kingdom, United States and Canada.
• Documents provided by the SIIP Working Group including internal reviews and evaluations commissioned by the ADF or DVA.
• Documents provided by Veterans’ Affairs Canada including information on defence / defense rehabilitation services in the US and Canada.
The contemporary practice review considered the spectrum of services available to persons who are injured at work and the support and rehabilitation services available to them including the 10 The term ‘grey literature’ refers to research that is either unpublished or has been published in non-commercial form
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
systems and processes that support the journey of the individual. This information was then related back to the management of injured or ill ADF members both during their Defence career and in transition from Defence. This information was gathered to inform the gap analysis and is summarised in section 11.
The areas of investigation for this document review included:
• Injury management system design and implementation;
• RTW rehabilitation services and management;
• Employer’s roles and responsibilities – welfare, healthcare, rehabilitation and compensation policy, procedure and processes;
• Healthcare provider’s roles and responsibilities and involvement in rehabilitation;
• Worker’s roles and responsibilities, including characteristics that effect RTW;
• Rehabilitation providers – roles and responsibilities;
• Vocational rehabilitation; and
• Compensation and transition.
4.3.3 Field analysis phase
The approach included a field analysis phase where input from key stakeholders including Medical Officers, Commanding Officers, Rehabilitation Coordinators, Training establishments, Single Service representatives, Defence Transition Services, Defence Community Organisation (DCO), DVA and VVCS was sought.
Over 70 stakeholders were engaged with during this field analysis phase. Details of stakeholders who participated are found in Appendix D.
With the exception of HMAS Cerberus, these discussions occurred face to face. These discussions with key stakeholders were informal in nature and generally followed this format:
• Introductions including description of stakeholder’s role in relation to supporting injured or ill members;
• Background to the SIIP;
• Discussion of stakeholder perceived gaps and issues – drawing on current local issues, circumstances and examples;
• Positives with the current system – what works well; and
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
55
• Suggested improvements to the current system.
Locations where field analysis occurred were:
• RAAF Base Amberley, Enoggera Barracks and Lavarack Barracks in Queensland;
• HMAS Stirling, Leeuwin Barracks and Campbell Barracks in Western Australia;
• HMAS Kuttabul, HMAS Penguin, Defence Plaza Sydney, RAAF Base Wagga, Kapooka and Holsworthy Barracks (2nd Commando Regiment) in New South Wales; and
• HMAS Cerberus in Victoria (via phone hook-up).
4.3.4 Issue identification and gap analysis
The understanding of the current state, (developed through the process mapping and documentation review and field analysis phase), along with the contemporary practice findings informed the gap analysis and issues identification activity for this review.
A detailed description of these issues and gaps is located in section 12.2.
4.3.5 Recommendations Recommendations to address gaps and issues identified during the current state review (process maps, field analysis/ stakeholder consultation and contemporary practice/ literature review) are listed in section 3.
4.4 SIIP review limitations There were a number of logistical and practical limitations to the SIIP review which include:
• Availability of stakeholders to contribute – impacted by current/ existing work obligations, sickness, annual leave, overseas travel and EX HAMIL;
• Information was requested/ sought during field analysis. The Review team was unable (due to time constraints and the sheer volume of information received) to independently validate all views and opinions expressed by stakeholders during this field analysis; and
• Contemporary practice review was based on available literature. The Review team was unable to locate information/ Reviews which validated the efficiency and effectiveness of initiatives and programs described in this literature – i.e. not in a position to describe these initiatives as “best practice”. It is not possible for the Review team to validate the efficiency of the initiatives and programs documented in the contemporary practice section of this review.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
5 ADF Workforce Profile This section provides an overview of some of the key statistics in relation to ill or injured members of the ADF – including funded strength, Occupational Health and Safety incident notification, the ADF rehabilitation program utilisation, liability determination and medical separations.
5.1 At a glance …. • The FY2008/09 average funded strength (AFS) of the ADF is 55,091 members. This is
represented by Army – 27,833, Navy – 13,182 and Air Force – 14,066 and is an increase of 3.6% from FY 2007/08 (53,167) 11
• The Medical Employment Classification (MEC) of the AFS (at 30 Jun 2010) is MEC1 – 71.1%; MEC2 – 19.9%; MEC3 – 7.7% and MEC4 – 1.2%
• 12,906 AC563 Incident Notification forms were recorded for ADF members during FY 2009/10.12
• There were 4,189 referrals into the Australian Defence Force Rehabilitation Program (ADFRP) during FY 2009/10. This is a slight increase on FY 2008/09 where there were 4,117 referrals into the ADFRP.
• An 84.1% total return to work rate was achieved for the 3,959 rehabilitation programs closed during FY 2009/10.
• For all closed rehabilitation programs - 61.4% (2,430) achieved Rehabilitation Goal 1, 1.8% (72) achieved Goal 2, 13.4% (532) were Goal 3 and 23.4% (925) did not require a rehabilitation program.
• The top 5 injury categories (tri-service) for FY 2009/10 requiring rehabilitation plans were “Other musculo-skeletal (1,172), Mental health disorders (577), Disorders of the knee (558), Disorders of the back (415) and Obesity (167).
• There were 9,649 new VEA Veterans’ Income Support and Allowance claims during FY 2009-10.13, 16,821 primary claims for VEA Veterans’ Disability Support14, 2,589 incapacity payees under SRCA and 3,381 initial liability claims for injury received and 1,254 incapacity payees under MRCA and 3,181 initial liability claims for injury received.15
• The average claims processing times for Veterans’ Income Support and Allowances (VEA) was 43 days (target 32 days), Veterans’ Disability Support (VEA) – 70.3 days (target 75
11 Defence Annual Report 2008-09 Volume 1 Page 27 - Defence Annual Report 2007-08 Volume 1 Page 99 12 Caution should be used in linking OHS AC563 data to actual OHS incidents. The AC563 is principally designed as a ComCare notification form. Every incident is not captured through the AC563 process – including near misses/ dangerous occurrences. In additional, multiple members can be covered by the same AC563 form. 13 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 109 14 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 114 15 Department of Veterans’ Affairs Annual Report 2009/10 pages 135 and 137
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
57
days), Incapacity payees (SRCA) – 89 days (target 120 days) and Incapacity payees (MRCA) – 123 days (target 120 days) during FY 2009/10.
• As at Aug 2010, the average elapsed time between incident/ injury and the member submitting a claim with DVA is 1.6 years (570 days) for MRCA claims and 16.7 years (6,113) for SCRA claims.16
• There were 5,043 tri-service separations during FY 2008/09 of which 3,012 were voluntary, 825 were involuntary, 2 were age retirement and 1,204 were cadets and trainees.
17
• 13.4% of the FY 2009/10 total separations were medically unfit for further service (MUFS), 12.0% were retention not in the Service interest and 0.7% as a result of death.
5.2 Average Funded Strength (AFS) Average funded strength is the average number of full-time equivalent permanent Force members and Reservists on continuous full time service (CFTS) paid over a number of pay periods commencing from the start of the financial year.
2008-09 Actual18
2007-08 Actual 19
2006-07 Actual 20
2005-06 Actual 21
2004-05 Actual 22
Army
27,833 26,611 25,525 25,241 25,356
Navy 13,182 12,935 12,690 12,767 13,089
Air Force 14,066 13,621 13,289 13,143 13,368
Total 55,081 53,167 51,504 51,151 51,813 Table 2 ADF Average Funded Strength - extracted from Defence Annual Reports
Notes:
• Figures are average funded strength; Reservists on CFTS are included in the figures. Employees on forms of leave without pay (LWOP) are not included. Excludes APS employees.
• Includes ADF members in the Defence Materiel Organisation (DMO).
16 Information provided by DVA Director Defence Links - MRCA stats excludes all non-primary removed (AAT, Recons, and VRB). SRCA stats exclude Removed claims with no MCRS received date or Date of Effect recorded and excludes all Claims where the TTTC (total days) is less then 0 17 Defence Annual Report 2008-09 Volume 1 Page 196 18 Defence Annual Report 2008-09 Volume 1 Page 27 19 Defence Annual Report 2007-08 Volume 1 Page 99 20 Defence Annual Report 2006-07 Volume 1 Page 125 21 Defence Annual Report 2005-06 Volume 1 Page 218 22 Defence Annual Report 2005-06 Volume 1 Page 218
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
5.2.1 MEC classification of ADF permanent workforce The following two tables show the MEC, at 30 Jun for FYs 2009/10 (Table 3) and 2008/09 (Table 4) for the ADF AFS.
Totals 27,482 12,791 13,965 54,238 Table 4 MEC classification of ADF AFS at 30 Jun 2009
Noting there is a minor discrepancy between the data utilised in the Defence Annual reports and the data extracted for this query – 843 extra members are included in the above statistics for FY 2008/09. This has not been investigated as it is considered immaterial for the purposes of this analysis (approximately 1.5% variance).
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
59
5.3 Occupational Health & Safety The following table data relevant to the lodgement of AC563 Incident Notification forms for ADF members. The data is extracted from OHSCAR and excludes APS employees and contractors.
As this data have not been analysed further, no inference is drawn from the annual increase in lodgement of AC563s. It could be a result of increased awareness of the requirement to lodge an AC563, recognition of the increased military tempo of the ADF, increases in AFS etc.
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
5.3.1 Average time taken to lodge an AC563 – by type of incident Caution: this ‘average’ data can be skewed by significant delays in lodging an AC563 (measured in years) for a small number of incidents/ exposures.
Measurement in this table is in days and commences when the incident, injury or exposure first occurs and concludes when OHS branch is notified of the incident.
20010-09 2008-09 2007-08 2006-07
Death 11 11 48 2
SPI 21 27 33 60
Incapacity 41 77 75 92
Minor Injury 79 37 33 54
DO 19 17 17 49
Exposure 85 124 100 164
Total Average 74 72 55 113 Table 6 Average time taken to lodge AC563 Incident Notification - by incident type
Where:
• (DO) Dangerous occurrence: An incident where no person is injured, but could have been injured, resulting in Serious Personal Injury, Incapacity or Death. Commonly called a ‘near miss.’
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
61
5.4 Rehabilitation - ADFRP The data on rehabilitation statistics is sourced from RCIMT (Rehabilitation Coordinators Information Management Tool) – an Access database utilised and updated by the Australian Defence Force Rehabilitation Program (ADFRP) Rehabilitation Coordinators (RC) and the Directorate of ADF Rehabilitation Services (DRS).
5.4.2 Closed rehabilitation cases for 2009/10 – by Service and goal23
“The ADFRP aims to achieve a seamless rehabilitation process through the early identification of injury of illness, coordinated clinical and occupational rehabilitation as well as vocational retraining. The success of any occupational rehabilitation program is dependent on all key stakeholders working together to achieve successful outcomes directly related to the member’s needs, duties and workplace.”24
The ADFRP rehabilitation goals are:
Goal 1: Fit for duties and rehabilitate to member’s pre injury status.
Goal 2: Fit for duties with change in duties/ location/ service.
Goal 3: Stabilise member then transition out of ADF to the civilian environment.
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
Total 2,378 904 677 3,959 Table 8 Closed rehabilitation cases – by Service and goal – 2009/10
5.4.3 Closed rehabilitation cases for 2009/10 – by Service and rehabilitation closure outcome26
Army Navy Air Force Totals
Return to Work 1,454 61.1% 425 47.0% 389 57.5% 2,268 57.3%
No Program required
449 18.9% 325 36.0% 151 22.3% 925 23.4%
Medical discharge27
303
12.7% 99 11.0% 87 12.9% 489 12.4%
Discharge Own Request
66 2.8% 12 1.3% 16 2.4% 94 2.4%
Interstate Tsf. 44 1.9% 18 2.0% 9 1.3% 71 1.8%
Skills Waiver 27 1.1% 11 1.2% 17 2.5% 55 1.4%
Other28 25 29 1.1% 9 1.0% 7 1.0% 41 1.0%
25 Includes 2 x Foreign Military on Rehabilitation (Goal 1) 26 Table 1: ADF Rehabilitation Annual Report – FY 09/10 27 Rehabilitation Case has been closed and the case may have been transferred to DVA (if compensable), and either:
a) The member has already been Medically Discharged; or b) The decision has been made by the Service that the member is to be Medically Discharged, the member
has been advised of a discharge date and all rehabilitation plan actions are complete and there is no further value the Program Case Manager (PCM) can add
28 Includes Members who did not want to participate (opted out of Rehabilitation), were terminally ill and “other” reasons that do not fit into the categories listed. 29 Includes 2 x Foreign Military
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
63
Medical Waiver 6 0.3% 5 0.6% - - 11 0.3%
DVA Transfer 4 0.2% - - 1 0.1% 5 0.1%
Total 2,378 904 677 3,959 Table 9 Closed rehabilitation cases – by Service and ADFRP Closure Outcome – 2009/2010
5.4.4 Top 5 injuries by Service for Financial Year 2009/1030
Army Navy Air Force Totals
Disorders of the back
254 61.2% 76 18.3% 85 20.5% 415 12.1%
Disorders of the knee
370 66.2% 93 16.7% 95 17.1% 558 16.2%
Other musculo-skeletal
1,172 68.2% 284 16.5% 263 15.3% 1,719 50.0%
Mental Health disorders
262 45.4% 218 37.8% 97 16.8% 577 16.8%
Obesity 54 32.3% 71 42.5% 42 25.1% 167 4.9%
Totals 2,112 742 582 3,436 Table 10 Top 5 injuries – by Service – 2009/10
Note:
Information on how a member entered the ADFRP (self-referral, referral from CO, referral from MO) was not available.
Information on the MEC classification level of a member receiving rehabilitation was not available.
5.5 Liability determination/ compensation DVA’s service charter states:
• action or acknowledge your correspondence within 28 days;
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• attend to you within 10 minutes of your specified appointment time;
• process travel claim reimbursements within 28 days; and
determine claims for:
• compensation under the Veterans’ Entitlements Act 1986, on average, within 75 days of lodgement, or inform you if a determination is going to be delayed;
• initial liability under the Military Rehabilitation and Compensation Act 2004, on average, within 120 days of lodgement, or inform you if a determination is going to be delayed;
• initial liability under the Safety, Rehabilitation and Compensation Act 1988, on average, within 120 days of lodgement, or inform you if a determination is going to be delayed; and
• income support pensions, on average, within 32 days of lodgement, or inform you if a determination is going to be delayed.31
Table 11
describes DVA’s clients – by type at 30 Jun 2010.
VEA major beneficiaries MRCA and SCRA major benefits
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
65
5.5.1 Beneficiaries – VEA, MRCA and SRCA At 30 June 2010, there were 367,815 Veterans’ Entitlements Act 1986 (VEA) beneficiaries and a total of 14,510 Military Rehabilitation and Compensation Act 2004 (MRCA) and Safety, Rehabilitation and Compensation Act 1988 (SRCA) beneficiaries who received benefits in the past two years. 33 Table 12 This is represented, by age group, in and Table 13 below.
Age group – VEA beneficiaries Total %
Under 55 years 28,291 7.7%
Between 55 and 59 years 17,747 4.8%
Between 60 and 64 years 42,937 11.7%
Between 65 and 69 years 24,427 6.6%
Between 70 and 74 years 20,263 5.5%
Between 75 and 79 years 28,691 7.8%
Between 80 and 84 years 69,494 18.9%
Between 85 and 89 years 99,696 27.1%
Over 90 years 36,269 9.9%
TOTAL 367,815 Table 12 VEA beneficiaries by age - as at 30 June 201034
Over 55% of VEA beneficiaries are aged 80 years or over.
Less than 8% of VEA beneficiaries are aged under 55 years.
33 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 27 34 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 28
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
Age group – MRCA and SRCA beneficiaries Total %
Under 20 years 51 0.4%
Between 20 and 24 years 627 4.3%
Between 25 and 29 years 1,533 10.6%
Between 30 and 34 years 1,732 11.9%
Between 35 and 39 years 2,135 14.7%
Between 40 and 44 years 1,903 13.1%
Between 45 and 49 years 1,448 10.0%
Between 50 and 54 years 1,073 7.4%
Between 55 and 59 years 1,031 7.1%
Between 60 and 64 years 1,317 9.1%
65 years or more 1,660 11.4%
TOTAL 14,510 Table 13 MRCA and SRCA beneficiaries who received benefits in the two years to Jun 201035
5.5.2 Claims processing There were 9,649 new VEA Veterans’ Income Support and Allowance claims during FY 2009-10. This represents a decline of 24% from the 12,711 cases last financial year. This reduction is attributable to the number of surviving veterans with qualifying service steadily declining and there being no new policy proposals to stimulate increases in claims. 36
There were 16,821 primary claims for VEA Veterans’ Disability Support during FY 2009/10.
37
During FY 2009/10 there were 2,589 incapacity payees under SRCA and 3,381 initial liability claims for injury received. These payees receive benefits during the year for differing periods according to the length of time they were unfit for service and whether they are on a current
35 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 30 36 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 109 37 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 114
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
67
rehabilitation program. It is possible that one member can be included multiple times within this figure where incapacity payments are made for more than one separate period. 38
During FY2009/10 there were 1,254 incapacity payees under MRCA and 3,181 initial liability claims for injury received.
39
Table 14
below shows the average claims processing times against DVA’s average target claims processing time. It highlights that, on average Veterans’ Income Support and Allowance and MRCA Incapacity payee claims were processed outside DVA target processing times.
Claim type Mean time (days)
Target (days)
Veterans’ Income Support and Allowances (VEA) 43 32
Veterans’ Disability Support (VEA) 70.340 75
Incapacity payees (SRCA) 8941 120
Incapacity payees (MRCA) 123 120 Table 14 Claim processing times - actual vs. target, for FY 2009/1042
Table 15
highlights that approx one quarter of MRCA primary claims take in excess of 6 months to be decided.
30 Jun 2008 30 Jun 2009 30 Jun 2010
No. % No. % No. %
4 months or less 617 64% 691 60% 705 60%
Between 4 – 6 months 146 15% 189 16% 180 15%
Between 6 – 12 months 174 18% 259 22% 259 22%
Greater than 12 months 25 3% 22 2% 32 3%
TOTAL 962 1,161 1,176 Table 15 Undecided MRCA primary claims by age at 30 Jun 2008, 2009 and 201043
Issues which impact on the time required to process a claim, and therefore the target average processing times under each of the three Acts include:
38 Department of Veterans’ Affairs Annual Report 2009/10 page 131 39 Department of Veterans’ Affairs Annual Report 2009/10 pages 135 and 137 40 Department of Veterans’ Affairs Annual Report 2009/10 page 114 – Processing a primary claim (days) 41 Department of Veterans’ Affairs Annual Report 2009/10 page 132 42 Department of Veterans’ Affairs Annual Report 2009/10 Performance Reporting section 43 Department of Veterans’ Affairs Annual Report 2009/10 Performance Reporting section page 137
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• Establishing member proof of identity (POI). With VEA claims, the majority of claimants have claimed previously and are already in receipt of ongoing payment from DVA - hence they have already established POI to our satisfaction. With MRCA and SRCA claimants, the majority have not claimed previously so POI must be established in full.
• Location of and provision of required service and health information and records. With VEA, service documents have usually been requested previously so DVA often have a copy of all required documents on the file. With MRCA and SRCA claims – DVA experiences significant delays in obtaining necessary documentation from Defence. Refer 9.1.12
• Obtaining a Specialist diagnosis of the claimed condition (including Specialist waiting list delays). Where Defence does not have a definitive diagnosis from a Specialist regarding musculo skeletal claims from serving members, X-rays/scans and specialist appointments are required. SRCA requires a diagnosis from an appropriate Specialist. MRCA/SRCA claimants are more likely to be working (or even serving overseas) and it is more difficult to make medical appointments which are suitable to them. With VEA claims, the LMOs are often able to provide documentation confirming diagnoses of claimed conditions because they have an established relationship with the member.
• Assistance provided by advocates. Additional assistance is provided for VEA claimants through TIP trained ESO advocates. ESOs are much more proficient with the VEA and a higher percentage of VEA claimants go through ESOs. ESOs are able to assist the veterans submit well prepared claims.
• DVA processing systems – separate processing systems and databases for each Act.
5.5.3 Claims lodgement As at Aug 2010, the average elapsed time between incident/ injury and the member submitting a claim with DVA is 1.6 years (570 days) for MRCA claims and 16.7 years (6,113) for SCRA claims.44
44 Information provided by DVA Director Defence Links - MRCA stats excludes all non-primary removed (AAT, Recons, and VRB). SRCA stats exclude Removed claims with no MCRS received date or Date of Effect recorded and excludes all Claims where the TTTC (total days) is less then 0
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
69
5.6 ADF Separations
2008-09 Actual45
2007-08 Actual 46
2006-07 Actual
47 2005-06 Actual
48
Army
2,767 10.3% 2,735 10.6% 2,967 11.9% 3,122 12%
Navy 1,383 10.8% 1,395 11.0% 1,554 12.3% 1,446 11%
Air Force 893 6.4% 982 7.2% 1,199 9.0% 1,083 8%
Total 5,043 9.4%49 5,112 9.8%50 5,720 11.2%51 5,651 11%52
Table 16 ADF separation figures, by Service for FY 2005-6 to 2008-09
Notes:
• % representation is the 12-month rolling separation rate for the Permanent Force.
• These figures represent headcount.
45 Defence Annual Report 2008-09 Volume 1 Page 196 46 Defence Annual Report 2007-08 Volume 1 Page 109 47 Defence Annual Report 2006-07 Volume 1 Page 136 48 Defence Annual Report 2005-06 Volume 1 Page 228 49 12 month rolling separation rates for the Permanent Force – Defence Annual Report 2008-09 Volume 1 Page 209 50 12 month rolling separation rates for the Permanent Force – Defence Annual Report 2007-08 Volume 1 Page 109 5112 month rolling separation rates for the Permanent Force – Defence Annual Report 2006-07 Volume 1 Page 136 52 Separation rates for the permanent force – Defence Annual Report 2005-06 Volume 1 Page 228
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
5,043 5,112 5,720 5,651 Table 17 Separation breakdown - by Service
Where: • V = “Voluntary” – includes voluntary redundancies and resignations
• I = “Involuntary” – members who are medically unfit, unsuitable for further duty, who died whilst serving or who fell into the “Management Initiated Early Retirement” category
Totals 2,095 1,157 730 3,982 Table 18 Separation Reason FY 2009/10 - by Service
Note 1: Data excludes separation of members on CFTS (Army 1,029, Navy 313, Air Force 291 – predominantly classified as “Military – Completed CFTS in data”)
Note 2: Defence Annual Report figures for FY 09/10 not available at time of report preparation
57 Data extracted from PMKeys – (2009 Q3, 2009 Q4, 2010 Q1, 2010 Q2 – Number of Terminations 58 Includes False Statement on Enlistment, Disciplinary, Failed to Enlist, In Absence, Civil Offence 59 Includes Compulsory Retirement Age, Management Initiated Retirement, Retired after Age 55 60 Includes Unfit for Service DPR 87-1-e, Completed CFTS
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
Totals 2,723 1,435 867 5,025 Table 19 Separation Reasons FY 2008/09 - by Service
Note 1: Analysis excludes separation of members on CFTS (Army 1,439, Navy 237, Air Force 344 – predominantly classified as “Military – Completed CFTS in data”)
Note 2: Defence Annual Report figures for FY 09/10 not available at time of report preparation
61 Data extracted from PMKeys – (2008 Q3, 2008 Q4, 2009 Q1, 2009 Q2 – Number of Terminations 62 Includes False Statement on enlistment, Disciplinary, Failed to Enlist, In Absence 63 Includes Compulsory Retirement, Management Initiated Retirement, Retired after Age 55 64 Includes Completed CFTS, Contest Election, Irregular Enlistment
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
6 Current system
6.1 Interactions between member, service providers and support Figure 17 highlights the entities involved in the support for injured or ill members. It also represents a member’s interactions with processes including MEC, Determine Liability and Separation. There are many stakeholders involved and therefore many handoffs and interactions – this attests to the complexity of some member’s situations.
The importance of ‘Command, Welfare and Casualty Management’ and its 7+ interactions points in the support or injured or ill members are highlighted. The red circles labelled “entitlements” refer to DVA entitlements and include VVCS support.
Separation
OH&SIncident
Managementand
Incident Prevention
Health Rehabilitation
CentrelinkDVAComSuper
ComCare
Command, Welfare and Casualty Management
MEC
Determine Liability
Entitlements
DCO Family
EntitlementsDCO Family
Figure 17 Interactions an injured or ill member may have with the "system"
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
6.2 Description of the “system” For the purpose of this analysis, the in scope end to end processes and activities which support an injured or ill member is described as the “system”. It is really a collection of systems – such as the Medical/ clinical care system, rehabilitation system etc.
The end-to-end in scope processes relevant to the support available and provided to injured or ill members is documented in significant detail in the process summary tables and process maps in Appendix B. Relevant process steps, stakeholders, controls and technology is captured in each map.
The relationship between key systems and processes within the SIIP is displayed in Figure 18. It is important to note that this diagram is a broad representation of situational procedures and processes and does not describe an individual member’s circumstances or journey through the system. Although the process, as displayed below, appears linear this is certainly not the case – there are many system activities that can occur in parallel - such as rehabilitation, liability determination and separation activities. The member perspective of the “system” – and the way they interact with it and move through it is represented in Figure 17 on the preceding page.
Occ. Health and Safety
Injury Prevention
Illness Prevention
Incident/ Presentation
Rehabilitation
Return to ADF Duty
(MEC1 and MEC2)
Determine Liability/ Compensation
Medical Separation
Primary Healthcare/ Treatment
Key systems within Support for Injured or Ill Project (SIIP)
Superannuation
Post Separation healthcare Services:
• DVA• External
healthcare providers
• Centrelink• ComSuper
TransitionServices
Figure 18 Key systems relevant to the support provided to injured or ill members
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
The systems and process objectives are defined as follows
• Occupational Health and Safety/ Injury Prevention/ Illness Prevention - A Defence environment where people work together to improve capability by preventing injury and illness and effectively managing their impact on people, reputation, recruitment and retention. Noting this element of the system is out of scope for the SIIP review so this is not a comprehensive representation of the OH&S function within Defence.
• Incident/ Presentation - The appropriate course of action, including notification and/or treatment, is initiated following an incident.
• Primary Healthcare/ Treatment - ADF members receives necessary/ required primary healthcare and/or treatment for their injury or illness.
• Rehabilitation - Goal 1: Fit for duties and rehabilitate to pre-injury status Goal 2: Fit for duties with change in duties/ location/ service Goal 3: Stabilise then transition out of ADF to the civilian environment
• Determine Liability/ Compensation - To enable a member who has been a compensable injury or illness to have their liability determined and receive their entitlements and compensation
• Return to ADF Duty (MEC1 and MEC2) - Member returns to ADF duty
o MEC1: Members who are medically fit for employment in deployable or sea going environments without restriction
o MEC2: Members who have medical conditions that require access to various levels of medical support or employment restrictions, however they remain medically fit for duties in their occupation in a deployed or seagoing environment
• Medical Separation - Ill or injured member medically separates in an efficient and effective manner. Member is supported through separation process.
• Transition Services - Reasonable assistance and support provided to ADF member to ensure a smooth transition to civilian life. This includes a smooth transition of case management to DVA (if applicable) and confirmed engagement with members post separation to ensure successful transition
• Superannuation - To determine ill or injured member’s eligibility for superannuation and to initiate timely payment of superannuation entitlements.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7 Available support The following matrix describes the support services generally available to injured or ill members and their families. There are a number of factors which, when overlayed, introduce significantly more complexity into this matrix. These factors include:
• Mental Health considerations;
• “Family” dynamics;
• Whether the injury or illness is compensable;
• Very Serious Injuries or Incidents (including where there are multiple instances/ casualties); and
• High profile cases including those with media involvement.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
Available support/ service providers Section reference
A: C
urre
nt A
DF
Mem
ber -
N
ot d
eplo
yed
B: C
urre
nt A
DF
Mem
ber -
D
eplo
yed
C: C
urre
nt A
DF
Mem
ber
CFT
S - N
ot d
eplo
yed
D: C
urre
nt A
DF
Mem
ber
CFT
S - D
eplo
yed
E : F
orm
er M
embe
r -
Act
ive
Serv
ice
F : F
orm
er M
embe
r - N
o A
ctiv
e Se
rvic
e
G: R
eser
vist
- not
on
CFT
S
H: S
epar
atin
g A
DF
Mem
ber
I : Li
abili
ty A
ccep
ted
(DV
A)
Fam
ily o
f A
Fam
ily o
f B
Fam
ily o
f C
Fam
ily o
f D
Fam
ily o
f E
Fam
ily o
f F
Fam
ily o
f G
Fam
ily o
f H
Garrison Health Support Branch (JHC) 6.1 Y Y * YDirectorate of ADF Rehabilitation Services 6.2 Y Y Y Y YDefence Force Psychology Organisation (DFPO) 6.3 Y Y Y Y YADF Mental Health Strategy (ADFMHS) 6.4 Y Y Y Y YADF Transition Services 6.5 Y YDefence Community Organisation (DCO) 6.6 Y Y Y Y Y Y Y Y Y YDepartment of Veterans' Affairs (DVA) (Note 1) 6.7 Y Y Y Y Y Y Y YTransition Management Service (TMS) 6.8 YVVCS - Veterans and Veterans Families Counselling Service (VVCS) 6.9 Y Y Y Y Y Y Y Y Y YDefence Housing Australia (DHA) 6.10Australian Centre for Post-Traumatic Mental Health (ACPMH) 6.11Chaplaincy/ Padres 6.12 Y Y Y Y Y Y Y Y YNational Welfare Coordination Centre (NWCC) 6.13 Y Y Y YAll-hours Support Line (ASL) 6.14 Y Y Y Y Y Y Y Y1800 IMSICK 6.15 Y YEmergency Support to Families Scheme (ESFS) 6.16 Y YOperation CARE (RSL) 6.17 YAUSDIL 6.18 Y Y Y Y YDefence School Transition Aide (DSTA)/ Defence Transition Mentor (DTM) 6.19 Y Y Y YTrade Transfer and Retention 6.20 Y Y Y Y Y Table 20 Support Services available to ADF members and their families
Note 1: DVA may be involved with a member in categories A-G. A member can make a claim whilst still serving and receive benefits such as permanent impairment (PI) payments.
Further details on these services follow.
78
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7.1 Garrison Health Operations Branch The services provided through Garrison Health Operations Branch, for all members eligible for ADF healthcare (in accordance with DI(G)PERS 16-1 Healthcare of Australian Defence Force Personnel) include:
• Medical outpatient departments/services;
• Dental outpatient departments/services;
• Psychology/ mental health;
• Case management and complex case management;
• Physiotherapy;
• Pharmacological;
• Imaging;
• Inpatient medical services including operating theatres at two locations;
• Laboratory Services;
• Referrals to specialist services; and
• Communication with Command.
7.2 Directorate of ADF Mental Health, Psychology and Rehabilitation (DMHPR) The Directorate of ADF Rehabilitation Services is responsible to the CJHLTH and the Service Chiefs for overseeing the effective and efficient coordination and delivery of four inter-related rehabilitation programs as follows:.65
The Directorate reduces the impact of injury or illness on the ADF through the delivery of the following programs:
• ADFRP;
• ADF Compensation Support;
• ADF Integrated People Support Strategy activities related to JHC; and 65 http://intranet.defence.gov.au/vcdf/sites/DRS/chkLink.asp?URL=comweb.asp?page=43192
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• ADF Paralympic Sports Program.
7.2.1 ADF Rehabilitation Program (ADFRP) The purpose of the ADFRP is to ensure Defence meets its duty of care obligations and legislative responsibilities to its members. It provides a nationally consistent and managed rehabilitation process drawing on multi-disciplinary professional services aimed at maximising a member’s potential for restoration to pre-injury status (physical, occupational, social, educational and psychological).
The ADFRP is delivered by the Garrison Health Support Branch as an allied health service on behalf of the Service Chiefs. The Service Chiefs have delegated their authority for clinical, vocational and psychosocial rehabilitation to JHC.66 CJHLTH is accountable to VCDF and the Service Chiefs for the delivery of health services including ADFRP.67 68A member must be eligible for health care to be eligible for the ADFRP.69
The ADFRP was developed to sustain ADF capability by assisting members return to a state of readiness as soon as is practicable after injury or illness through the provision of a personal case manager and structured support. It is workplace or occupational based as this provides the most realistic environment to assess fitness for work through the restoration of productive work functioning and focuses on:
• Achievement of optimal physical and mental recovery;
• Return to suitable work at the earliest possible time;
• Returning ADF members to a deployable level of fitness where possible, in a timely and cost efficient manner; and
• The reduction of the human and economic cost of disability to members, the ADF and the broader community.
“The ADFRP aims to achieve a seamless rehabilitation process through the early identification of injury of illness, coordinated clinical and occupational rehabilitation as well as vocational retraining. The success of any occupational rehabilitation program is dependent on all key stakeholders working together to achieve successful outcomes directly related to the member’s needs, duties and workplace.”70
The ADFRP enables Defence to meet its duty of care obligations under relevant legislation including: 66 The Service Chief’s powers and functions as a member’s Rehabilitation Authority are delegated to the Directorate of ADF Rehabilitation Services and the ADF Rehabilitation Coordinators by signed instruments under Section 162 of the SRCA and Section 438 of the MRCA. 67 DI(G)PERS 16-22 Australian Defence Force Rehabilitation Program 68 Service delivery aspects of the ADRFP are addressed through Service Level Agreements between the Services and JHC 69 DI(G)PERS 16-1 Health Care of the Australian Defence Force Personnel 70 DI(G)16-22 page 7
80
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Military Rehabilitation and Compensation Act 2004 (MCRA);
• Occupational Health and Safety Act 1991; and
• Safety Rehabilitation and Compensation Act 1988 (SCRA).
Figure 19 provides an overview of the functions, outputs and enablers of Defence Rehabilitation and Compensation Service Delivery framework. A comprehensive description of these elements is available in Australian Defence Force Rehabilitation Program (ADFRP) Review Work Package 2 – Governance Framework – 2 October 2007.
Figure 19 Australian Defence Force Rehabilitation Program Service Delivery Framework
ADF Rehabilitation Coordinators (RC) The ADF Rehabilitation Coordinators are responsible for the contracting and coordination of rehabilitation case management services. They work to the Deputy Director - Operations (DDOPS) of the DRS and are responsive to the needs of Units and Commanders in coordinating rehabilitation services for members.
Sustainment
Health Care
Rehabilitation
Compensation
Career Management
Transition Management
Program Case Management
Services Program Case Management
Services Capability
Management
Program Case
Management Services
SRCA & MRCA
Delegations Capability and Goal
Achievement Reports /
Information
Rehabilitation Coordination and Liaison Rehabilitation
Assessments
MECR Assessments
Health and Medical
Services
R & C Referrals
Rehabilitation Referrals
SRCA & MRCA
Delegations Notification of
Claim Lodgement
Referral for Compensation
Capability Goal Achievement and Program
Reports
Assessment of Medical Aid
Requirements
MECR Assessments
Retraining Training
Programs Program Case Management
Advice
Vocational Assessments
Information on Compensation
Claims
Program Case Management
DVA Claim Notification
Compensation Coordination
Function Output Enabler
Deployability Employability
Career Advice
Capability and Goal
Achievement Reports /
I nformation Awareness and Communication
SRCA & MRCA Delegations
Rehab Assessment
SRCA & MRCA Delegations
Defence Delegations
R & C Coordination and Advisory
Services
Rehabilitation Plans
Advice to Command /
PCM Referral to Rehabilitation
Referral to Compensation
Reoccurring Claim
Information
MEC Review Posting
Referral to Transition
Management SRCA & MRCA Delegations
MECR Assessments
Rehabilitation Assessments
Referral to Compensation
Information to Assist
Transition
Services to assist with
Civilian Employment
Referral from Career
Management
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
RC duties include to:
• Arrange and coordinate rehabilitation assessments and rehabilitation programs (as the delegate of the Rehabilitation Authority);
• Procure and manage rehabilitation case management service providers and monitor their performance;
• Monitor and review member's rehabilitation programs;
• Assist in the development and implementation of the ADFRP;
• Manage, collect, analyse and report ADFRP performance data and expenditure;
• Manage rehabilitation related administration activities including the rehabilitation database, operating procedures and documents; and
• Manage effective workplace relationships including the coordination of activity and the flow of information between members, Commanders and managers, internal and external health and rehabilitation providers and the DVA.
7.2.2 ADF Compensation Support In accordance with compensation legislation, the ADF Compensation Support Team receives and registers copies of compensation claims and determinations from DVA. Defence uses this information to ensure Service Chiefs have visibility of the health status of serving members, in order to manage any medical and/or rehabilitation requirements of the individual. The legislation affords for the provision of claim information to Defence for the purpose of meeting readiness criteria and to provide visibility of the health status of ADF personnel.
7.2.3 ADF Integrated People Support Strategy activities Refer to 7.4.1.
7.2.4 ADF Paralympic Sports Program (ADFPSP) The Australian Defence Force Paralympic Sports Program is a JHC program providing high-level rehabilitation and support services and adaptive sport for members who have acquired a disability.
The services are delivered through a strategic partnership with the Australian Paralympic Committee (APC) which is the national governing body for Paralympic sport in Australia. This partnership provides the ADFPSP with access to subject matter expertise and elite coaching services.
82
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
The ADF Paralympic Sports Program aims to assist severely injured ADF members regain and maximise their functional independence by:
• Facilitating and supporting the attainment of physical fitness and an active lifestyle. This is achieved through member participation in high performance camps and adaptive sport;
• assisting members to meet the physical fitness requirements of DI(G)PERS 16-11;
• the provision of support;
• development and distribution of information resources to support severely injured members and their families;
• Delivering the MATES mentoring program - enables suitable current and former ADF members to mentor colleagues with similar injuries and assist them in their rehabilitation;
• providing networking opportunities with other ADF members with an acquired disability; and
• Developing an ADF adaptive sport policy and adaptive sport pathways.
7.3 ADF Mental Health Strategy (ADFMHS) The ADFMHS recognises that mental health is not solely related to diagnosable mental disorders, but encompasses a broad range of lifestyle, mental wellbeing and job performance factors. The Strategy has a primary focus on prevention and evidence-based treatment to maximise retention and enhance the quality of life for Defence personnel. It is being implemented through the Directorate of Mental Health, Psychology and Rehabilitation.. 71
7.3.1 Integration and Enhancement of ADF Mental Health Services
The six key initiatives within the ADFMHS are listed below.
This initiative has resulted in the development of 22 Regional Mental Health Teams (RMHT) which have been established to support personnel within Australia as well as two mental health teams for operational environments. Liaison with key stakeholder and other organisations on matters of mutual interest is of a high priority, particularly with respect to the liaison with the DVA to maintain continuation of mental health care for ADF members post separation.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7.3.2 ADF Mental Health Research and Surveillance ADF mental health research is focused on care of the member and enhancement of operational capability.
7.3.3 Enhanced Resilience and Wellbeing Collaborative work with the ACPMH on the course and predictors of psychological resilience (risk and protective factors) over the first 3 years of service in the ADF.
7.3.4 ADF Critical Incident Mental Health Support The provision of Critical Incident Mental Health Support (CIMHS) is a fundamental part of the ADF's response to critical incidents and potentially traumatic events. Developed in conjunction with the ACPMH, CIMHS is considered best practise and offers a framework to mitigate and alleviate possible psychological injuries following a critical incident. Consistent with the stepped care approach to mental health in the ADF, CIMHS assets are multi-disciplinary and include a range of Mental Health Peers, Providers, Professionals and Specialists trained internally through a Train the Trainer model.
7.3.5 ADF Suicide Prevention Program Through collaboration with Living Works, the ADF introduced ASIST courses into the ADF. Additionally, suicide awareness training is conducted annually for all ADF members and more recently, the ADF commenced rollout of suicide first aid training as a component of the Keep Your Mates Safe series (Keep Your Mates Safe - Suicide) and Clinical Upskilling for Mental Health Professionals working with clients/patients experiencing a suicidal episode.
7.3.6 Alcohol Tobacco and Other Drugs Program (AToDP) The Alcohol Tobacco and Other Drugs Program facilitates education, training and treatment programs in the ADF including.
• AToDP Awareness Course
•
: an overview of the effects of alcohol, tobacco and other drugs (ATOD) use, information on issues and trends in ATOD use/management and ATOD treatment services within the ADF.
Keep Your Mates Safe (KYMS) Alcohol Workshop
•
: is an education workshop that informs members how to keep themselves and mates safe / safer when out drinking.
Outpatient Alcohol Treatment Program (OATP)
•
is a 4-day group program which aims to educate members on the various techniques and strategies useful in successfully reducing alcohol intake to safe levels.
Alcohol Rehabilitation and Education Program (AREP) – AREP’s mission is to rehabilitate alcohol dependent ADF members by catering for their physical, psychological, emotional
84
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
and spiritual needs and return them to the workforce as active, reliable members. AREP also offers outpatient counselling and aftercare support for local members. As alcohol dependence impacts on the family unit, spouses are encouraged to attend during the fourth (and final) week of the program.
• ADF Outpatient Alcohol Treatment Program (OATP)
•
- is an evidence based group program which aims to minimise alcohol misuse amongst ADF members. The program is run over four consecutive days at various bases around Australia. The program has been running nationally since 2005.
Royal Australian Navy Alcohol and Other Drugs Program
7.4 ADF Transition Services
(RANAODP).
7.4.1 ADF Integrated People Support Strategy (IPPS) IPSS is the framework through which Defence sustains a whole of government approach to the provision of adequate and accurate information on the support services available to ADF members and their families. The IPPS has four (4) pillars:
• Through Service Support – ensure ADF members and their families are informed of and encouraged to access educational, financial, rehabilitation and other services throughout their careers to facilitate sound planning during times of need, including separation.
• Separation Ready – ensure all reasonable assistance and support is available and utilised by members and their families preparing to transition to civilian life, particularly for those members who have been injured and require rehabilitation as a result of their service in the ADF. This pillar also seeks to ensure the smooth transition of case management services to DVA and other support agencies where applicable.
• Separation Reconciliation – maximum effort to ensure all Defence related matters are resolved before transition occurs.
• Separation Review – maintain continued engagement with members post-separation to ensure successful transition. This includes engagement with those who may wish to re-enlist with the ADF.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7.4.2 ADF Transition Centres Defence provides separation service to all ADF members. This service is provided through regional ADF Transition Centres – of which there are 18 nationally, located near major Defence establishments. 72
The Centres provide an environment where a member and their family can discuss all aspects of their separation. This support extends to providing ADF members and their families with an individually tailored service to assist them in successfully planning their post-separation life.
The Transition Centres are responsible for providing transition and support service related information as well as ensuring all separation administrative requirements are completed prior to the member’s date of separation.
7.4.3 ADF Transition Seminars The ADF Transitions team conduct 25 times 2-day Transition Seminars per year – in various locations throughout Australia. A standardised agenda operates for each seminar – ensuring consistency in delivery of information to members who are separating.
The Agenda includes information on/ presentations from:
• Transition Support Services (TSS);
• Your career and you – a new world of work, skills and competencies, the tools of good career decision and management;
• Financial management – personal wealth creation and financial management, Financial Advisers, Understanding the Healthcare System, Non-military superannuation, protecting assets and operating a business.
72 Transition Support Service Report – dated 29 Oct 2009 proposed the rationalisation of ADF transition centres from 18 to 10, with the redistribution of staff and resources. This report is being revisited to take account of SRP, changes to the regional structure and the requirement to fully implement and deliver the IPSS. Transition Support Service Newsletter September 2010
86
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7.4.4 Career Transition Assistance Scheme (CTAS) CTAS provides members with assistance that will facilitate their transition to civilian employment on separation. Benefits are determined by length of qualifying service and include:
• Career transition training – vocationally-oriented education and training;
• Career Transition Management Coaching – identifying transferable skills, career options, job search strategies;
• Resume coaching; and
• Financial coaching.
7.5 Defence Community Organisation (DCO) On behalf of Command, the Defence Community Organisation provides a broad range of individual and program related services to the ADF community including COs, uniformed members (including single members) and families. Many of these services aim to support ADF personnel and their families to balance the demands of military service with personal and family commitments. These services and programs are delivered by DCO Area Teams, located on or near major ADF establishments around Australia.
DCO provides assistance in the case of accident, illness, hospitalisation and financial difficulty and in managing casualties and estates at times of bereavement. All members of the ADF and their families are entitled to access the DCO.
The Defence Community Organisation works with:
• Service Commanders at all levels;
• Defence members and their families;
• Defence Chaplains, Padres and Psychologists; and
• Defence sponsored groups, allied service providers and other agencies at local, state and federal government levels.
DCO is guided by the policy DI(G) PERS 42-1 Amdt No1 Australian Defence Force Family Support Policy.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
DCO offices are staffed by:
• Defence Social Workers (DSW): qualified professionals who are knowledgeable about the Defence lifestyle and system. The services they provide include limited counselling and casework services which focus on assessment and referral. The DSW also assists members and their families through community development programs, group work and educative programs and referrals to appropriate services and agencies within the community. The DSW may also provide advice, assistance and professional reports to Command as required, particularly for requests based on compassionate or family grounds.
• Military Support Officers (MSO): uniformed members from the three Services who provide support, advice and assistance to individual clients and undertake a liaison function with Units and Command. They have a particular role with Command and families in the event of illness or if there is a death of a serving member. MSOs provide advice, assistance and practical support to members and their families in relation to military matters.
• Regional Education Liaison Officers (RELO): professionally trained teachers with an understanding of the different State and Territory education systems and the Defence environment. They are available to provide advice to Defence families on education issues, particularly matters relating to mobility and relocation. REDLOs can assist with the transition between State and Territory primary, secondary and tertiary education systems.
• Family Liaison Officers (FLO): provide community based information, support and assistance to individual members, partners, families and Defence sponsored groups. These services are available at any time, however FLOs are particularly proactive in regard to welcome activities in relation to a new posting and settling in to a new area, or during the deployment of ADF members. 73
7.6 Department of Veterans’ Affairs (DVA)
DVA delivers government programs for war veterans, members of the ADF, members of the Australian Federal Police and their dependants.
Outcomes against which the DVA performance is measured against include ensuring eligible veterans, serving and former members, their war widows and widowers and dependants have access to:
• Appropriate compensation and income support in recognition of the effects of war and defence services
• Health and other care services that promote and maintain self-sufficiency, well being and quality of life
• Advice and information about benefits, entitlements and services; and
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Support services provided through joint arrangements between DVA and Defence.
DVA administers the Veterans’ Entitlements Act 1986 (VEA), the Safety, Rehabilitation and Compensation Act 1988 (SRCA) and the Military Rehabilitation and Compensation Act 2004 (MRCA).
7.6.1 Pensions, allowances, compensation, supplements and other benefits Pensions and allowances available to eligible members and their dependants through the DVA include:
• Pension: disability compensation (VEA) - a tax-free benefit paid to Australian veterans who have had an illness or injury accepted by DVA as being caused by their service, prior to 1 July 2004. Supplements and allowances, which can be paid in association with disability compensation, include clothing allowance, attendant allowance, recreational transport allowance and recognition of certain medals and decorations.
• Pension: income support (VEA) - provides a regular income for people with limited means. A service pension can be paid to eligible veterans (with qualifying service) on the grounds of age or invalidity and to eligible partners. Widows and widowers may be eligible for the Income Support Supplement.
• Pension: War Widows and Widowers, Orphans (VEA) – a tax-free pension paid when the death of the veteran is accepted as being caused by service, or to widow/ers of recipients of certain rates of disability pension.
• Incapacity Benefits - taxable payments for economic loss due to the inability to work because of an accepted condition.
• Payments: Permanent Impairment (PI) (CRCA/MRCA) - Compensation for any permanent physical and/or mental impairment in combination with any lifestyle restrictions which an eligible member may be suffering as a result of injuries or diseases accepted as being related to the member’s ADF service.
Supplement payment assist with the cost of prescriptions, rates, telephone and internet connections, energy, water and sewerage and include:
• Pension supplement,
• Seniors supplement;
• Veterans supplement; and
• MRCA supplement.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7.6.2 Health Care Health care under the VEA is provided through the Repatriation Health card system. Certain MRCA clients may also be provided with a Repatriation Health Card while others are reimbursed for costs of reasonable medical treatment (after separation from the ADF). SRCA clients are reimbursed for reasonable medical treatment costs.
A broad range of health care and support services is available to meet the clinical needs of eligible veterans and eligible dependants including:
• General practitioner services;
• Medical specialist services including pathology and radiology;
• Allied health services including podiatry and physiotherapy;
• Dental care;
• Community nursing;
• Spectacles and hearing aids;
• Care in public and private hospitals;
• Ηome support services; and
• Subsidised pharmaceuticals under the Repatriation Pharmaceutical Benefits Scheme (RPBS).
Holders of Gold (Repatriation Health Card – For All Conditions within Australia) and White (Repatriation Health Card – For Specific Conditions) cards are entitled to defined health care services at DVA’s arranged expense. Cardholder entitlement may also extend to aids and appliances. There were 207,945 Gold Card holders as at 30 Jun 2010.74 There were 49,621 White Card holders as at 30 Jun 2010.75
7.6.3 Rehabilitation Services
Under SCRA and MRCA, DVA can provide holistic rehabilitation services as follows:
• Medical rehabilitation: all reasonable treatment and approved allied health services for accepted conditions e.g. simple (physiotherapy) through to complex (teaching a member to walk again with special equipment).
74 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 28. This number includes a small number of MRCA card holders. 75 Department of Veterans’ Affairs Annual Report 2009/10 Overview – page 28. This number includes a small number of MRCA card holders.
90
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Psychosocial rehabilitation: referral to community support services, adjustment counselling, skill development, lifestyle programs, attendant care services, drug and alcohol management programs, assistance to a member and their family in adjusting.
• Vocational rehabilitation: assisting a member return to the workforce including assistance to adapt in their current job or assistance to find, or to train for, a more suitable job.
The Veterans’ Vocational Rehabilitation Scheme (VEA) is a voluntary vocational rehabilitation scheme which can assist eligible veterans requiring assistance to return to paid work, to increase their work hours, or who are at risk of losing their job or are finding it increasingly difficult to maintain their employment or require help with job seeking activities. The scheme can provide assistance for those who need to upgrade their skills or undergo short term retraining to gain employment.
7.6.5 Housing Subsidised loan assistance and insurance benefits are available to eligible current and former ADF personnel including:
• The Defence Service Homes (DSH) provides a subsidised loan of up to $25,000 repayable over 25 years to ex-service men and women (and certain dependents) who have completed a qualifying period of service in wartime or peacetime.
• A Home Support Loan of up to $10,000 to assist with the cost of home maintenance and modifications and other housing-related purposes.
• The Defence Home Ownership Assistance Scheme (DHOAS) is available to current and former ADF personnel, and their surviving partners, who have served in the ADF after 1 July 2008, completed a qualifying period and accrued a Service Credit.
• Defence Service Homes Insurance (DSHI) provides economical home and content insurance to all persons who are eligible under the VEA and/or the abovementioned schemes, regardless of whether they have a DSH or DHOAS loan.
7.6.6 Counselling services Refer to 7.8.
7.6.7 Health and wellbeing DVA provides links to advice, reference material and further information on:
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Physical health;
• Mental wellbeing;
• Caring including Veterans’ Home Care (VHC) Program which provides services to eligible veterans and war widows and widowers;
• Self management;
• Physical and social activities; and
• Health programs, publications, research and health related websites.
7.7 Transition Management Service (TMS) (DVA) Transition Management Service is a joint initiative under the Defence/DVA Links Project.
TMS assists full time serving members of the ADF who are separating from the ADF on invalidity grounds. DVA administers TMS on behalf of Defence. TMS operates as an extension of services already provided by Rehabilitation Coordinators within the MCRS.
The roles of Defence and DVA in providing TMS are defined in Appendix I.
7.8 VVCS - Veterans and Veterans Family Counselling Service (VVCS)
The VVCS is a specialised, free, confidential Australia wide service for Australian veterans and families, eligible peacekeepers and families and all F-111 deseal/ reseal workers and other F-111 fuel tank maintenance workers and their families. VVCS staff are professionally qualified with skills in working with life problems to do with service. They can also provide a wide range of programs and treatment for war and service related mental health conditions.
VVCS has a comprehensive Outreach Program, providing veterans and their families living in rural, remote and some outer metropolitan areas with access to contract counsellors and other health services.76
It is a specialised, free and confidential Australia-wide service available to:
• Australian veterans of all conflicts and peacekeeping operations as defined by the VEA;
• Partners and dependent children under 26 years of age of veterans with issues arising from the veteran’s service;
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• War widows/widowers;
• Ex-partners, within five years of separation;
• F-111 deseal/reseal workers and other F-111 fuel tank maintenance workers and their families;
• All children of Vietnam veterans regardless of age with psychological, emotional and social needs arising from the impact of their parent’s operational or warlike service;
• Ex-service personnel with a mental health condition as a DVA-accepted disability and their family member; and
• Current serving members of the ADF who have been formally referred by the ADF under the Agreement for Services.
VVCS provides services including:
• Individual, couple and family counselling;77
• Case management services (refer to
7.8.1);78
• After-hours crisis telephone counselling (Veterans Line – refer to
7.8.2);
• Group programs for common mental health issues (e.g. Anxiety, depression, sleep and anger);
• Psycho-educational programs for couples, including a residential lifestyle management program;
• Health promotion programs including Heart Health (refer to 7.8.3);
• Stepping Out Program (refer to 7.8.4);
• Operation Life Program (refer to 7.8.5);
• Changing the Mix Program (refer to 7.8.6); and
• Referral to other services and information, education and self-help resources.79
There were 10,789 unique clients receiving intake referral services from VVCS during FY 2009/10. 11,775 unique client counselling sessions were delivered (i.e. clients in receipt of counselling).
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7.8.1 Case Management Services The VVCS case management service is appropriate for eligible members and their families who have multiple issues impacting on their mental health and who may need help to manage the different health and social support services. Services may include medical, pharmaceutical, psychological, psychiatric, social, family, vocational and financial.
An eligible member and/or their families may self-refer. With an eligible member’s consent referrals can also be made from:
• General Practitioners;
• Psychiatrists;
• Psychologist/Social Workers; and
• Health or Human Service Professionals including allied health professionals, welfare workers, nurses, etc.
During FY 2009/10 there were 64 cases managed nationally.81
7.8.2 Veterans Line
Veterans Line is the after hours crisis counselling service provided by the VVCS.
The service is designed to assist veterans and their families in coping with crisis situations outside of VVCS office hours. Counselling is provided free of charge. 82
There were 4,610 calls received by the after hours counselling service during Fy 2009/10.
83
7.8.3 Heart Health Program
The Heart Health Program aims to increase a client’s physical health and wellbeing through practical exercise, nutrition and lifestyle management support. It is a year long program and includes two physical activity sessions per week that are tailored to meet individual needs.
The program covers topics including setting healthy goals, eating well, lowering alcohol consumption, communication and stress management, quitting smoking, taking care of your body, solving problems and maintaining a healthy heart.
The program is offered in two formats – the Heart Health Group Program and the Outreach Heart Health Program.84
80 Department of Veteran’s Affairs Annual report 2009/10 Page 162
81 Department of Veteran’s Affairs Annual report 2009/10 Page 165 82 http://www.dva.gov.au/health_and_wellbeing/health_programs/vvcs/services/Pages/veteransLine.aspx 83 Department of Veteran’s Affairs Annual report 2009/10 Page 162 84 http://www.dva.gov.au/health_and_wellbeing/health_programs/vvcs/services/Pages/heart_health.aspx
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
A total of 479 participants commenced the Heart Health Group Program during FY 2009/10, and at 30 Jun 2010 there were 30 groups running nationally. There were 67 enrolments in the Outreach Heart Health Program during the same period.85
7.8.4 Stepping Out Program
The Stepping Out Program aims to improve a member’s transition from Defence to civilian life. It focuses on lifestyle and personal issues facing ADF members and their families, both in the short and long term. Content includes:
• cultural differences between military and civilian life;
• development of skills and resources to benefit their new job and lifestyle;
• strategies for enhancing motivation, health and wellbeing ; and
• strategies for enhancing couple and family relationships during transition to civilian life.
The Stepping Out Program is voluntary. All members who are in the process of separating from the ADF, or have separated within the last 12 months, and their partners are eligible to attend. Members can self-refer or be referred through the ADF Transition Centres, Defence Rehabilitation Coordinators or TMS.86
During FY 2009/10, 22 programs were delivered nationally to 180 participants.
87
7.8.5 Operation Life Program
Operation Life provides a framework for action to prevent suicide and promote mental health and resilience across the veteran community. Its major components include a range of suicide prevention programs and services for the veteran community.88
7.8.6 Changing the Mix Program
“Changing the Mix” is a self-paced alcohol reduction program delivered via correspondence. 33 participants registered and received assistance from this self help program in FY 2009/10.89
85 Department of Veteran’s Affairs Annual report 2009/10 Page 168
86intranet.defence.gov.au/.../sites/chkDoc.asp?S=9079&D=73359&URL=docs/steppingoutprogramforseatalk.doc 87 Department of Veteran’s Affairs Annual report 2009/10 Page 168 88 http://www.dva.gov.au/health_and_wellbeing/health_programs/vvcs/services/Pages/operation_life.aspx 89 Department of Veteran’s Affairs Annual report 2009/10 Page 167
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
7.8.7 Vietnam Veterans’ Children’s Support Program (VVCSP) The program is available to children who were conceived after their parents’ service in Vietnam and who have spina bifida manifesta, cleft lip, cleft palate, acute myeloid leukemia or adrenal gland cancer.
The program offers a contribution towards medical, hospital and pharmaceutical costs associated with these conditions and provides assistance with necessary aids and appliances, home help, respite care, home modifications, physical rehabilitation and allied health services.
There were 65 children registered under this program and 18 of these children accessed services during FY 2009/10.90
7.9 Defence Housing Australia (DHA)
DHA can assist ill or injured members with housing special needs including provision of housing close to health care facilities. This process is facilitated through a 'Special Needs Recognition' letter or the 'Assessment of Assistance on Posting' letter.
If an ill or injured member in a DHA property requires property modifications including ramps, lighting or accessibility modifications, DHA will negotiate with the Head of Defence Corporate Support (HDCS) to approve the modifications. 91
7.10 Australian Centre for Post-Traumatic Mental Health (ACPMH)
The Australian Centre for Posttraumatic Mental Health (ACPMH) at the University of Melbourne undertakes world class trauma related research, policy advice, service development and education. Our innovative services help organisations and health professionals who work with people affected by traumatic events. Services include:
• Internationally acclaimed research into the incidence and impact of trauma;
• Development of standards for trauma assessment and intervention, including National Health and Medical Research Council approved guidelines for the treatment of posttraumatic stress disorder;
• Policy advice on prevention, early recognition, assessment, treatment and compensation;
• Strategic planning for the optimum provision of mental health services;
• Education and skills development for health professionals, policy makers and compensation staff; and
90 Department of Veterans’ Affairs Annual report 2009/10 Page 170 91 http://www.dha.gov.au/for-adf-members/specialneeds.html
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Evaluation and outcome monitoring .92
7.11 Chaplains/ Padres
Chaplains/ Padres provide pastoral care to serving members and their partners and families. All ADF serving members and their families can access the services of an ADF Chaplain/ Padre.
7.12 National Welfare Coordination Centre (NWCC) NWCC provides a 24-hour a day point of contact and information service for members and families of personnel deployed on or in support of operations and on designated exercises.
All deploying members are required to complete a Family Registration form which is lodged with the NWCC. It contains names, addresses and telephone numbers of emergency contacts and details of family circumstances Defence should be aware of.
7.13 All-hours Support Line (ASL) ASL is a triage service to help ADF members and their families access ADF or civilian mental health services more easily.
7.14 1800 IMSICK 1800 IMSICK is a toll free after hours nationwide service available to all permanent ADF members within Australia. The service is intended to assist ADF members obtain healthcare when they become ill or injured away from the workplace.
It is noted that there is a project within the Garrison Health Operations Branch to combine the ASL and1800 IMSICK.
7.15 Emergency Support for Families Scheme (ESFS) ESFS was developed to provide short-term assistance to an ADF member’s dependants in an emergency situation where the member is absent from the dependant’s location for service reasons.
7.16 Operation CARE The RSL & Services Clubs Association, the Returned & Services League of Australia and the Department of Defence joined forces in 2006 to establish Operation CARE.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
The scheme provides up to one week’s ‘Rest and Recuperation’ at sites throughout Australia for selected Defence personnel and their immediate family, where the member has been repatriated to Australia as a consequence of combat operations wounds. Operation CARE is extended to the widows of members killed in action.
The aim of Operation CARE is to assist wounded Defence personnel and their immediate family to recover from the physical scars from combat and by providing the member and family some quality time together in a relaxing and stress-free environment.
In launching the program in October 2006, CDF Air Chief Marshall Angus Houston, said the program would improve morale and retention of personnel and strengthen the relationship between veterans and current personnel:
“We hold our forebears in great regard and for them to be doing something like this for the young people who go out there today and serve is a huge step in the right direction and certainly adds to morale and hopefully will be another thing that supports the need to retain people in the ADF.”93
7.17 AUSDIL
Sponsored visits by next of kin, relatives or nominated persons to members of the Defence Force hospitalised through serious injury or illness.94
7.18 Defence School Transition Aide (DSTA) and Defence Transition Mentor (DTM)
DSTA (Primary school) and DTM (Secondary school) are programs funded by Defence but and provided by State Education Departments to provide hands on support within schools to ADF members and their families.
7.19 Trade Transfer and Retention The role of the Trade Transfer and Retention Officer is to assist individuals and Units by providing straight-forward advice on Retention issues including re-allocation, trade transfers and Corps transfers as part of the MECRB process, Service transfer, Transfer to reserves, Separation, bonuses and allowances. This service is also available to members who are not ill or injured.
93 http://www.rslservicesclubs.com.au/default.aspx?id=3 94 DI(G) PERS 11-1 Amdt 6 Defence Force Sponsored visit to service members suffering serious illness or injury – The Australian Dangerously Ill Scheme (AUSDIL)
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
8 Local/ Regional/ Service initiatives The following section provides information on local, regional and Service specific support initiatives. It is not, and is not intended to be, a comprehensive listing of all local/ regional support initiatives – rather a description of the initiatives discussed with stakeholders during the field trip phase of this review.
8.1 Casualty Management, Claims Assistance and Complex Case Management Duties of an employer in relation to their employees
The Chief of the Defence Force (CDF) has employer functions as outlined in the OHS Act 1991.
“An employer must take all reasonably practicable steps to protect the health and safety at work of the employer's employees”.95
Service Chiefs’ delegation
“A service chief may delegate in writing any of his or her functions or powers under the provision of this Act to:
(a) a person:
(i) who is engaged under the Public Service Act 1999 and performing duties in the Department administered by the Defence Minister of the Veteran’s Affairs Minister: and (ii) whose duties relate to matters to which the provision relates; or
(b) a member of the Defence Force whose duties relate to matters to which the provision relates.”96
Definition of Rehabilitation Authority
97
The function of the Rehabilitation Authority commences when an employee is injured.
“The rehabilitation authority for a person at a time is:
(a) the person’s service chief for a time when the person is:
95 OHS Act 1991 Section 16 96 MRCA 2004 Section 438 97 SRCA 1988 Section 146(1) Rehabilitation authority :”This Act applies to the employee in relation to a defence-related claim as if the rehabilitation authority in relation to the employee were the rehabilitation authority applicable under subsection 39(3) of the MRCA”
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
(i) is a Permanent Forces member or a continuous full-time Reservist; and (ii) has not been identified by or on behalf of the person’s service chief as being likely to be discharged from the Defence Force for medical reasons; or
(b) the Commission for any other time.98
“Likely to be discharged … for medical reasons” occurs when:
1 A MECRB determines that a member is to be terminated on medical grounds; and
2 All appeal avenues have been waivered or exhausted; and
3 The member’s discharge is to take effect within the next 120 days.
8.1.1 Comparison of Single Service frameworks Each Service has developed a framework for the administration and management of casualties, complex cases and compensation claims. Table 21 below contains a summary view of the similarities and differences between the three Services.
These tables (Table 21 and Table 22) serve to highlight the significant differences between the approaches and member support provided by the Services. The Air Force approach (Complex Claims Liaison Office – CCLO) has a compensation claim assistance focus, the Navy approach (Complex Case Management – CCM) concentrates on complex case management (noting the complexity of a case is a function of Command, medical/ clinical, administrative and “other” factors) and the Army approach (Casualty Administrative Support – Army - CAS-A) which includes compensation claims assistance for MRCA, Command support, member welfare responsibilities and complex case management.
CAS-A CCM CCLO GENERAL
Service Army Navy Air Force Name Casualty Administrative
Support – Army (CAS-A) Complex Case Management service (CCM)
Compensation Claims Liaison Office (CCLO)
Established Sept 2009 2010 May 201099
Applies to:
• Permanent Army – inc CFTS • Reservists on days • Recruits and Trainees • Officer Cadets
• Permanent Navy • Naval Reserve Members • Members of foreign services on exchange
• Permanent Air Force – inc CFTS
• Reservists on duty • ex-members involved
with deseal/reseal100
98 MRCA 2004 Section 39(3)
99 Office first established in 2000 to assist those affected by deseal/reseal, and has evolved through several iterations since then. 100 Recruits, Trainees and Officer Cadets are all part of either the PAF or reservists on duty so not mentioned separately
100
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
CAS-A CCM CCLO Excludes Army Cadets Australian Naval Cadet
(ANC)101
Description of role/ service
Provide support to seriously ill or injured Army members including those who have complex medical management needs requiring extended rehabilitation (2 year separation quarantine period) and/or extended transition (3 year separation quarantine period). All members are afforded appropriate opportunities to complete clinical and rehabilitation treatment plans. Additionally, when decisions are made to medically discharge Army members, that (1) retiring medical conditions have been given an opportunity for DVA determination. (2) Army Extended rehabilitation and transition programs are completed (3) clinical and rehabilitation plans have been transferred to DVA if conditions are determined compensable. (JHS action under MRCA r.272 required); requiring ‘Discharge ready’ certification being issued to the relevant discharge authority in Army, before agreed separation date.
Assist Navy members whose cases are considered complex, to access the services and systems available to support their case. It also assists Command, Supervisors and other involved agencies by coordinating access to available support services. To improve transition and separation outcomes for Navy personnel who have been injured during the course of their service.
Assist Air Force personnel with the preparation of military compensation claims and their submission to DVA. Assist members with on-going military compensation claims issues, who are being discharged from the Air Force, to locate suitable ESO of other civilian advocates for assistance. Provide advice and assistance to members involved in deseal/reseal in terms of tier placement and subsequent claims for compensation. Liaise with other Defence, Government and external agencies as required in relation to the preparation and progression of military compensation claims for serving Air Force personnel. Provide advice to Air Force Commanders, Manager and Supervisors on military compensation issues relating to serving Air Force personnel.
Entry point Complex medical case. Severely ill or injured
Complex case. All MEC4 cases
Any member requiring assistance with submission of a claim to DVA
Point of contact/ gatekeeper
Unit Welfare Officer (UWO)/Unit Rehabilitation Liaison Officer (URLO)
Regional Complex Case Officer (CCO)
Member can self refer to CCLO.
Training Induction program – delivered by CAS-A
Induction program being developed. National meeting of all COOs - quarterly
Customised TIP training including: • Induction • MRCA e-learning • Welfare
101 ANC members are not eligible for rehabilitation services within the ADFRP. Rehabilitation for ANC is managed by the Military Rehabilitation and Compensation Commission (MRCC)
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
RCASO: CAS-A Canberra $1.060m for FY 2010/11 – daily full cost by rank for period.
Information stored in:
Army Case Management Database (Excel) on DRMS
Case Management Database (Excel)
MCLO Client Database (Access)
STRUCTURE and LOCATIONS Reports to: DGPERS-A
through Director Army Health (DAH)
Director Navy Health (DNH) – through Manager Navy Complex Case Support
DGPERS-AF through COS DGPERS-AF
Responsible for casualty management
Unit Commanders Divisional Officers Commanders
Referral • NOTICAS/MEDICAS • Complex Case Referral • MECRB via e-mail.
102 Including: DI(G)PERS 16-15 Australian Defence Force Medical Employment Classification System and DI(G)PERS 11-2 Notification of Australian Defence Force and Non-Australian Defence Force Casualties 103 Not all cases are mutually exclusive and the status of the cases vary from day to day as a member moves from Seriously ill (requiring High dependency or acute care) back to Satisfactory (the condition is stable). The 27 (Extended management cases) are managed from a different statistic group - Complex Medical Management (currently the figure today is 29). The second statistic group that I work with is 2010 NOTICAS/MEDICAS cases only and these change daily 104 Resourced from Defence White Paper allocation of $1.1.4m – which is split equally between the Services
102
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
8.1.2 Overview of services provided Table 22 below provides a breakdown of the specific support and services provided by each Service.
CAS-A CCM CCLO SUPPORT and INFORMATION
Support and advice during medical procedures, rehabilitation, re-deployment, transition • Member • Member’s family • CO and delegate
Y Y Y
Y Y Y
For people being
medically separated
where requested
Primary liaison between command and agencies responsible for services including: • JHC • DCO • DSG • Transition Services • DVA • ComSuper • Centrelink
Y Y Y Y Y Y Y
CCO provides a
coordination service
For complex case
management when
requested
Ensure members are aware of and able to access all appropriate available services – including: • Provision of mentorship • Information on rehabilitation services • Information on health programs • Information on psychological programs • Information on social support programs • CA Wounded Soldier forum - website • ADF Paralympics activities
Y Y Y Y Y Y Y
Y Y Y Y Y
Upon cessation of TMS – will
provide these types of services
REHABILITATION and CASE MANAGEMENT Facilitate members access to adequate and timely rehabilitation services
Y Y
Collection, collation and analysis of case management workload, outcomes and key result areas
Y Y
(UWO)Develop Individual Welfare Plan (IWP) – if required
Y Assists
Participate in Welfare Boards Y Y Rehabilitation Plan development Y Coordinates Assign appropriate workplace duties to member Y Vocational rehabilitation in readiness for re-employment Y Seek early UMECR and consider requirement for extended Rehabilitation
Y
Prepare MEC 4 casualties for vocational re-employment and future transition
Y
Cessation of case management when additional assistance is no longer required
Y Y
APPOINTMENT OF MRCA S64 TRANSITION CASE MANAGER
104
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
CAS-A CCM CCLO Delegation of Service Chief requirement to appoint a S64 Transition Case Manager for members who are medically separating
CA delegation to DGPS
DSG
CCO
COMPENSATION CLAIMS Guidance and Support – MRCA claims Y # Y Guidance and Support – SRCA claims # # Y Guidance and Support – VEA claims # # Y Provide information to DVA to facilitate a decision by DVA
Y Y Y
Advocacy SERVICES, AIDS and APPLIANCES
Housing and accommodation requests – liaison with local DHA staff processing applications
Y
Identify transportation needs of casualty and extended family
Y Assists
Identify continuing casualty carer support requirements Y Assists Table 22 Services provided through Service casualty management frameworks
# in conjunction with ESOs
8.1.3 Casualty Administrative Support – Army (CAS-A) “Commanders are to be personally involved in ensuring the needs of our injured or ill members and their families are being met. I want you to lean forward. I want you to involve families in your Welfare Boards and I want you to challenge supporting agencies, and me if necessary, for more effective solutions .I want you to do this because this is the essence of command: delivering what our people deserve”106
The key tenants of DI(A)PERS 33-11 are:
• Commanders are responsible for the health and welfare of members under their command;
• Rehabilitation of members is an essential component of a unit commander’s personal management responsibility;
• ADFRP Rehabilitation Plan with Command Involvement for each case where extended rehabilitation applies; and
• Every member returned to the workplace after an injury or illness contributes to ongoing capability.
The policy and provisions are applicable regardless of the duty status (on/ off duty) of the member at the time of the injury or onset of illness
106 Chief of Army, 17 February 2010
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Structure – CAS-A
DAHCOL
CAS-A
NT/SA Nth Qld Sth Qld/Vic/Tas NSW/ACT WA
DGPERS-ABRIG
C3
Figure 20 CAS-O Organisation structure
Army Casualty Assisting Officers (ACAO) The responsibility of the ACAO personnel is to provide a full-time CAS-A presence in major troop concentration areas to provide casualty administration and assistance to unit commanders when a unit has a seriously injured or ill member requiring management. Additionally the ACAO staff will provide task allocation and control of the RCASO allocated to the region. In this regard, the ACAO is to administer and provide technical control and manage the Army Reserve training salaries for allocated RCASO personnel in the regions allocated. Tasks supporting the ACAO responsibilities include:
• assist with the identification of casualty support needs;
• identify the continuing need for casualty carer support requirements;
• consider housing or accommodation assessment requests, involving liaison with local DHA staff processing applications for a married quarter allocation to allow for modifications necessary for independent living arrangements;
• identify transportation needs of the casualty and extended family, if considered necessary by CAS-A;
• provide the avenue for information regarding the conduct of the CA Wounded Soldier forums, and ADF Paralympic Sport activities;
• individual support to the casualty to assist in the completion of superannuation invalidity, and disability support benefits applications during the transition phase of administration;
106
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• support and guidance to a unit CO managing a seriously injured or ill member, in the following areas:
• provide guidance and advice to the IWB ensuring casualty management actions provided from support agencies are addressed at the board;
• within the complex medical management provisions, provide guidance to the staff procedure required for DAH and CMA consideration of:
• extended rehabilitation, normally for a maximum period of 24 months;
• individual rehabilitation plan development;
• extended transition, normally for not more than 36 months associated with vocational training and skills development in readiness for re-employment.
• provide guidance and advice of potential gaps in support available from internal agencies such as DCO, DSG and external organisations such as DVA, ComSuper and Centrelink relevant to meeting the casualty needs;
• Provide a link between unit CO and enabling agencies such as ADFRP, ADF Transition Centres (ADFTC), DVA, ComSuper and Centrelink;
• Provide advice to the unit CO when established procedures or available resources are not meeting the member’s needs;
• advice to unit commanders when established procedures or available resources are not meeting the member’s needs; and.
• their presenting medical condition, if it is related to military service.
Requests to engage ACAO support in conducted by the Unit CO to the CAS-A.
Regional Casualty Administration Support Officers (RCASO)
RCASO is an initial support resource available to provide assistance directly to the severely injured or ill soldier, particularly with the preparation and DVA lodgement of a MRCA claim covering their presenting medical condition, if it is related to military service.
RCASOs assist serious injured or ill members and their families with their immediate concerns. They are an Army Headquarters resource and are located in every Australian capital city. These Reserve members are the conduit between the injured member, the unit welfare officer the CO and all the Agencies that provide support to the member and the member’s family.
Requests to engage RCASO support in conducted by the Unit CO to the CAS-A.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Army Complex Medical Management/ Extended Rehabilitation
Army complex medical management is designed to streamline administrative processes and provide a greater level of assurance for severely injured personnel. This allows the injured member to focus on their clinical treatment and rehabilitation plan (recovery and wellbeing) before more formally considering whether to remain or separate from the Army.
Army Complex Medical Management is divided into:
1 Phase 1: Army Extended Rehabilitation – a 24 month focuses on medical management for members with a MEC302 grade and approved at MECRB for extended Rehabilitation (MEC302). Clinical oversight and management of casualty expectation is maintained by CAS-A. A CAS-A process review occurs around the 18-month mark to ensure actions are in place to return the casualty to the Army workplace or prepare for consideration of Phase 2.
2 Phase 2: Extended Transition – (vocational employment phase) prepares severely injured members for the transition from Army process with a focus on civilian employment or lifestyle change (members with a MEC 401 grade annotated for Extended Transition). Limited retention of the severely injured member is available for up to 36 months, to allow reasonable opportunity to gain the applicable/ required skills for civilian employment.
Welfare Boards
The Welfare Board process provides for effective management of members with significant health and/or welfare issues. It enables the CO and command group to consider all relevant information regarding a member’s care (including welfare needs). They are used to assist decision making and monitoring of members throughout the recovery process.
A member, and if requested next of kin/ family, should be provided the opportunity to participate in the welfare board.
There are four types of welfare boards:
• Individual Welfare Board (IWB): Managed through the CAS-A. All severely ill/injured casualties and all battle casualties AME to Australia will automatically be discussed through an IWB chaired by the Unit CO. Members with complex health conditions, high in profile and require intensive case management can also be managed through an IWB.
• Unit Welfare Board (UWB): Managed by Unit Commanders. Provides an important information flow to a unit commander that allows them to make informed decisions about a member’s health and welfare. A UWB is to consider members who are MEC 3 or MEC 4.
• Formation Welfare Board (FWB): Managed by Formation HQ. A FWB is coordinated and administered by staff under command of the Senior Medical Officer of the respective formation headquarters.
108
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Area Welfare Board (AWB): Managed by the Senior Army Representative. Non-Army group personnel and units will be managed at an AWB. The frequency and nature of participation should be specified in the local Regional Level Agreement for health services.
8.1.4 RAN Complex Case Management arrangements (CCM) Divisional officers and existing command structures retain primary responsibility for the member. Health staff retains health care responsibilities. The Complex Case Officer (CCO) role, where there are identified difficulties or complexities, is to facilitate at the earliest opportunity, access to those services needed and ensure appropriate support is being provided to the member and command.
CCOS have direct liaison authority to COs, Fleet Command, JHC, DCO and DVA when needed in the management or co-ordination of a complex case.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Where an individual is absent from the workplace for an extended period of time or where they have been evacuated from their deployed unit;
• Other cases where it is considered necessary to provide additional support to ensure appropriate access to services available; and
• Where there has been an assessment by the complex case manager who has determined that it is a complex case requiring assistance to facilitate resolution.
Referral process
A written referral is the preferred method (utilising a Navy “Complex Case Referral” form) for referring a member to a CCO. An initial phone call to a CCO, followed by a completed referral form within 3 days is also acceptable.
A referral to a CCO can be initiated by (but not limited to):
• Anyone involved in the healthcare or welfare of the member including medical, psychology, chaplains, rehabilitation staff or other agencies involved in provision of care or support;
• Command, Divisional staff, PERSO etc;
• Career Management personnel; and
• Self-referral by a member, family or concerned acquaintance.
Participation requires the informed consent of the member.107
Case closure
If a member withholds consent this will limit the communication between agencies and may impact on the support that can be provided to the member. If the member continues to withhold consent, it is recommended the CCO discusses options for support with DNH.
Case closure is at the discretion of the CCO – being guided by the following criteria:
• Discharge from hospital – unless significant rehabilitation is still required.
• Where no further specialist medical care is required.
• Return to work – graduated return to work program completed or nearing completion.
• Separation from the RAN has been affected.
107 Privacy Act 1988 and DI(G)PERS 16-20 Privacy of Health Information in Defence
110
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• The member is able to access all appropriate services/agencies/networks without CCO support.
• At the request of or consent of the member.
Upon closure a staff-in-confidence summary report from the CCO is prepared and placed on the member’s personnel file. If health resources have been involved in the case, a second copy of the summary report is placed on the member’s medical record.
8.2 Army Personnel Coordination Detachments Army is establishing 12 Army Personnel Coordination Detachments (APCD) co-located, where possible, with ADF Transition Centres. The APCD will provide a visible, uniformed command and management presence enabling Army to effectively command, administer and support Army personnel undertaking transition.
APCD staff will assist in the preparation and coordination of Army personnel seeking to transition. They do not assume or override any DTSS transition responsibilities, but will greatly enhance the coordination and management of personnel and their administration. Additionally the APCD will undertake the ACO role of command and management of select APNRE positions and as or when required provide a formal Army Chain of Command for select personnel in the Non-Army Group (NAG).
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
There will be one APCD in each Australian capital city and four others in regional areas of major military personnel concentration or identified need. The first six APCDs have been stood up in:
• ACT – Brindabella Business Park;
• Nthn NSW – RAAF Williamtown;
• Sthn NSW – Kapooka;
• SA – Edinburgh;
• VIC – Defence Plaza Melbourne; and
• WA – Leeuwin Barracks.
The remaining six APCD will be stood up in March 2011 in the following locations:
• NT - Berrimah Defence Establishment;
• Nthn QLD - Lavarack Barracks;
• Sthn QLD - Gallipoli Barracks;
• Sydney Central NSW - Defence Plaza-Sydney;
• NSW- Steele Barracks; and
• TAS - Anglesea Barracks.108
When the second six APCDs are stood up the coverage across Australia is represented in
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Figure 23 Army Personnel Coordination Detachment locations – March 2011
8.3 Project AKESA Chief of Army initiated Project AKESA to identify the primary mental health issues of both permanent and part-time Army members. The project is focussed on finding the weaknesses or deficiencies in the current personnel support mechanisms for serving and former troops and making recommendations on how the safety net for these individuals can be strengthened to better cater for their needs.
Focus of the study is on the mental health and wellbeing of Army members and it did not address in detail the mental health issues of spouses or families.
8.4 Wounded Diggers Forum On 29 Mar 2010 the CA convened the first Wounded Diggers Forum to gain feedback from affected Army members and their families on issues surrounding their care.
“It isn’t good enough for us to simply say that we owe you a debt of gratitude for the things that happened to you because of the things we asked you to do. I don’t think there’s a higher priority for any government of any political colour at the moment than to see you get the rehab and care you need”109
109 Defence Minister John Faulkner as reported in Army April 15 2010 – page 3
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
8.4.1 Gaps identified
• Absence of policy in some areas – “We are putting our troops in 21st century harm and I think it’s time our policies caught up with that”110
• Difference in entitlements/ benefits available to injured serving members who choose/ elect to remain in Defence (possibly in a different role/ function post injury) rather than accept medical separation – i.e. the member and their family would be better off financially if the member accepted medical separation as a result of their injuries – “We will take than on board and sort it out”
111
• Participants generally not aware of the existence of Unit Welfare Boards as well as lack of family and member involvement
• Follow up psychological support not occurring. Suggestion from participants that Defence is waiting for people to contact them to request help rather than initiating contact with the member to see if they require assistance and support.
8.5 Transition case manager – Section 64 MRCA Section 64 of the MRCA 2004 requires any member who has been identified as being likely to be separated from the Defence Force for medical reasons to be appointed a case manager by their Service Chief.
“The person’s service chief must appoint a case manager for the person”112
“The role of the case manager is to assist the person in the transition to civilian life, including by advising the person about entitlements and services for which the person may be eligible as a member or former member, and about how to obtain access to such entitlements and services”
113
It was recently identified that this appointment was not formally occurring. The Service response to this requirement follows:
• Army: The appointment of a case manager has been formally delegated by CA to the Director General People Services, Defence Support Group (DGPS DSG) as per 17 August 2009 CA Instruction titled “Delegation of Powers and Functions under the Military, Rehabilitation and Compensation Act 2004”.
• Navy: All cases that have MECRB outcomes of MEC 4 or greater will have their regional CCO appointed as a case manager by the chair of the Navy MECRB in accordance with section 64 of MRCA 2004. The CCO will assist the person in the transition to civilian life
110 CA Lt-Gen Gillespie as reported in Army April 15 2010 – page 3 111 DHPERS-A Brig Gerard Fogarty as reported in Army April 15 2010 – page 3 112 MRCA Part 5 – Transition Management, 64 (2) 113 MRCA Part 5 – Transition Management, 64 (3)
114
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
including advising the person about entitlements and services for which the person may be eligible as a member or former member and how to obtain access to such requirements.
• Air Force: response pending.
Why relevant?
• Legislative obligation of Rehabilitation Authority.
• Another person assigned the title of ‘case manager’ may add to the confusion of the member.
8.6 Project Warrior Welfare – SOCAUST In response to increasing casualty numbers and operational tempo a proposal seeking approval to establish two Personnel Exceeding Establishment Guidance (PEEG) positions was submitted on 1 Sep 2010. These positions were to create a sustainable welfare and rehabilitation construct within SOCOMD eastern Region – Project Warrior Welfare (PWW)
The PWW is intended to provide COs with a regional Welfare Officer (ARA) to manage all administrative and co-ordination functions relating to the seriously ill or injured on behalf of the Unit CO and UWO. They will act as a conduit between unit and external welfare agencies as well as fulfilling reporting and monitoring responsibilities to COs and JO7
The proposal aligns with the RCASO framework and acknowledges the increasing demands of the welfare and rehabilitation framework which have been amplified in SOCOMD due to casualty numbers.
Why relevant?
• Acknowledges responsibility to provide appropriate levels of support to all injured or ill members and the demands this places on the units.
• Recognises Unit obligations to establish processes and systems that facilitate open and early engagement between Cos, CMA and DAH and manage the interactions with external stakeholders providing support to members and their families.
• Ensures members are managed in an appropriate and timely manner to maximise recovery and facilitate positive outcomes for the member and Army.
• Develop case management and rehabilitation management capability.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
8.7 Case conferences – Lavarack Barracks Medically separating members and their families are invited to attend personal case conferences to bring together representatives from ADF Transition Services, DVA (TMS) and the ADFRP to enable member questions to be discussed and addressed.
These meetings are facilitated by the ADFRP Rehabilitation Coordinator and are generally well received by the member. Attendance is voluntary and a member can request/ attend as many case meetings as necessary to resolve their questions and concerns.
41 members utilised a case conference(s) during FY 09/10. This FY (10/11), 27 members have utilised the case conference, which is an increase from 13 (for the same time period last year). Case conferences are now held on a fortnightly basis (previously monthly) due to the increasing volume of members wishing to utilise this service.
This initiative will be rolled out across DCO over the coming 12 months.
8.8 Deployment Support Booklet Many of the DCO offices produce location specific deployment support booklets.
The booklet is designed to assist members in preparing for deployment by providing information on issues to consider before deployment, tips for families when members are deployed and useful contacts/ phone directory including information on Emergency Support to Families Scheme (ESFS) and the DCO and their services. “Whether a member is deploying as part of a larger contingent from his/her parent Unit, or detached from another unit, this booklet will provide useful information for how to successfully manage deployment”114
8.9 Re-integration Booklet
DCO Townsville produces a reintegration booklet. The aim of the booklet is to provide all uniformed members and their families with a range of easily accessible information that will assist with reintegrating into family and working life following deployment and time away from home base.
The booklet includes information on stress, trauma and Defence support services available to members and their families.
8.10 Family Care Plan (FCP) DCO Townsville produces a FCP booklet. A FCP is a working plan for the care of loved ones and personal property during periods of absence. It is designed to provide vital information about personal arrangements applicable to member’s families. It provides a basis for a
114 Page 3 Deployment Booklet DCO Townsville
116
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
preparation checklist to identify areas that need to be considered. A FCP plan should consider the following information which may be relevant in the result of member illness of injury:
• General information including personal, medical and unit details;
• Plan of action for emergencies;
• Legal authorisations and legal information (Power of Attorney, Will etc); and
• Contact details for support agencies, local community numbers and 24 hour support lines.
This initiative will be rolled out across DCO over the coming 12 months.
8.11 Generating AC563 - Army Army is progressing the ability to generate an AC563 from within AIMS (Army Incident Management System).
8.12 How are you travelling? Project The "How Are You Travelling?" project is an initiative in the Barwon South Western Region of Victoria to encourage veterans and former serving members who have concerns about their
mental health and wellbeing to get help.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
9 Projects and initiatives which affect or impact on SIIP
9.1 Current projects and sub-projects with SIIP impacts There are many initiatives which have the capacity to influence and enhance the support provided to injured or ill members. These are described in more detail in this section of the review and summarised in Table 23 Initiatives which influence and enhance support provided to injured or ill members below. The ‘current systems’ as described in the process maps has been utilised to show which areas these initiatives may impact.
OH
S
Inci
dent
Pre
sent
atio
n
Prim
ary
Hea
lthca
re
Reh
abili
tatio
n
Lia
bilit
y/ C
ompe
nsat
ion
Ret
urn
to A
DF
Dut
y
Sepa
ratio
n
Med
ical
Sep
arat
ion
Supe
rann
uatio
n
Post
Sep
arat
ion
Com
man
d/ W
elfa
re
Garrison Health Transition Y Y Y Y Y Y
JeHDI Y Y Y Y Y Y Y Y
Modification - MEC Y Y Y Y Y
JP 2080 Phase 2B
TMS Contract expiry Y
Simpson Assistance Package Y Y Y Y Y
OHS Strategic and OHSMIS Y
ADFRP – Conversion to APS Y
MRCA Review Y Y Y Y Y Y Y
Transition Case Manager Y
OMHCP Y Y Y
Military Health Outcomes
Single Access Mechanism Y
118
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Represented in a timeline over the coming 16 months, with key milestones for individual projects and initiatives:
Dec 10 Mar 12Feb 12Jan 12Dec 11Nov 11Oct 11Sep 11Aug 11Jul 11Jun 11May 11Apr 11Mar 11Feb 11Jan 11
Transition Management Services (TMS) Contract
ADFRP – PCM to APS Roles
Simpson Assistance Package
Medical Employment Classification (MEC) changes
Interdepartmental Working Group Initiatives – Various (ongoing)
Joint eHealth Data and Information System (JeHDI)
Defence Occupational Medicine and Occupational Hygiene Capability
Garrison Health Transition Project
MRCA Review - Ongoing
Military Health Outcomes Program (MilHOP)
JP 2080 Phase 2B1 – HR Shared Service Transition Project
Single Access Mechanism – clear backlog
Occupational Health and Safety Strategy 2007-2012
Figure 24 Representation of key projects (and milestones) having the capacity to influence support for injured or ill members
9.1.1 Garrison Health Transition Project
Defence is transforming and revolutionising the way health services are delivered. It has been identified in numerous reviews that our current health service delivery model is fragmented and dislocated. To remedy this, the decision was made to formally transfer responsibility for Garrison Health Services from the three Services to JHC.
It provides Defence with the opportunity to develop and implement health services, systems and governance procedures in a consistent, standardised and coordinated manner across the ADF. This is a radical transformation and requires a great deal of change to implement successfully and holistically.
The transformation of Defence Garrison Health Service should not be seen as an isolated or independent activity that is encompassed by the 'handover' of single Service facilities, staff and services to JHC. While it is certainly an important and defining step in the future of garrison health, it must be seen as simply a 'first step' in the evolution of Defence health. The Garrison Health Transition Project incorporates parallel objectives comprising the initial handover of materiel, personnel, facilities from the single Services and the longer term and
120
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
ongoing projects which will form the basis for JHC operations. In order to effectively transition to the new Garrison Health Service the following JHC related activities require implementation within a synchronised and risk managed process:
• The transition of nine AHSs to five RHS;
• RHS QLD
• RHS Northern NSW
• RHS Southern NSW
• RHS Victoria & Tasmania
• RHS Central & West
• Recruiting, appointment and induction of 5 Regional Health Directors (RHD);
• Development of an Induction Package for RHDs;
• Development of a series of directives to define the scope of responsibilities of RHD;
• Implementation of supporting instruments issued pursuant to Regulation 4 of the Defence Force Regulations 1952 (Cth) (DFR4);
• Development and issue of a Communications Plan;
• A Facilities Review and a Facilities Master plan needs to be finalised;
• A comprehensive maintenance program and other base support services must be agreed as part of the Defence Support Group (DSG) Base Accountabilities Model (BAM) Project;
• A JHC Establishment Review and development of a Single Entitlement Document;
• Future Workforce Modeling Project;
• Transfer of uniformed workforce as appropriate;
• Establishment of working groups in order to determine the more specific details around issues such as training, specialist support and emergency response.
• Finalisation and implementation of the Clinical Governance and Performance Indicator Framework;
• Establishment of strategic alliances;
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Implementation of the findings of the Dunt Review;
• Integration of Regional Mental Health Teams;
• Implementation and integration of the new rehabilitation workforce model;
• Health Services improvement initiatives, such as review of imaging and pathology services and workforce, contracting arrangement;
• Medical Employment Category project;
• Review of Garrison Health Operations Branch roles, function and structures; and
• Implementation of the Joint Electronic Health Data Information (JeHDI) system.
9.1.1.1 Garrison Health Model
COSC 50/08 recommendation 6 was that unit-level health support will be centralised within hub facilities for the provision of garrison health support. The Regional Reviews have identified a number of smaller health facilities (such as Regimental Aid Posts - RAP - on large Army bases) for closure in the short to medium term. The intent is for all health delivery points to be progressively "hubbed" to establish a single health precinct at all Defence sites in the longer term. Hubbing will be achieved via a staged approach using the Regional Reviews to prioritise rebuilds and maintenance based on:
• Quality of existing infrastructure (fit for purpose);
• Capacity of major health facilities to accept increased workload;
• Funding availability; and
• The strategic direction of Bases.
The GHM at the base level will be organised within a health precinct operating within a RHS under a clear chain of command and management. It is anticipated with future programming of JHC facilities into the Major Capital Funding (MCF) Program, a single health precinct on each base can be established at key Defence Force establishments by 2020. Under the above model, garrison health arrangements will be based on the following principles:
122
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Primary health consolidated and delivered via a multidisciplinary model in JHC facilities (including dental services, central dispensing points, mental health and psychology and rehabilitation);
Regionally organised inpatient holding within appropriate JHC facilities or ADF wards within civilian facilities under strategic alliance arrangements;
Regionally coordinated specialist outpatient services provided from within JHC facilities where sessional payment and service delivery arrangements are advantageous to Defence;
Some regional specialist health capabilities will be retained within JHC facilities (where appropriate for training and efficiency reasons); and
The remainder of specialist, allied health and tertiary level health services outsourced via a global model of fee-for-service contracts with civilian agencies/providers
As a guiding principle, wherever possible, smaller, low capacity and inefficient health delivery points (facilities) will be closed, with workforce and other health assets consolidated into larger, central health facilities. This initiative will:
• achieve infrastructure and materiel efficiencies in accordance with the Strategic Reform Program (SRP);
• achieve health delivery quality improvements in line with national benchmarks;
• enable coordinated workforce utilisation and technical oversight to maintain high standards of health delivery;
• promote civilian and Service opportunities for professional support, mentoring, multidisciplinary care team practice and skills exchange;
• provide support to the single Services to maintain and develop operational health capability;
• provide an enterprise related response to the international and national shortage of health professionals;
• enable realisation of market-weight for national fee-for-service and prime contracting;
• improve clinical and corporate governance for accreditation, safety and other quality objectives; and
• improve training opportunities for ADF health personnel to enhance operational capability.
Any requirement for JHC to operate in-patient holding capabilities will be determined on a location by location basis. This may range from hostel type / low acuity accommodation (for self-caring patients not requiring full hospital clinical support), through to some retained capacity to care for higher acuity patients where agreed clinical requirements exist. Such
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
requirements will be agreed between JHC, the single Services and DSG (the latter for facilities implications), taking into account effectiveness, efficiency, and clinical safety requirements.
Key dates/milestones
• Dec 2010 – Four Regional Health Directors appointed as APS employees.
• Feb 2011 –Townsville transition.
• Mar 2011 - Victoria & Tasmania transition.
• Mar – Jun 2011 –Southern QLD transition.
• Apr 2011 – Southern NSW transition.
• May 2011 –Northern NSW transition.
• July 2011 – Central & West transition.
9.1.2 JeDHI: Joint eHealth Data Information System
The objective of the JeHDI project is to develop and implement an ADF electronic health information system that will rationalise and consolidate the information currently gathered through existing systems to enable better health service provision, effectiveness and efficiency. It includes linking member health data from recruitment to separation and subsequent management in other agencies and will:
• Provide an electronic health record (EHR) for ADF personnel;
• Improve the productivity of health care personnel/ contractors;
• Provide the ability to map health related trends and patterns from ADF health data;
• Provide the ability to derive financial reports related to the provision of health care to ADF personnel; and
• Maintain the security of member health data.
The five categories of business functionality addressed by JeHDI are:
124
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Key dates/milestones
• Oct 2008 – Jul 2009 Rapid Prototype Development and Evaluation (RPDE)
• Jun 2010 – Prototype system operating
• Jun 2011 – Pilot system operating
• Dec 2011 – Partner system operating
• Dec 2013 – Project concludes – Business as usual
Why relevant?
• Technology solution to address communication, manual workflow, system functionality/ capability/ support issues identified during this review.
• Ability to define business rules/ user requirements from SIIP perspective and incorporate requirements into the JeHDI development.
• JeHDI may result in the rationalisation of documents/ forms and related changes to processes, Health Directives, Defence Instructions (DI) and process documentation. These will need to be updated to reflect this new operating model.
• Complements the SRP – allowing identification and remediation of inefficiencies.
• Present lack of electronic clinical informatics restricts Commanders from readily ascertaining the health status, and therefore the deployability status of their members.
9.1.3 Modification – Medical Employment Classification system MEC policy is being reviewed to provide greater flexibility for employment of members with permanent injuries.
“The intent of the agreed changes is to refocus the MEC system from deployability to one of deployability, employability and rehabilitation. In essence, the changes increase employment flexibility by placing greater emphasis on the functional ability of personnel to perform tasks in specific operating environments.”116
The new draft classifications are:
• MEC 1 – Fully Employable and Deployable;
• MEC 2 – Employable and Deployable with Restrictions; 116 CA Directive 09/10 Management of Medical Discharges in Army – section 1
126
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• MEC 3 – Rehabilitation;
• MEC 4 – Employment Transition; and
• MEC 5 – Medically Unfit for Further Service.
More detail on the MEC classification including a description and coding is included in Appendix J.
Key Milestones/ dates
• Rollout is expected by Jun 2011
Why relevant?
• Change in relevant Health Directives, Defence Instructions and legislation to reflect changes to MEC classifications including:
o DI(G)PERS 16-15 – Australian Defence Force Medical Employment Classification System
o Health Directive (HD) 236—Medical Employment Classification procedures.
• Will the new classification and education of MOs and MECRB users of the new classification system increase the MECRB workload and increase the time taken for MECRB determinations?
9.1.4 JP 2080 Phase 2B1: HR Shared Services Transformation Project JP2080 is in the planning stage. First pass “lite” includes describing the high-level objectives, rationale and approach for JP2080 and obtaining DCP funding to develop an Interim 2nd Pass business case. Interim 2nd pass includes obtaining endorsement for project scope and implementation options and obtaining funding and approval for key activities to achieve 2nd pass business case approval. The 2nd pass phase involves obtaining endorsement for implementation of the preferred solution and obtaining funding for project implementation.
Key dates/ milestones
• Nov 2010 – First pass “lite”
• Jul 2011 – Interim 2nd pass submission
• Sep 2011 - 2nd pass approval
• 2014 - Implementation
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Why relevant?
• Requirements including interfaces and potential changes to PMKeyS need to be indentified and included in the project scope – fed into the high-level business requirements and solution design.
9.1.5 Expiry of TMS Service Level Agreement (SLA) Defence commenced reviewing the TMS SLA in 2008 and has identified that many of functions provided through TMS are now provided through the ADFRP, ADF Transition Services and/or the Services Claims and Complex Case Management programs. The review also identified that TMS had evolved into an enhanced DVA specific function, such as claims processing arrangements at two Defence bases and scheduled visits to other major Defence bases. TMS staff were also evaluating client outcomes, responding to ministerial correspondence, handling client complaints, promotion and marketing of TMS and maintaining the TMS website.
In early 2010, discussion at the Defence/ DVA Links Steering Committee focused on the support provided to injured or ill ADF members. This resulted in the commencement of SIIP and Defence and DVA agreeing to extend the TMS SLA until 30 June 2011 pending the outcome of SIIP.
Key dates/ milestones
• Contract expires 30 Jun 2011
9.1.6 Simpson Assistance Package (SAP) This recent government initiative provides support and benefits for severely wounded or severely incapacitated members and their families. It focuses on improved coordination and integration of existing services and development of specialist programs to ensure a comprehensive approach to tailored recovery programs supporting the needs of individual wounded personnel and their families.
Key dates/ milestones
• Feb 2011 - Scoping of this package of projects is to commence.
• Research visits to US and UK military advanced trauma and rehabilitation centres of excellence has occurred.
• The concept for an ADF advanced trauma and rehabilitation centre has been developed.
Why relevant?
It is expected that SAP will be developed in conjunction with the outcomes of this review to establish an integrated and joint Service capacity building program bringing together the
128
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
RCASO, CCM, rehabilitation, health and welfare service providers across Defence to deliver better monitoring and coordination of tailored and integrated services.
9.1.7 Defence OHS Strategy and OHSMIS The Defence OHS Strategy defines the strategic objectives that are required to achieve Defence’s desired OHS culture and deliver a high standard of OHS performance – reshaping Defence OHS management and realising performance improvements. The foundation of this work is developing and implementing the elements of the Defence OHS Management System (OHSMS), a critical element of which is the OHS Management Information System (OHSMIS).
OHSMS provides a planned, documented and quantifiable approach for the comprehensive and systematic management of OHS. It encompasses leadership, incident prevention, incident management and management arrangements.117
It moves beyond a focus on legislative compliance and evolves into a values based learning organisation where workplace hazards are proactively managed. It expresses a shift in thinking in issues of mental health from a model of compensation to rehabilitation. Two of the plan’s priorities highlight this: reducing the impact of occupational injury, illness and disease and improving the capability of leaders and staff to identify and manage hazards effectively.
The 8 original priorities from the Defence OHS Strategic Plan 2004-06 have been recast and prioritised as strategic objectives - focussing on foundation, outcome and enabling objectives. Those objectives which are particularly relevant to the SIIP review include:
• Outcome objective 3 – Reduce the frequency and severity of risks to people’s health and safety;
• Outcome objective 4 – Improve prevention of occupational injury, illness and disease; and
• Outcome objective 5 – Reduce the impact of occupational injury, illness and disease.
Key dates/ milestones
• Defence OHS Strategy 2007-2010
9.1.8 Conversion of PCM roles to APS positions The purpose of this initiative is to transform the ADFRP workforce to an internal (APS) workforce that is a ComCare registered Workplace Rehabilitation Provider. This is a sub project within the Garrison Health Transition Project.
Key dates/ milestones
• Recruitment of Regional Rehabilitation Managers (EL1) - Mar to Jun 2011 117 Message from the DOHSC Chairman – Defence Occupational Health and Safety Strategy 2007-2012
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Recruitment of Rehabilitation Consultants (APS6) - Apr to Jun 2011
Work in progress includes:
• A Rehabilitation Consultant procedures manual, ADFRP information management system and enhanced web forms/ paperwork;
• An ADFRP governance and quality management manual; and
• Blended-learning training modules for the new (APS) staff.
Why relevant?
An internal workforce is expected to provide numerous benefits to Defence including:
• A multidisciplinary team approach which should improved communication with Commanders and improve the quality of outcomes for members;
• Greater value for money and realisation of savings in accordance with SRP objectives; and
• Reduced complaints from members, Command and MOs through an improved and seamless service.
9.1.9 Review of Current Military Rehabilitation and Compensation Arrangements (MRCA)
The Review is examining the adequacy and suitability of military rehabilitation and compensation arrangements including perceived disparities and inequities between legislative schemes. The review includes visits to Defence Force facilities and consultations with current and former members of the Australian Defence Force, ex-service organisations, key agencies and other stakeholders including The Prime Ministerial Advisory Council on Ex-service matters and the Ex-Service Roundtable.
The Review’s Steering Committee is chaired by Ian Campbell, Chair of the Military Rehabilitation and Compensation Commission. Its members are: Major General Craig Orme, Department of Defence; Ms Peta Furnell, The Treasury; Ms Joan Ross, Department of Finance and Deregulation; Ms Michelle Baxter, Department of Education, Employment and Workplace Relations; and Peter Sutherland, an independent expert in military rehabilitation and compensation law and a Visiting Fellow at the Australian National University College of Law.
Key dates/ milestones
The Review was expected to report to Government in the first half of 2010, subject to the complexity of the matters raised.
130
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Why relevant?
“We need to ensure that the experiences of those who have been through the military rehabilitation and compensation system are considered as part of the Review, and I am grateful to those organisations and individuals who have made submissions,” Mr Griffin said. The Review is critical in identifying solutions for wider concerns relating to military rehabilitation and compensation. It is a significant step by the Government towards addressing concerns with military rehabilitation and compensation legislation and the administration of the schemes.” 118
9.1.10 Defence Occupational Medicine and Hygiene Capability Project
The Occupational Medicine and Hygiene Capability project is designed to address Recommendations 2.1, 2.2, 2.5 and 2.6 from the F111 Deseal/Reseal Board of Inquiry (F111 BOI) and their associated End State Descriptors (ESDs).
The EDSs require Defence to establish an occupational medicine program, particularly where significant industrial activity occurs, including ensuring that occupational medicine and occupational hygiene support is available. These recommendations also require Defence to reconsider its requirement for medical services, so that doctors delivering primary health care at Defence establishments are afforded the time to familiarise themselves with workplaces and practices as well as the time to do any training and necessary research.
The key focuses of the project are on a strategic approach to occupational hygiene and the provision of relevant equipment, training, career paths, corporate policy and operational direction for occupational medicine and occupational hygiene in Defence. This will result in the implementation of a program of risk controls and associated health surveillance, biological and environmental monitoring across Defence, designed to ensure Defence is meeting regulatory requirements and its duty of care, and progressively reducing exposures to occupational health risks.119
The vision for the project is:
“Within five years, the Department of Defence guarantees 100% compliance with all relevant Occupational Hygiene Standards and can demonstrate a sustained continual reduction in work-related fatalities and the incidence of serious workplace injury, through the provision of occupational medicine and occupational hygiene support”120
118 Media Release The Hon Alan Griffin MP, Minister for Veterans’ Affairs 15 July 2009
119 http://ohsc.defence.gov.au/Programs/DCOH/default.htm 120 Defence Occupational Medicine and Occupational Hygiene Capability presentation – page 3
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Key dates/ milestones
• Jun 2009 – Defence OHS Committee (DOHSC) endorsed Business Case for project
• Jun 2010 – 3 x Exposure Reduction Plans due (Fuels, Noise, Hand-arm vibration)
• 2012 – Transition to BAU
Why relevant?
• Reducing exposure of ADF members to occupational health risks – prevention of illness and/or injury
• Contribution to the capability maturity of element 7 of the OHSMS – leading long term to lower rates of injury, illness and disease
9.1.11 Military Health Outcomes Program (MilHOP) The Military Health Outcomes Program (MilHOP) aims to better inform Defence on the health challenges faced by personnel across the services as well as documenting the impact of deployments to the Middle East Area of Operations (MEAO).
As one of the most extensive studies ever conducted on the health and well-being of Australian serving and ex serving personnel, MilHOP will provide Defence with the information it needs to develop health services in the future. All members are being actively encouraged to participate in the program.
MilHOP is run by the Centre for Military and Veterans Health (CMVH).
Key dates/ milestones
• The study is scheduled to be complete by 30 Jun 2012
132
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Why relevant?
• “Consistent with the recommendations to Defence from the 2009 Dunt Review, this study will also seek to establish the prevalence of mental health issues within the Australian Defence Force, and explore issues of stigma and barriers to seeking care,”121
• Information collected will enable Defence to develop health services which support injured or ill members
9.1.12 Single Access Mechanism (SAM) – reducing the backlog and enhancements
In January 2008, Defence and DVA signed a SLA for the “Provision of Health Records and/or Particular Service of Serving and ex-Serving members’.
With effect from 1 July 2010, the Defence SAM team was established within the Directorate of Transition Support Services (DTSS). It acts as the only access point within Defence through which DVA is to request information to assist with determining compensation claims, and through which Defence will provide this information to DVA. It is also the only access point through which the Medical Employment Classification Review Boards (MECRB) can seek information from DVA on the status of ADF member’s claims. Discussions are underway with ComSuper to replicate SAM for the provision of MECRB information to assist ComSuper with determining superannuation benefits for medically separating ADF members.
Key Performance Indicators
• Non-urgent requests – 28 days from the date request is sent
• Urgent requests – 3 days from the date request is sent
The SAM team has inherited a significant backlog of information requests. Since the team was established in July it has received approx. 7,000 requests for information and/or records to support current and former ADF member’s compensation claims. 7 x NOG staff are being recruited to assist in reducing this backlog.
Total Requests Closed Processed Unprocessed
6,933 1,699 2,359 2,875 Table 24 SAM Requests for the period Jul to Sep 2010
Where “Total Requests” are specific information requests, from DVA to Defence, per member per Act, “Closed” represents requests that have seen information returned to DVA; “Processed” represents those information requests that have been logged and are being progressed by the
121 Ministerial Media Release 15 June 2010 Minister for Defence Personnel launches Defence’s largest health study – Minister for Veteran’s Affairs and Minister for Defence Personnel Alan Griffin http://www.cmvh.org.au/index.html?page=136348&pid=128009
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
SAM team and “Unprocessed” represents those requests that have been sent through by DVA but no action had occurred.
Key dates/ milestones
• Jun 2011 – current backlog cleared. Business as usual operations commence
Why relevant?
• Assists in the determination of compensation claims by facilitating the timely provision of claims related information and supporting documentation.
• Can be a bottleneck in the claims process if not appropriately resourced.
9.1.13 Consolidating a member’s medical and psychology record JHC is progressing a project which will see a member’s medical and psychology record consolidated into a single/combined health record.
9.1.14 Interdepartmental Working Group (IWG) The IWG have progressed a number of initiatives aimed at reducing the administrative burden on current and former ADF members and their families when dealing with government Agencies. Refer to 10.1.2.
These initiatives include:
• Proof of Identity (POI) - align POI requirements for ADF members across government agencies. This activity has concluded – a POI pack has been designed and details are in the Dec 2010 ADF Transition handbook.
• ADF Transition Handbook - to assist members and their families at the time of separation by providing easy access to information and entry points into the IWG agencies and other support services. IWG representatives will assist in the annual production of the handbook by ensuring the information contained in it is accurate. A revised edition was produced at the end of each year. DTSS is responsible for producing the handbook.
• Allowance Summary – The IWG compiled a table that details the treatment of ADF allowances for Taxation, Centrelink benefits and ComSuper pension entitlements to ensure transitioning and former ADF members and their families receive consistent and accurate advice. Defence is responsible for maintaining the accuracy of the information in the table.
• Combined Medical Review Form –Refer to 9.2.3
• Medical Reviews for Totally and Permanently Incapacitated Veterans - A change to processes which will exempt Totally and Permanently Incapacitated (TPI) veterans from
134
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
having to also undertake medical reviews to receive the Disability Support Pension from Centrelink formally commenced in March 2010, following the amendment of formal Centrelink guidelines and policies. Eligibility for TPI will be an indication of eligibility for the Disability Support Pension, therefore negating the need for these medical reviews. An interim process was established in the lead up to March to ensure TPI veterans were not disadvantaged in the interim. The change applies only to TPI veterans at this stage.
• Separation Health Examination Trial - Refer to 9.2.2
• Engaging with the ex-service community and continuing the work simplification of Defence Force Income Support Allowance (DFISA) payments and also around reducing the requirement for reviews by multiple agencies in regards to incapacity and carer payments.
Key dates/ milestones
• Ongoing
Why relevant?
• Examining then implementing process improvements to reduce the administrative burden on Veterans, ex-service personnel and their families.
9.1.15 Service Model/Mix Review - VVCS Following discussion with the Minister’s National Advisory Committee of the VVCS, the Secretary of the DVA and the Deputy President of the Repatriation Commission, an independent review was commissioned to provide advice on the appropriate service delivery model for VVCS to meet the changing needs of the veteran and defence communities and their families and to ensure VVCS continues to provide responsive flexible services.
The review will provide advice on a model of service delivery that meets the changing needs of the veteran and defence communities.
Independent consultants were appointed to conduct the review. A Project Board provided leadership for the review. The board included the National Manager VVCS, the Chair of the National Advisory Committee, a DVA Deputy Commissioner and other key staff.
The review will utilise available data and reports on VVCS operations and evaluation of programs. The reviewers will consult with staff and management of VVCS, the Department, consumers and other significant stakeholders including ESOs, ADF and VVCS providers.
The review may result in recommendations relating to:
• Better service planning;
• Streamlining work flow processes;
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Consistency in the way business is performed; and
• Meeting the changing needs of clients.
Key dates/ milestones
The review concluded at the end of Jul 2010. The report has been provided to the Project Board and the VVCS for consideration. It is expected a communication of the decisions and outcomes will be available later in 2010.
Why relevant?
• Ensure VVCS continues to provide responsive flexible services/ support to eligible members.
9.1.16 Rehabilitation and Compensation (R&C) Business Redesign Blueprint Project (DVA)
DVA’s ICT Strategic Plan 2010-2015 has identified a number of priority projects for optimising ICT costs and risks, transforming the business and delivering on government commitments. Compensation processing has been identified as a medium term priority and a critical first step is for DVA to formalise its business strategy and desired future state for this area of the business.
The business drivers include the need to:
• implement a shared capability within Rehabilitation and Compensation for processing claims under the VEA, SRCA and MRCA;
• better support DVA staff who work in the Rehabilitation and Compensation area; and
• take a whole-of-client and client-centric approach to meeting the needs of career serving and ex-serving members of the ADF.
Key dates/ milestones
• Oct 2010 – Draft Blueprint available
• Nov 2010 – Revised Blueprint prepared
• Dec 2010 – Final Blueprint available for consideration by the Executive Management Group (EMG)
136
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Why relevant?
The R&C Redesign Project has close ties with Defence Links as many of the improvement opportunities identified during the project will leverage off the work currently being undertaken by Defence Links with Defence.
9.1.17 ADF Compensation Support A Health Directive to support the distribution of claims and determinations to ADF medical officers has been submitted to the Health Policy Working Group for clearances and publication.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
9.2 Completed projects with SIIP impacts
9.2.1 Response to Dunt Review and recommendations (in progress) Professor David Dunt was commissioned to conduct an independent review of the effectiveness of ADF mental health care and programs, and support through the transition process from Defence to DVA122. He was also commissioned to conduct an independent study into suicide in the Ex-Service Community.123
The review’s focus was to benchmark the current ADF mental health support services against best practice and administrative perspectives, including the transition process to DVA and the extent to which mental health services meet the needs of serving and transitioning ADF members.
Defence has agreed to 49 of the 52 recommendations and partially agreed to three recommendations. Funding of $83M has been allocated to start a major program of reform that will address the gaps identified, including providing improved mental health governance and policy, an enhanced mental health workforce, improved mental health training for ADF personnel and providers, enhanced prevention strategies including better research and surveillance, enhanced mental health rehabilitation and transition services, greater involvement of families in the mental health of ADF members, and better facilities from which mental health services will be delivered.
Defence’s comprehensive plan to address the Dunt Review recommendations focuses on the following major goals:
• Improving mental health governance;
• Improving mental health policy;
• Enhancing the mental health workforce;
• Improving mental health training;
• Prevention strategies;
• Enhanced research and surveillance;
122 Review of Mental Health Care in the ADF and Transition through Discharge Jan 2009 (Dunt Review – ADF) http://intranet.defence.gov.au/vcdf/sites/dmh/ComWeb.asp?page=39084
123 Independent Study into Suicide in the Ex-Service Community Jan 2009 (Dunt Study – DVA) http://www.dva.gov.au/health_and_wellbeing/research/Documents/Dunt%20Suicide%20Study%20Executive%20Summary%20Jan%202009.pdf
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Rehabilitation and return to work programs;
• Transition services;
• Families; and
• Facilities.
Appendix K details DVA’s progress against their recommendations, as at 30 Jun 2010. Of the 21 recommendations DVA are tracking 8 have been closed because the action is complete or the recommendation is finalised and 1 has no direct role for DVA as the recommendation is being implemented by Defence. Work in progress includes:
• Reviewing the Operation Life workshops to ensure the programs that are evidence based are being implemented;
• Reviewing the outcomes of the Lifecycle, Barriers to Rehabilitation and Hard-to-Engage initiatives
• Study into the health effects of service on families (the Vietnam Veterans’ Family study)
• Holding a Family Forum – in collaboration with a nationally recognised centre;
• A joint Keeping in Touch program post-discharge is being trialled;
• Appointment of relevant mental health practitioners to provide high quality clinical and policy advice;
• A review of current business processes across the 3 Compensation Acts is being conducted. This is associated with the single claim form process. A full business process re-design is expected to be completed by 30 Jun 2011;
• A phased implementation strategy is being considered to ensure every VRB hearing for a veteran involving a mental health related condition aims to have one member with a clinical mental health background on the member board; and
• A strategic review of departmentally funded PTSD programs covering service access, acceptability and cost and most successful models of care.
9.2.2 Separation Health Exam (SHE) trial The purpose of the SHE is to provide Defence with a picture of the member’s health at the time of their separation from the ADF. DVA and ComSuper require similar information for those members seeking benefits from those organisations. Therefore, members could potentially undergo the same examination multiple times around the time of separation.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
The SHE trial was a government initiative conducted to simplify the submission of compensation claims to DVA and, where relevant, ComSuper by all separating ADF members. The trial was held between 3 Nov 2008 and 31 Jul 2009 in Canberra and Wagga Wagga.
The trial process combined the SHE, DVA claims submission, the ComSuper DM042 form and the Privacy and Disclosure by the DVA and/or ComSuper sheet into four distinct parts of one Defence form.
The process that was trialled included:
• ADF Transition Staff provided members with the SHE form and advised them to complete as much of the form as possible prior to the SHE consultation;
• Defence MO conducted the SHE and completed the relevant components of the revised form;
• Members wishing to submit claims for DVA entitlements listed all relevant medical conditions on the SHE. Member completed the Privacy and Disclosure by the Department of Veterans’ Affairs and/or ComSuper (PM554-4) section;
• MOs provided comments on the medical conditions for which the claims were submitted and flagged relevant documents for photocopying. Health administrative staff photocopied these flagged documents and forwarded copies to Transition Services; and
• ADF Transition Staff confirmed proof of identity and provided the PMKeyS ADO service history record to DVA and ComSuper as applicable.
Findings
• The single claim form significantly reduced the administrative burden imposed on members submitting claim forms under the multiple applicable Acts.
• An unintended consequence of the trial was the transfer of responsibility from the member (and their ESO advocate) to health staff for the identification, photocopying and transmission of medical documentation to support claims (with no additional resourcing provided for these activities during the trial).
• DVA experienced a significant delay between the date of the SHE and when the claim was received by DVA. DVA also reported a lack of supply of relevant documentation which had a significant impact on the Delegate’s ability to determine a claim prior to separation.
Further actions
• Defence/DVA Links Steering Group to address issues relating to Agency responsibility for providing assistance to members wishing to submit DVA claims and the resourcing of the
140
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
claims management function. Communication strategies for any subsequent trial need to include ESOs. Resolve the financial and human resource burden associated with photocopying documentation to support DVA claims.
• “If DVA Links can resolve the claims management function issues, CJHLTH would support the conduct of a further SHE trial”.124
• “It is recommended that ComSuper, DVA and Defence meet and complete a detailed evaluation and then look to progress the simplified process either as a continuation or modified version of the SHE trial.”
125
Why relevant?
• Attempt to reduce administrative burden on separating ADF members by providing an integrated and simplified claim process – minimising the requirement for multiple separation medical exams.
9.2.3 Single Claim Form (SCF) – DVA The trial of the Single Claim Form (SCF) and associated business processes was run in three locations (Queensland, Victoria and Western Australia).
The SCF trial was not intended to test every complexity related to claiming compensation but was designed around testing the form itself and a new way of processing and then evaluating the client experience.
An evaluation is underway to assess the outcomes from the trial including whether the trial achieved its objectives. Feedback to date suggests that the SCF makes it much easier to lodge a claim and significantly reduces some of the administrative work involved in obtaining and photocopying a member’s service and medical documents.
Why relevant?
• Member experience: Entitlements are explored under all applicable Acts and the outcome explained to members so they understand the options available to them and the general impacts of any choice they make, particularly where there is entitlement under more than one Act.
9.2.4 Think Tank 2010 – Centre for Military and Veterans’ Health (CMVH) On 27 and 28 Oct 2010 the CMVH hosted a Think Tank event titled “Readjustment to normal – how can DVA and Defence help?”
124 Clearance of Separation Health Examination (SHE) Trial Defence Evaluation Report January 2010 SGADF 19 April 2010 (CJHLTH/OUT/2010/AF2272022 125 Separation Health Examination evaluation - DVA
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
The Think Tank sought to answer two questions:
• What are serving personnel’s actual experiences of adjustment (characteristics of adjustment, challenges faced, mechanisms and behaviours used to cope)? and
• How well are Defence/DVA dealing with and assisting in these adjustment experiences?
Outcomes
Outcomes are not currently available.
Why relevant?
• Enables DVA and Defence to identify strategies (or additional strategies) that can be implemented to improve the support provided to members, former members and their families.
.
142
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
10 Governance, reporting and feedback
10.1 Current Governance arrangements
10.1.1 Defence /DVA Links Steering Committee (DLSC) This is a joint Departmental Committee managing the activities of Defence DVA Links (a joint Departmental forum on issues relating to transition management, rehabilitation, compensation and initiatives aimed at assisting ADF members and their families).
The aim of the Defence/DVA Links is to provide seamless service provision to ADF members between the two Departments.
The role of the DLSC is to:
• Monitor emerging issues;
• Support and review Defence/DVA business opportunities; and
• Improve policy development and service delivery to serving and former ADF members.
Several working groups and forums have been established under Defence/DVA Links including:
• Data Transfer Working Group (DTWG): A forum established under Defence/DVA Links to work consider and develop opportunities for streamlining business processes relating to the transfer/ sharing of electronic data between Defence and DVA.
• Defence/ DVA Health Consultative Forum: A forum integrating all business areas responsible for developing and implementing health related services to ADF members. It advises the steering committee on health issues, policy and implementation, services and delivery, post-deployment mental health, research direction and management of health hazards.
• Regional Stakeholder Forums (RSF) A forum focussed on integrated transition support services relating to ADF members. Refer to 12.1.
10.1.2 Interdepartmental Working Group (IWG) for Streamlining Administration of Transitioning and Former ADF Members
The Interdepartmental Working Group (IWG) first met in November 2007 as a result of the Government’s commitment to examine ways of rationalising the administrative burden (dealing with multiple agencies) on veterans and ex-service personnel. It aim included
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Consolidation of initial work capacity and entitlement assessments.
The IWG has recognised that it will likely be an enduring working group and that its long term Terms of Reference should be to:
• Identify where the administrative burden on transitioning and former ADF members and their families can be reduced when dealing with government agencies;
• Consider and respond to issues raised by ESOs and DFA to identify areas of potential improvement in government administration associated with current and former ADF members; and
• Provide contact points in agencies for resolution of specific issues or cases.
10.1.3 Inter-Departmental Committee (IDC) An Inter-Departmental Committee (IDC) of agency heads was formed to review the work undertaken by the IWG, and to confirm future priorities and directions for the IWG. The IDC has been meeting annually since the establishment of the IWG in 2007.
The IDC has recently made the following changes:
• annual meetings were inadequate as opportunities were being missed and there was inadequate accountability on the progress of IWG items – move to 6 monthly meetings; and
• outcomes of IDC meetings be reported to the Minister for Veterans’ Affairs - providing increased expectation and reporting, elevating the profile of the IDC and the work it progresses.
10.2 Current feedback mechanisms
10.2.1 ADF Post Separation Survey The ADF Post Separation Survey was trialled by the Directorate of Transition Support Services (DTSS) during Dec 2008 to Feb 2009. Following this successful trial it was agreed that the survey would continue and be conducted bi-annually.
The survey is designed to gather information on awareness of, access to and utilisation of the transition support services available to ADF members during their transition.
The survey is designed to evaluate the effectiveness of the transition experience provided to all separating ADF members (including non-medical separations) three to six months post separation. The survey is sent electronically to the former member’s email address and participation is voluntary. There are no unique identified – so individual member responses cannot be identified.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
The transition support services covered by the survey include:
• Transition support delivered through the regional ADF Transition Centres;
• Career Transition Assistance Scheme (CTAS);
• ADF Transition Seminars; and
• The provision of information on support services – including those provided by DVA.
Areas for improvement from the last survey period (Jun to Nov 2009(identified the following improvement opportunities:
• Increasing family involvement in the transition process including enhancing the support and assistance provided to ADF families during separation;
• Increasing awareness of the complete range on transition services; and
• Increase Unit/Ship involvement and awareness of transition services and benefits. 126
The governance and feedback mechanisms – overlaid on the systems interaction diagram suggest there are coverage gaps and that additional opportunities to obtain member feedback and overarching governance arrangements addressing support for injured or ill members would be useful additions to Defence’s SIIP framework.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Where:
• 1: Service Chiefs powers and functions as a member’s Rehabilitation Authority is delegated to DRS and ADF Rehabilitation Coordinators127
• 2: CJHLTH reports on ADFRP key reporting indicators, performance against SLAs and the results of audits/ reviews
• 3: CJHLTH reports on ADFRP key reporting indicators, performance against SLAs and the results of audits/ reviews
• 4: CJHLTH reports on ADFRP key reporting indicators and issues relating to DVA performance impacting on ADFRP outputs
• 5: CJHLTH reports on ADFRP key reporting indicators for recruitment and retention priorities
• 6: DGOHS reporting on rehabilitation and return to work outcomes and conformance with Defence policy and legislative compliance
• 7: DGOHS (through Head People Capability) reporting on ADFRP key reporting indicators for submission to Military Rehabilitation and Compensation Commission (MRCC).
127 Section 152 of the SRCA, Section 438 of the MRCA
148
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
11 Contemporary practice overview A literature review was undertaken to extract principles of contemporary practice relevant to the management of injured or ill ADF members during their Defence career and in transition from Defence.
The review considered published and grey literature128
C
, evaluations and guidelines which discuss policies, processes and services in the areas of incident reporting, welfare, health care, rehabilitation, compensation and transition. Information from Australia, UK, Canada and the US was reviewed. A detailed description of the approach to the contemporary practice review is included in Appendix .
The document review highlighted that the management of injured and ill members is a complex process involving a variety of stakeholders including the member, their family, Return to Work (RTW) coordinators, supervisors, human resource staff, claims and injury managers, treating practitioners and rehabilitation professionals. A key factor in successful injury management is a coordinated approach between all stakeholders129
Figure 27
.
represents the need for all stakeholders to work together, be educated about injury management processes and for policies and procedures to be in place to support collaborative working. Table 25 describes in more detail the key systems, the policy and procedure to support these and the best practice principles that should underpin service delivery.
Figure 28 is an overview of the journey of the injured or ill member through the systems that support return to work or separation. The diagram steps out the intervention and support required at key stages in the process and the interactions that occur between the systems.
This is a high-level view of the system and processes only and is not inclusive of all stages or variations in an individual member’s journey.
128 The term ‘grey literature’ refers to research that is either unpublished or has been published in non-commercial form 129 WorkCover WA (September 2007) Best practice in injury management and return to work: Literature review, Western Australian Government.
Rehabilitation/ coordinated
RTW
Case management/ claim management
Welfare support
Organisations Injury Management System
Primary health care
Vocational rehabilitation
Systems in place to prevent injury
Coordinated procedures to
manage workplace injury
Figure 27 Organisation Injury Management System
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
The following is a summary of the findings from the document review and includes a description of:
• Key systems required to support seamless and integrated services;
• Protocols, policy and procedures to support key systems; and
• Contemporary practice principles that underpin service delivery to injured or ill ADF members. :
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
Organisation Injury Management System
Employer
Members
Safe work practices, return to work (RTW) and injury management policies.
Compliance with injury management and workers compensation legislation.
Compliance with local workplace health and safety legislation.
Quality assurance and
Ongoing education to all members and supervisors regarding injury management procedures.
Supervisors trained in work injury prevention including RTW planning.
The workplace has a strong commitment to health and safety which is demonstrated by the behaviours of the workplace parties.
Ongoing health promotion activities and
AC563 compliance an ongoing awareness/ educational issue.
Enhanced data management systems required.
ComCare130,131
WorkCover WA
132
Heads of Workers Compensation Authorities
WorkCover Tasmania133
130
http://www.comcare.gov.au/rehab_management_systems/introduction 131 Beyond Working Well: A Better Practice Guide. A practical approach to improving psychological injury prevention and management in the workplace. Comcare. http://www.comcare.gov.au/forms__and__publications/publications/safety_and_prevention/?a=55853 132 WorkCover WA (September 2007) Best practice in injury management and return to work: Literature review, Western Australian Government. 133 WorkCover Tasmania Board. (2006). Return to Work and Injury Management Model.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
continuous improvement systems.
Data management system that is able to capture rehabilitation, processes involving referral, follow up and quality assurance, including client satisfaction and domains that explore unmet need.
Standard, comprehensible information packs, which include information on workers’ compensation, injury management, claims processes, rights, responsibilities and obligations according to legislation and best practice etc are available for employees, employers, healthcare providers and insurers
injury prevention activities.
A no-blame response to workplace injury.
Designated personnel responsible for the coordination of rehabilitation.
Commitment to workplace based rehabilitation.
Mental health literacy programs should target military staff at every level and the veteran services sector. Psycho-education programs need to be made available to clients and be proactively offered to clients and their families.
Productivity Commission134
RTW Knowledge Base
135
Institute for work and health, Canada.
136
134 Productivity Commission 2004, National Workers’ Compensation and Occupational Health and Safety Frameworks, Report No. 27, Canberra, March.
135 Factors that can affect a person's ability to return to work. RTW Knowledge Base. http://www.rtwknowledge.org/article_print.php?article_id=17 136 Seven ‘Principles’ for Successful Return to Work. Institute for Work & Health, Toronto Canada 2007.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
Incident reporting
Supervisor
Member
Organisation
Clear, well known system and procedures in place that prompt workers to notify Employer of an injury as soon as it occurs so that early intervention can occur.
A records management system meeting State and Commonwealth legislation requirements.
The workplace takes action to ensure further workplace injuries are prevented including assessment and management of the risks arising from the psychosocial working environment.
Monitoring of incidents and a proactive response to prevent similar.
Usage of (and ability to aggregate) incident data to inform a Command, Unit or Service response can be improved.
Heads of Workers Compensation Authorities137
ComCare
138
Initial treatment (first aid / primary healthcare)
Treating Doctor or
Communication protocols for information sharing between healthcare provider, employer and insurer.
Comprehensive medical record maintained in an electronic patient information management
Appropriate medical treatment provided - workers receive prompt attention and intervention appropriate to their needs.
Healthcare provider provides education and information about the injury and self-management.
Continuity of care and handover to external service providers can be improved.
Feedback to Command (need to
WorkCover WA139
Journal Of Occupational Rehabilitation
140
137 Heads of Workers Compensation Authorities. Guide: Nationally Consistent Approval Framework for Workplace Rehabilitation Providers. Accessed August 2010 at
http://www.hwca.org.au/documents/Guide%20-%20Nationally%20Consistent%20Approval%20Framework%20for%20Workplace%20Rehabilitation%20Providers.pdf 138 Safety, Rehabilitation and Compensation Act 1988: Guidelines for rehabilitation authorities. http://www.comlaw.gov.au/ComLaw/Legislation/LegislativeInstrument1.nsf/0/0B7DF5D963AF5F2CCA257051000773EE/$file/s+41+Rehab+Guidelines+-+instrument+_final_.pdf 139 WorkCover WA (September 2007) Best practice in injury management and return to work: Literature review, Western Australian Government. 140 Rasmussen, K. & Anderson, J.H. (2005) Individual Factors and GP Approach as predictors for the Outcome of Rehabilitation Among Long-Term Sick Listed Cases. Journal of Occupational Rehabilitation, 15:2, 227-235.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
Health professional
Member
system.
Clearly defined, evidence based, triggers for referral to rehabilitation.
Positive communication and reassurance provided by healthcare provider.
Patient centred approach to care and continuity of treating doctor.
Communication with employer about the workplace demands as needed, and with the worker’s consent.
know) vs. Medical-in-Confidence issue to be addressed.
ComCare
RTW Knowledge Base141
Ongoing input to facilitate RTW
Treating doctor
Member
RTW
Assessment protocols including a comprehensive assessment of the issues that impact recovery and RTW.
Guidelines for referral to rehabilitation / triggers for a rehabilitation assessment.
Evidence based decision making regarding treatment and services.
Outcome driven and patient focused treatment including the collaborative development of goals at the commencement of the program.
RTW plan established and clearly defined
Co-ordination of and communication between all stakeholders who are supporting a member can be improved.
The Heads of Workers Compensation Authorities142
Productivity Commission
141 Healthcare Provider participation is important in achieving early return to work. Return to Work: Knowledge Base. http://www.rtwknowledge.org/article_print.php?article_id=21 142 Biopsychosocial injury management. Heads of Workers’ Compensation Authorities. Accessed August 2010 at: http://www.hwca.org.au/documents/Biopsychosocial%20Injury%20Management.pdf
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
coordinator
Rehabilitation coordinator
Supervisor
Guidelines for workplace based rehabilitation and modified work.
Roster of suitable duties.
Practice guidelines for best practice clinical management of various work related conditions that should be available for clinicians.
Designated responsibility within the organisation to coordinate RTW.
Adoption of Biopsychosocial approach principles to injury management.
as soon as possible following the injury, including immediate management and strategies for RTW.
Early identification of the psychosocial barriers to recovery and RTW to determine the most effective treatment and rehabilitation approach.
Injury management is actively coordinated so treatment and return to work activities are integrated.
Regular review of progress with treatment and RTW plan and management of risk factors.
A coordinated approach between all stakeholders is essential (particularly important is linking the clinician/treating
WorkCover WA
LaTrobe University143
ComCare
144
Safety, Rehabilitation and Compensation Act
145
143 Foreman, P. Murphy, G., & Swerissen, H. (2006). Barriers and facilitators to return to work: A literature review. Australian Institute for Primary Care, La Trobe University, Melbourne.
144 Australian Government: Comcare. Rehabilitation assessment, accessed August 2010 from http://www.comcare.gov.au/injury_management/return_to_work_planning/rehabilitation_assessment 145 Safety, Rehabilitation and Compensation Act 1988: Guidelines for rehabilitation authorities. http://www.comlaw.gov.au/ComLaw/Legislation/LegislativeInstrument1.nsf/0/0B7DF5D963AF5F2CCA257051000773EE/$file/s+41+Rehab+Guidelines+-+instrument+_final_.pdf
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
Supervisor
Vocational Rehabilitation
Rehabilitation provider
Member
Treating healthcare provider
RTW coordinator
Assessment and reporting guidelines – to assess the worker’s vocational capacity and potential through vocational assessment and counselling.
Designed system of vocational services that support the full spectrum of client need.
Screening tools and assessment to identify injured persons that may not return to pre-injury role.
Policy and protocol regarding the provision of modified work and accommodations.
Return to work should be a key
Early identification of the need for vocational rehabilitation and provision of early intervention.
Provide access to direct and rapid placement opportunities into the competitive job market.
Provision of specialist support and intervention on an individual needs basis.
designed as an ongoing or indefinite system of support to the same degree that clinical services are delivered by way of a continuum of care.
Communication and coordination between the key players (individual, healthcare, and the workplace) is critical to effective
ADF Post Separation Survey statistics suggest this can be improved.
Heads of Workers Compensation Authorities147
University of Sydney
148
Department of Veterans’ Affairs
149
Vocational Rehabilitation Task Group, UK
150
147 Heads of Workers Compensation Authorities. Guide: Nationally Consistent Approval Framework for Workplace Rehabilitation Providers. Accessed August 2010 at
http://www.hwca.org.au/documents/Guide%20-%20Nationally%20Consistent%20Approval%20Framework%20for%20Workplace%20Rehabilitation%20Providers.pdf 148 Matthews, L.R. Fundamental concepts and evidence-based practices in psychosocial rehabilitation. University of Sydney: Ageing, Work and Health Research Unit. 149 http://www.dva.gov.au/rehabilitation/rehabservices/Pages/Vocationalrehabilitation.aspx 150 Waddell G, Burton A, & Kendall N (2008) Vocational Rehabilitation: What Works, For Whom, And When?, TSO, UK.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
outcome measure for vocational rehabilitation.
Vocational rehabilitation needs to be underpinned by education; the public, health professionals and employers all need to be aware of the value of work for wellbeing and healing, and also of their role in the clients return to work process.
vocational rehabilitation.
Welfare / support to members and family and transition support
Interagency agreements regarding communication and information sharing.
Consistent approach to assessment and management of psychosocial problems.
Comprehensive assessment tools sensitive to physical mobility needs, cultural diversity, gender, socio-economic and age-related
Early intervention and comprehensive assessment.
Universal access, equity of access and parity across the spectrum of need.
Consideration should be given to community tenure, family cohesion and maintaining social networks.
Inter-agency/stakeholder collaboration to meet the needs of the individual and their
Interactions with family and the management of expectations vs. entitlement can be improved.
Australian Centre for Posttraumatic Mental Health151
151 Australian Centre for Posttraumatic Mental Health. Australian Government Mental Health Lifecycle Package: Transition Mental Health and Family Collaborative (Townsville). Final Report. (April 2010)
158
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
needs, and needs of people in rural or remote locations.
Supporting veterans with rehabilitation needs to return to civilian life thus enhancing their quality of life. This may include assisting in their goals for involvement in home, community and work environments.
family.
Effective engagement and communication practices between stakeholders and the member.
Assessment and recognition of mental health problems, other social problems and related issues.
Family sensitive and inclusive practices by all stakeholders to effective and individualised advice, support and treatment.
Seamless transition between Defence and community.
Case management/ claims management
Sound customer service delivery systems promote the constructive engagement of all stakeholders and enable timely and appropriate resolution of issues.
Coordinated case management services are essential for a client-centred approach to service planning. Case managers play a core role in maintaining the continuum of care from the initial assessment, through care planning to the re-evaluation of
Status updates and communication can be improved.
Claims processing timeframes can be
RTW Knowledge Base152
WorkCover NSW
153
152 Colledge, A.L. & Johnson H.I. (2000) A simple proven return to work model. Occupational Health & Safety, 69(2):64-9.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Systems and Stakeholders
Protocols, policy and procedures Principles Current Gaps and opportunities
Information Source
All personal, health and other confidential or private information will be protected and only released in accordance with appropriate legal and governing standards.
Information management systems that enable tracking of individuals and identify risk factors.
progress. Best practices are underpinned by the quality of the communication between case managers and clients.
Injured workers and employers are treated with dignity and respect.
Rehabilitation and return to work services directly support the worker’s restoration to the community (if that is appropriate) as well as a return to work outcome.
Case management is person-centred rather than disease specific.
Claims management services are responsive to the rights and needs of our diverse population.
Claims management services are holistic
reduced. WorkCover SA154
Veterans’ Affairs Canada
155
153 Occupational Health and Safety and Injury Management Improvement Standards, 2007.
http://www.workcover.nsw.gov.au/formspublications/publications/Documents/improvement_standards_occupational_health_safety_injury_management_return_to_work_5302.pdf 154 WorkCover SA: Injury and Case Management Manual. www.workcover.com/public/download.aspx?id=1621 155 Thompson JM., MacLean MB, & Pedlar D. (2009) Literature Review of Case Management – Basis for Further Research. Veterans’ Affairs Canada, Charlottetown, Draft Version.
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
Publically available information relating to efficiency reviews and effectiveness measures on many of these programs was limited. As a result further investigation would be necessary to determine what features would be appropriate for adoption and are in fact “best” practice.
11.1 Comcare Strategic Plan 2010-2015
Comcare is an Australian government agency that works in partnership with employees and employers to reduce the human and financial costs of workplace injuries and disease in the Commonwealth jurisdiction. There is consistency between the SIIP recommendations and Comcare’s strategic direction in relation to “Back to Work”156
which is reproduced below.
“5: Strengthen recovery and support services for workers with injury • Understand the service experience and expectations of workers with injury, their
employers, unions and service providers • Provide guidance, information and support to help workers and families exercise
their compensation rights
• Co-design of a new service delivery model reflecting best practice, risk and needs
segmentation • Provide customised support to vulnerable workers at risk through case worker
intervention
• Effective and timely response to high-risk cases guided by improved performance
metrics • Simple, fast and appropriate resolution of disputes and delivery of lump sum
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
11.2 Transition Mental Health and Family Collaborative (Townsville157
The aim of the Transition Mental Health and Family Collaborative (Collaborative) was to improve mental health and family support provided to medically discharging ADF members and their families. The Collaborative was developed, implemented and evaluated by the Australian Centre for Posttraumatic Mental Health (ACPMH), in partnership with Defence and DVA.
)
The Collaborative identified 5 change priorities to improve transition mental health and family support practices:
• Engagement: More effective engagement and communication practices;
• Recognition: Better recognition of mental health problems and related issues;
• Families: Improved family sensitive and inclusive practices; and
• Interventions: More effective advice, support and treatment.
Project evaluation reflected that the Collaborative achieved considerable practice improvement in the five priority change areas. It was recognised that the challenge is now to expand this successful initiative across Australia.
More detail regarding the Collaborative is included in Appendix C.1.
11.3 Defence Military Rehabilitation Centre (DMRC), Headley Court UK158
The DMRC is a dedicated rehabilitation service provided to UK Defence members with physical injuries/ disabilities on an inpatient basis. Rehabilitation staff include specialist medical officers, nurses, exercise rehabilitation instructors (ERI), physiotherapists, occupational therapists, speech and language therapists, cognitive therapists, social workers, engineers, and administration support staff. DMRC also deals with members suffering from post-traumatic stress disorder. DMRC relies on significant public and charity funding.
The guiding principles in rehabilitation service delivery at DMRC:
• Multidisciplinary teams delivering interdisciplinary rehabilitation.
More detail regarding DRMC is included in Appendix C.2. 157 Australian Centre for Posttraumatic Mental Health. Australian Government Mental Health Lifecycle Package: Transition Mental Health and Family Collaborative (Townsville). Final Report. (April 2010) 158 English, R. Post Visit Report: U.S.A and U.K. Military Rehabilitation Services. 2nd April to 3rd May 2010. Directorate of ADF Rehabilitation Services.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
11.4 Veterans’ Affairs Canada (VAC) Rehabilitation Program (RP)159
The Veterans’ Affairs Canada (VAC) Rehabilitation Program (RP) is a program within the NVC offering medical, psychosocial and vocational rehabilitation. The VAC RP has three main goals:
• Provide client centred rehabilitation to Canadian Force (CF) members including restoring physical, mental, social and vocational functions to an optimal level.
• Supporting veterans with rehabilitation needs to return to civilian life thus enhancing their quality of life. This may include assisting in their goals for involvement in home, community and work environments.
• Supporting family adjustment to the veteran’s disability.
The VAC RP is available to CF members after separation and has two main client groups:
• Individuals who apply to the program within 120 days of being medically separated. For these individuals VAC covers expenses not covered by SISIP like medical/psychosocial rehabilitation and earning loss beyond the two year post-release period.
• Any veteran with a Service-Related Rehabilitation Need (SRRN) that causes a difficulty to re-establishment in civilian life.
11.5 Primary Care Partnerships160
Primary Care Partnerships (PCP) have been established in Victoria to create a more effective primary care system and improve coordination of care between providers. Primary Care Partnerships are voluntary alliances of primary care providers and typically cover two or three local government areas. PCP aim to improve the health and well-being of their catchment's population through better coordination of planning and service delivery in response to identified needs. The improved outcomes of the PCPs include:
• better access to services;
• improved continuity of care; and
• chronic disease prevention and management.
Central to this collaborative approach is the sharing of consumer health and care information between Agencies.
Some features of the PCPs that could be adopted into the management of injured or ill Defence members include:
• The use of secure electronic systems to share consumer health and care information.
159 MacLean, MB., Thompson, JM., & Poirier, A. (2010) Rehabilitation Needs of VAC Clients Post Eligibility for the SISIP Vocational Rehabilitation Program, Research Directorate Technical Report, Veterans’ Affairs Canada, Charlottetown. 160 Primary Care Partnerships strategic directions 2004-2006. Victorian Government. Accessed October 2010 from http://www.health.vic.gov.au/pcps/downloads/strategy/pcp_strat_2004_06.pdf
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Practice standards - agreed standard practices for coordinating services and sharing health and care information.
• Standard suite of tools – ‘service coordination tool templates’ used to document consumer information, identify consumer needs, coordinate care planning and make referrals.
• Electronic service directories – to access information about other services.
• Electronic referral systems.
11.6 Australia Post - Rehabilitation Management System Australia Post (AP) was awarded a SRCC Safety Award in 2009 for, Creating a Nationally Consistent Approach to the Provision of Rehabilitation Management161
AP identified there were inconsistencies in their approach to rehabilitation management between states as well as between internal and external rehabilitation providers. While good return to work outcomes were being achieved, AP endeavoured to establish a management system and nationally consistent approach to rehabilitation that would become industry best practice.
.
In 2006 AP’s Workplace Injury Prevention and Management Unit (WIPM) was formed. This branch brought together each state rehabilitation function under national management with the aim of:
• Forging closer working relationships between Rehabilitation, Workers’ compensation and OH&S.
• Ensuring Rehabilitation, Workers’ compensation and OH&S issues and outcomes were tabled and discussed at the National Executive level.
• Standardising rehabilitation processes and procedures, drawing on the strengths of each state to create a national approach .
• Ensuring injured workers receive consistent service regardless of their location.
• Creating strong working relationships between state rehabilitation managers.
• Reducing workers’ compensation costs.
A more detailed description of this system is included in Appendix C.3.
161 Comcare: The Safety, Rehabilitation and Compensation Commission (SRCC) Safety Awards. http://www.srcc.gov.au/safety_awards/2009_srcc_safety_awards/winners_and_finalists/about_the_winners#five
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
12 Stakeholder consultation Significant stakeholder consultation through field analysis, the involvement of the SIIP Project Steering Group and SIIP Working Group stakeholders has occurred during this review.
This section contains a summary of their input – identifying what is good with the current system and where there are gaps and issues with the current system .
12.1 Positives Stakeholders were generally pleased with the following elements of the current support for injured or ill members:
• The clinical care provided to injured or ill members is generally appropriate to the needs of the member. Good clinical treatment is provided in a timely manner. There are generally no barriers to the provision of treatment although stigma associated with mental health issues still exist.
• The ADFRP framework – the existence of a framework and its flexibility - especially that feedback from the MOs regarding entry to rehabilitation triggers had been acknowledged and reflected in recent modifications to the framework.
• The conversion of Program Case Manager (PCM) roles to APS positions and integration into Garrison Health Regional Health Services as part of the Garrison Health Transition Project – it is felt this will provide greater likelihood of case manager continuity as the APS roles will be committed/ dedicated to a Unit or Health Centre. The review team were made aware of one example where a member, separating on medical grounds had 13 different PCMs during her separation. It is also felt that converting these into APS roles will provide more focus on member rehabilitation rather than the perception of the current strong commercial/ business focus. It is also expected to allow for greater consistency of the services (and level of services) being provided by the case managers.
• Infrastructure investment in health facilities – Kapooka (Kapooka Health Centre, new RAP, rehabilitation/hydrotherapy facilities and Digger James 2 (Rehabilitation) platoon facilities) and Amberley (1EHS health facilities) were examples where infrastructure investment was significantly improving the health and rehabilitation facilities available for members.
• Integration/ co-location – Service providers including counsellors, rehabilitation Coordinators, claims assistance and transition service providers felt that the co-location (or close relationships and networks where co-location due to available workspace) resulted in the best outcome for members. Being able to offer a “one-stop” shop where a service provider can cross refer and introduce a member to the appropriate service provider (often arranging interviews/ appointments during the initial consultation) provided greater comfort to the member and increased the likelihood of the member following through with the service provider. The ability of family members/ support to attend these meetings was also viewed positively.
166
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Regional Stakeholder Forums (RSF) – the purpose of the RSF is to enable a regionally based coordinated interdepartmental forum to focus on issues relating to the provision of transition support services. These are conducted in 9 locations around Australia – based on geographic spread and the size of the Defence presence in the area. The RSF structure brings together organisations that contribute to the total delivery of services to transitioning ADF members. It comprises key stakeholders from Defence, DVA and other agencies that have specific responsibility for delivery of transition support services to separating ADF members. Minutes are recorded for each meeting and forwarded to Head Defence Support Operations (HDSO) to inform them of regional issues which may require a consolidated response/ approach to addressing. Participants viewed these as very worthwhile communication forums.
• Defence Force Recruiting (DFR) familiarisation visits – by visiting Defence establishments including training facilities it was felt this enabled DFR contractors to better understand the requirements of Defence training, training activities and facilities and therefore better inform potential recruits about what to expect and how to prepare physically and mentally. These familiarisation visits are, in part, believed to contribute to improved training facility success statistics.
• Cultural change – new recruit training – it was felt that newer entrants into the ADF were aware of their requirements with respect to completing OHS incident notification and claim/ compensation paperwork as a result of the entry training they were receiving in these areas. It is felt this translates into higher compliance by this demographic.
• Local focus groups/ case conferences – many of the locations visited hold regular command meetings (variously called focus group, rehabilitation meeting, and case conference) where a member’s situation is discussed. Depending on the location, these meetings were held weekly, fortnightly, monthly or on an as required basis. Their focus could be administrative, medical or a combination of both but are generally designed to inform Command of the status and issues affecting their members. Stakeholder representation varied by location but generally included MOs (including Psychologists, Physiotherapists), COs, Case Managers (CCM, RCASO), Rehabilitation Case Managers, PTIs, DCO etc. These meetings were viewed as particularly useful in informing Command of the member’s situation and progress, ensuring service providers were aware of a member’s needs and preventing a member from shopping around for their preferred outcome (being economical with the truth etc). Refer to 12.2.11 for issues applicable to this approach.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
12.2 Gaps and issues The following circumstances and situations were raised by stakeholders as potential places where a member can fall through the “gap”, thereby not receiving the support they require or are entitled to:
• Overall visibility of members on rehabilitation programs - from a Unit and Service level - absence of management reports, performance metrics to inform Command and Unit of available capability, emerging trends etc. For instance – there is no flag/ field in PMKeyS which indicates that a member is on a rehabilitation program.
• Support system at times relies on member to hold up their hand and request assistance - self refer - noting some members are not in a position/ comfortable doing this to do this.
• Converse to the above point, a member may self refer to VVCS, civilian practitioners or to a psychologist and the CO has no visibility of this. The requirement to treat this information as medical-in-confidence is acknowledged and understood by Command but concerns about them not being informed of any workplace issues this referral and treatment may lead to (side effects of treatment, restrictions on operating heavy machinery/ equipment/ driving etc, if/how the workplace is contributing to the condition etc) were raised.
• Members on long term convalescence leave who return to family (i.e. posted away from their Unit/ CO) - concern they are not visible to new CO/ structure for the duration of their convalescence leave. Issue where contact details have not been provided/ accurately recorded (noting this is a member’s responsibility) or the location where convalescence leave is being taken is a significant distance from a Defence establishment. An additional issue in these circumstances is ensuring appropriate handover of medical information between Defence MOs and local/ civilian medical facilities and practitioners.
• Members on maternity leave – example provided where a member was on maternity leave. Following successful delivery of child the member suffered post natal depression. The Unit was unaware of this and required dedication of significant effort to support member and get them to re-engage with Defence.
• Separated members who have not seen active service and do not have an accepted claim with DVA - not eligible for VVCS (due to no service) or DVA support. Reliant on community support services. This is not recorded here as a gap in services provided as this is the design of the support system, more so a gap in the expectation of former members and their family regarding entitlement.
• Trainees - medically separate quickly – may be unaware of their entitlements, support services available to them,
• Trainees – medically separating with a MEC 3 classification. Refer to 12.2.9 for a description of this gap.
168
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• Members who voluntarily separate when a medical separation is appropriate.
• Members who medically separate but choose not to engage, or are not in a position to engage with Transition Services so are unaware of their full entitlements and may not be linked in to available services.
• Defence services geared towards the member and not the member’s family even though Service related activity may have caused or contributed to the need for services. Marriage counselling was one example noted where the member costs of counselling were covered but spouse related costs (if the spouse is not an ADF member) are generally not covered after the allowable number of DCO funded consultations have been exhausted. It was suggested that members are opting out of counselling in these instances where they might have to pay for the service.
12.2.1.1 Recommendations
REC 1.2 - It is recommended a program of work be established to progress and implement recommendations arising from this review. A dedicated Program Manager should be appointed to provide oversight across the program of work and to monitor and report on progress, dependencies, issues and risks.
REC 2.1 - It is recommended Defence provides qualifying ill or injured members with a Member support framework which, depending on the individual member circumstances could consist of a Member Support Officer (MSO), Rehabilitation Consultant (RC) and Command (always). This framework provides member case coordination across all stakeholders to ensure an injured or ill member and their family are supported throughout their injury, illness and rehabilitation outcome and, possibly, medical separation and transfer to external health care and support services.
REC 2.2 - It is recommended Defence fully defines the role, function and responsibilities of the MSO, RC and Command as they relate to supporting injured or ill members. It is further recommended that Defence defines and documents the triggers, criteria, conditions and circumstances that would “qualify” a member for entry into the Member Support framework.
REC 2.6 – It is recommended DGPERS Air Force and DG Navy People implement a individual member ‘welfare board’ equivalent within their Service for seriously ill or injured members.
REC 3.1 – It is recommended Defence investigates content/ knowledge management solutions to support the effective management of information.
REC 3.2 – It is recommended Defence investigates a technology solution to “push” personalised information to an injured or ill member (and/ or family) based on information.
REC 4.1 – It is recommended Defence utilise information technology to better support injured or ill members. Required information is available on a need to know basis to support effective
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
information exchange, management reporting and enable informed decision-making. Workflow functionality is utilised to educate, guide and encourage compliance from service providers. An audit trail of activity is maintained.
REC 4.2 – It is recommended that a requirements team of subject matter experts is formed to develop and feed SIIP requirements into the JeHDI and JP2080 projects.
12.2.2 Governance and ownership As can be seen from the process maps, there are a significant number of entities that can be involved in an injured or ill member’s journey – hereafter referred to as the “system”. The review team identified the following gaps in the overarching governance arrangements which ensure ill or injured members are supported, including:
• Who owns the system?
• Who has accountability for ensuring the system works?
• What quality assurance metrics are utilised to measure if the system is operating efficiently and effectively?
12.2.2.1 Recommendations
REC 1.1 – It is recommended an owner is appointed to provide oversight to the systems which support injured or ill members. The owner will determine appropriate system performance metrics and report on these. The owner will ensure an effective and appropriate system governance framework is in operation.
REC 5.1 - It is recommended the SIIP Project Steering Committee continues to convene after the conclusion of the SIIP review to provide overarching governance to Defence’s support for injured or ill members. It is further recommended that the title of the Steering Committee incorporates “wounded” to demonstrate an inclusiveness of injuries sustained whilst on Operations, in addition to illness or injury.
REC 5.2 – It is recommended that a joint review, update and redrafting of the overarching memorandum of understanding (MOU) between Defence and DVA occurs – to provide a refreshed/ current framework for implementing SIIP recommendations.
REC 2.2 - It is recommended Defence fully defines the role, function and responsibilities of the MSO, RC and Command as they relate to supporting injured or ill members. It is further recommended that Defence defines and documents the triggers, criteria, conditions and circumstances that would “qualify” a member for entry into the Member Support framework.
170
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
REC 6.1 - It is recommended CJHLTH defines and establishes performance metrics for the MECRB process areas within Joint Health Command control. It is recommended that the Services (including their personnel management agencies) define and establish performance metrics for the MECRB process areas within their influence and control.
REC 8.1 – It is recommended the Program Manager assigned in REC 1.2 oversee the development of a comprehensive and interrelated roles and responsibilities framework. This must include the functions each role performs and handoffs between roles.
REC 10.1 - It is expected that the conversion of PCM roles into APS positions and integration into Garrison Health Services as part of the Garrison Health Transition Project, will suitably address a number of the gaps in the ADFRP. It is recommended the conversion activity, including appropriate and sufficient resourcing levels, are monitored and reported on to the governance committee (REC 5.1).
12.2.3 Australian Defence Force Rehabilitation Program (ADFRP) A number of stakeholders interviewed during the field analysis phase of this review raised issues with the ADFRP – both in the way people were utilising and referring members into the program as well as some of the handoffs that exist within the rehabilitation framework.
• MOs not referring suitable members for rehabilitation. Reasons include:
o The MO not being fully aware of the ADFRP, entry triggers and services offered through the program.
o MO determining they should provide the rehabilitation program for the member.
o Residual issues when the ADFRP was first implemented – including the cost of services provided being visible to the Unit and MO (even though these were funded by the ADFRP), MO resentment with perceived limited consultation prior to implementation etc.
o The member opting out of rehabilitation. Whether the member was in a position to make an informed choice to opt out of rehabilitation, and their motives for doing so were not considered in this review.
• Concern that members on rehabilitation programs are transferred to roles that do not provide them with a conducive environment for rehabilitation. Units wear the liability for members on rehabilitation. One example involved a member (MEC3) being transferred into a busy training role due to Unit resourcing constraints. This concern also extends to where field waivers are being provided to MEC3 members – although no hard evidence was available to support this view – Rehabilitation Coordinators felt that approx 60% of Army MEC302 members in a certain location had field waivers.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• PCMs providing information to COs when the information is more appropriately directed to the MO for actioning.
• The service provided by some (a minority) PCMs was unsatisfactory. Instances where a single phone call was the only contact between the member on rehabilitation and their PCM or where the PCM tried to contact the member via phone, left a voice message for the member and that was the extent of contact.
• Handover between Defence and civilian MOs/ treatment facilities can be improved.
• Absence of any system containing appropriate performance metrics to enable rehabilitation referral patterns and PCM individual case manager workloads to be measured and monitored.
• The significant workload of PCMs in some regions results in instances where service provision is prioritised – less visible or demanding members might not get the services they are entitled to in this instance.
12.2.3.1 Recommendations
REC 10.1 - It is expected that the conversion of PCM roles into APS positions and integration into Garrison Health Services as part of the Garrison Health Transition Project, will suitably address a number of the gaps in the ADFRP. It is recommended the conversion activity, including appropriate and sufficient resourcing levels, are monitored and reported on to the governance committee (REC 5.1).
REC 2.1 - It is recommended Defence provides qualifying ill or injured members with a Member support framework which, depending on the individual member circumstances could consist of a Member Support Officer (MSO), Rehabilitation Consultant (RC) and Command (always). This framework provides member case coordination across all stakeholders to ensure an injured or ill member and their family are supported throughout their injury, illness and rehabilitation outcome and, possibly, medical separation and transfer to external health care and support services.
REC 2.6 – It is recommended DGPERS Air Force and DG Navy People implement a individual member ‘welfare board’ equivalent within their Service for seriously ill or injured members.
REC 4.1 – It is recommended Defence utilise information technology to better support injured or ill members. Required information is available on a need to know basis to support effective information exchange, management reporting and enable informed decision-making. Workflow functionality is utilised to educate, guide and encourage compliance from service providers. An audit trail of activity is maintained.
REC 5.1 - It is recommended the SIIP Project Steering Committee continues to convene after the conclusion of the SIIP review to provide overarching governance to Defence’s support for
172
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
injured or ill members. It is further recommended that the title of the Steering Committee incorporates “wounded” to demonstrate an inclusiveness of injuries sustained whilst on Operations, in addition to illness or injury.REC 8.1 – It is recommended the Program Manager assigned in REC 1.2 oversee the development of a comprehensive and interrelated roles and responsibilities framework. This must include the functions each role performs and handoffs between roles.
REC 10.2 - It is recommended the Services, through their DGPERS, consider whether it is appropriate for members classified as MEC 302 to be posted into Unit pool positions so that their active position can be filled by an able member until the member on rehabilitation is assessed as fit to return to work.
REC 10.3 – It is recommended the ADFRP implement a process to seek member feedback on the efficiency and effectiveness of the rehabilitation and support received through the ADFRP.
12.2.4 Awareness – roles, responsibilities, functions Not surprisingly with a system of this size, local and regional nuances and recent changes to elements of this system, there were a number of gaps identified in relation to peoples understanding of their (and others) roles, responsibilities and functions and how to appropriately hand over to other service providers.
• A member may have many “case managers’ including a medical, rehabilitation, compensation claims and transition case manager and possibly even a MRCA section 64 case manager (perhaps a CCM) assigned to them as a legislative obligation of their Rehabilitation Authority. This situation could be extremely confusing for the member as well as the added communication difficulties associated with communications between “case managers” and command.
• Confusion over roles, responsibilities and interactions between case managers, RCASOs, DCO, APCDs and Transitions teams. This contributed to instances where some service providers were making decisions outside their responsibilities or expertise including:
o Some COs involving themselves in medical decisions – including determining that a member does not require rehabilitation.
o ESOs/RCASOs providing services that DCO social workers believe are not in the longer term best interests of the member or their family.
o APCDs involved in transition/ administrative processes – although it is acknowledged that at times it is appropriate for a command representative to assist a member to comply with their transition obligations.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• Limited understanding of requirement to hold Welfare Boards, in what circumstances they should be held and who should attend. Belief in some Units that these should only be held for MEC3 and MEC4 members.
• Limited understanding of the role of APCDs and the services they can provide to a member – especially their interaction with Transition Services. This lack of understanding is not surprising given the first 6 of the 12 APCD roles have only recently been stood up.
• Limited general awareness of the CCLO function within Air Force.
• Members not maintaining complete NOK, PEC details in PMKeyS - especially pre-deployment.
• Difficulty in encouraging Reservists (on CFTS) to complete RTAPS and POPS when they return to Australia.
• Difficulty in encouraging Reservists to complete the MECRB process for medical separation - no incentive for the Reservist to go down this path and given the administrative overhead this places on Command – this is not pushed.
12.2.4.1 Recommendations
REC 8.1 – It is recommended the Program Manager assigned in REC 1.2 oversee the development of a comprehensive and interrelated roles and responsibilities framework. This must include the functions each role performs and handoffs between roles.
REC 2.1 - It is recommended Defence provides qualifying ill or injured members with a Member support framework which, depending on the individual member circumstances could consist of a Member Support Officer (MSO), Rehabilitation Consultant (RC) and Command (always). This framework provides member case coordination across all stakeholders to ensure an injured or ill member and their family are supported throughout their injury, illness and rehabilitation outcome and, possibly, medical separation and transfer to external health care and support services.
REC 2.2 - It is recommended Defence fully defines the role, function and responsibilities of the MSO, RC and Command as they relate to supporting injured or ill members. It is further recommended that Defence defines and documents the triggers, criteria, conditions and circumstances that would “qualify” a member for entry into the Member Support framework.
REC 4.1 – It is recommended Defence utilise information technology to better support injured or ill members. Required information is available on a need to know basis to support effective information exchange, management reporting and enable informed decision-making. Workflow functionality is utilised to educate, guide and encourage compliance from service providers. An audit trail of activity is maintained.
REC 5.1 - It is recommended the SIIP Project Steering Committee continues to convene after the conclusion of the SIIP review to provide overarching governance to Defence’s support for
174
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
injured or ill members. It is further recommended that the title of the Steering Committee incorporates “wounded” to demonstrate an inclusiveness of injuries sustained whilst on Operations, in addition to illness or injury.
REC 5.2 – It is recommended that a joint review, update and redrafting of the overarching memorandum of understanding (MOU) between Defence and DVA occurs – to provide a refreshed/ current framework for implementing SIIP recommendations.
REC 6.5 – It is recommended Defence and DVA (through the DLSC) agree to accelerate and leverage the co-location of injured or ill member support services.
REC 7.1 – It is recommended that all areas responsible for the development of health related policy (including CJHLTH, the single Services and Transitions Support) leverage the policy development and reform activity in the Personnel Policy and Employment (PPEC) Branch of People Strategies and Policy Group (PSPG) and Human Resources Shared Services Program (HRSS) to better inform the development, alignment and delivery of Defence health policy.
12.2.5 Information Technology limitations Defence, like many large organisations, has a complex IT platform underpinning and supporting its operations. In many instances the available corporate systems have not been/ not been able to be configured to maximise usability and provide users with the information they require to make informed decisions. As a result, many smaller, non-corporately supported, but business critical, systems have been developed.
Generally, these systems do not interface with other systems, have been developed by people who have since moved on, are not maintained and are not audited to ensure they are returning the correct information to users. The necessary information in these systems should be capable of being accessed whilst on Operations and this is not always the case.
Other technology issues include:
• The absence of an effective system (including interface/ mechanism as well as procedures and conditions for information/ data exchange – including Privacy considerations) to transfer information and data between Agencies.
• User and business requirements gathering for JeHDI: Many of the stakeholders visited during the review were unaware of the aims and functionality of the JeHDI project and have not provided any input into the requirement gathering and specification phase of this project.
• Absence of workflow capability to support/ guide/ inform users of the IT systems.
• Limitation of IT systems to support Defence personnel in performing their duties. This includes the limited availability of key performance metrics and information not available to make informed decisions.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• Information is generally not able to be presented/ filtered based on an individual's need to know. For instance, medical-in-confidence information may not always be separated out before a member’s situation is discussed at Welfare Boards, weekly case conferences etc.
• Difficulty extracting required OHS information from OHSCAR – Stakeholders reported that they have to request information - it does not appear to be readily available or pushed out to them. The (perceived) time taken to request this data actually prevents users from requesting it and as a result, other systems are developed and utilised for this purpose – i.e. DIPP being utilised by Kapooka for OHS and Safety statistics. Note: this may be a user education/ training issue.
• PMKeyS does not track MECRB dates which limits the ability of COs to keep on top of the MECRB process.
12.2.5.1 Recommendations
REC 4.1 – It is recommended Defence utilise information technology to better support injured or ill members. Required information is available on a need to know basis to support effective information exchange, management reporting and enable informed decision-making. Workflow functionality is utilised to educate, guide and encourage compliance from service providers. An audit trail of activity is maintained.
REC 4.2 – It is recommended that a requirements team of subject matter experts is formed to develop and feed SIIP requirements into the JeHDI and JP2080 projects.
12.2.6 Expectation management A number of stakeholders identified the management of expectations (often unrealistic and inconsistent with the mandate of the service provider) as a significant issue for them. Situations include:
• Separated members attempting to reach back into the Defence system when they now should be relying on the public system for their health needs;
• Expectation that services an injured or ill member who has medically separated should exceed those services available to the general community; and
• Member support networks not aware of the services DCO can provide.
176
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
12.2.6.1 Recommendations
REC 3.1 – It is recommended Defence investigates content/ knowledge management solutions to support the effective management of information.
REC 2.6 – It is recommended DGPERS Air Force and DG Navy People implement a individual member ‘welfare board’ equivalent within their Service for seriously ill or injured members.
REC 3.2 – It is recommended Defence investigates a technology solution to “push” personalised information to an injured or ill member (and/ or family) based on information.
REC 6.5 – It is recommended Defence and DVA (through the DLSC) agree to accelerate and leverage the co-location of injured or ill member support services.
REC 8.1 – It is recommended the Program Manager assigned in REC 1.2 oversee the development of a comprehensive and interrelated roles and responsibilities framework. This must include the functions each role performs and handoffs between roles.
Could engagement with the member’s family be enhanced at the recruitment and orientation stages so a family is aware of the services that could be available to them in the event the member becomes ill or injured?
12.2.7 Administrative versus Medical separation A member can separate as either a medical or administrative discharge. In many cases the facts are clear as to whether the separation should be on administrative or medical grounds. In many cases, however, there can be administrative and medical factors contributing to the separation. Medical conditions may cause, contribute or exacerbate administrative grounds for separation or vice versa.
The identified gaps include:
• Two modes only for discharge – medical or administrative; and
• Guidance is not available to MOs and COs on the appropriate mode of discharge for members who have contributory medical and administrative factors.
This result in the some members separating on for administrative grounds (and the underlying suspicion of some stakeholders that this is the preferred option as it is a more expedient process) when they should, in the opinion of their MO, be separating on medical grounds. It is noted that the support (including DVA and ComSuper entitlements) a member received when medically separating is generally greater than those received by a member who separates administratively.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
12.2.7.1 Recommendations
REC 9.1 - It is recommended that Defence Instructions be reviewed to consider circumstances where a member has health and administrative reasons for separation.
REC 9.2 - It is recommended the Interdepartmental Working Group (IWG) address the interpretation and application of legislation relating to trainees medically separating with a MEC 3 classification (MUFS).
12.2.8 Medical Employment Classification Review Board (MECRB) The MECRB is the process used to consider a member’s suitability for continued service and employment in the ADF based on the member’s medical condition. Triggers for entry into the MECRB process include:
• MO classifies member as MEC4.
• Member has been classified as MEC 301 or MEC 302 for greater than 12 months.
• Member has been classified as MEC 304 for greater than six months.
• Member has been classified MEC 205 for greater than 24 months.
Following on of the abovementioned triggers, the Unit RAP/SMO/MO will collect all relevant paperwork, including the Member’s Health Statement (MHS), Workplace Disability Report (WDR) and Member Consent to Release Medical Information (PM543) and forward this to the DMM with Central Medical Employment Classification Review (CMECR) documentation.
MSU review the member's medical documentation and provides the members Service MECRB with a written MECRB record summary. This summary looks at the member's medical history and details the member's health care requirements, prognosis and the effect of the member's medical condition on their ability to carry out primary and general service duties. The MSU summary provides medical guidance to the MECRB when considering the member's medical condition/s.
The MECRB assesses a member’s suitability for continued service within the limitations of their medical condition and makes a determination based on the material before them.
Outcomes range from reclassification of the member to another MEC class, reallocation to another Unit and/or trade if medically fit for that ECN, or granting of a waiver for a specific timeframe if it is deemed the member possesses a skill (skills waiver - SW) and their medical limitations can be managed in the short term. Where the continued service is not in the medical interests of the member, the MECRB will determine that the soldier is MEC 40X and state that
178
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
there is evidence present for a Termination Notice (TN) under DPR 87(1)(c) as 'Medically Unfit'.
The president of the MECRB advises the member's CO in writing of the decision, including any waivers, restrictions or upgrades to the member's MEC.
The member is to sign and return the acknowledgement form to the MECRB through their relevant Career Management Agency (CMA).
If the decision is that the member is non-deployable and non-employable (MEC 40X), the CMA will issue the member with a Termination Notice (TN). At this point in time the member is encouraged to contact their local DVA Transition Management Service (TMS) representative for advice regarding their discharge entitlements, regardless of whether they are contesting their TN.
A member then has 28 days to contest the TN by compiling a statement of reasons (SOR).
Once a member has acknowledged the TN and returned it back to the CMA the TN is then considered by the CMA Delegate. If it is determined that the member's service is to be terminated, a discharge date is set and CMA will forward the Decision letter and a Statement of Reasons (SOR) explaining how the Delegate came to his/her decision to the member's CO. At this stage, the member is required to sign the acknowledgment form stating a preferred date of discharge, not longer than three months. The member is also encouraged to have a Separation Health Exam (SHE) as soon as possible after a discharge date has been set.
A member can request an extension to the discharge date on medical grounds by submitting, in writing, a formal request to the delegate for consideration. A member's discharge will not be postponed due to the requirement of post-separation health care that is not of a critical nature. If the member sustains an injury that requires treatment, which will not be completed prior to the discharge date, the SHO should grant post-separation health care when confirming the SHE. This is to be recorded on the PM532 SHE and arrangements made to facilitate the required medical management, post-separation.
Defence has a responsibility to assess a member’s level of fitness at discharge.
Considerations for extension to the discharge date can be where:
• The requested medical procedure is of a critical nature and not a procedure that can occur post separation.
• The medical procedure is supported by the member's treating MO (preferably a Specialist).
• Appropriate claims for compensation been submitted, the member been pro-active in submitting the claims in a timely manner but an acceptance of liability has not occurred.
• Where information about a member's medical condition was not known and therefore not considered at the MECRB.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• The extension will provide a reasonable time to allow for post operation rehabilitation.
In the case where a member submits a SOR and it is unsuccessful, they may elect in accordance with DI(G) PERS 34-1 to submit a Redress of Grievance (ROG) to their CO. The processing of ROGs is not to interfere with a member continuing their discharge administration.
Each Service has its own Board. The following table shows MERCB volumes for FY09/10 – by Service.
MECR Boards during FY 09/10
Total members considered by Board
Average No. members per Board
DOCM 10 215 22
SCMA 11 866 79
DSCM All out of session
DNOP 8 96 12
RAAF 14 245 17 Table 26 MECRBs by Service for FY 09/10
Where:
• DOCM – Directorate of Officer Career Management (Army).
• SCMA – Soldier Career Management Agency (Army).
• DSCM – Directorate of Sailor’s Career Management (now amalgamated with DNOP into the Navy People Career Management Agency (NPCMA)).
• DNOP – Directorate of Navy Officers – Postings.
References for the MECRB process include:
• DI(A) PERS 116-5 Separation of Regular Army Soldiers, Army Reserves Soldiers and Soldiers on full-time service – Policy and Procedures.
• DI(A) PERS 124-29 Medical Employment Classification System in the Australian Army.
• DI(A) PERS 159-1 PULHEEMS Employment Standards.
• DI(G) Admin 60-1 Australian Defence Force Separation Administration Procedures.
180
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• DI(G) PERS 16-1 Health Care of the Australian Defence Force Personnel.
• DI(G) PERS 16-15 Australian Defence Force Medical Employment Classification System.
It is noted that modified MECR processes are generally utilised for Trainees/IET/Recruits. For instance:
“A training Authority may consider a recruit/IET unsuitable for training because of employment restrictions arising from a medical condition such that the member is unlikely to be able to recommence training within four months, but may be able to attain MEC 1 or 2 status within 12 months. In this case a UMECR is to be conducted, confirming the member as MEC 3. The member may then be discharged in accordance with section 87(1)(d) of the Defence (Personnel) Regulations 2002 without referral to the MECRB.”162
Likewise:
“Due to the nature of training, circumstances occur where a recruit suffers an injury or illness that will require extended treatment and Rehabilitation. Ref B dictates. “if during recruit training a recruit falls below the medical standard required to continue training, they are to be reviewed by Commanding Officer (CO)/ Chief of Staff (COFS) through the MECRB to determine their medical status for continued service.”163
During the field analysis phase of the SIIP project the efficiency of the MECRB process was raised in multiple locations as a significant issue with the current Defence system supporting injured or ill members. Timeliness and Communication were the key pressure points.
In relation to timeliness – stakeholders were concerned with the timeliness of the process and specifically the time taken to:
• Have a member complete and return their Member’s Health Statement (MHS) in a timely manner (member may be away from Unit) or have a Unit complete and return the Workplace Disability Report (WDR) in a timely manner.
• Have a summary prepared by the MS-DMM – upwards of two weeks was mentioned as a quick turnaround. Turnaround is dependant on resource availability and existing workloads.
• The time taken between notification that a member’s case is being considered by the MECRB and the actual date of the MECRB. The review team saw evidence where a signal came out on 16 September 2010 advising that the member was panelled for a MECRB on 21
September 2010 – less than 3 working days.
162 Australian Navy Systems Command Minute – Termination on Medical Grounds – Recruit/Seaman* Medical Management CAPT P.G. LAVER 20 Dec 05 163 Kapooka Health Centre Minute MAJ L.M. RAE – OC Kapooka Health Centre 12 Oct 2010
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• The time taken for a member’s situation to be scheduled to come before the MECRB.
• The time taken for MEC upgrade requests to be considered and determined by the MECRB – noting this may result in a member who could (if their MEC had been considered and upgraded) be deployed from being deployed.
• The time taken for the outcome of the MECRB to be communicated to COs and through them communication of the outcome to the member (noting there are two delay points here – MECRB to CO and then CO to member).
• The infrequency of the MECRBs and that there is a significant break in MECRB meeting schedule over the Christmas period (3 months).
Statistics which support stakeholder feedback on communications and timeliness follow:
MSU actioned duration – the time taken from receipt at MS-DMM, collection of information, preparation of a MS-DMM medical summary for MECRB and forwarding to the appropriate personnel agency.
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
To MECRB Duration – the time between MS medical summary being provided to the MECRB by MS-DMM and the member being panelled for a MECRB (noting a MECRB may occur in the interim for which members are not panelled).
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
In some circumstances, the member (not wanting to be medically discharged) and their MO (feeling that member would benefit from remaining in the system for a longer duration) are more than happy for the process to take as long as possible (possible creative inactivity).
From a communications perspective – stakeholders advised of the following concerns:
• The quality of information submitted to the MECRB for consideration. The Workplace Assessment forms often explain the member’s current limitations only rather than address the member’s potential/ future expected performance.
• Members not understanding the MECRB process including understanding/ acknowledging that a possible result from the MECRB could be medical discharge from Defence
• Members not being aware their case was before the MECRB. Noting the member involvement required in the process, the SIIP Review Team considers this is an unlikely situation and believes it is more the case that a member chooses not to believe they could be medically discharged
• Members only being aware of the outcome of MECRB when they received a termination notice. Noting a member must sign an acknowledgement form and return it to their CMA before a termination notice is issued, it is questioned whether this is in fact the case.
• Entities providing support to members not being informed in a timely manner of the outcome and therefore not being in a position to effectively support and guide the member during this time.
Consequences of this include:
• Members feel they failed/ unsupported by Defence due to the time this process takes. This is especially so when a member is ready for and wants to be medically discharged.
184
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• A member feeling their life is being put on hold whilst waiting for a determination.
• Members exhibiting recalcitrant behaviour during the wait, causing downstream administrative/ disciplinary issues.
• The delay is exacerbating underlying mental issues of some members.
• The circumventing of the MECRB process – possible temporary upgrade to MEC classification and subsequent (almost immediate) downgrade so as not to trigger the 12 month MEC 301/ 302 process
• Members choosing to separate at own request rather than wait for medical discharge (possible loss of entitlements)
• Opportunity cost – from an ADFRP perspective of members remaining on the rehabilitation program whilst awaiting a determination from the MECRB. We were also made aware of instances where member’s rehabilitation program was assessed and concluded ahead of a MECRB determination.
Possible solutions to address this issue include:
• MECRBs to meet more frequently to clear backlog (issue of availability of skilled resources to sit on the Review Boards)
• Regional tri-service MECRBs (perhaps aligned to area health regions) – with awareness/ visibility of service level critical skills and resource shortages.
• MECRB lite process (perhaps out of session approvals) – where extended rehabilitation required, chronic psychotic conditions etc
• MECRBs to establish service level agreements regarding determinations (performance metrics and criteria)
• HD236 guidance on compiling MHS and WDR to be enhanced.
12.2.8.1 Recommendations
REC 6.1 - It is recommended CJHLTH defines and establishes performance metrics for the MECRB process areas within Joint Health Command control. It is recommended that the Services (including their personnel management agencies) define and establish performance metrics for the MECRB process areas within their influence and control.
REC 6.2 - It is recommended CJHLTH initiate a review of the resourcing requirements for the MECRB process to ensure it is adequately resourced to achieve defined performance metrics
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
and provides greater transparency to people administering the MECRB process as well as members awaiting a determination
12.2.9 Liability determination/ claims processing
• Perception that submitting a DVA claim will affect career progression.
• A service level turnaround of 120 days, from receipt of all required information, is not timely and efficient.
• Length of time taken for liability determination and claims processing to occur is not timely and efficient. Army recruit process allows for approx 3 month turnaround where member still being supported. Experience is that process is taking longer than this - even when evidence of injury, supporting documentation etc suggests it is a clear case where liability should be accepted. At Kapooka – the trainee member remains in Weary Dunlop platoon until their issue is sorted. It is questioned whether this is the most appropriate location for the member (who will shortly be separating)?
12.2.9.1 Recommendations
REC 6.3 – It is recommended DVA and Defence establish mechanisms to improve claims processing times.
REC 8.1 – It is recommended the Program Manager assigned in REC 1.2 oversee the development of a comprehensive and interrelated roles and responsibilities framework. This must include the functions each role performs and handoffs between roles.
REC 8.3 – It is recommended that Defence, following classification of a member as MEC 3, advises DVA of the circumstances surrounding the classification – to enable DVA to commence liability determination. Processes and the mechanism for automated information exchange must be agreed between Defence and DVA.
REC 2.4 - It is recommended Defence and DVA develop processes and procedures that enable Defence to advise DVA of higher priority claims for liability processing and determination. Agreed service levels and benchmark processing times for these higher priority claims should be developed as part of this recommendation.
REC 2.5 - It is recommended that DVA pursue the development of processes that simplify the acceptance of liability under MRCA/SRCA/VEA.
186
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
12.2.10 Trainees – medically separating with a MEC 3 classification A reference to a “trainee” in this section includes a Recruit, Initial employment Training (IET) and Officer Trainees.
MEC 3. Members who have medical conditions that make them medically unfit for duties in their occupation in a deployed or seagoing environment. The member so classified should be medically managed towards recovery and should be receiving active medical management with the intention of regaining MEC 1 or 2 within 12 months of allocation of MEC 3. After a maximum of 12 months their MEC is to be reviewed. If still medically unfit for military duties in any operational environment, they are to be downgraded to MEC 4 or, if appropriate, referred to a Medical Employment Classification Review Board (MECRB) for consideration of an extension to remain MEC 3.164
MEC 4. Members who are medically unfit for deployment or seagoing service in the long-term. Members who are classified as MEC 4 for their military occupation will be subject to review and confirmation of their classification by a MECRB.
165
If a training establishment considers a recruit/IET/officer trainee unsuitable for training due to medical reasons, then that member should be downgraded to a more appropriate MEC and may be medically discharged under the most relevant regulation in accordance with the Defence Personnel Regulations (2002). The Discharge Authority may decide to discharge the trainee (enlisted members) as a medical discharge in accordance with Defence Personnel Regulation 87(1)(d) if they are MEC 3, without being referred to a MECRB, as they are no longer suitable for training in their engaged employment. This will ensure these members receive the same entitlements as a member who is medically discharged when they are classified MEC 4 even though as MEC 3 they may technically recover within 12 months.
166
“20.8.3 Entitlement immediately following medical (MEC 4) discharge
On the basis of the loss of Commonwealth employment due to the involuntary medical discharge, it is RCG policy to accept the Medical Board recommendation for MUFS discharge as certification of up to four weeks incapacity, from the date of discharge.
However this ‘default’ authorisation of payment does not, of course, extend beyond the start-date of any civilian employment commenced during that same four week period.
Important note: Following this four week period of grace, all RCG clients must – if payments are to continue – produce further medical certificates from civilian doctors, to demonstrate continuing incapacity for civilian employment.”167
“6.5.11.2 Entitlement immediately following medical (MEC 4) discharge
On the basis of the loss of Commonwealth employment due to the involuntary medical discharge, it is policy to accept the MECRB decision for medical discharge (that is
164 DI(G)PERS 16-15 Amdt 2 – Australian Defence Force Medical Employment Classification System – page 3 165 DI(G)PERS 16-15 Amdt 2 – Australian Defence Force Medical Employment Classification System – page 3 166 DI(G)PERS 16-15 Amdt 2 – Australian Defence Force Medical Employment Classification System – page 6 167 SRCA Incapacitation 20.8.3
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
related to an accepted service injury or disease) as medical certification of up to four weeks incapacity, from the date of discharge. However this ‘default’ authorisation of payment does not of course, extend beyond the start-date of any civilian employment commenced during that same four week period.
Important note: Following this four week period, the person must, if payments are to continue, produce further medical certificates from their treating doctors, to demonstrate continuing incapacity for civilian work”168
DVA relies on the MEC classification and the condition that lead to that classification to determine if legislative support exists to support a decision that a person is incapacitated for service because of an accepted condition under MRCA or SRCA. If a member separates and is unable to directly commence civilian employment, DVA can determine that the member is also incapacitated for civilian employment.
DVA has a policy that 4 weeks is a reasonable period of time for a medically separating member to relocate/ resettle, find a GP and obtain medical certification of capacity for work and/or engage with DVA and arrange a rehabilitation program. As a result, members separating at MEC4 are entitled to an automatic 4 weeks of incapacity payments.
If Defence did not continue to use MEC information on the termination paperwork, DVA would have to request from each separating member certification from the date of separation. As the member may not have visited a civilian MO this certificate would likely be requested from a Defence MO – thereby duplicating some of the MEC process and paperwork.
This results in issues where DVA interprets that trainees being separated with a MEC 3 classification are not being medically separated/ discharged. This appears contrary to the intent of DI(G)PERS 16-15 Amdt 2 – Australian Defence Force Medical Employment Classification System – page 6 (reproduced above). This impacts the entitlements the medically separated trainee receives:
• DVA does not consider a member's medical classification when determining liability, however MEC rating does impact on access to DVA benefits following discharge. Medically separating as a MEC3 doesn't exclude trainees from receiving entitlements, it just means that they have to prove more and jump through more hoops to access the same entitlements as a member who separates as MEC 4.
• Discharge classifications and access to ComSuper benefits have an interrelationship with DVA benefits. The calculation of incapacity payments are affected by ComSuper payments resulting in offsetting implications.
Note: this issue will still exist after changes to the MEC system wherever a trainee medically separates at MEC 3.
Some injuries will result in a trainee being discharged as MEC4. In other instances where the trainee sustains an injury that interferes with their training, but from which the trainee is
168 MRCA Incapacitation Chapter 6.5.11.2
188
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
expected to recover and would likely be invited to rejoin training – the trainee will generally not be discharged MEC4 but should be eligible for payment without immediate certification.169
DVA relies on the MEC rating as ADF confirmation that a client has been medically discharged. Where a trainee medically separates as MEC3, DVA would not automatically consider the member medically discharged (as MEC 3 is, in this sense viewed as ‘Rehabilitation’) and therefore not provide the first 4 weeks of any incapacity payments without a medical certificate for any compensable condition. This disadvantages trainees who are medically discharged as MEC3
In the absence of detailed information about the reason for their classification it is difficult for DVA to assess their needs and eligibility.
Whilst not a direct effect on DVA services, discharge classifications and access to ComSuper benefits have an interaction with DVA benefits. For instance, the calculation of incapacity payments is affected by ComSuper and the calculation of MRCA SRDP payments is required to offset ComSuper payment.
12.2.10.1 Recommendations
REC 9.2 - It is recommended the Interdepartmental Working Group (IWG) address the interpretation and application of legislation relating to trainees medically separating with a MEC 3 classification (MUFS).
Resolution must include MECRB guidance as to the appropriate MEC classification for Trainees who separate medically from the ADF.
It is noted that the introduction of new MEC classifications, as referred to in 9.1.3 and Appendix J, will necessitate a review and amendment of relevant legislation including:
• MRCA Chapter 6.5.11.2
• SRCA Section 20.8.3
Note: the MEC Project is aware of this issue and is in the process of addressing this – the proposed solution is that if the words “medically unfit” appear in the discharge documentation the trainee will be medically separated
12.2.11 Absence of framework for Command focus groups/ case conferences As discussed in 12.1, local focus groups/ case conferences are a prime local communication tool utilised to inform Command of the status of, and actions required, regarding their members. These meetings are an important tool which informs Command, and relevant stakeholders, about the status of their members. 169 SRCA Policy 20.8.5, MRCA Policy 6.5.11.3 or Defcare commentary – Discharge as untrainable
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
There is inconsistency in the frequency, expected outcomes and participants attending these meetings by location and Service. The success of these meetings as a communication and planning tool is often dependant on the command skills of the person chairing these meetings.
12.2.11.1 Recommendations
REC 9.3 - It is recommended the three Service DGPERS collectively adopt an outcomes based framework which guides COs in the conduct of command focus groups. There should be sufficient flexibility in the framework to ensure its applicability to each Service (size, location, primary function) and in Tri-Service situations.
12.2.12 Health policy development and distribution “Policy” in this section includes Defence Instructions (DI) and Health Directives (HD).
Many stakeholders expressed concern over how:
• Health policy is developed in Defence – including stakeholder consultation;
• Health policy is communicated to stakeholders once it has been endorsed; and
• Defence ensures stakeholders are aware of, and educated in the implementation of the new health policy.
Identified issues include:
• There are many policy documents which relate to support for injured or ill members. Stakeholders raised current workloads and the inability for them to keep abreast of health policy and instructions (some policy documents exceed 50 pages) in addition to successfully fulfilling all other elements of their role.
• There is no overarching document/ user guide which maps how all the individual health policies interact with each other.
• Health policy is often confusing, conflicting or difficult to understand. Limited effort appears to be directed to plain English expression of the health policy. Examples include confusion over HD290 - ability for MOs to use their discretion, ease of understanding this if non-medical CO, confusion regarding interaction with HD289 (pharmaceutical exclusions), people being aware of its existence and what their responsibilities are under it
• Key stakeholders do not feel they are always adequately consulted during the development of health policy. As a result, the stakeholder may choose to disengage from the policy
190
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
direction – the example most commonly mentioned during the field analysis was MOs not referring a member into the ADFRP as they did not were not consulted with during its development and did not agree with elements of it.
• Existing health policies do not always appear to be updated/ amended in a timely manner to reflect changes and additions to health policy.
12.2.12.1 Recommendations
REC 7.1 – It is recommended that all areas responsible for the development of health related policy (including CJHLTH, the single Services and Transitions Support) leverage the policy development and reform activity in the Personnel Policy and Employment (PPEC) Branch of People Strategies and Policy Group (PSPG) and Human Resources Shared Services Program (HRSS) to better inform the development, alignment and delivery of Defence health policy.
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
12.3 Gaps and issues identified - not within scope of the SIIP Review Following is a listing of gaps and issues identified and expressed by stakeholders during the SIIP Review field analysis phase which are not within scope of the SIIP review.
These issues have been documented to provide visibility of stakeholder concerns.
The SIIP Working Group has determined who the issue should be referred to for further investigation and action and advise as follows:
• Defence Health system's ability to cope with increasing incidence of PTSD – is the system geared up to support the increasing presentation of PTSD amongst Defence members? Refer to : Director General Mental Health, Psychology and Rehabilitation (David Morton)
• Concern about the safety of Defence service providers including members, permanent and contracted staff (immediate as well as emotional/ long term) in dealing with members with significant mental health issues. Some stakeholders reported dealing with members who were very angry, verbally abusive, threatening of self harm as well as harm to others etc and enquiring as to the support mechanisms Defence has in place to support these service providers. Refer to : Director General Garrison Health Operations (AIRCDRE Tracy Smart) – service delivery and Director General Mental Health, Psychology and Rehabilitation (David Morton) – policy and governance
• Defence providing health/medical/counselling services to the member only170 It was noted from many of the MOs that participated in the review that it would be beneficial for the member’s treatment
• Concern from some COs that managing members on extended rehabilitation within the Defence environment results in the transference of stress within the workplace. Refer to : Director General Mental Health, Psychology and Rehabilitation (David Morton) – education, tools and addressing stigma associated with mental health issues and Command – investigate underlying issues
if Defence could provide required counselling services to the member’s family. An example is a member returning from Operations with PTSD Refer to : Director General Mental Health, Psychology and Rehabilitation (David Morton) and Director General Defence Community Organisation (Michael Callan)
• Continuum of member support during Operations/ Training exercises and over public holidays and the Christmas break – These issues do not “go away” during Operations and holidays but service provider numbers/ availability declines. An example provided to the Review team was during EX HAMIL where the majority of Lavarack Barracks psychologists were assigned to this operation. Whilst approx 80% of the available workforce was also on this operation this ignored the fact that many of those members who
170 DI(G)PERS 16-1 Health Care of the Australian Defence Force Personnel
192
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
were unable to deploy were major users of the psychology services. Refer to : Director General Garrison Health Operations (AIRCDRE Tracy Smart)
• High dependency members with mental health issues being treated/ housed at Balmoral Naval Ward. A CO questioned whether this is an appropriate mental health facility for this situation and was concerned that the presence of these members and their significant needs reduces the support and services available to other members being treated at this facility. Refer to : Director General Garrison Health Operations (AIRCDRE Tracy Smart) with advice from Director General Mental Health, Psychology and Rehabilitation (David Morton) - addressing stigma associated with mental health issues
• Process for obtaining a waiver for operational deployment and/or training - multiple signatures (including non-medical) required and everyone signing the waiver must be in agreement that the waiver should be issued - example where in excess of 10 signatures were required for a waiver Refer to : HQ JOC and Functional Command
• Class VIII supply chain issues (Medical, dental and pharmaceutical equipment and supplies) – including the time taken for a Unit to receive required Class VIII items; the time taken to repair broken medical equipment within the current medical equipment repair process; the cost benefit of sending a member outside Defence for medical services which could be provided within Defence if equipment was available (the Review team were provided with examples where broken hearing test equipment and skin cancer removal equipment resulted in Defence members receiving these services from external healthcare providers –at significantly greater cost to Defence and inconvenience to the member); absence of fleet management system for medical equipment resulting in old/out dated equipment still being in service. Request for ability to re-instigate local purchase accounts. Why is Class VIII supply treated separately from the regular supply chain? Procurement prioritisation of operational needs over medical needs - example of Gunner being short a back up rifle whilst on operations being given priority (1) over member with medical needs receiving required pharmaceutical/ medical items in a timely manner (priority 4). Refer to: Director General Future Health Capability (CDRE Robyn Walker) and Joint Logistics Command (JLC).
• Recruits enlisting with un-declared pre-existing medical conditions and the resource drain this places on the medical system in “proving” this and then processing (discharge/ administration/ liability determination). Refer to : Defence Force Recruiting
• Road Safety Program – some stakeholders thought this was a worthwhile investment in injury prevention/ training and felt consideration to again providing this course should occur. Refer to : Director General Occupational Health and Safety Branch (Lindsay Kranz)
• Stakeholders confirmed that “near-misses” were generally not reported through AC563s Refer to : Director General Occupational Health and Safety Branch (Lindsay Kranz)
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• Concern from some ex-service organisations that the more junior members of Defence did not see benefit in involving themselves in ESOs once they separate from Defence and the potential ability this might have on the capacity of ESOs to continue to provide services to members.
• High proportion of “no plan required” rehabilitation outcomes – does this suggest further work may be required to refine triggers for entry to rehabilitation or is this an acceptable level noting the elapsed time to provide rehabilitation and that rehabilitation plans may be developed during the initial consultation with the member? Refer to : Director General Mental Health, Psychology and Rehabilitation (David Morton)
• There is a low % of Rehabilitation Goal 2 outcomes - fit for alternative duty (1.8%) which should be investigated further. Does more effort need to be addressed towards inter-service transfers or re-education that full recovery or medical separation is not the only options? Refer to : Director General Mental Health, Psychology and Rehabilitation (David Morton))
• Opportunity cost for patient care if MOs/Psychs required to travel to, and attend many Welfare Boards. Does the authority exist to request a contracted MO to attend multiple welfare Boards when their contract for service is based on patient contact hours? Can teleconference facilities be utilised? Refer to : Director General Garrison Health Operations (AIRCDRE Tracy Smart)
• Provision of resources (paper, photocopier, scanner, supervision) to facilitate copying of health documents (including UMR and CMR) required to support a member’s claim for liability determination. Director General Defence Community Organisation (Michael Callan) – SAM and Director General Garrison Health Operations (AIRCDRE Tracy Smart)
194
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
A Engagement Terms of Reference
TERMS OF REFERENCE ADF SUPPORT FOR INJURED OR ILL PROJECT (SIIP) REVIEW
Background: The areas of rehabilitation, compensation and transition continue to be the subject of extensive attention within Defence with a view to developing a seamless and integrated support service for injured and ill ADF members. There has been a number of process mapping exercises that have defined the range of services available and how they relate to each other. Most recently these exercises have focused on a developing area of concern, that is, the service responsibility boundaries between Defence and the Department of Veterans’ Affairs (DVA) with regard to medical separations. The issues have also been raised in the context of the Review of Military Compensation Arrangements and in the agenda of the Defence/DVA Links Steering Committee, the latter focusing on the decommissioning of the Transition Management Service. The opportunity to improve the integration and streamlining of services is also supported by the Defence Strategic Reform Program (SRP). Head of People Capability (HPC), Head of Defence Support Operations (HDSO) and Commander Joint Health (CJHLTH) have agreed to conduct a gap analysis against best practice of the elements of service delivery and related policy in the areas of incident reporting, welfare, health care, rehabilitation, compensation and transition. The scoping will be undertaken in a collaborative manner with DVA. Purpose: To develop a seamless and integrated support process for injured or ill ADF members throughout their Service career and in transition from Defence. Terms of Reference:
• To define evidence based best practice that might be applied to the delivery of seamless and integrated support services for injured or ill ADF members.
• To examine and conduct a gap analysis of Defence, single Service and DVA incident reporting, welfare, health care, rehabilitation, compensation and transition policies, processes and services using process maps that Defence and DVA have developed, as well as the previous reviews of these services.
• To be cognisant of the issues arising through the MRCA Review and the Defence/DVA Links Steering Committee (DDLSC) that may inform the seamless and integrated delivery of incident reporting, health care, welfare, rehabilitation, compensation and transition services.
• To be cognisant and inclusive of the services provided by other government agencies, including DVA, and information exchanges between Defence and other government agencies.
196
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• To identify possibilities for any shared services in line with SRP principles.
• To recommend a framework, process map(s) and improvements that will better meet the needs of ADF members and their families, and incorporate commanders’ welfare, personnel management and administrative responsibilities.
• To develop the Implementation Strategy and Plan, Evaluation Plan and Tools, and a Communications Strategy and education/awareness packages for the new framework.
Governance: The governance of the SIIP will include a Project Steering Group and a Working Group. It is expected that recommendations or outcomes requiring a joint Defence/DVA response will be considered for discussion at the DDLSC (JHC to coordinate). Project Steering Group. The steering group members are:
a. Commander Joint Health (CJHLTH);
b. Head People Capability (HPC);
c. Head Defence Support Operations (HDSO);
d. General Manager Services Division, DVA;
e. Director General Navy People (DGNP):
f. Director General Personnel – Army (DGPERS-A);
g. Director General Personnel – Air Force (DGPERS-AF);
h. Director General Mental Health, Psychology and Rehabilitation (DGMHPR);
i. Director General Garrison Health Operations (DGGHO);
j. Director General Defence Community Organisation (DGDCO);
k. Director General Occupational Health and Safety (DGOHS);
l. National Manager Defence Support Services, DVA. Working Group (O6/EL2). The working group members are:
a. Director ADF Rehabilitation Services (DRS);
b. Director Transition Support Services (DTSS);
c. Director Safety and Rehabilitation Policy (DSRP);
d. Director Army Health (DAH);
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
e. Special Projects Officer, DGPERS-AF;
f. Director Navy Health (DNH);
g. Director Defence Clinical Services (DDCS); and
h. Director Defence Links, DVA.
Deliverables and Milestones: The project’s key deliverables and milestones are:
1. The Gap Analysis Report (of current Defence, single Service and DVA incident reporting, welfare, health care, rehabilitation, compensation and transition policies, processes and services compared with evidence based best practice) prepared and approved by the Project’s Steering Group by 18 October 2010;
2. The Future State Framework, Process Map(s) and recommended improvements Report prepared and approved by the Project’s Steering Group by 3 December 2010; and
3. The Implementation Strategy and Plan, Evaluation Plan and Tools, and a Communications Strategy and education/awareness packages for the implementation and evaluation of the new framework prepared and approved by the Project’s Steering Group by 17 December 2010.
Proposed Timeframes:
1. Approval of TOR by the Management Board by 30 Jun 10.
2. Invite single Service and DVA representation by 30 Jun 10.
3. Identification of the consultancy firm to undertake the scoping by 21 Jul 10.
4. Working Group to develop the project plan with milestones by 30 Jun 10.
5. First meeting of the Steering Committee by 23 Jul 10.
6. Consultancy firm to commence on 2 Aug 10.
7. First meeting of the Steering Group by 5 Aug 10.
8. First progress report to DLSC on 6 Sep 10.
198
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
B.1 Occupational Health and Safety – Injury Prevention – Illness Prevention Noting this element of the system is out of scope for the SIIP review, any information that has arisen in the context of the SIIP review has been included. This is not a comprehensive representation of the OH&S function within Defence.
Process Name: OH & S Process Owner:
DG OHS – Mr. Lindsay Kranz
Process Objective: A Defence environment where people work together to improve capability by preventing injury and illness and effectively managing their impact on people, reputation, recruitment and retention
Process Start: Incident/Presentation
Process Steps: Inputs Activities Outputs
• AC563
• OHSIR Signal
• Manual entry of data
• Metrics and performance data
• Feedback
Process End: • Incident recorded
• Metrics recorded and data available for analysis
Related processes: Supplier (inputs) Customer (outputs)
• N/A • N/A
Org. units, stakeholders:
• Occupational Health and Safety Branch
• Army Safety Organisation
• Navy Safety Organisation
• RAAF Safety Organisation
• ComCare
Technology: • OHS-MI (Occupational Health and Safety Branch)
• OHSIR (Navy)
• AIMS (Army)
• DIPP (Army)
Key Process Controls:
• OHSCAR Systems Overview
• DI(G)PERS 14-2
• DI(G)PERS 16-11
• DI(G)PERS 16-15
200
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• Occupational Health and Safety
Org. units, stakeholders:
• ADF Member
• Supervisor/Commander/Manager (WRR)
• Member’s Family
• Defence Community Organisation
• AUSDIL (next of kin, relative or nominated person)
• ComCare (if incident involves a contactor or member of general public)
Technology: • Intranet Web Forms
• PMKeyS – primary emergency contact details
Key Process Controls:
• Defence Force Regulations 1952-58F (1)
• DI(G)PERS 11-1
• DI(G)PERS 11-2
• DI(G)PERS 14-2
• DI(G)PERS 16-1
• DI(G)PERS 16-11
• ABR 6303
• OHSCAR Systems Overview
• Navy Divisional Handbook
• OH&S Act 1991 Table 34 Process: Incident, presentation of injury or illness
B.3 Primary Healthcare/ Treatment Process Name: Primary Healthcare/
Treatment Process Owner:
Process Objective:
ADF members receives necessary/ required primary healthcare and/or treatment for their injury or illness
Process Start: Incident/ Presentation
Process Steps: Inputs Activities Possible outputs
• Incident/ Presentation
• Healthcare/ Treatment
• Change in MEC?
• Determine Liability/ Compensation
• CMECR
202
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• Medical Employment Classification Review Board Air Force
Technology: • MIMI
• HealthKeys
• PMKeyS
• Web forms
Key Process Controls:
• DF Regulations 1952 – 58F(1)
• HD 236
• DI(G)PERS 11-1
• DI(G)PERS 16-1
• DI(G)PERS 16-15
• DI(G)PERS 16-20
• DI(A)PERS 159-1
• DI(AF)OPS 4-8
• Australian Book of Reference 1991 – Royal Australian Navy Health Service Manual Vol 1
Table 35 Process: Primary Healthcare and Treatment
B.4 Rehabilitation Process Name: Rehabilitation Process
Owner: Garrison Health
Process Objective: Goal 1: Fit for duties and rehabilitate to pre-injury status Goal 2: Fit for duties with change in duties/ location/ service Goal 3: Stabilise then transition out of ADF to the civilian environment
Process Start: Primary Healthcare/ Treatment
Process Steps: Inputs Activities Outputs
• Referral from Primary Healthcare/ Treatment
• Rehab Assessment
• Screening
• Member interview
• Rehabilitation Program
• Compensation Claim?
• Change in MEC?
• Metrics / Evaluation
• Closed Rehabilitation Program
204
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• DI(G)PERS 11-1
• DI(G)PERS 16-1
• DI(G)PERS 16-15
• DI(G)PERS 16-20
• DI(G)PERS 16-22
• DI(G)PERS 16-24
• DI(A)PERS 33-11
• DI(G)PERS 36-2
• DI(A)PERS 36-2
• HD236
• HD289
• HD290
• HD291
• HD294
• HD295
• HD919
• MRCA s39
• Privacy Act 1988
• Procedures for Program Case Management in the ADF Rehabilitation Program
Table 36 Process: Rehabilitation
B.5 Determine Liability/ Compensation Process Name: Determine Liability/
Compensation Process Owner:
DVA
Process Objective: To enable a member who has been a compensable injury or illness to have their liability determined and receive their entitlements and compensation
Process Start: Incident/ Presentation, Primary Healthcare/ Treatment, Rehabilitation, Medical Separation, Compensation
Process Steps: Inputs Activities Outputs
• Incident/ Presentation
• Decide to lodge claim
• Lodge claim
• Liability determined
• Appeal
206
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
B.6 Return to ADF Duty (MEC1 and MEC2) Process Name: Return to ADF Duty Process
Owner: Various
Process Objective: Member returns to ADF duty
MEC1: Members who are medically fit for employment in deployable or sea going environments without restriction
MEC2: Members who have medical conditions that require access to various levels of medical support or employment restrictions, however they remain medically fit for duties in their occupation in a deployed or seagoing environment
Process Start: Incident Presentation, Primary Healthcare / Treatment
Process Steps: Inputs Activities Outputs
• Primary Healthcare /
• Determine whether change of duties is
• Return to ADF
208
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
• Separation Notification
Process End: Medical separation from ADF
Related processes: Supplier (inputs) Customer (outputs)
• Determine Liability / Compensation
• Transition Services
• Superannuation
• Rehabilitation
• Determine Liability / Compensation
Org. units, stakeholders:
• ADF Member
• Supervisor / Commander / Manager
• Member’s family
• Department of Veterans’ Affairs
• ADF Health Professionals
• Personnel/ Career Management Agency
• ADF Transition Centre
• Medical Employment Classification Review Board Army
• Medical Employment Classification Review Board Navy
• Medical Employment Classification Review Board Air Force
• ComSuper
Technology:
Key Process Controls:
• DI(G)ADMIN 60-1
• DI(G)PERS 03-4
• DI(G)PERS 16-15
• DI(A)PERS 47-10
• DI(A)PERS 116-5
• DI(G)PERS 124-29
• DI(AF)PERS 07-3
• Defence Force Regulations 2002
• HD236
• HD284
• MRCA
210
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Table 39 Process: Medical separation
B.8 Transition Services Process Name: Transition Services Process
Owner: Defence Transition Services
Process Objective: Reasonable assistance and support provided to ADF member to ensure a smooth transition to civilian life. This includes a smooth transition of case management to DVA (if applicable) and confirmed engagement with members post separation to ensure successful transition
Process Start: Medical Separation, Determine Liability / Compensation
Process Steps: Inputs Activities Outputs
• Lodge Benefits Claim
• M20
• DM42
• TFN?
• Medicare Levy Variation
• Process Payment of benefits
• Separation
Process End: Post Separation Healthcare Services, Superannuation
Related processes: Supplier (inputs) Customer (outputs)
N/A N/A
Org. units, stakeholders:
• ADF member and family
• Defence Support Group
•
• External Health Agencies
• Centrelink
• ComSuper
• DVA
Technology: • ComSuper Databases
Key Process Controls:
N/A
Table 40 Process: Transition
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved.
KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.
B.9 Superannuation Process Name: Superannuation Process
Owner: ComSuper
Process Objective: To determine ill or injured member’s eligibility for superannuation and to initiate timely payment of superannuation entitlements
Process Start: Medical Separation, Determine Liability / Compensation
Process Steps: Inputs Activities Outputs
• Medical Separation
• Determine Liability / Compensation
• Apply for benefits
• Lodge Benefits Claim
• Process payment
• Seek financial advice
• Payment processed
• Member information
Process End: Timely determination of Pension/ correct superannuation entitlements
Related processes: Supplier (inputs) Customer (outputs)
• Medical Separation
• Determine Liability / Compensation
• Determine Liability / Compensation
Org. units, stakeholders:
• ADF Member
• Centrelink
• ComSuper
Technology: • ComSuper Database
Key Process Controls:
• Defence Force Retirement and Death Benefits Act 1973
• Military Superannuation and Benefits Act 1991 Table 41 Process: Superannuation
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Incident/ Presentation
ADF Policy and Directives• OHSCAR Systems Overview • DI(G)PERS 14-2 Organised ADF Sporting
Activity• DI(G)PERS 16-11 Australian Defence
Force Policy on Physical Fitness• DI(G)PERS 16-15 Amdt 2 Australian
Defence Force Medical Employment Classification System - all service personnel are to be employed appropriately according to their MEC
• DI(G)PERS 16-18 Australian Defence Force Policy for Health Promotion Programs
• DI(G)PERS 16-20 Privacy of Health Information in Defence
• SAFETYMAN• ABR 6303 Navy Safety Systems Manual• Defence OHS Strategy
Legislative Obligations• OHS Act 1991 – Duty of care provisions
and responsibilities• Privacy Act 2004
Documentation• AC563 Defence OHS Incident Report
Notes:1: Incident Self Service (ISS) – will enable Defence incidents to be entered via PMKeys. Will replace current AC563 web form – data captured will flow to CRM database and information translated into OHSCAR. Go live expected early 2011
Occupational Health and Safety
OHS-MI
Manual entry of AC563 dataAC563
OHSIR
?? Army
OHSCAR ReportsMonthly
1
CRMOSIRISDefcare
ComCare
OHSIR Signal
Feedback
42
40
40 434241 44
Occupational Health and Safety Branch
RAAF Safety Organisation (?)
Navy Safety Organisation
Army Safety Organisation (?)
40
43
42
41
44
Stakeholders
ComCare
ABCD
213
Incident occurs AC563
NOTICAS
MEDICAS
Return to ADF Duty
Determine Liability/
Compensation
Primary Healthcare/ Treatment
Not always competed
1 2
ADF Policy and Directives• Defence Force Regulations 1952 – 58F(1)
– Authority for provision of healthcare to ADF members
• DI(G)PERS 11-1 Amdt 6 Defence Force sponsored visits to Service members suffering serious illness or injury – The Australians Dangerously Ill Scheme
• DI(G)PERS 11-2 Notification of Service and Non-Australian Defence Force Casualties
• DI(G)PERS 16-1 Healthcare of the Australian Defence Force
• DI(G)PERS 16-11 Australian Defence Force Policy on Physical Fitness. 21.e Commanding Officers are to ensure that all injuries attributable to physical fitness training are investigated and reported in accordance with ADF and Single Service policies
• DI(G)PERS 14-2 Organised ADF Sporting Activity
• ABR 6303 Navy Safety Systems Manual• OHSCAR Systems Overview • Navy Divisional Handbook
Legislative Obligations• Managers and supervisors have a legal
responsibility under section 69 of the OHS Act 1991 to report all OHS incidents in the workplace.
motor vehicles• AD088 ComCover Notification Record –
incidents involving member of public• AD097 ADF Leave Application• NOTICAS – Notification of Casualty• MEDICAS – Notification of Medical
Conditions“Other” forms of notification of incident/ presentation can include:• Statutory declaration• Hospital Admission paperwork• AD097• Remittance Advice – Service Provider• Complaint• Family concern• Clinical Record• Specialist Report• Ambulance Report
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Treatment - initial
Incident/ Presentation
ADF Policy and Directives• Defence Force Regulations 1952 – 58F(1)
– Authority for provision of healthcare to ADF members
• HD 236 – new or reconfirmed MEC and employment restrictions are to be promulgated to members, members’ CO and Supervisor and Personnel/ Career Management Agency
• DI(G)PERS 11-1 Amdt 6 Defence Force sponsored visits to Service members suffering serious illness or injury – The Australians Dangerously Ill Scheme
• DI(G)PERS 16-1 Healthcare of the Australian Defence Force
• DI(G)PERS 16-15 Amdt 2 Australian Defence Force Medical Employment Classification System - Whenever a member presents to a health facility or is hospitalised, health service personnel must assess the appropriateness of a member’s existing MEC. MOs must initiate or cause to be initiated timely MECR actions
• DI(G)PERS 16-20 Privacy of Health Information in Defence
Members are to be assessed for medical fitness for operational deployment ...• Australian Book of Reference 1991 –
Royal Australian Navy Health Services Manual Vol 1, Chapters 7-9
• DI(A)PERS 159-1 PULHEEMS Employment Standards
• DI(AF)OPS4-8 – Individual Readiness
Legislative Obligations• .
Documentation• AD097 ADF Leave Application• AD523 Workplace Disability Record• AD524 Member Health Statement• PM006 Specialist Referral and Report• PM008 Report on a case referred for
Psychiatric or Psychological Examination• PM101 Medical or Dental Fitness Advice• PM518 Medical Employment Classification
Review Record• PM532 Medical Employment Classification
Specific Assessment includes:• Home Assessment• Detailed Workplace Assessment• Activities of Daily Living (ADL)
15 working days
Primary Healthcare/ Treatment
ADF Policy and Directives• Defence Force Regulations 1952 – 58F – Authority for
provision of healthcare to ADF members• HB11/2009 Mental Health Screen for Casework• HD236 – new or reconfirmed MEC and employment
restrictions are to be promulgated to members, members’ CO and Supervisor and Personnel/ Career Management Agency
• HD289 Mental Health Case Management• HD290 Health Procedures for the Delivery of the ADF
Rehabilitation Program• HD291 Management of deliberate self-harm in the
Australian Defence Force for Primary Care Providers• HD294 Suicide Risk Assessment and Management in the
Australian Defence Force for Primary Care Providers• HD295 Mental Health and Psychology Services in Joint
Health Command• HD919 Guidelines on Australian Defence Force Access to
Health Support• DI(G)PERS 11-1 Amdt 6 Defence Force sponsored visits
to Service members suffering serious illness or injury – The Australians Dangerously Ill Scheme
• DI(G)PERS 16-1 Healthcare of the Australian Defence Force
• DI(G)PERS 16-15 Amdt 2 Australian Defence Force Medical Employment Classification System - Whenever a member presents to a health facility or is hospitalised, health service personnel must assess the appropriateness of a member’s existing MEC. MOs must initiate or cause to be initiated timely MECR actions
• DI(G)PERS 16-20 Privacy of Health Information in Defence
• DI(G)PERS 16-22 Australian Defence Force Rehabilitation Program – occupational rehabilitation to ADF members irrespective of whether injury or illness is work related
• DI(G)PERS 16-24 Mental Health Provision in the Australian Defence Force
• DI(A)PERS 33-11 Army Casualty Administration and Support Framework - rehabilitation of members is an essential component of a Unit Commander’s personnel management responsibilities
• DI(G)PERS 36-2 Australian Defence Policy on Individual Readiness
• Procedures for Program Case Management in the ADF Rehabilitation Program 1 Feb 2010
Legislative Obligations• MRCA s39 – 3 x Service Chiefs are responsible for the
rehabilitation ‘Rehabilitation Authority” of their full time serving members
• MRCA s39(3)(b) MRCC (DVA) is Rehabilitation Authority when serving member has been identified as being likely to be discharged for medical reasons, has been medically discharged or person is no longer serving in the forces
• Privacy Act 1988
Documentation• PM101 Medical or Dental Fitness Advice• PM514 Refusal to Submit to Medical or Surgical Treatment• PM532 Medical Employment Classification Advice• PM544 Rehabilitation Program Amendment• PM546 Referral for Rehabilitation Assessment• PM546-4 Rehabilitation Program• PM546-5 Rehabilitation Activity Schedule• PM547 Rehabilitation Closure Report• PM543 Authority to Collect and Release Information
Note: Many trigger points to determine if compensation claims have been lodged – including initial Member interview,
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Primary Healthcare/ Treatment
ADF Policy and Directives• DI(G)PERS 16-15 Amdt 2 Australian
Defence Force Medical Employment Classification System - 37 Cos responsibilities – the member must be advised to make appropriate military compensation and/or Veteran’s entitlements claims with the DVA if the member considers the medical condition attributable to ADF service
• DI(G)PERS 16-20 Privacy of Health Information in Defence
Legislation/ Legislative Obligations• Defence Act 1903• Military Rehabilitation and Compensation
Act 2004 (MRCA) – compensation for injury or illness as a result of service on or after 1 July 2004
• Safety, Rehabilitation and Compensation Act 1988 (SRCA)
• Veterans’ Entitlements Act 1986 (VEA)• Occupational Health and Safety Act 1991
(OHSA)• Privacy Act 1988
Documentation• D2582 Claim for Disability Pension and/or
Application for Increase in Disability Pension
• D2020 Claim for Compensation and Rehabilitation (SCRA)
• D2049 Injuries and Disease Details Sheet (Post Jul 2004)
• D2051 Claim for liability and/ or compensation (MRCA)
• M40 Application for Invalidity Benefits• “Needs Assessment” - Questionnaire
Processes• Single Access Mechanism (SAM)
Compensable entitlements and other benefits may include:• Disability Pension (VEA)• Incapacity Payments (SRCA/ MRCA)• Permanent Impairment payments (SRCA/
MRCA)• Aids and Appliances• Home and workplace alterations• Vehicle modifications• Household assistance and services• Attendant Care services• Clinical treatments and services• Rehabilitation services including medical,
psychosocial and vocational (SRCA/MRCA) and voluntary vocational rehabilitation (VEA)
Determine Liability/ Compensation
Medical Separation
Superannuation
Rehabilitation
Incident/ Presentation
SAM
Process Claim
DRMS
Log and update requests
Lodge Claim Claim Received
CCPS(VEA)
1
Log, Update
Legislation
Further information
(ADF)
Determine Liability
Determine applic. Acts
CompensableEntitlements
If compensable
1Member informedAppeal?
1
1
D2051MRCA
Decide to claim?
CADET(MRCA)
DEFCARE(SRCA)
PMKeyS10
103
10
101010 10
13
AppealsProcessD2582
VEA
D2020SRCA
11
11 20 3110
33 3534
12 36
15 16 171 3 12
Yes
10
10
10
XXXX
Inform Defence(Generic /Specific)
Log claim
13
13
10
XXXX13
Inform Tri-Services
13
Inform Services
13
A N F
Only MRCA and SRCA
D2049
18
NeedsAssessment
Eligibility“Other
Benefits”10
1
“OtherBenefits”
Yes
1
3
Rehabilitation
DocTracker18
1
3
12
36
37
Must advise Defence
Incapacity payments
PIPSPC
IPS
DOLARS
Other payments
10
10
10
10
M40
ABCD
217
ADF Policy and Directives• DI(G)ADMIN 60-1 ADF Separation
early Retirement and Termination of Service in the Australian Defence Force
• DI(G)PERS 16-15 Amdt 2 Australian Defence Force Medical Employment Classification System - COs are to actively manage the employment of their personnel in terms of their MEC, especially during the transition from MEC4 to separation from the ADF
• DI(A)PERS 47-10 Resignation, Retirement and Termination of Service - Officers
• DI(A)PERS 116-5 Amdt 3 Separation of Regular Army Soldiers, Army Reserve soldiers and Soldiers on full time service – Units and transition centres are to ensure that soldiers separate from the Army with a minimum of personal disruption and with recognition that their personal contribution to the Army has been appreciated
• DI(A)PERS 124-29 Medical Employment Classification System in the Australian Army
• DI(AF)PERS 07-3 General discharge/ transfer procedures - PAF
• Defence Force Regulations 2002 – Medical Discharge
• HD236 – Medical Employment Classification System procedures
• HD284 – Medical assessment and dental examination requirements for ADF personnel
Legislative Obligations• Section 64 MRCA – must appoint a
Transition Case Manager
Documentation• AD147 Comprehensive Preventative
Health Examination• DM042 Invalidity Retirement from the
Defence Force Medical Information• PM070 Separation Health Statement• PE071 Discharge or Transfer Certificate• PM387 Authority to release Health
Information• PM515 Request to access Dental Records• PM518 Medical Employment Classification
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
C Contemporary practice examples and case studies This Appendix describes some programs or initiatives identified through the literature review or stakeholder consultation as examples of contemporary practice.
C.1 Transition Mental Health and Family Collaborative (Townsville171
The aim of the Transition Mental Health and Family Collaborative was to improve mental health and family supports provided to medically discharging ADF members and their families. This initiative was developed, implemented and evaluated by the Australian Centre for Posttraumatic Mental Health (ACPMH), in partnership with Defence and DVA.
)
The Collaborative identified 5 change priorities to improve transition mental health and family support practices:
• Engagement: More effective engagement and communication practices.
• Recognition: Better recognition of mental health problems and related issues.
• Families: Improved family sensitive and inclusive practices.
• Interventions: More effective advice, support and treatment.
Ten teams were formed to participate in the collaborative. The interventions that were provided as part of the initiative included the delivery of plenary addresses on the importance of effective transition mental health and family supports; teaching participants content of materials, including the effective practices, measurement strategies, and improvement methods; and the provision of advice and support to participants.
The evaluation of this project reported that it achieved considerable practice improvement in the five priority change areas. It was recognised that the challenge is now to expand this successful initiative across Australia. The following recommendations are suggested:
1 Implement the five transition change priorities. It is recommended that the five change priorities for mental health and family practice improvement developed in the pilot be implemented across all Defence and DVA transition services.
2 Implement affordable practice improvements. Having demonstrated the effectiveness of the approach used in this project under ideal conditions, it is recommended that less resource intensive practice improvement methods are implemented nationally by:
• Identifying local internal leaders with authority and support to implement
• Reducing the amount of face to face training, increase emphasis on a package of simple written guidelines and video modelling of core skills
171 Australian Centre for Posttraumatic Mental Health. Australian Government Mental Health Lifecycle Package: Transition Mental Health and Family Collaborative (Townsville). Final Report. (April 2010)
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
219
• Reducing face to face communication between teams in favour of virtual communication (phone, email, teleconference)
• Maintaining the requirement for demonstrating practice changes over time.
The core elements of building motivation to make practice improvements, learning the required ideas and skills, and monitoring their execution within existing resources and on a sustainable basis must be retained to achieve real practice change.
3 Use objective measures of practice change. It is recommended that the main practice priorities be monitored using common objective measures across sites. These measures were developed and used successfully in the pilot. This process allows for benchmarking across services and builds a common will to change.
4 Joint Defence and DVA leadership of transition improvement efforts. A seamless transition between Defence and DVA is one of the most important challenges in this area. It is recommended that the full range of Defence and DVA funded transition services be included in the implementation of these practice improvements (e.g., health, chaplaincy, rehabilitation, transition, compensation, DCO, VVCS). This will build their identity as a seamless system of transition support services. Implementation of these recommendations should be led jointly by Defence and DVA.
C.2 Headley Court – Defence Military Rehabilitation Centre (DMRC) DMRC aims to return ill or injured Service personnel to duty wherever possible or to civilian vocational activity appropriate to their abilities. It also has a key role in coordinating the care of casualties returning from operations, and is the specialist centre for the rehabilitation of all Service amputees.
Facilities and staffing levels have been developed to provide an intensive rehabilitation program and vocational assessment, which is carried out by a specialist and highly experienced multi-professional team.
The majority of patients treated at Headley Court have sustained orthopaedic injuries, but a whole scope are seen, from amputees to neurological injuries. Most patients are treated at DMRC in three week blocks, however, neuro-patients and those with complex rehabilitation needs are accommodated in the Unit’s hospital ward, may remain for much longer periods.
Also based at DMRC is the Joint Services School of Remedial Instruction. Remedial Instructors are Senior Physical Education Instructors who have completed a six-month residential course at the school in basic medical skills relevant to rehabilitation172
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
C.2.1 Facilities and services There is a rehabilitation staff of around 200 from all three services Medical and Nursing branches, including Princess Mary's Royal Air Force Nursing Service, providing specialist medical officers, nurses, remedial instructors, physiotherapists, occupational therapists (OT), speech and language therapists, a cognitive therapist, social workers, engineers, and administration support staff. Not only does the centre deal with patients with new physical disabilities, but it also deals with patients suffering from post-traumatic stress disorder.
The rehabilitation areas of the unit consist of hydrotherapy pools, gymnasiums, and workshops for prosthetics.
The specialist rehabilitation services on site include:
• Three Force Generation Teams - titled lower limb, upper limb and medical, and spines.
• Complex trauma team headed up by a civilian OT.
• Neurological team headed up by a civilian OT.
• There is a team of professional leads (e.g. senior clinicians that manage their specific discipline).
• Human performance, sports medicine and injury research team x 5 persons.
• PTSD team – staffed by a visiting psychiatrist
• Social workers – manage the link between the military and civilian world and work with families to determine social needs and psychological adjustment needs. Provide a point of contact throughout life of the case.
• Cognitive rehabilitation – part of the neuro rehabilitation services and is delivered by education officer, OT, speech therapist, psychologist and neuropsych support.
• Battle Back – adventure training with the onus on reintegration.
• Complex trauma team – multidisciplinary team meeting to discuss clinical, admin and social management of members.
• Complex trauma physiotherapy and prosthetics.
• Neurological service.
C.2.2 Mission statement “To provide clinical rehabilitation, training and personnel for the operational role and research in order to achieve optimal levels of health and fitness.”
C.2.3 Crest and motto The crest of the DMRC consists of a serpent constricting a sword that runs through a pair of shackles. The shackles represent injury. The sword is breaking the shackles of injury with the
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
221
aid of the medical profession represented by the constricting serpent. The motto "Per Mutos" is Latin for mutual effort that is required to break the shackles of injury
C.2.4 Help for Heroes (H4H) Launch speech “Before I go any further, let me make a couple of points. Firstly, I am not a soldier. I was a Rifleman 22 years ago and I am very proud of it. I have a son who is at Sandhurst and I am very proud of him too, but I am not a soldier. I am a civilian and, as a cartoonist, this is way out of my normal life, so please make allowances for that. If I say soldiers I mean Servicemen and women.
Secondly, this has nothing to do with politics. I’m not concerned about the rights and wrongs of policy. I’m concerned about the impact on the young people who get hurt doing their duty and carrying out that policy. Nor am I criticising what happens to them now by way of treatment. It’s very good, but I just think we can and should do better.
What is Help for Heroes all about? The answer is really very simple; it’s about the blokes. I spent ten years in the army and that was the constant refrain. We were taught at Sandhurst that we were to 'Serve to Lead' and at every level of the services that’s what it is all about; look after the blokes.
Soldiers serve their country; they are Servicemen. They get sent to wars and they fight, that’s their job and they do their job brilliantly. Sometimes they are killed while serving their country and when that happens it is a tragedy and we remember them with pride.
Sometimes they are wounded and when that happens we must care for them. These days our front line treatment and our medics are so good that our soldiers are surviving wounds that they would have died from 10 years ago. Some of those injuries are horrific, many of the wounded are amputees and many are complex trauma cases. Nowadays they don’t die, they survive and we must ensure that they go on to live good fulfilling lives.
These wounded soldiers are our boys and girls,…most of them are the same age as my children, and they are our responsibility. We, the people of Great Britain, are their parents, regardless of what we might think of the wars that they fight. They are just ordinary people who we ask to do extraordinary things; we ask them to risk their lives on our behalf. Which means doing our utmost to support them when things go wrong.
Today is a great day for me – it’s when H4H actually starts doing things instead of talking about doing them. For the last few weeks I’ve lived in a flurry of phone calls, meetings, e-mails, rushing around sorting out admin details. But now - today - H4H actually exists.
I admit it has all been a bit of rush. And it shouldn’t have been possible to do all this and get such an ambitious idea up and running so quickly. The fact that it now exists to me shows how necessary it was and that other people share my feelings. I’ve had incredible offers of help in the last few weeks; we have been given offices, office kit and half a million leaflets. We have volunteers, even General’s wives, manning the telephones and that is just the beginning.
222
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
To the media, I say thank you for the great reception you’ve given our message. Now we need all the newspapers backing this appeal, all the TV and radio companies joining in. We want schools to raise money, we want sports teams, pubs and clubs all doing their bit to support our wounded.
Today is the expression of a widely felt - but so far unstated - feeling that we need to do something. It’s struck a chord deep in the heart of the British people.
In my parents’ generation, normal people got involved in war, horribly in many cases. They were bombed, shot at, torpedoed, invaded, made homeless and went short of food. We all knew the suffering of war. Then after WW1, war became once again a professional activity for a small number of dedicated people, often far from the public's eyes and minds. Iraq & Afghanistan have changed that. Large numbers of British forces have become involved in ferocious struggles far from home and the result has been a steady stream of casualties coming back.
We have all seen them on TV. We may even know some of them. You have to see them in person, I think, to realise that we owe them something. When my wife Emma and I first went up to Selly Oak Hospital, we met courageous young people with awful wounds facing a difficult and uncertain future. But it was their cheerfulness that got to us and determined us to start Help for Heroes. They gave for us, time for us to give for them.
Emma and I accept that we can’t stop people getting hurt but we can do something to help them get better. We think that the vast majority of people in this country feel the same, but do not have a way to express their support for our Servicemen.
That’s where H4H comes in. H4H can become a focus for people to show that they really do care. H4H is an appeal, an appeal to the people of Great Britain to show that they support our wounded servicemen, and to do that by raising a huge amount of money to give them the very best treatment facilities that money can buy.
Let me tell you some of the things we’ll spend the money on. Top of the list is a swimming pool at Headley Court, the marvellous treatment centre which deals with casualties after they come out of hospital. At the moment, they are being put in a minibus and taken to a public swimming pool miles away to do the exercises that are so vital to them regaining their strength. And they have to show their wounds off in public. I think we can do better than that.
Our soldiers should get the best. They give more, risk more, sacrifice more, and they should be given more. We can give them more.
What is H4H all about? It’s about the blokes. It’s about Derek, a rugby player who has lost both his legs, it's about Carl whose jaw is wired up so he has been drinking through a straw. It’s about Richard who was handed a mobile phone as he lay on the stretcher so he could say goodbye to his wife. It is about Ben and it’s about them all. They are just blokes but they are our blokes; they are our heroes. We want to help our heroes.
Ladies and Gentlemen. Please join me in a toast to our heroes…173174
173 Bryn Parry Launch Speech - 30th September 2007
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
223
C.3 Australia Post Australia Post won an award at the SRCC Safety Awards in 2009 for Creating a Nationally Consistent Approach to the Provision of Rehabilitation Management. The following is a description of this system from the SRCC website.
Australia Post has 35,000 employees over three core business areas: delivering letters, handling parcels and operating retail outlets. It operates Australia’s largest transport fleet and retail network.
C.3.1 The problem Australia Post employs both in-house rehabilitation providers and external rehabilitation providers, thus creating a challenge to unify their approach to service delivery so that every employee receives the same level of rehabilitation intervention, regardless of their location. Underlying this was a commitment to providing every employee with an offer of meaningful suitable duties.
It was identified that there were inconsistencies in Australia Post’s approach to rehabilitation management between states and between internal and external rehabilitation providers. While good return to work outcomes were being achieved, Australia Post endeavoured to establish a management system and nationally consistent approach to rehabilitation that would become industry best practice.
C.3.2 The approach In 2006 Australia Post’s Workplace Injury Prevention and Management Unit (WIPM) was formed. This branch brought together each state rehabilitation function under national management. The aim of this initiative was to:
• forge closer working relationships between rehabilitation, workers’ compensation and OHS
• ensure that rehabilitation, workers’ compensation and OHS issues and outcomes are tabled and discussed at a national executive level
• standardise rehabilitation processes and procedures, drawing on the strengths of each state to create a national approach
• ensure that injured workers receive consistent service regardless of location
• create strong working relationships between state rehabilitation managers
• reduce workers’ compensation costs.
C.3.3 The outcome The WIPM Unit is now recognised as a key business unit within Australia Post and in 2007 was awarded an Australia Post National Excellence Award.
224
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Australia Post has achieved impressive results in the areas of return to work, reduction in lost working days and provision costs. Australia Post has exceeded the scheme average in return to work performance from 2005–06 to 2007–08, for the following indicators: employees who returned to work for some period since the injury; employees who returned to work with their original employers; and employees who returned to work to their original duties.
Australia Post’s commitment to best practice rehabilitation is further evidenced by its well developed and constantly evolving management systems.
Australia Post holds a tier 3 licence in prevention, rehabilitation and workers’ compensation, and its commitment to early intervention is evidenced by the fact that in the majority of cases rehabilitation services commence prior to a claim being accepted.
C.3.4 Future plans Due to the success of this initiative, plans for the future are to continue with more of the same. Australia Post will continue to strive to exceed service standards and set an industry benchmark for occupational rehabilitation services. It will further its commitment to ensuring that all injured workers receive the highest level of care and that in all instances suitable duties are provided, thus reducing the human, workplace and financial impact of work related injuries.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
225
D Stakeholder engagement
SIIP Working Group Meetings 9
SIIP Project Steering Group Meetings 5+
Stakeholders consulted 100+
Date Engagement/ Meeting Discussion
20 Dec 2010 SIIP Project Steering Group – 5th meeting
13 Dec 2010 CDRE Grant Ferguson SWIIP Phase 2 Terms of Reference
9 Dec 2010 CDRE Grant Ferguson Implementation Planning – Phase Tow
6 Dec 2010 Director Personnel Systems (Karen Giovinazzo)
3 Dec 2010 SIIP Project Steering Group – 4th meeting Recommendations
3 Dec 2010 CHAP Robert Sutherland Canadian Forces and US Marines
2 Dec 2010 MAJGEN Craig Orme Next steps
25 Nov 2010 9th SIIP Working Group Meeting Member Support function
22 Nov 2010 SIIP Project Steering Group – 1* meeting SIIP Recommendations – impacts and implications
17 Nov 2010 8th SIIP Working Group Meeting
16 Nov 2010 2 CDO Regt – Holsworthy Barracks – various stakeholder meetings including: CO 2 CDO Regt (LTCOL Ian Langford) MAJ Simon Patching 1 x PADRE 2 x PTI 1 x MO 1 x FLO 1 x Psychologist 1 x RSM 1 x ADJT 1 x OC LSC 1 x HRM
226
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
E Glossary and acronyms Acronym Full name Description ACAO Army Casualty Assisting Officer CAS-A ACPMH Australian Centre for Post-traumatic
Mental Health
ACMS Army Capability Management System ADF Australian Defence Force ADFMHS ADF Mental Health Strategy ADFPSP Australian Defence Force Paralympic
Sports Program
ADFRP ADF Rehabilitation Program Developed to ensure Defence meets its duty of care to its members and meets its responsibilities under relevant legislation
ADFTC Australian Defence Force Transition Centre
ADFTSS ADF Transition Support Services ADFTSS is responsible to the Services for the provision of transition management support to members who are undergoing separation from the ADF
ADJT Adjutant ADL Activities of Daily Living Rehabilitation Assessment AFS Average Funded Strength AHA Annual Health Assessment AHQ Army Headquarters AIMS Army Incident Management System AMA Advanced Medical Assistant ANC Australian Navy Cadet APA Army Personnel Agency APCAS Army Physical Conditioning Assessment
System DI(A)PERS 148-2 Army Physical Conditioning Assessment System
APC Australian Paralympic Committee APCD Army Personnel Coordination
Detachment
APPVA Australian Peacekeepers and Peacemakers Veterans Association
ESO
APNRE Army Personnel not related to establishment
APS Australian Public Service ARA Australian Regular Army AREP Alcohol Rehabilitation and Education
Program
ARPANSA Australian Radiation Protection and Statutory Authority
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
231
Acronym Full name Description Nuclear Safety Authority responsible for radiation
issues within the Commonwealth jurisdiction
ASAC Armed Services Assistance Centre ASL All-hours Support Line ATO Australian Taxation Office AToDS Alcohol, Tobacco & Other Drugs ADFMHS AUDIT Alcohol Use Disorder Identification Test ADF Mental Health screen AUSDIL Australians Dangerously Ill System AWB Area Welfare Board BOI Board of Inquiry CA Chief of Army CAS-A Casualty Administration Service - Army CAMECR Central Aircrew Medical Employment
Classification Review
CCLO Compensation Claims Liaison Office CCM Complex Case Management System CCO Complex Case Officer Navy CCPS Compensation Claims Processing System VEA claims management
system CDF Chief of Defence Force CF Canadian Forces CFA Combat Fitness Assessment CFTS Continuous Full Time Service contract CIMHS Critical Incident Mental Health Support ADFMHS CJHLTH Commander Joint Health CMA Career Management Agency Responsible for management,
facilitation and support of alternative career pathways for members on ADFRP Goal 2 Rehabilitation Programs
CMECR Central Medical Employment Classification Review
Conducted when consideration by the MECRB is required
CMVH Centre for Military and Veteran’s Health CMM Defence OHS Capability Maturity Model CO Commanding Officer ComCare Commission for the Safety, Rehabilitation
and Compensation of Commonwealth Employees
CPHE Comprehensive Preventative Health Examination
CRA Compulsory Retirement Age CRTA Compassionate Return to Australia CSW Critical Skills Waiver
232
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Acronym Full name Description CTAS Career Transition Assistance Scheme Provides ADF members with
assistance to facilitate their transition to civilian employment upon separation. Scheme is available to all Permanent and Reserve Force members who have rendered CFTS. Benefits are determined by length of qualifying service
DAH Director Army Health DCO Defence Community Organisation Responsible for delivering
professional social work and support services to Commanders, members and their families
DDOPS Deputy Director Operations DEEWR Department of Education, Employment
and Workplace Relations
DFA Defence Families Australia DFDA Defence Force Disciplinary Act 1982 DFISA Defence Force Income Support
Allowance
DFPO Defence Force Psychology Organisation DFR Defence Force Recruiting DFRDB Defence Force Retirement and Death
Benefits Act 1973
DFWA Defence Force Welfare Association ESO DHOAS Defence Home Ownership Assistance
Scheme
DIO Defence Insurance Office DIPP DISCON Defence Integrated Secure
Communications Network
DISPAY Discharge Pay DMM Directorate of Military Medicine DMO Defence Materiel Organisation DNOP Directorate of Navy Officers - Postings Amalgamated with DSCM
into NPCMA DOCM-A Directorate of Officer Career
Management - Army
DOHSC Defence Occupational Health and Safety Committee
DOHSMS Defence Occupational Health and Safety Management System
DOLARS Departmental On Line Accounting and Reporting Systems
DVA payments system
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
233
Acronym Full name Description DPSYCH Directorate of Psychology DRH Directorate of Relocations and Housing DRMS Document Records Management System DRS Directorate of ADF Rehabilitation
Services
DSCM Directorate of Sailor’s Career Management
Amalgamated with DNOP into NPCMA
DSG Defence Support Group DSH Defence Service Homes DSHI Defence Service Home Insurance DSO Defence Support Operations DSTA Defence School Transition Aide DSW Defence Social Workers DTM Defence Transition Mentor DTSS Directorate of Transition Support
Services
DVA Department of Veterans’ Affairs ECN Employment Category Number EHR Electronic Health Record EMG Executive Management Group DVA ERWBA Enhancing Resilience and well being ADFMHS ESFS Emergency Support to Families Scheme ESO Ex-Service Organisations FaHCSIA Department of Families, Housing,
Community Services and Indigenous Affairs
FBT Fringe Benefits Tax FCE Functional Capacity Evaluation FCP Family Care Plan FIS Financial Information Service Centrelink – free,
confidential and unbiased FIS to clients and those people approaching retirement or facing retrenchment
FLO Family Liaison Officers FMO Fleet Medical Officer FPS Fixed period of Service FWB Formation Welfare Board GHS Garrison Health Support HDSO Head of Defence Support Operations HIA Held in abeyance HPC Head of People Capability HPE Head Personnel Executive HPP ADF Health Promotion Program Provide preventative health
screening and to determine
234
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Acronym Full name Description medical fitness to meet individual readiness requirements
HRM Human Resource Management HRSS Human Resources Shared Services
Reform
HSR Health and Safety Representative HWCA Heads of Workers’ Compensation
Authorities
ICF International Classification of Functioning
IDC Interdepartmental Committee IES Integration & Enhancement of Services ADF MHS IET Initial employment Training IMPS Initial Minimum Period of Service IPPS ADF Integrated People Support Strategy IPS Integrated Payments System DVA payments system IPSM Integrated People Support Model DEPSEC DS ‘whole of
government’ initiative ISS Incident Self Service Will replace AC563 webform
process IWG Interdepartmental Working Group JHC Joint Health Command JHSA Joint Health Support Agency Now DMM K10 Kessler Psychological Distress Scale - 10 ADF Mental Health screen LWOP Leave without pay MCLO Military Claims Liaison Officer MCRA Military Rehabilitation and
Compensation Act 2004
MCRS Military Compensation and Rehabilitation Service
MEAO Middle East Area of Operation MEC Medical Employment Classification
System
MECR Medical Employment Classification Review
MECRB Medical Employment Classification Review Board
MECRR Medical Employment Classification Review Record
MEDALS Managing Emotions During Absence and Learning Skills
MEDICAS Notification of Medical Conditions MHS Member’s Health Statement MIER Management Initiated Early Retirement MilHOP Military Health Outcomes Program
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
235
Acronym Full name Description MIMI Medical Information Management Index MNO Medical Nursing Officer MRCC Military Rehabilitation and Compensation
Commission
MSB Military Superannuation and Benefits Act 1991
MSO Military Support Officers MSU MUFS Medically Unfit for Further Service MUNS Medically unfit for Naval Service NAG Non-Army Group NSA National Support Area NOK Next of Kin NOTICAS Notification of Service and Non-
Australian Defence Force Casualty
NPCMA Navy People Career Management Agency NWCC National Welfare Coordination Centre OATP Outpatient alcohol Treatment Plan OC Officer Commanding OC LSC Officer Commanding Logistics Support
Company
OHS Occupational Health and Safety OHSB Occupational, Health and Safety Branch OHSCAR Occupational Health, Safety,
Compensation and Analysis Reporting
OHSIR Occupational Health and Safety Incident Report
OHSMIS OHS Management Information System OHSMS Defence OHS Management System OMPQ Orebro Musculoskeletal Pain
Questionnaire ADF Mental Health screen
PACMAN ADF Pay and Conditions Manual PAF Permanent Air Force PCL-C Post-traumatic Stress Disorder checklist ADF Mental Health screen PCM Program Case Manager PCP Physical Conditioning Program PEC Primary Emergency Contacts PEEG Personnel Exceeding Establishment
Guidance
PERSO Personnel Officer Navy PFS Physical Fitness Standard PFT Physical Fitness Assessment DI(AF)PERS 53-13 Physical
Fitness in the Royal Australian Air Force
PI Permanent Impairment PIPS Pension Information Processing System DVA payments system
236
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Acronym Full name Description PMA Personnel Management Agency PMKeyS Personal Management Key Solution POI Proof of Identity POPS Post Operation Psychological Screening Psychological screening that
is employed following operational deployment
PRB Personnel Review Board Army – convened by Units to review members with administrative or disciplinary concerns
PSO Prescribed Service Officer Commissioning Scheme
PSPG People Strategies and Policy Group PSYMAN Psychology Services Manual PTI Physical Training Instructor PTSD Post Traumatic Stress Disorder PWW Project Warrior Welfare RANAODP Royal Australian Navy Alcohol and Other
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
237
Acronym Full name Description RTAPS Return to Australia Psychological Screen Psychological screening that
is employed following operational deployment
RTW Return to work SAM Single Access Mechanism Provision of personnel
services (including Reserve Service) and medical information to the DVA to support compensation claims submitted by current and former ADF members
SAP Simpson Assistance Package SC Service Centres SCF Single Claim Form SCMA Soldier Career Management Agency Army SDE Separation Dental Examination SHE Separation Health Examination SHO Senior Health Officer SI Seriously Ill or Seriously Injured SLA Service Level Agreement SOP Statement of Principles SOR Statement of Reasons SPEC Specialist Employment Classification SPP Suicide Prevention Program ADF MHS SRCA Safety Rehabilitation and Compensation
Act 1988 Workers compensation scheme oriented to rehabilitation
SSS Surviving Service Separation STRAT AME Strategically Aero Medically Evacuated SW Skills Waiver TIP Training and Information Program TMS Transition Management Service TN Termination Notice TOOCS Type of Occurrence Classification System OHS classification system
developed by the Australian Safety and Compensation Council
TPI Totally and Permanently Incapacitated TPMC Transient Personnel Management Cell TSS Transition Support Services UMECR Unit Medical Employment Classification
Review Conducted when decision is able to be made at the Unit or local level
UMR Unit Medical Record UOR Unit Orderly Room URLO Unit Rehabilitation Liaison Officer
238
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Acronym Full name Description UWO Unit Welfare Officer UWP Unit Welfare Plan VEA Veterans’ Entitlements Act 1986 VHC Veterans’ Health Care Program VRB Veterans’ Review Board VSI Very Seriously Ill or Very Seriously
Injured
VVCS Veterans’ and Veterans Families Counselling Service
VVCSP Vietnam Veterans Children’s’ Support Program
WDR Workplace Disability Report WHO World Health Organisation WRR Workplace Rehabilitation Representative WSSR Workforce and Shared Services Reform
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
239
F Forms • AC563 Defence OHS Incident Report – notification and reporting form for all OHS
incidents o Used by all ADO employees – ADF, Civilian, Reservists, ADF Cadets, contractors
and visitors o Information collected under the authority of the Defence Act 1903, OHS Act 1991,
ARPANS Act 1998 and the information is protected according to privacy principles in the Privacy Act
o Minor injuries must be reported within 28 days (Part 1) o All other incidents (including dangerous occurrence) – within 24 hours (Part 1) o No statute of limitations for timeframe to report OHS incident o Employer is required to complete and submit
• AC626 Vehicle Accident Report o Whenever a Defence vehicle is involved in an accident
• AC848 Tri-Service discharge Coordinators check list • AC849 Tri-Service Discharge or Transfer Clearance • AC853 Application for Resignation, Separation, Discharge and Transfer to the Reserve • AD088 ComCover Notification Record
o Where incident involves a member of the general public or a contractor o To be completed at same time as AC563 and AC626 (if applicable) o Notifies DIO of any incident that gives, or is likely to give rise to a liability claim
against Defence • AD145 ADF Transition Seminar Application • AD147 Comprehensive Preventative Health Examination (CPHE) • AD514 Refusal to Submit to a Medical or Surgical Treatment • AD523 Workplace Disability Report • AD524 Member Health Statement • AD576 Defence Employee Bank and Financial Institution Account Authorisation • PM006 Specialist Referral and Report • PM008 Report on a Case referred for Psychiatric or Psychological Examination • PM070 Separation Health Statement • PM101 Medical or Dental Fitness Advice • PM105 Outpatient Clinical Record • PM165 Medical History Questionnaire • PM166 Entry Medical Examination Record • PM344 Dental Clinical Record • PM384 Personal Health Records Transit Note
o Issue and Receipt voucher • PM387 Authority to release health information • PM514 Refusal to consent to health treatment • PM515 Request to access dental records • PM532 Medical Employment Classification(MEC) Advice • PM543 Authority to collect and release information • PM544 Rehabilitation Program Amendment • PM546 Referral for Rehabilitation Assessment – referral which triggers the requirement for
a rehabilitation assessment • PM546-4 Rehabilitation Program
240
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
o Details Rehabilitation Program activities and services • PM546-5 Rehabilitation Activities Schedule (RAS)
o Required activities detailed considered to be essential for the member’s clinical rehabilitation and successful return to work
• PM547 Rehabilitation Closure Report o A) Assessment – no program required o B)Program
Goal of the program have been reached Member returned to work with temporary restrictions but no longer requires
active rehabilitation management Member returned to work with permanent restrictions but no longer
requires active rehabilitation management Member discharges from the ADF at their own request or the member is
administratively discharged o C)Posted – member is posted to a new locality
• PM554-1 Separation Health Statement and Claim (Single claim form trial) o Forms part of a members medical records which document health history during
entire ADF service o Info on health statement will be used to assess eligibility for benefits under MRCA,
VEA, SRA, DFRDB Act, MSB o Information collected on behalf of Defence and can be disclosed to DVA,
ComSuper • PM554-2 Separation Health Statement and Claim – Separation Health Exam (Single claim
form trial) • PM554-4 Privacy and Disclosure by Department of Veterans’ Affairs and/or ComSuper • PE071 Discharge or Transfer Certificate • D0541 Compensation and Damages (VEA claim form) • D2020 Claim for Compensation and Rehabilitation (SCRA Claim Form) • D2049 Injuries and Disease Details Sheet (post July 2004) • D2051 Claim for liability and/or compensation (MRCA Compensation Form) • D2582 Claim for Disability Pension and/or Application for Increase in Disability Pension
(VEA claim form) • DM42 Invalidity Retirement from the Defence Force Medical Information • DM043 Members Particulars (request for a medical opinion based on the medical
documents and the DM42) ComSuper forms • M1 Application for Resignation Benefits • M10 Application for Benefits on Retrenchment • M20 Application for Retirement • M40 Application for invalidity benefits • Medicare Levy Variation Declaration – exemption from paying Medicare Levy after
discharged
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
241
G Policies, Instructions and Procedures
• ABR 6303 – Navy Safety System Manual • Defence Force Regulation 1952 – regulation 58F(1)
o provides authority for the provision of healthcare to ADF personnel • Defence Personnel Regulations 2002
o DPR 87(1)(c) Medically unfit o DPR 87(1)(d) The member does not comply with the medical standard for the trade
or employment in which they are engaged o DPR 87(1)(e) Not suited to be a member (psychological reasons) o DPR 87(g)(ii) Retention not in the interests of the Defence Force
• DI(G)ADMIN 60-1 ADF separation administration procedures • DI(G)PERS 03-4 Management Initiated Early Retirement and Termination of Service in the
ADF • DI(G)PERS 11-1 Amdt 6 Defence Force sponsored visits to service members suffering
serious illness or injury – The Australians Dangerously Ill Scheme (AUSDIL) o Principles, criteria and conditions that are to apply to sponsored visits under the
AUSDIL scheme by next of kin, relatives or nominated person to a member of the Defence Force hospitalised through serious injury or illness
• DI(G)PERS 11-2 Notification of Service and Non-Australian Defence Force Casualties o DCO has a central role in supporting the chain of command to meet its notification
responsibilities o Service Chiefs and Heads of the Defence Groups are responsible for co-ordinating
casualty notification with, as appropriate, support from the DCO • DI(G)PERS 14-2 Organised ADF Sporting Activity • DI(G)PERS 16-1 Health Care of Australian Defence Force Personnel
o Eligibility for health care • DI(G)PERS 16-11 - Australian Defence Force Policy on Physical Fitness
o Requirement that personnel must be physically fit o All ADF personnel should be capable of achieving and maintaining a defined ADF
minimum Physical Fitness Standard (PFS) as a function of operational preparedness o Commanders at all levels are responsible to ensure that personnel under their
command achieve and maintain appropriate levels of minimum and operationally required physical fitness and that physical training is conducted regularly and meets OHS requirements
• DI(G)PERS 16-15 Amdt 2 - Australian Defence Force Medical Employment Classification System
o All service personnel are to be employed appropriately in accordance with the MEC o MEC is determined according to each members primary military occupation o The ADF must make all reasonable efforts to retain and provide appropriate
employment opportunities for service personnel where MEC is downgraded during their service when the downgrading is attributable to their military service
o Medical fitness will impact on decisions involving postings, training, occupational rehabilitation, transfers between employment categories, payment of specialist allowances and retention in the ADF
242
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
o Whenever a member presents to a health facility or is hospitalised, health service personnel must assess the appropriateness of a members existing MEC. MOs must initiate or cause to be initiated timely MECR action
o Cos are to actively manage the employment of their personnel in terms of their MEC, especially during the transition from MEC4 to separation from the ADF
• DI(G)PERS 16-18 – Australian Defence Force Policy for Health Promotion Programs • DI(G)PERS 16-20 - Privacy of Health Information in Defence • DI(G)PERS 16-21 - Absence due to illness and absence for convalescence • DI(G)PERS 16-22 - Australian Defence Force Rehabilitation Program
o Occupational rehabilitation to ADF members irrespective of whether injury or illness is work related
o MRCC is Rehabilitation Authority for ADF Cadets and Declared Members • DI(G)PERS 16-24 – Mental Health Provisions in the Australian Defence Force • DI(G)PERS 19-18 – Defence Safety Manual
o Authority for SAFETYMAN as primary source for strategic safety policy in the Defence Organisation
• DI(G)PERS 20-6 Amdt No.2 – Death of Australian Defence Personnel o Expeditious return of remains and personal effects to family without compromising
positive identification, preservation of remains, chain of custody, investigative and coronial requirements and the health and welfare of personnel associated with the recovery and repatriation of the deceased
o ADF responsibility for controlling and managing provision of mortuary services for deceased ADF members
o Extends to civilians who are deployed in support of ADF operations in accordance with DI(G) OPS 05-3 Civilians in support of ADF Operations
• DI(G)PERS 25-2 Amdt No1 Employment and voluntary activities of the ADF members in off duty hours
• DI(A)PERS 33-6 - Welfare Responsibilities within the Army o All unit Commanders are to appoint a Unit Welfare Officer (UWO) and develop a
Unit Welfare Plan (UWP) • DI(A)PERS 33-11 - Army Casualty Administration and Support Framework
o Details the Army policy and procedures to be followed in order to support members suffering long term injury or illness
o Rehabilitation of members is an essential component of unit commander’s personnel management responsibilities
o Every member returned to the workplace after an injury or illness contributes to ongoing capability
o CA has delegated his Rehabilitation Authority function under SCRA and MRCA to enable DVA, JHC, DSG and AHQ to manage the day to day functions associated with the provision of health services, compensation claims management and transition to members
• DI(G)PERS 34-1 – Redress of Grievance – Tri Service procedures o Opportunity to appeal a MEC decision
• DI(G)PERS 36-2 Australian Defence Force Policy on Individual Readiness o Members are to achieve and maintain a standard of medical fitness as determined
by their Service • DI(G)PERS 42-1 Amdt No. 1 Australian Defence Force Family Support Policy
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
243
o ADF accepts an obligation to assist in providing appropriate family support to members
o Ensure adequate support measures are provided to enable members to render effective service and at same time to meet their personal responsibility to their family
• DI(A)PERS 47-10 Resignation, Retirement and Termination of Service - Officers • DI(A)PERS 116-5 Amdt 2 Separation of Regular Army Soldiers, Army Reserve Soldiers
and Soldiers on full time service policy and procedures o Units and transition centres are to ensure that soldiers separate from the Army with
a minimum or personal disruption and with the recognition that their personal contribution to the Army has been appreciated
o Soldiers who are going through the involuntary discharge process are to remain on CFTS until that process has been completed
• DI(A)PERS124-29 Medical Employment Classification System in the Australian Army o All soldiers undergoing voluntary separation are to undertake a SHE o Where a soldier is confirmed either MEC3 and is not considered ‘fit for discharge’,
or is confirmed MEC4 their discharge may be HIA in order for MECRB to consider their medical condition and most appropriate discharge mode
• DI(A)PERS 159-1 PULHEEMS Employment Standards • DI(A)PERS 173-6 Employment of Army Reserve members on continuous full time service • DI(AF)PERS 07-3 General discharge/ transfer procedures – Permanent Air Force • DI(AF)OPS 4-8 Individual Readiness • HB11/2009 Mental Health Screen for Casework • HD236 – Medical Employment Classification System procedures
o How new or reconfirmed MEC and employment restrictions are to be promulgated • HD278 – Health responsibilities on completion of a period of service • HD284 – Medical assessment and dental examination requirements for ADF personnel • HD289 – Mental Health Case Management in the ADF
o Practice guidelines to ADF mental health professionals and mental health specialists for the overall clinical case management of ADF members presenting with mental health problems and/or disorders
o Mental Health Disorders
o
– diagnosable mental health conditions that result in distress and/or impaired functioning Mental Health Problems
• HD290 – Health Procedures for the Delivery of the ADF Rehabilitation Program
– may include short-term stress reactions, reactive transient depressed mood and other stress related conditions which do not satisfy full criteria for a formal diagnosis of a mental health disorder according to widely accepted diagnostic systems
• HD291 – Management of Deliberate self-harm in the Australian Defence Force for Primary Care Providers
• HD294 – Suicide Risk Assessment and Management in the Australian Defence Force for Primary Care Providers
• HD295 – Mental Health and Psychology Services in Joint Health Command • HD919 – Guidelines on Australian Defence Force Access to Health Support • Defence Safety Manual (SAFETYMAN)
o Volume1, Part 2, Chapter 4 o Volume1, Part 1, Chapter 9 – Defence Incident Reporting
244
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
• CDF/SEC Joint Directive 08/2007 – Directive on Support to our Australian Defence Force Personnel
o Ensuring ADF members and their families are provided with exemplary support services throughout their career, particularly at times of separation
o Emphasis on seamless transition from military service to civilian life o DEPSEC DS is developing a ‘whole of government’ Integrated People Support
Model (IPSM) • CA Directive 09/10 Management of Medical Discharges in Army 11 May 2010
o Articulates interim medical discharge arrangements to be applied within the Army pending release of revised MEC in July 2012
o DAH input into all MECRB discharge decisions to ensure no member is discharged before DVA compensation liability is decided
• CAF Directive 0*/10 Operation of the Compensation Claims Liaison Office – Air Force (Draft)
• DEFGRAM No 440/2007 – 1 Aug 07 – Reporting of Occupational Health and Safety Incidents
o S69 OHS Act 1991 – Managers and Supervisors to report all OHS incidents in the workplace
• Defence Occupational Health and Safety Maturity Model – a systematic approach for managing OHS improvement
o Element 14 Treatment o Element 15 Incident Management o Element 16 Rehabilitation o Element 17 Compensation
• SOCAUST 16-2009 Welfare Policy
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
245
H Legislation
Military Rehabilitation and Compensation Act 2004 (MCRA) • The 3 Service Chiefs are responsible for the rehabilitation (Rehabilitation Authority) of
their full time serving members – s39 • Military Rehabilitation and Compensation Commission (MRCC) to provide generic and
specific information on compensation claims to the Service Chiefs Military Rehabilitation and Compensation (Consequential and Transitional Provisions) Act 2004 Occupational Health and Safety Act 1991
• Duty of care provisions and responsibilities Occupational Health and Safety (Commonwealth Employment) Amendment Act 2006 Safety Rehabilitation and Compensation Act 1988 (SCRA)
• Military Rehabilitation and Compensation Commission (MRCC) to provide generic and specific information on compensation claims to the Service Chiefs
Privacy Act 2004 Australian Radiation Protection and Nuclear Safety Act 1998 (ARPANS Act) Defence Act 1903 Veterans’ Entitlement Act 1986 Defence Force Disciplinary Act 1982 (discharge/ separation modes)
246
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
I TMS Roles – Defence and DVA SCHEDULE A – ROLES OF DEFENCE AND DVA IN PROVIDING TRANSITION MANAGEMENT SERVICES
DEFENCE
Referral to TMS by Defence:
ADF Members can be referred to TMS by:
• Joint Health Command following a medical review where the prognosis for continued employment in the ADF is poor. This referral would be to provide the ADF member with information on the DVA TMS only.
• The Career Manager (CM) or CO/OC following a recommendation of the unit Medical Employment Classification Review (MECR) or a decision of a Medical Employment Classification Review Board (MECRB) that the member is MEC4.
• The ADF Rehabilitation Program Case Coordinator that a member is likely to be medically separated.
• The ADF Transition Centre that a member is medically separating.
Transition Support provided by the ADF Transition Centres:
• The ADF Transition Centres provide administration and/or advice on the following:
• Requirement for a Separation Health Examination and Separation Dental Examination
• Confirmation that leave, Prior Service/Non-Effective Service/Long Service Leave, pay, allowances and allotments have been finalised.
• Confirmation that there are no financial debts in Roman, Relief Trust Fund etc.
• Housing and relocations entitlements and how to access these.
• Career Transition Assistance Scheme entitlements. (ADF Transition Centre staff also hold delegations to approve these applications)
• Accessing information and forms for superannuation.
• Retaining, obtaining or returning of ADF Identification Cards, Access Cards, and Retired ID Cards.
• Accessing the Retired List.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
247
• Retaining or returning Official Passports
• Accessing Records of Employment, Training and Certificates of Service, Civil Accreditation and ADF Higher Education Advanced Standings Scheme
• Retaining or returning Defence Travel Cards, Defence Purchasing Cards
• Converting ADF Licences to civilian equivalents
• Accessing and updating ADF Wills
• Accessing Honours and Awards
• Completing the ADF Separation Clearance Form
• Accessing Medicare Cards, Private Health Insurance and Ambulance Cover
• Accessing Defence Community Organisation services
• Accessing Defence Families Australia support
• Accessing Centrelink, the Financial Information Service and the Financial Information Seminar Program.
• Completing the Department of Veterans’ Affairs/Veterans’ and Veterans’ Families Counselling Services Questionnaire
• Accessing the Training and Information Program and ex service organisations for assistance with completing claims paperwork.
• Accessing the Stepping Out Program
• Accessing the ADF Financial Consumer Council services
Responsibilities of Directorate of Transition Support Services in relation to TMS:
• Administration/advice to the ADF Transition Centres
• Management of Service Level Agreement
• Evaluation of TMS against the SLA.
• Training, education and communication within Defence.
• Maintaining currency of information available to members through Defence media.
248
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
DEPARTMENT OF VETERANS’ AFFAIRS
Pre Medical Employment Classification Review Board (MECRB):
• Contact member, to discuss TMS and requirement for Discharge Impact Statement (DIS) and Member’s Health Statement (MHS).
• Initial interview and preparation of the DIS. To be provided to the MECRB secretary within 28 days of notification and in time for the MECRB.
• Assist member, if required, with completing the MHS. Where a member needs such help, the TMS role is that of a “friend” and access to medical details should not be necessary.
Transition Assistance for Medically Separating ADF members who elect to access TMS:
• Provide ADF members information and advice on DVA entitlements only. The TMS should not advise the ADF member on any Defence related entitlements.
• If the member has separated TMS can refer member to the following:
• Rehabilitation providers
• Community service providers
• Income support providers
• Community medical or employment/financial support organisations.
• Assist in the preparation of claims for ADF members with complex or specific needs (such as mental health problems, head injuries etc).
• Presentation of the national DVA presentation at the ADF Transition Seminars.
• Provide unit briefings (in addition to the ADF Transition Seminars)
• Represent DVA at the Regional Stakeholder Forums (RSFs).
• Ministerials involving TMS.
• Client complaints handling and resolution for DVA services including TMS only.
• Promotion/marketing of the TMS.
• Maintenance of DVA Intranet and TMS Internet web site.
• Provide Defence with the TMS quarterly report against the KPIs stipulated in the SLA.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
249
DEPARTMENT OF VETERANS’ AFFAIRS
On-Base Visiting Schedule:
Department of Veterans’ Affairs are to provide an On-Base Visiting Schedule as follows:
Queensland:
• Enoggera Barracks, Townsville – full time presence
• Cairns – 1 day per fortnight
NSW:
• Sydney and Wagga Wagga – 2 days per week
• Liverpool, Richmond, RAAF Williamtown, Shoalhaven – 1 day per fortnight
Victoria and Tasmania:
• Melbourne – 2 days per week
• Bandiana, Anglesea Barracks (Hobart) – 1 day per fortnight
ACT:
• Canberra – 2 days per week
South Australia:
• Adelaide – 1 day per fortnight
Western Australia:
RAAF Pearce, Leeuwin, Fleet Base West – 1 day per fortnight
Northern Territory:
Darwin – 2 days per week
250
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
K DUNT RECOMMENDATION – DVA PROGRESS as at June 2010
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
2.1 In considering the wider focus for Operation Life expressed in the five priority areas, the Department of Veterans' Affairs (DVA) should closely consider the evidence-based literature on suicide prevention and should only implement programs that are evidence-based and most likely to be successful in veterans. These are most importantly doctor education on detection and treatment of depression and restricting access to lethal means.
The Government will review the Operation Life workshops at the conclusion of the first year of the Operation Life expansion, in June 2010, to ensure that programs that are evidence-based are being implemented.
In addition, doctor and mental health practitioner education on detection and treatment of depression and other mental health conditions will continue.
A formal review will commence June 2010. The new suite of Workshops commenced May 2009.
Responses to a select tender are currently being evaluated and it is expected the tender process will be finalised by end July 2010. Ex-service representatives have agreed to act as a reference group for the review.
December 2010.
3.1 It is likely that a study of suicide in a full cohort of post-Vietnam veterans will be conducted at some time in the future. Before making a decision to proceed, there should be a review of findings of: the Australian Institute of Health and Welfare investigation into the cause of death of DVA clients by
If a further study is commissioned following the above investigation and study as well as the current study into health effects of service on families (the Vietnam Veterans’ Family Study), the findings of this research and the
This recommendation will be re-visited following further analysis of the AIHW data and when the Family Study is completed or can provide
A suicide study in a full cohort of post Vietnam veterans will not be considered at this stage until the Family Study has been completed.
No action required until after completion of the Family Study.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
253
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
age/sex/conflict with a specific focus on suicide; and ‘Preventing suicide: a psychological autopsy study of the last contact with a health professional before suicide’ being undertaken by Griffith University.
The former will indicate whether numbers and difference between veterans and non-veterans are sufficient to justify a full cohort study. The latter should further identify likely factors in suicide in Australian veterans. In addition, any decision will need to take full account of the methodological problems to which veteran suicide studies are susceptible, particularly misclassification of veterans and unadjusted demographic differences between veterans and the comparison group.
methodological problems identified by Professor Dunt will be taken into account.
adequate data.
254
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
5.1 The ADF and DVA should have joint responsibility for a comprehensive transition service that works closely with the ADF Transition Centres and extends to at least 12 months post-discharge. It should resolve the duplication in services now being offered by the IPSS and TMS. ADF should fund pre-discharge activities and DVA post-discharge activities within this joint responsibility.
Defence and DVA are working collaboratively to deliver a seamless transition service that ensures all reasonable assistance and support is available and utilised by members and their families preparing to transition to civilian life.
Collaborative forums – Defence Links and the Interdepartmental Working Group – are used to improve current transition material and to develop procedures that maximise support through transition.
Action complete March 2010
Action complete March 2010.
5.2 The Lifecycle pilot adds value to existing programs (IPSS/TMS) in improving staff training and support. If successfully evaluated it should be rolled out nationally.
The Lifecycle Transition Mental Health and Family Collaborative is an initiative currently being trialled in Townsville. The aim of the initiative is to establish more effective mental health and family support services for medically separating personnel at risk of, or experiencing, mental health problems. Outcomes and recommendations from the trial will inform further
Regular progress reports submitted by ACPMH have been reviewed for potential improvements.
Ongoing monitoring until evaluation.
An ADF/DVA advisory committee of key stakeholders
The final report has been accepted by Defence and DVA. Future proposals will be considered by both Departments and it has been agreed that the intent of this recommendation is now finalised.
Action complete and this recommendation is finalised.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
255
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
development of the enhanced transition support service. The Government notes that the timetable for the evaluation of the Lifecycle pilot in Townsville is mid 2010.
(LAG) has been established to provide oversight of this initiative.
5.3 In principle, families should have an involvement in transition programs. This could be at the Transition Seminars involving the Stepping Out program that may need some redesign.
The Government recognises the importance of families in the Defence transition services and will explore strategies to increase family involvement in the transition service including ADF transition seminars and the Stepping Out Program.
Recommendation will be taken into account as part of the evaluation of the Stepping Out Program.
Defence Support Services Group consults Defence Community Organisation and Defence Families Australia on all aspects of transition and are now delivering family-friendly programs.
A Family Forum is proposed in late 2010 in collaboration with a nationally recognised centre.
Resilience training for Defence members and families is currently
Item completed and action finalised.
December 2010
July 2010
256
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
being introduced into the ADF. This will be incorporated into the transition seminars as ‘LifeSMART’ by July 2010.
Stepping Out re-design element complete March 2010.
Item complete March 2010.
5.4 It is important that members leaving the ADF with mental health (or other problems) are fulsomely acknowledged for their contribution to the ADF, particularly so as their health had deteriorated while they were in the ADF. This could take the form of a letter of thanks from CDF or Passing out Parade.
ADF members who are separating are to be pro-actively engaged and treated with care, consideration, and compassion. The separation process is to be as uncomplicated and stress free as possible and include formal acknowledgment of the member’s contributions to the ADF.
No direct role for DVA as recommendation to be implemented by Defence.
ADF will proactively engage with members separating with mental health problems and mental illness to formally acknowledge their contribution to the ADF. Single Services currently have extant policy on dignity during separation. A scoping study is currently underway.
30 June 2012 (as advised by ADF).
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
257
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
5.5 A Keeping in Touch program post-discharge with responsibility jointly by the ADF and DVA extends this healing process. In doing so, it is likely to make an important contribution to the proactive management of any emerging mental health problems.
As mental health issues may not surface for some period after separation from the ADF, a robust program that encourages contact with Defence and veteran organisations may serve to assist the better management and early detection of emerging mental health problems. Defence and DVA are currently exploring this issue.
A joint program will be trialled, commencing in 2009-10.
The Keeping In Touch website is currently under development and due for completion by the end of July 2010. ESO representatives were briefed at the Emerging Issues Forum in early June and have been asked to participate as part of the user acceptance testing for the website. A separate brief (B10/0539) on progress and launch of the website was forwarded on 25 May 2010.
30 June 2011.
6.1 Initiatives such as the Single Claim Form, Separation Health Examination and the Client Liaison Unit are valuable and, subject to satisfactory trialing can
In particular, DVA is currently implementing the following initiatives consistent with this recommendation:
Four separate issues:
1. Single Claim Form;
1) Single Claim Form trial ran from May 2009 to November 2009. Evaluation commenced in
Single Claim Form trial has been concluded.
258
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
be strongly supported.
The changing business processes of the MRCA group including a strong orientation to client-service are welcomed but should extend to all three schemes, particularly the VEA group and be further strengthened with business, training and evaluation plans.
Experienced case managers should be assigned to claims of clients having complex multiple needs claims.
A Separation Health Examination (SHE) trial is running until mid 2009. This will be evaluated with a view to a national roll out. It incorporates a single medical assessment form for all DVA Acts as well as ComSuper benefits.
It is the Government’s intention to introduce a Single Claim Form, commencing with a trial from May 2009. This will provide the opportunity for driving the application of more consistent work practices across all three Acts.
The concept of risk based differentiation for the management of claims will be extended to cover the Military Rehabilitation and
2. Separation Health Examination (SHE);
3. Client Liaison Unit; and
4. Use of experienced case coordinators.
February 2010 and has been delayed due to unforseen circumstances. Report to Commissions on findings due early July2010.
2) SHE –trial completed, July 2009. Evaluations from DVA and ComSuper have been received. The evaluation from Defence was received in late May 2010. The draft evaluation report is being finalised.
3)CLU – the Client Liaison Unit was established in 2007.
4) Case coordinators element complete March 2010.
SHE trial has been concluded.
Item complete March 2010.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
259
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
Compensation Act (MRCA). Incoming claims are screened then streamed into different business process teams based on work types or triggers. This targets ‘low risk’ claims for quick and simplified processes enabling the diversion of resources into those clients who need more personalised support and close management. The Government will provide funding to increase the number of experienced case managers to manage complex claims.
6.2 A separate process for claims involving chronic mental conditions should be established involving formal consultation with an appropriate mental health professional (psychiatrist or clinical psychologist) to assess the mental health impact of DVA decisions on veterans at all important decision points (e.g. primary claims, Section 31 and
This process will be managed with Recommendation 6.1 above. DVA will introduce a protocol for ‘Managing the provision of advice to clients at the risk of self-harm’. This protocol will expand the conduct of internal DVA case conferencing on identified clients together
Commission submission to be developed in relation to the TTI in early 2010.
A joint Commission Submission incorporating this recommendation and 7.1 has been developed. The submission covers approval to extend the TSR where there is robust medical evidence that a veteran
Due to
Complexities of the consultative framework, particularly with external bodies such as the RANZCP, the timeframe for finalisation of
260
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
where relevant VRB and AAT appeals, as well as suspension and downgrading of benefits and CDDA applications. The mental health professional should ‘sign-off’ for the action to proceed.
It is desirable that the period of the Temporary Special Rate pension (or equivalent) can be extended if the veteran’s doctor (or in the event that a doctor is not able to do this, a representative of the veteran) can provide robust evidence of a level of patient distress or risk of self-harm sufficient to render dangerous the conduct of a GARP (V) or GARP (V) M assessment of impairment and lifestyle.
with obtaining advice from the treating health professional on how best to manage the delivery of the advice.
The Temporarily Totally Incapacitated (TTI) special rate of pension under the VEA is payable if the person meets the eligibility criteria for special rate pension, with the exception of the war caused incapacity being only temporary. It would not be within the intent of the payment to continue eligibility if the person is no longer prevented from continuing to work due to their war caused disabilities. However, where the mental illness is accepted as war caused and a change in circumstances such as a re-assessment would likely result in an exacerbation of the condition, and the veteran's doctor can provide
may be at risk of self harm or suicide. Due to delays with legal clearance, it is anticipated that this will be considered by Commissions in early July 2010.
The protocol for ‘Managing the provision of advice to clients at the risk of self-harm’ was approved by Commissions on 16 June 2010 following consultation with the National Mental Health Forum. An all staff instruction is currently being finalised.
March 2010 has been revised to September 2010.
Action complete and this element of the recommendation has been finalised.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
261
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
robust evidence of this, it would be appropriate for the period to be extended.
MRCA shares the many underlying features of TTI in that it provides for incapacity payments which are payments for economic loss payable while an accepted condition continues to impact on a person's ability to earn. If an accepted mental health condition is impacting on the person's ability to work the period of incapacity payments will continue. Any change in payments is generally based on a rehabilitation assessment which includes consideration of psychological and other socioeconomic factors. Permanent Impairment (PI) payments are also payable as a weekly pension or lump sum equivalent and are not contingent on a person's
262
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
ability to work but rather on whether the condition has reached a threshold of permanent and stable impairment. Once this threshold is met, the payment will continue irrespective of whether the person is in paid employment.
6.3 Every VRB hearing for a veteran involving a mental health-related condition should aim to have one member with a clinical mental health background on the two or three member board.
The Government notes there are practical difficulties that may arise from time to time for particular hearings. The first step is to aim for inclusion of persons with clinical mental health background among VRB members.
A phased implementation strategy will be considered.
The VRB have advertised for new members via the Mental Health Council of Australia as well as via the usual channels. The advertisements have included a specific request for members with clinical mental health expertise. The intent of this recommendation is being actioned through the appointment process, which is still underway.
Ongoing.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
263
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
6.4 DVA will need to increase its capacity to access psychiatric/clinical psychological advice for both individual cases and policy involving mental health more generally
DVA does have access to external, independent psychiatric specialist advice in the development of policy and clinical programs. The Government agrees to fund additional full time clinical psychologists as well as the provision of consultant psychiatrist advice. This additional support will also increase DVA’s capacity, where relevant, at important decision points as identified in Recommendation 6.2 above.
The appointment of relevant mental health practitioners to provide high quality clinical and policy advice.
Following Commissions approval, advice received on recruitment action resulted in an open tender process being undertaken. The Request for Tender (RFT) was published on AusTender on 25 June. The RFT will close on 26 July 2010.
Recruitment action expected to be finalised by August 2010.
6.5 In the event that a veteran’s claim is incomplete, DVA should consider a further step in the primary application process whereby the application could be returned to the veteran indicating areas where further supporting documentation is the necessary. This would be different in nature to a Section 31 review.
As stated above at Recommendation 6.1, a review of current business processes across all three Acts will be conducted.
In some cases, the client or their representative is personally contacted by DVA to clarify what further information may need to be
A review of current business processes across all three Acts will be conducted.
This is associated with the single claim form process (Recommendation 6.1).
Revised business processes for the single claim form involve DVA making early contact with clients or representatives to advise if further information is required. Evaluation of the single claim
A full business process re-design to be completed by 30 June 2011.
264
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
provided to properly assess a claim. DVA will review this process to ensure this occurs in all cases where appropriate.
form will look at revised business processes (see Recommendation 6.1 above).
Rehabilitation & Compensation re-aligned its business from early June 2010 into Liability Determination and Rehabilitation & Benefits. The focus will now move to business improvements, consistent and quality and this aspect will be considered as part of this process. Oakton Consulting Firm has also been contracted to provide a report on performance reporting and will consider this issue. Due to report August
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
265
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
2010.
7.1 Since diagnosing and assessing service connection for PTSD is not straightforward, it would be worthwhile to develop suitable guidelines for this, to supplement the Statement of Principles (SoPs). It is envisaged that these might involve a suitably qualified clinician taking a structured detailed history that established both diagnosis and possibly exposure to service-related and non-service-related traumatic stressors service. This would be conducted at the time of the veteran’s health examination in the lead up to the submission of their claim for compensation to DVA.
Until such time as these best practice methods can be decided and instituted and given the difficulties outlined in the use of historical military record sources, it would be better to generally avoid their use. In other words, processes for PTSD should
DVA, the Royal Australian and New Zealand College of Psychiatrists and ex-service organisations agreed in 2005 to a diagnostic and assessment protocol, ‘Guidelines for Psychiatric Compensation Claims: Diagnosing, Investigating, Determining and Assessing’, for psychiatrists’ use in the diagnosis of PTSD. The content, format and use of the protocol will be reviewed in the context of this recommendation, noting that this is not a supplement to a SOP. However, it will provide improved support for psychiatrists and assessors.
Implications for Statement of Principles will be examined. The relevant diagnostic and assessment protocol for psychiatrists’ use in the diagnosis of PTSD will be reviewed.
A joint Commission Submission incorporating this recommendation and 6.2 has been developed. If agreed, guidelines for managing claims involving veterans at risk of self harm will be developed in consultation with the Royal Australian and New Zealand College of Psychiatry (RANZCP) and the Australian Centre for Posttraumatic Mental Health (ACPMH). Due to delays in legal clearance it is anticipated that this will be considered by Commissions in July 2010.
Due to
Complexities of the consultative framework, particularly with external bodies such as the RANZCP and ACPMH the timeframe for finalisation of March 2010 has been revised to September 2010.
266
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
proceed more like other claims. This is as judged by the presentation of material in the veteran’s claim and its conformity with the relevant SoP both in terms of disease causation and service connection based on a reasonable hypothesis that can not be disproved.
7.2 The use of historical military service records should move more to the investigation of fraud cases w here their use can very clearly demonstrate that a fraud has been perpetrated. Their use should not be routine. If there were particular reasons that they would have value in unusual cases other than for the investigation of fraud, the information needs interpretation and signoff by a mental health professional.
The Government notes that Professor Dunt has subsequently clarified that the use of military service records can be an essential part of any investigation into a claim for liability, but that the use of military researchers should not be routine. The Government supports the development of procedures whereby a case conference is held prior to the use of military researchers with the requirement that the Repatriation Commission and the Military Rehabilitation and
As outlined in the Client Contact investigation practice statement, military research is part of a range of preliminary checks that can occur as part of the two-step screening of all investigations.
Action complete September 2009.
Action complete September 2009.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
267
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
Compensation Commission be charged with the task of ensuring ongoing monitoring of this process. It should be noted that the use of military researchers in DVA reduced from 296 to 147 claims between 2006 and 2008, and currently occurs in less than one per cent of claims.
7.3 Tip off cases should only be investigated where there is further substantiation and where there are reasonable chances of success. Reliance on anonymous ‘informant networks’ alone is insufficient to form the basis of subsequent investigation
DVA has moved in the past six months to incorporate this process. Instructions have been recently issued to DVA fraud investigators that contact with the subjects of allegations and potential witnesses should only occur where there is evidence in support of the allegation or there is evidence which requires clarification. DVA does receive anonymous allegations, both verbally and in writing, of fraud by others. By law, all allegations must be examined. About 17 per cent of fraud allegations
DVA has moved in the past six months to incorporate this process.
Action complete June 2009.
Action complete June 2009.
268
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
‘screened’ are referred for fraud investigation.
Of 63 cases that have been assessed by a new two step process (the vast majority of these would be tip offs), since January 2009 only two cases have been referred to formal investigation.
8.1 While volunteer Pension Officers endorsed by ESOs have provided a great community service, it is time to move to a new two-tier system. The first tier would consist of largely volunteer TIP-trained Officers as at present. They would in future restrict their advice to straightforward cases.
The second tier would consist of a new group of trained Pension Officers and Advocates who would be accredited on the basis of their completion of a Diploma or Certificate IV TAFE qualification. They would be paid through BEST or similar DVA-funded program.
The Government agrees there are some issues that need to be reviewed regarding the future operations of Pensions Officers and the TIP and BEST programs. These initiatives may result in significant change. To ensure changes are appropriate, the Government will consult with key groups. This will be a government priority in 2009-10.
A process will be developed, which can then form the basis of consultation with key stakeholders.
The Report on the Review of Advocacy and Welfare Services is not yet finalised. A range of administrative arrangements have been referred to the Secretary of DVA for action in regard to the BEST grants round 13. A document discussing the key policies, principles and service models that underpin the proposed new BEST grants, and the
December 2010
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
269
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
They would provide advice to veterans in cases that were not straightforward including appeals and tribunal appearances.
Both groups would be subject to appropriate quality assurance procedures.
Both tiers of Officers would operate with the endorsement of an ESO. The second-tier, paid, accredited Officers would operate on a day-to-day basis more independently of the ESOs so they can provide services both to veterans who align themselves with an ESO and those who do not by reaching out to the veteran.
proposed enhancements to the TIP structure and management will shortly be circulated to a wide range of stakeholders for comments.
9.1 DVA’s mental health strategy beginning in 2001 has led to the development of a number of community mental health promotion programs. DVA’s intention to consider how this strategy might be further developed is strongly supported. Programs for suicide and alcohol
Accepted. DVA’s future mental health strategy will incorporate findings of the ACMPH evaluation on mental health initiatives due for
This recommendation will be a two staged approach.
A submission for both Commissions was considered in February 2010 regarding a mental health update
December 2010.
270
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
misuse require particular attention. The ACPMH have been contracted by DVA to evaluate its Mental Health Initiatives for 2007-10 and this will be very useful in identifying other areas.
completion in September 2010.
on activity and key directions framework. An updated mental health policy incorporating outcomes of the ACPMH evaluation will be considered by the end of 2010; and
The Right Mix - Your Health and Alcohol website and associated resources have been updated and released. A media campaign to promote The Right Mix in the context of Anzac Day was approved by Department of Finance and Deregulation on 23 March 2010.
9.2 VVCS is a very successful DVA program that is likely to expand and further develop. Recent developments in Medicare Australia whereby subsidy is now
VVCS only employs qualified psychologists and social workers as clinical staff, and supports evidence-
A range of improvements is being developed.
Action complete March 2010.
Action complete March 2010.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
271
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
available to psychologists and social workers for counselling are having major impacts and defining new standards for psychologist services. It supports only evidence-based interventions. These are Focused Psychological Strategies for registered psychologists and GPs and Psychological Therapy for clinical psychologists. VVCS should be able to demonstrate that they conform to this standard or how it plans to do so.
It is important that there should be some level of involvement of psychiatrists or GPs with interests in mental health in all VVCS centres. This is because the treatment of DSM-IV mental conditions may require psychotropic drugs which only doctors can prescribe. This involvement could largely take the form of shared care, participation in case conferences and education.
based therapies.
VVCS consults regularly with psychiatrists and general practitioners in the development of case plans and where appropriate refers clients to specialist mental health services.
272
ABCD Department of Defence - Joint Health Command
Support for Injured or Ill Project (SIIP) - Review of current practices December 2010
All rights reserved. KPMG and the KPMG logo are registered trademarks of KPMG International.
Liability limited by a scheme approved under Professional Standards Legislation.
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
9.3 The Hard-to-Engage and Barriers to Social and Vocational Rehabilitation Lifecycle Initiatives undertaken by the ACPMH, on contract with DVA can be strongly supported. The Keeping-in-Touch Initiative (Recommendation5.5 above), could be extended to offer group proactive health and wellness with possible individual follow-up to veterans and their families.
The Hard-to-Engage and Barriers to Social and Vocational Rehabilitation initiatives are components of the Lifecycle initiative, one of the Government’s key election commitments. The Government will review the Keeping In Touch initiative to take into account this recommendation, and will pilot an extension of Keeping in Touch, commencing in 2010.
Review the outcomes of the Lifecycle initiatives and, if appropriate, consider rolling these initiatives out to the ‘Keeping In Touch’ cohort.
Actions on track. The final report for the Hard to Engage pilot has been completed. Recommendations will be considered by Commissions in July 2010.
The Barriers to Rehabilitation project is on track and will be completed in September 2010.
The Keeping in Touch initiative is covered in recommendation 5.5.
30 June 2011.
9.4 A strategic review of PTSD programs in Australia should be urgently commissioned. This should be comprehensive in scope and cover service access, acceptability and cost and most successful models of care. Priorities should be defined such that their implementation will have
The Government agrees to fund a review of departmentally funded PTSD programs. This review is expected to commence in late 2009 and conclude by mid 2010.
A working group across a number of business areas is to be established to advise on the best way forward.
The open Request for Tender (RFT) was published on AusTender on 13 May 2010. The RFT closed on 4 June 2010 and DVA is currently evaluating the tender responses. It is
December 2010.
Department of Defence - Joint Health Command Support for Injured or Ill Project (SIIP) - Review of current practices
December 2010
273
Rec #
Recommendation Government Response Implementation Strategy
Current status as at 30 June 2010
Proposed Completion Date
the most effect on the level of patient care i.e. the programs that are funded will be effective as well as efficacious.
anticipated that the tender process will be finalised by the end of July 2010.
9.5 DVA has been very active in supporting and funding research and this can be strongly supported. Its support for evaluation of its innovative programs has been a little less active and could be further developed.
DVA’s Applied Research Program has adopted new research priorities, ensuring that they are aligned nationally and follow best practice guidelines consistent with the Department's strategic directions. The evaluation of innovative programs in areas such as mental health, aged care and in supporting younger veterans leaving the military will be incorporated into these research priorities.
Recommendation 9.5 will be considered when determining research priorities.