58
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 1 Department of Diagnostic Medicine Laboratory Handbook
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 1
Department of Diagnostic Medicine
Laboratory Handbook

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 2
Table of contents
Our mission ............................................................................................................... 3 Where to find us ....................................................................................................... 4 Pavillion and area map ............................................................................................ 5 Calendar of Statutory Holidays 2009-2010 .......................................................... 6 Phlebotomy services................................................................................................ 7 Important Numbers .................................................................................................. 9 Requisition Form .................................................................................................... 10 Specimen ID & Rejection ...................................................................................... 12 Biohazard specimen bags .................................................................................... 13 Specimen Delivery ................................................................................................. 14 Blood ........................................................................................................................ 16 Results Reporting................................................................................................... 18 Panic Values (Telephone limits) .......................................................................... 18 Therapeutic Drug Monitoring ................................................................................ 21 Analytical interferences ......................................................................................... 22 Near patient testing................................................................................................ 23 Research and Trials............................................................................................... 24 Reference Intervals ................................................................................................ 25 Various tests requiring special collection ........................................................... 40 Glucose tolerance test........................................................................................... 43 Patient Instructions for a Clean-Catch Urine Collection................................... 44 Patient instructions for 24-Hour urine collection................................................ 45 24-Hour urine collection bottles ........................................................................... 46 Patient instructions for sputum collection ........................................................... 47 Patient instructions for stool collection................................................................ 48 Patient instructions for stool O&P collection ...................................................... 49 The following protocol is to be used for diagnosing Influenza. ....................... 50 Hemoccult screening - Patient information ........................................................ 51 Labeling of cytology specimens ........................................................................... 52 Procurement of cytology specimens ................................................................... 53 Transfusion service ................................................................................................ 55
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 3
Our mission
To provide medical laboratory services consistent with the needs of the health care team and their patients in a professional and caring manner.
To initiate and collaborate in research activities directed towards the improved understanding of disease, its diagnosis and monitoring
To ensure the optimal use of the laboratory service
To encourage and develop all staff to attain their true potential and to develop a milieu which promotes teamwork

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 4
Where to find us
Address:
Pavillion D-136
Jewish General Hospital
3755 Côte-Sainte-Catherine Road
Montréal, Québec, Canada
H3T 1E2
Entrances:
1. Main entrance on Côte-Sainte-Catherine
Road (Pavilion B)
This above entrance is temporarily closed
due to construction.
2. Légaré Street (Pavilion E) entrance,
across from the hospital's parking lot
3. Côte-des-Neiges Road (Pavilion A)
entrance
4. For Pavilion H, the entrance can be found
on Côte-des-Neiges Road
Parking:
A parking lot charging hourly or daily rates is
located on Légaré Street, between Côte-
Ste-Catherine Road and Bourret Avenue.
Valet parking is available at the Côte-des-
Neiges and Légaré entrances of the
hospital. Parking is also possible on many of
the nearby streets (some of which have
parking meters), but there may be limitations
or restrictions on the hours and days when
parking is permitted.
Public transportation:
The hospital is accessible through many
MTC/STM bus and metro lines.
Metro - Côte-Sainte-Catherine and
Plamondon (orange line), as well as Côte-
des-Neiges (blue line)
Bus Lines - 165, 535, 129, 124, 160, 161,
119 and 51
(Night bus lines - 368, 369 and 370)
Contact us:
Tel: 514-340-8222 ext 5094
Fax: 514-340-7510
Laboratory Hours
The laboratory operates 24 hours a day 7 days a week (including statutory holidays). Tests with turnaround times less than 24h are performed daily. Tests with turnaround times greater than 24h are performed Monday to Friday: 08h30 - 16h30 (excluding statutory holidays).
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 5
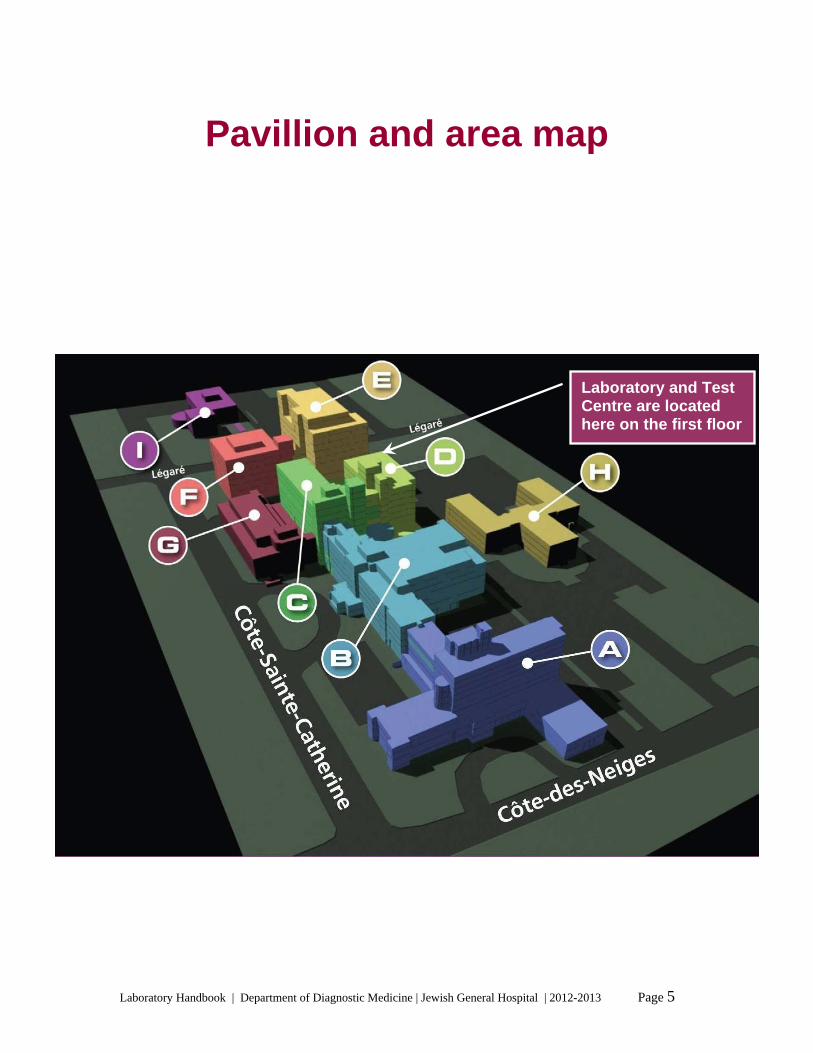
Pavillion and area map
Laboratory and Test Centre are located here on the first floor

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 6
Calendar of Statutory Holidays
2012-2013
*
Dimanche Sunday
1er juillet 2012 July 1st, 2012
CONFÉDÉRATION CANADA DAY
Lundi Monday
3 septembre 2012 September 3rd,2012
FÊTE DU TRAVAIL LABOUR DAY
Lundi Monday
17 septembre 2012 September 17th, 2012
1er JOUR DE LA ROSH HASHONAH 1ST DAY ROSH HASHONAH
Mercredi Wednesday
26 septembre 2012 September 26th, 2012
YOM KIPPOUR YOM KIPPUR
Lundi Monday
8 octobre 2012 October 8th, 2012
ACTION DE GRACE THANKSGIVING
Mardi Tuesday
25 décembre 2012 December 25th, 2012
NOËL CHRISTMAS DAY
Mercredi Wednesday
26 décembre 2012 December 26th, 2012
LENDEMAIN DE NOËL BOXING DAY
Lundi Monday
31 décembre 2012 December 31st, 2012
VEILLE DU JOUR DE L’AN NEW YEAR’S EVE
Mardi Tuesday
1er janvier 2013 January 1st, 2013
JOUR DE L’AN NEW YEAR’S DAY
Mardi Tuesday
26 mars 2013 March 26th, 2013
1er JOUR DE LA PASSOVER 1ST DAY PASSOVER
Vendredi Friday
29 mars 2013 March 29th, 2013
VENDREDI SAINT GOOD FRIDAY
Lundi Monday
20 mai 2013 May 20th, 2013
FÊTE DE LA REINE VICTORIA VICTORIA DAY
Lundi Monday
24 juin 2013 June 24th, 2013
SAINT-JEAN BAPTISTE
* *
Le lundi 2 juillet 2012 sera fêté et chômé en remplacement du dimanche 1er juillet 2012. Monday July 2nd, 2012 will be observed in lieu of Sunday, July 1st, 2012.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 7
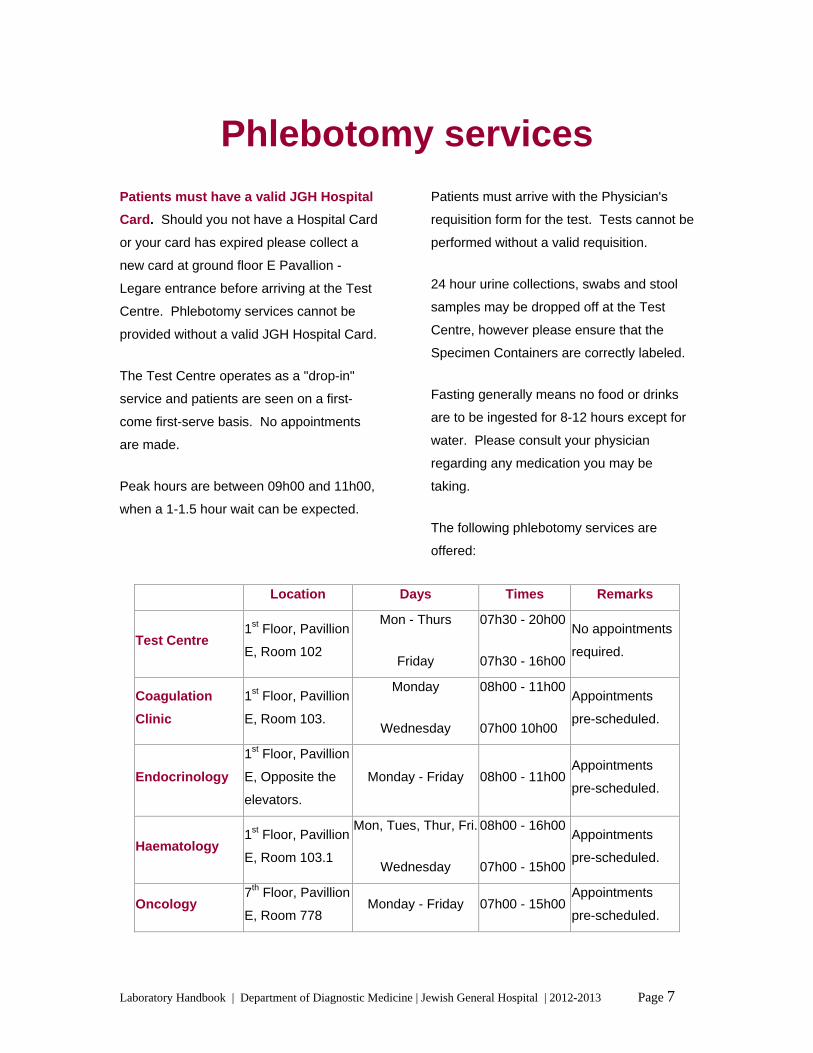
Phlebotomy services Patients must have a valid JGH Hospital
Card. Should you not have a Hospital Card
or your card has expired please collect a
new card at ground floor E Pavallion -
Legare entrance before arriving at the Test
Centre. Phlebotomy services cannot be
provided without a valid JGH Hospital Card.
The Test Centre operates as a "drop-in"
service and patients are seen on a first-
come first-serve basis. No appointments
are made.
Peak hours are between 09h00 and 11h00,
when a 1-1.5 hour wait can be expected.
Patients must arrive with the Physician's
requisition form for the test. Tests cannot be
performed without a valid requisition.
24 hour urine collections, swabs and stool
samples may be dropped off at the Test
Centre, however please ensure that the
Specimen Containers are correctly labeled.
Fasting generally means no food or drinks
are to be ingested for 8-12 hours except for
water. Please consult your physician
regarding any medication you may be
taking.
The following phlebotomy services are
offered:
Location Days Times Remarks
Test Centre 1st Floor, Pavillion
E, Room 102
Mon - Thurs
Friday
07h30 - 20h00
07h30 - 16h00
No appointments
required.
Coagulation
Clinic
1st Floor, Pavillion
E, Room 103.
Monday
Wednesday
08h00 - 11h00
07h00 10h00
Appointments
pre-scheduled.
Endocrinology
1st Floor, Pavillion
E, Opposite the
elevators.
Monday - Friday 08h00 - 11h00Appointments
pre-scheduled.
Haematology 1st Floor, Pavillion
E, Room 103.1
Mon, Tues, Thur, Fri.
Wednesday
08h00 - 16h00
07h00 - 15h00
Appointments
pre-scheduled.
Oncology 7th Floor, Pavillion
E, Room 778 Monday - Friday 07h00 - 15h00
Appointments
pre-scheduled.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 8
Director of Professional Services
Laboratory Chief
Division Chief:Microbiology
Division Chief:Hematology and Transfusion
Division Chief:Biochemistry
Quality and Safety Officer
Microbiologists
HematologistsBiochemists
Chief TechnologistMicrobiology
Assistant Chief Technologist
Chief TechnologistTransfusion
Chief TechnologistCorelab
TechnicalCoordinators
PhlebotomistsClerks Medical Technologists Graduate Technologists
Medical TechnologistBlood Bank Clerks
Transfusion Nurseand Technologist
Medical TechnologistsGraduate Technologists
Senior Clerk
Medical Technologist (BG)
Laboratory Manager
TechnicalCoordinators
TechnicalCoordinators
Technical Coordinators
Department Organigram

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 9
Important Numbers General Enquiries (514) 340-8222 ext. 5094
Test Results
Biochemistry & Haematology ext. 8212
Microbiology ext. 8261
Blood Transfusion Services ext. 5072
Laboratory Manager
Mr Rocco Starnino ext. 5092
Laboratory Chief
Dr E. MacNamara ext. 5091 (Laboratory Chief and Medical Biochemist)
Section Heads
Dr E. MacNamara ext. 5091 (Section Chief Biochemistry)
Dr S. Caplan ext. 8207 (Section Chief Hematology & Transfusion Services)
Dr A Dascal ext. 2933 (Section Chief Microbiology)
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 10
Requisition Form The requisition form must be completed legibly.
The following patient information must be recorded:
Unit number or RAMQ number
Last Name and First Name
Date of birth
The following physician details must be recorded:
Name or code
Location
The following specimen information must be recorded
Date of sample collection
Time of sample collection
Check the box corresponding to the required test(s)
Additional tests can be requested in the space indicated
Specify copies to:

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 11
Remember, please complete the requisition legibly.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 12
Specimen ID & Rejection 1. Specimen containers must be
labelled legibly
Full name
Date of Birth
MRN or RAMQ number
Where applicable date, collection site,
start stop times
2. The Laboratory reserves the right to
reject unacceptable samples such as:
Samples which may have leaked during
transit
Unlabeled specimen container
Inadequate or illegible information on
the requisition form
Blood gas syringes with needles
attached
Sample obtained or transported
incorrectly, or received in an incorrect
container
Grossly contaminated exterior of sample
container or biohazard bag
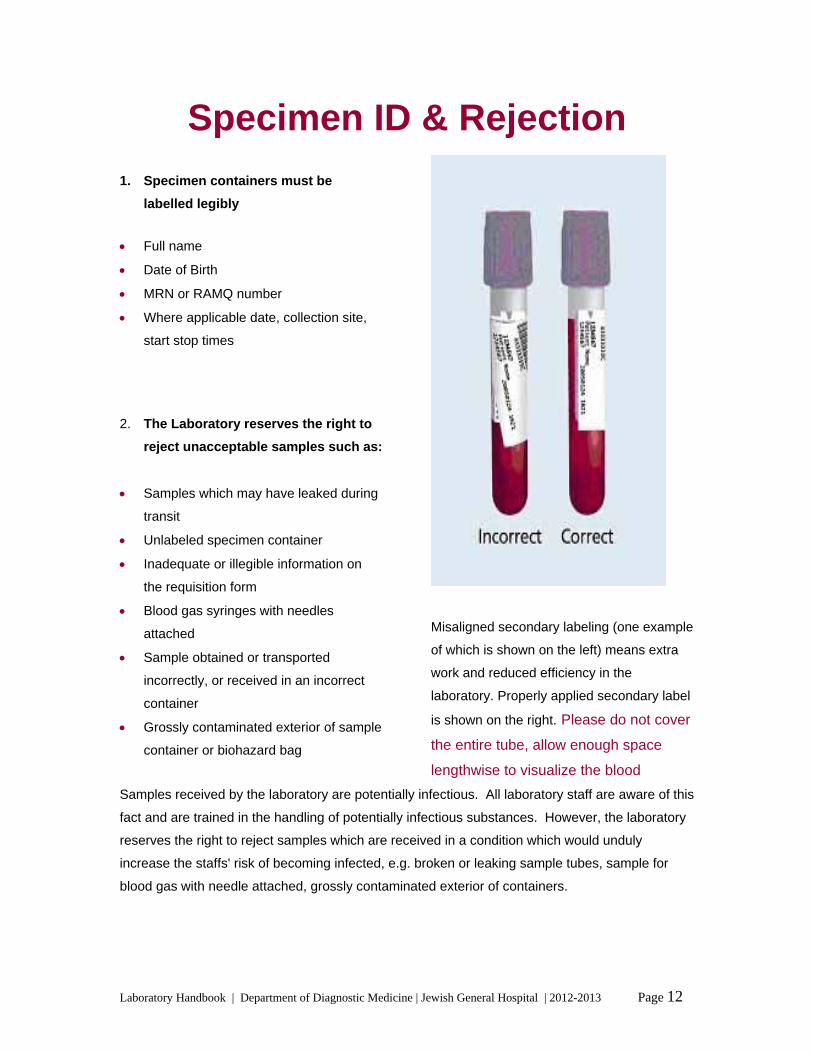
Misaligned secondary labeling (one example
of which is shown on the left) means extra
work and reduced efficiency in the
laboratory. Properly applied secondary label
is shown on the right. Please do not cover
the entire tube, allow enough space
lengthwise to visualize the blood
Samples received by the laboratory are potentially infectious. All laboratory staff are aware of this
fact and are trained in the handling of potentially infectious substances. However, the laboratory
reserves the right to reject samples which are received in a condition which would unduly
increase the staffs' risk of becoming infected, e.g. broken or leaking sample tubes, sample for
blood gas with needle attached, grossly contaminated exterior of containers.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 13
Biohazard specimen bags
1. Tubes containing blood must be placed
a biohazard specimen bag.
2. Urine specimens and other biological
fluids must be placed in separate
biohazard bags. i.e. Do not put a tube
of blood and a urine specimen in the
same bag.
3. Ensure that the urine containers are
tightly closed before being placed in the
bags.
4. The requisition accompanying the
specimen should be folded and placed
in the pouch on the outside of the bag.
Do not put the requisition in the same
compartment as the specimens.
5. The label identifying the patient must be
placed directly onto the specimens and
not on the bag. Specimens identified
only on the bag, will be regarded as not
identified and will be rejected by the
laboratory.
6. Make sure the bags are tightly closed
(same principle as "Ziploc" bags).

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 14
Specimen Delivery
1. Blood samples:
Make sure tubes are properly identified
Place in a plastic biohazard bag
Only use one bag per patient
Do not glue or staple the bag (do not
use elastic bands)
2. Urine or stool samples:
Make sure containers are properly
closed and identified
Place in a plastic biohazard bag, (1
urine specimen per bag)
Do not glue or staple the bag (do not
use elastic bands).
3. When sending specimens to the
Hospital from an outside location,
place all bags in a solid polystyrene
box.
The use of a refrigerant bag to keep
specimens cool during transport is
recommended, but the specimens
should not be in direct contact with the
refrigerant bag.
4. Label the box:
Apply a "Bio Hazard" sticker and
Clearly identify the institution sending
the specimens including address.
Samples are generally received in the
Laboratory via the following means:
A. Inpatient samples:
The messenger service. Samples are
picked up from the Nursing Stations.
Nurse aids and orderlies also deliver
specimens in certain situations (e.g.
STAT samples).
Pneumatic tube, delivers samples from
the Emergency Department (Red Unit,
Blue Unit and "Resuscitation") as well as
the Oncology Department. The tube
operates 24 hours a day. Specimens on
ice may also be sent via the pneumatic
tube, however the ice must be sealed in
a separate biohazard bag and then
placed with the sample into a second
biohazard bag and sealed. The
requisition slip must be placed in the
pouch of the second biohazard bag.
Microbiology samples may also be sent
via the pneumatic tubes, except blood
culture bottles which are delivered via
messengers.
Samples for the Blood Bank are
delivered by orderlies and messengers.
There is no pneumatic tube in Blood
Bank.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 15
STAT samples are delivered by hand to
the front window of the Laboratory.
B. Outpatient samples:
Samples from the Test Center, PAT,
Hematology Clinic and Endocrine Clinic
are picked up every 20 minutes and
delivered to the Laboratory.
Samples from the Herzl Family Practice
Center and ENT, Urology, Eye, Geriatric
and Methadone clinics are picked up at
approximately 09h00, 11h00, 13h00 and
15h00 and delivered to the Laboratory.
Samples from the Infectious Diseases
clinic are picked up every 30 min to 1
hour and delivered to the Laboratory.
CLSC's, Nursing Homes, etc make their
own arrangements for the samples to be
delivered to the Laboratory.
C. Research specimens: Person
responsible for the study arranges for
the samples to be delivered to the
Laboratory.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 16
Blood
1. Most biochemistry assays are performed on whole blood, plasma or serum. These samples
are obtained by collecting blood into tubes which may or may not contain various additives. It
is generally more economical and easier to collect blood into evacuated tubes.
2. Certain assays are very specific regarding the sample type and acceptable sample tubes are
indicated the Test Catalogue.
3. When collecting whole blood or blood samples which require plasma for analysis, the sample
tube containing anticoagulant must be gently inverted 6-8 times. This must be performed
immediately following collection to ensure the sample remains unclotted.
Please note: vigorous shaking will cause hemolysis and possible test interference. If required,
the sample may be centrifuged immediately and the plasma separated.
4. When serum is required, the sample must be allowed to clot for 20 - 30 min following
collection, before centrifugation. Clotting is generally complete within this time period but
may be prolonged if the patient is anticoagulated. Centrifugation, before clotting is complete,
will cause sample probe blockage and spurious results.
5. When multiple samples tubes are to be collected, the "order of draw” on the next page must
be adhered to in order to prevent contamination of serial tubes and consequent spurious
results.
6. Coagulation tubes (light blue top) MUST be filled to the indicated mark.
Never top-up a tube by transferring blood from one tube to another.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 17
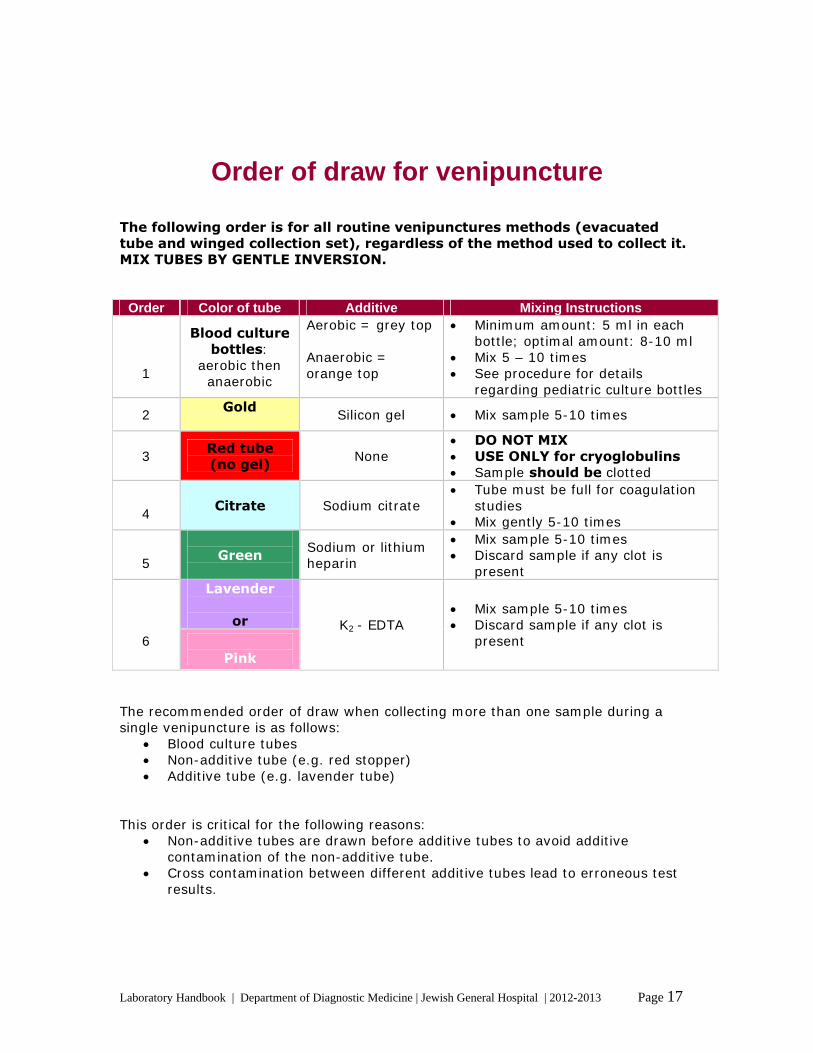
Order of draw for venipuncture The following order is for all routine venipunctures methods (evacuated tube and winged collection set), regardless of the method used to collect it. MIX TUBES BY GENTLE INVERSION.
Order Color of tube Additive Mixing Instructions
1
Blood culture bottles:
aerobic then anaerobic
Aerobic = grey top Anaerobic = orange top
Minimum amount: 5 ml in each bottle; optimal amount: 8-10 ml
Mix 5 – 10 times See procedure for details
regarding pediatric culture bottles
2 Gold
Silicon gel Mix sample 5-10 times
3 Red tube (no gel)
None DO NOT MIX USE ONLY for cryoglobulins Sample should be clotted
4
Citrate Sodium citrate Tube must be full for coagulation
studies Mix gently 5-10 times
5
Green
Sodium or lithium heparin
Mix sample 5-10 times Discard sample if any clot is
present Lavender
or
6
Pink
K2 - EDTA Mix sample 5-10 times Discard sample if any clot is
present
The recommended order of draw when collecting more than one sample during a single venipuncture is as follows:
Blood culture tubes Non-additive tube (e.g. red stopper) Additive tube (e.g. lavender tube)
This order is critical for the following reasons:
Non-additive tubes are drawn before additive tubes to avoid additive contamination of the non-additive tube.
Cross contamination between different additive tubes lead to erroneous test results.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 18
Results Reporting
As soon as test results are authorized in the
laboratory, they are available on the
laboratory computer terminals in the ward.
Hardcopies of in-patient results are printed
once a week and distributed to the wards.
Hardcopies of urgent results are printed on
the ward printer immediately after
verification.
Critical results phoned to the ward are also
printed on the ward printer following
verification.
When a patient is discharged, a cumulative
report of all the patient's results during that
stay is printed in Medical Records for
placement in the patient's hospital chart.
Outpatient results are printed daily and
mailed to the requesting clinician. The
laboratory also faxes results (replacing the
hardcopy) daily to certain clinics and doctors
who have arranged for this service with the
laboratory.
Whilst the laboratory performs internal and
external quality assurance throughout the
day, it is possible for random errors to
occur. Following technical validation it is
therefore possible for inaccurate results to
be released even though they have passed
through various checks and flags.
In this situation, the clinician is the best
person to detect these errors. Although
these errors are extremely rare, should the
situation arise where results do not agree
with the clinical condition, please contact the
laboratory and report the disagreement. We
will then be able to retest the sample if
possible and investigate a possible error.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 19
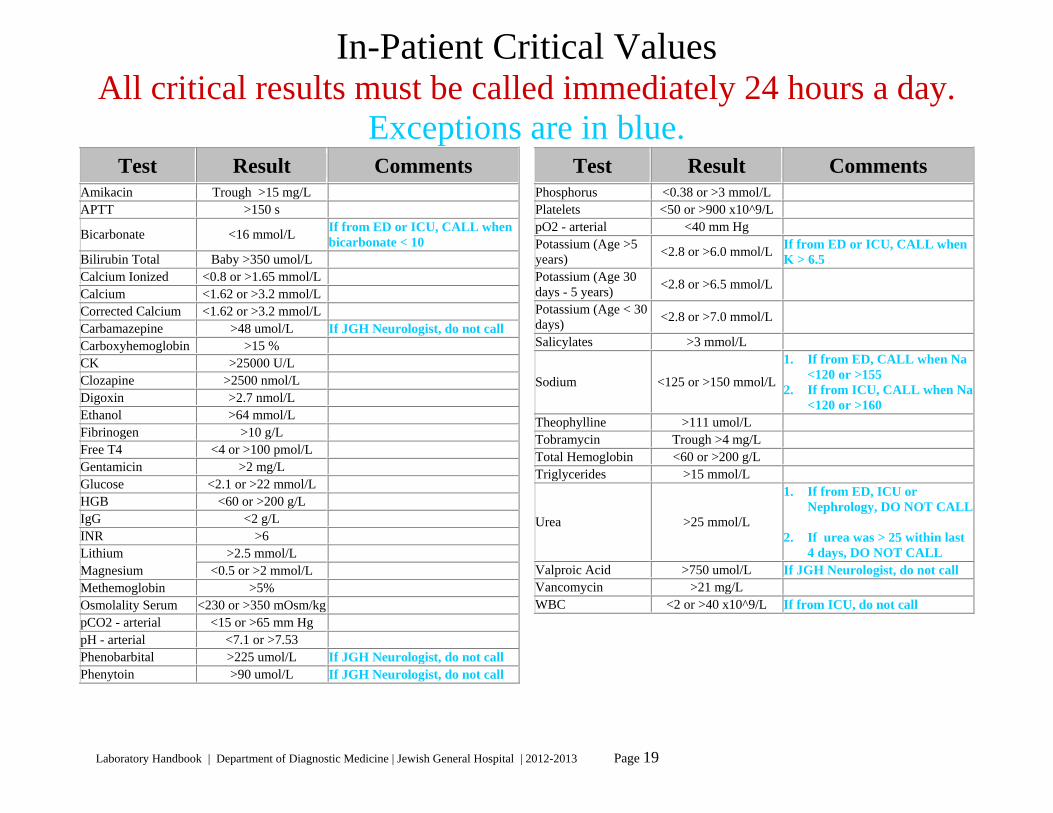
In-Patient Critical Values All critical results must be called immediately 24 hours a day.
Exceptions are in blue.Test Result Comments
Amikacin Trough >15 mg/L APTT >150 s
Bicarbonate <16 mmol/L If from ED or ICU, CALL when bicarbonate < 10
Bilirubin Total Baby >350 umol/L Calcium Ionized <0.8 or >1.65 mmol/L Calcium <1.62 or >3.2 mmol/L Corrected Calcium <1.62 or >3.2 mmol/L Carbamazepine >48 umol/L If JGH Neurologist, do not call Carboxyhemoglobin >15 % CK >25000 U/L Clozapine >2500 nmol/L Digoxin >2.7 nmol/L Ethanol >64 mmol/L Fibrinogen >10 g/L Free T4 <4 or >100 pmol/L Gentamicin >2 mg/L Glucose <2.1 or >22 mmol/L HGB <60 or >200 g/L IgG <2 g/L INR >6 Lithium >2.5 mmol/L Magnesium <0.5 or >2 mmol/L Methemoglobin >5% Osmolality Serum <230 or >350 mOsm/kg pCO2 - arterial <15 or >65 mm Hg pH - arterial <7.1 or >7.53 Phenobarbital >225 umol/L If JGH Neurologist, do not call Phenytoin >90 umol/L If JGH Neurologist, do not call
Test Result Comments Phosphorus <0.38 or >3 mmol/L Platelets <50 or >900 x10^9/L pO2 - arterial <40 mm Hg Potassium (Age >5 years)
<2.8 or >6.0 mmol/L If from ED or ICU, CALL when K > 6.5
Potassium (Age 30 days - 5 years)
<2.8 or >6.5 mmol/L
Potassium (Age < 30 days)
<2.8 or >7.0 mmol/L
Salicylates >3 mmol/L
Sodium <125 or >150 mmol/L
1. If from ED, CALL when Na <120 or >155
2. If from ICU, CALL when Na <120 or >160
Theophylline >111 umol/L Tobramycin Trough >4 mg/L Total Hemoglobin <60 or >200 g/L Triglycerides >15 mmol/L
Urea >25 mmol/L
1. If from ED, ICU or Nephrology, DO NOT CALL
2. If urea was > 25 within last
4 days, DO NOT CALL Valproic Acid >750 umol/L If JGH Neurologist, do not call Vancomycin >21 mg/L WBC <2 or >40 x10^9/L If from ICU, do not call
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 20
Res
ult b
etw
een
17h0
0-08
h00
call
Imm
edia
tely
Imm
edia
tely
Nex
t mor
ning
*N
ext m
orni
ng *
Nex
t mor
ning
*N
ext m
orni
ng *
Imm
edia
tely
Nex
t mor
ning
*Im
med
iate
lyIm
med
iate
ly
Nex
t mor
ning
*Im
med
iate
lyIm
med
iate
lyIm
med
iate
ly
Nex
t mor
ning
*N
ext m
orni
ng *
Nex
t mor
ning
*N
ext m
orni
ng *
Nex
t mor
ning
*N
ext m
orni
ng *
Nex
t mor
ning
*N
ext m
orni
ng *
Imm
edia
tely
**
Imm
edia
tely
**
Imm
edia
tely
**
Imm
edia
tely
**
Imm
edia
tely
**
Res
ult
<15
or
>65
mm
Hg
<7.
1 or
>7.
53>
225
umol
/L>
90 u
mol
/L<
0.38
mm
ol/L
>3
mm
ol/L
<20
20-5
0 or
>90
0 x1
0^9/
L<
40 m
m H
g<
2.2
or >
6.5
mm
ol/L
2.2-
2.8
or 6
.0-6
.5 m
mol
/L<
2.8
or >
6.5
mm
ol/L
<2.
8 or
>7.
0 m
mol
/L<
120
or >
160
mm
ol/L
120-
125
or 1
50-1
59 m
mol
/L>
111
umol
/LC
reux
>4
mg/
L>
15 m
mol
/L>
25 m
mol
/L>
750
umol
/LC
reux
>21
mg/
L<
2 or
>40
x10
^9/L
Pos
itif
Pos
itif
Pos
itif
Leg
ione
lla,
Cry
poto
, Mal
aria
pos
itif
Pos
itif
Hem
atol
ogy
Tes
t M
icro
biol
ogy
Tes
t
Bio
chem
istr
y T
est
Tes
t
pCO
2 -
arte
riel
pH -
art
erie
lP
héno
barb
ital
Phé
nyto
ine
Pla
quet
tes
pO2
- ar
teri
el
Pot
assi
um (
Age
30
j - 5
ans
)P
otas
sium
(A
ge <
30 j)
Thé
ophy
llin
eT
obra
myc
in
Tri
glyc
érid
esU
rée
Val
proï
que
acid
eV
anco
myc
ine
WB
C /
Glo
bule
s bl
ancs
Hem
ocul
ture
sF
rott
is L
CR
ou
autr
e si
te s
téri
lF
rott
is B
AA
R (
AF
B)
/ Mal
aria
Tes
t d'a
ntig
ène
Cer
tain
es te
st m
oléc
ulai
re
Res
ult b
etw
een
17h0
0-08
h00
call
Nex
t mor
ning
*N
ext m
orni
ng *
Imm
edia
tely
Nex
t mor
ning
*Im
med
iate
lyIm
med
iate
lyIm
med
iate
lyIm
med
iate
ly
Nex
t mor
ning
*Im
med
iate
lyIm
med
iate
ly
Nex
t mor
ning
*N
ext m
orni
ng *
Imm
edia
tely
Nex
t mor
ning
*N
ext m
orni
ng *
Nex
t mor
ning
*Im
med
iate
ly
Nex
t mor
ning
*N
ext m
orni
ng *
Nex
t mor
ning
*Im
med
iate
ly
Nex
t mor
ning
*Im
med
iate
ly
Nex
t mor
ning
*Im
med
iate
lyIm
med
iate
ly
Res
ult
Cre
ux >
15 m
g/L
>15
0 s
<10
mm
ol/L
10-1
6 m
mol
/LB
ébé
>35
0 um
ol/L
<0.
8 or
>1.
65 m
mol
/L<
1.62
or
>3.
2 m
mol
/L<
1.62
or
>3.
2 m
mol
/L>
48 u
mol
/L>
15 %
>25
000
U/L
>25
00 n
mol
/L>
2.7
nmol
/L>
80 m
mol
/L>
10 g
/L<
4 or
>10
0 pm
ol/L
Cre
ux >
2 m
g/L
<2.
1 or
>28
mm
ol/L
22.1
- 28
mm
ol/L
<60
or
>20
0 g/
L<
2 g/
L>
6>
2.5
mm
ol/L
<0.
3 or
>3
mm
ol/L
0.3-
0.5
or 2
-3 m
mol
/L>
5%<
230
or >
350
mO
sm/k
g
Tes
t
Am
ikac
ine
AP
TT
Bil
irub
ine
tota
leC
alci
um io
nisé
Cal
cium
Cal
cium
cor
rigé
Car
bam
azép
ine
Car
boxy
hém
oglo
bine
CK
C
loza
pine
D
igox
ine
Éth
anol
Fib
rino
gène
FT
4/T
hyro
xine
libr
eG
enta
mic
ine
Hém
oglo
bine
IgG
IN
R /
RN
IL
ithi
um
Mét
hem
oglo
bine
Osm
olal
ité
séru
m
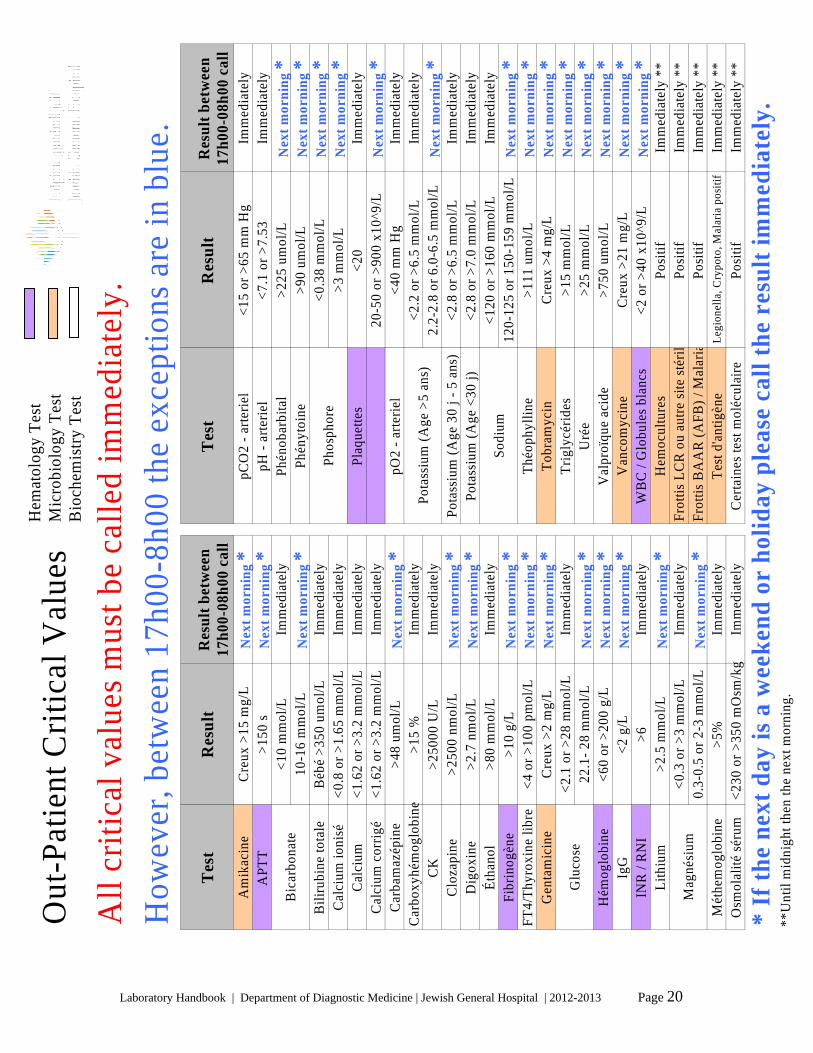
Out
-Pat
ient
Cri
tica
l Val
ues
Pot
assi
um (
Age
>5
ans)
Glu
cose
Mag
nési
um
Sod
ium
Bic
arbo
nate
Pho
spho
re
All
cri
tica
l val
ues
mus
t be
call
ed im
med
iate
ly.
* If
the
next
day
is a
wee
kend
or
holid
ay p
leas
e ca
ll th
e re
sult
imm
edia
tely
.**
Unt
il m
idni
ght t
hen
the
next
mor
ning
.
How
ever
, bet
wee
n 17
h00-
8h00
the
exce
ptio
ns a
re in
blu
e.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 21
Therapeutic Drug Monitoring
Therapeutic drug monitoring is most useful
when the drug in question has a low
therapeutic index and is used chronically.
Measurement may be of value in
assessment of compliance, therapeutic
dosing adjustment and confirmation of
clinical toxicity. It is important to note that
many factors may influence the
pharmacokinetics of a particular drug e.g.
protein binding, co-administration of other
drugs, pharmacogenetics.
Some patients may exhibit toxic effects at
concentrations less than the upper limit of
the therapeutic range.
Interpretation of a drug level is
dependant on the time the sample is
collected relative to the dosing time;
please indicate these parameters on the
requisition form.
Drug Therapeutic
Range Units Half life Sampling Time
Protein binding
Time to steady state
Carbamazepine 15-50 umol/L 12-17 hrs after repeated dosing
pre-dose ~80% 2-6 days
Digoxin 1.0-2.6 nmol/L adults 36-48 hrs 1 > 6hrs post-dose 20-30% 5 -10 days
Gentamicin trough 0.5-2 mg/L 2-3 hrs 2 trough-30 min pre dose
negligible -
0.6-1.2 mmol/Lyoung adult 18-24 hrs
12 hrs post dose negligible 3-7 days Lithium
0.6-1.2 mmol/L elderly 30-36 hrs 12 hrs post dose negligible 3-7 days Phenobarbital 65-170 umol/L 79-93 hrs pre-dose 40-60% 15-25 days
40-80 umol/L 3 pre-dose 90-95% 7-12 days Phenytoin
<3mth 39-67 umol/L children 3-4 hrs 4 pre-dose ~50% 2-3 days Theophylline adult 55-110 umol/L adults 9 hrs 4 pre-dose ~50% 2-3 days Valproic acid 350-700 umol/L 6-16 hrs in adults pre-dose ~90% 2-4 days
Vancomycin trough 10-15 mg/L 4-6 hrs 5 trough-30 min pre dose
~30% (variable)
-
1 Increases up to 6 days in renal impairment. 2 In renal failure half-life can be 24 hrs or longer. 3 Phenytoin does not obey first order kinetics at therapeutic concentrations therefore a true half-life cannot be calculated. In adults the apparent half-life is 18-36 hrs and in children 12-22 hrs. 4 In smokers half-life is 3 - 4 hrs, neonates and adults with CHF 20-30 hrs depending on degree of liver impairment. 5 In the elderly or those with renal impairment, half-life can be as long as 6 days.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 22
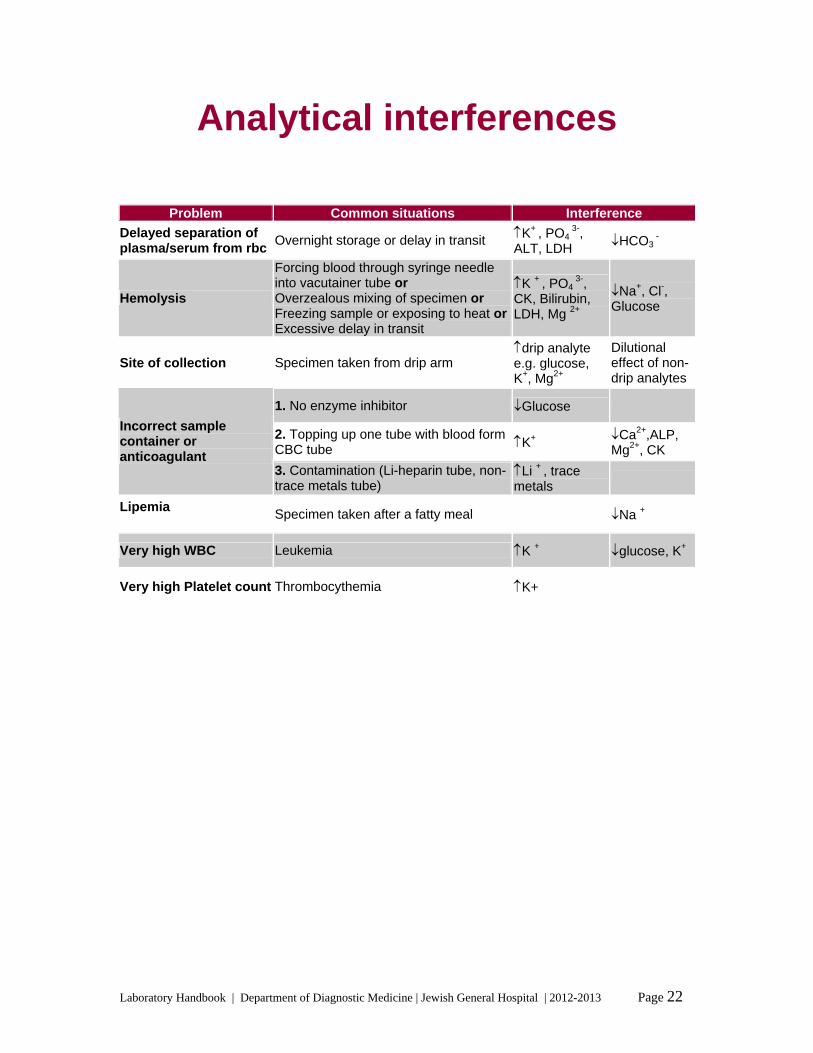
Analytical interferences
Problem Common situations Interference
Delayed separation of plasma/serum from rbc
Overnight storage or delay in transit K+ , PO4 3-,
ALT, LDH HCO3
-
Hemolysis
Forcing blood through syringe needle into vacutainer tube or Overzealous mixing of specimen or Freezing sample or exposing to heat orExcessive delay in transit
K + , PO4 3-,
CK, Bilirubin, LDH, Mg 2+
Na+, Cl-, Glucose
Site of collection Specimen taken from drip arm drip analyte e.g. glucose, K+, Mg2+
Dilutional effect of non-drip analytes
1. No enzyme inhibitor Glucose
2. Topping up one tube with blood form CBC tube K+
Ca2+,ALP, Mg2+, CK
Incorrect sample container or anticoagulant
3. Contamination (Li-heparin tube, non-trace metals tube)
Li + , trace metals
Lipemia
Specimen taken after a fatty meal Na +
Very high WBC Leukemia K + glucose, K+
Very high Platelet count Thrombocythemia K+
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 23
Near patient testing
Glucometers are available on the wards.
The Accu-Chek Inform glucometers are
linked to the hospital computer system as
well as the laboratory information system.
Patients admitted to a particular ward will
appear on the Inform glucometers located in
that ward.
The laboratory is responsible for monitoring
the quality control of the devices.
Nursing staff are responsible for performing
the QC on the instruments.
Once a test is performed, the result is
available on the instrument. However, only
when the Inform glucometer is docked will
the results be transmitted to the LIS and
made available on the laboratory computer
terminals on the ward.
The laboratory provides training of nursing
staff and can be contacted at ext 5094. The
clinical nurse instructor or resource nurse on
each unit, who have been certified as
trainers by the laboratory, may also train
nursing staff.
General support for Accu-Chek Inform
glucometers is available at ext 5094; ask for
the person on-call for these devices.
In addition, near patient testing includes
fecal occult blood, urine pregnancy testing,
blood gas analysers, jaundice meter, and
activated clotting time.
Under Quebec Law, the laboratory is
required to supervise near patient testing.
The laboratory is currently producing
certification videos for near patient testing
and will include the above tests and online
certification for health care workers.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 24
Research and Trials
To arrange for testing of samples for research and clinical trials:
Please contact
Rocco Starnino at ext. 5092
or
via email at [email protected]
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 25
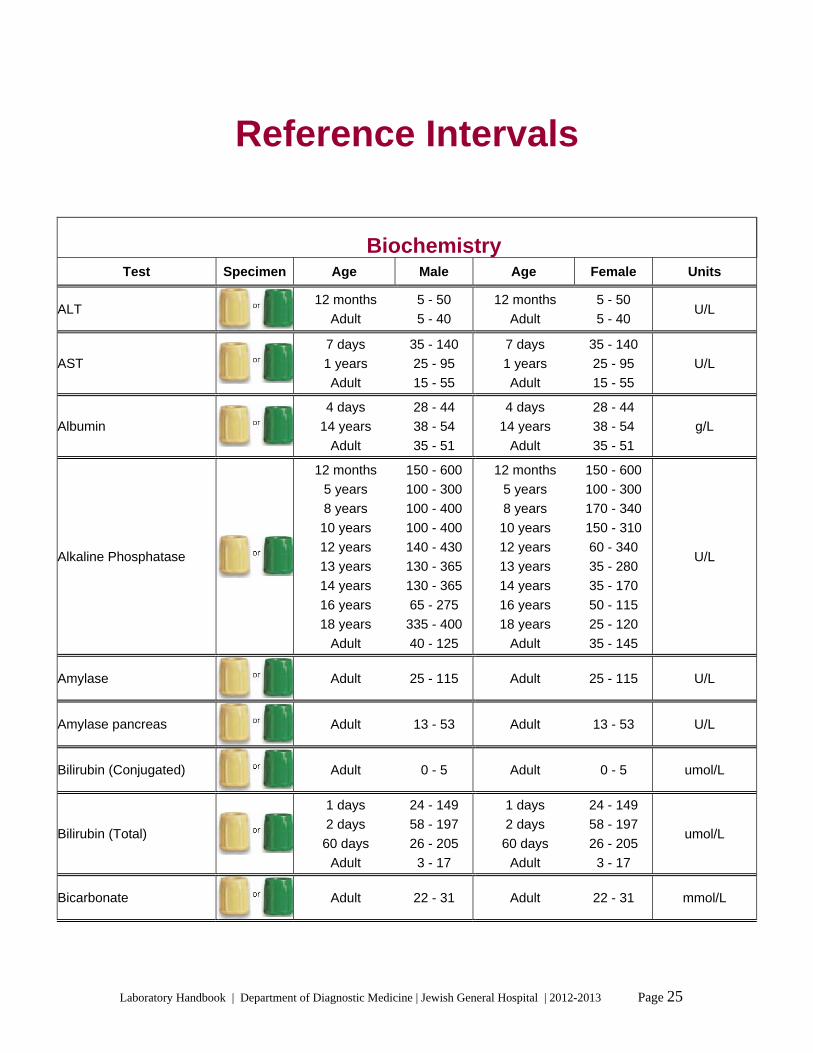
Reference Intervals
Biochemistry
Test Specimen Age Male Age Female Units
ALT 12 months 5 - 50
Adult 5 - 40
12 months 5 - 50
Adult 5 - 40 U/L
AST
7 days 35 - 140
1 years 25 - 95
Adult 15 - 55
7 days 35 - 140
1 years 25 - 95
Adult 15 - 55
U/L
Albumin
4 days 28 - 44
14 years 38 - 54
Adult 35 - 51
4 days 28 - 44
14 years 38 - 54
Adult 35 - 51
g/L
Alkaline Phosphatase
12 months 150 - 600
5 years 100 - 300
8 years 100 - 400
10 years 100 - 400
12 years 140 - 430
13 years 130 - 365
14 years 130 - 365
16 years 65 - 275
18 years 335 - 400
Adult 40 - 125
12 months 150 - 600
5 years 100 - 300
8 years 170 - 340
10 years 150 - 310
12 years 60 - 340
13 years 35 - 280
14 years 35 - 170
16 years 50 - 115
18 years 25 - 120
Adult 35 - 145
U/L
Amylase Adult 25 - 115 Adult 25 - 115 U/L
Amylase pancreas Adult 13 - 53 Adult 13 - 53 U/L
Bilirubin (Conjugated) Adult 0 - 5 Adult 0 - 5 umol/L
Bilirubin (Total)
1 days 24 - 149
2 days 58 - 197
60 days 26 - 205
Adult 3 - 17
1 days 24 - 149
2 days 58 - 197
60 days 26 - 205
Adult 3 - 17
umol/L
Bicarbonate Adult 22 - 31 Adult 22 - 31 mmol/L
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 26
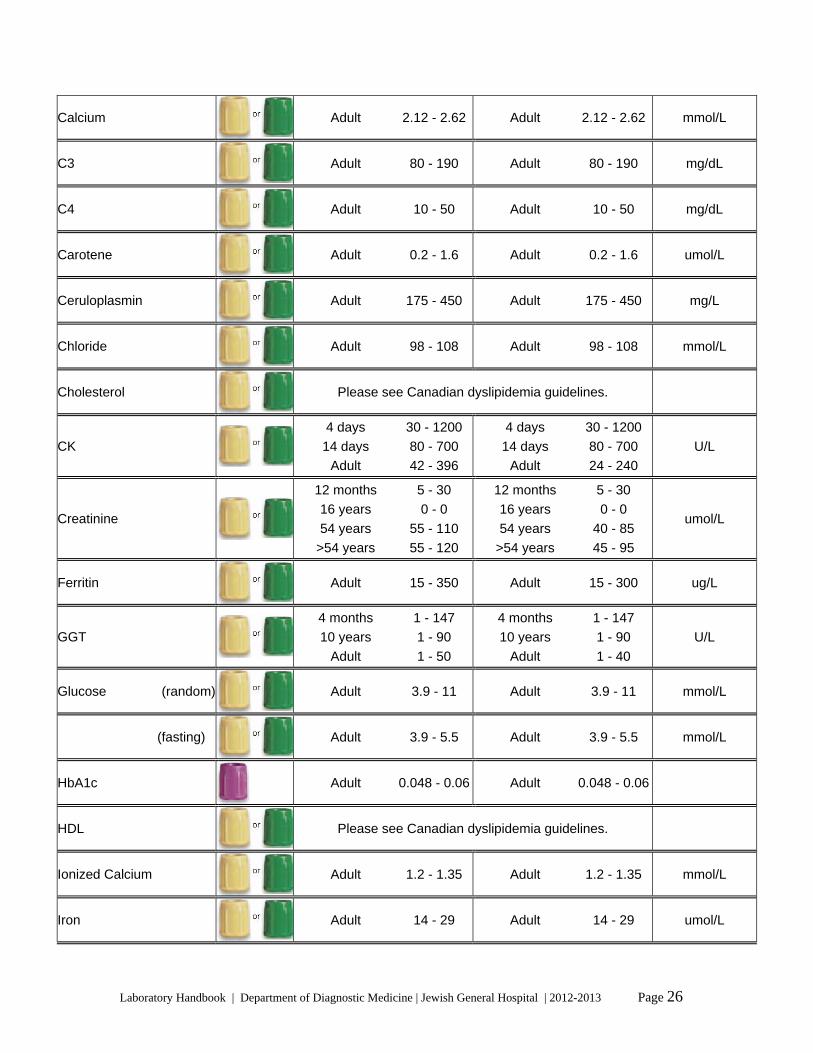
Calcium Adult 2.12 - 2.62 Adult 2.12 - 2.62 mmol/L
C3 Adult 80 - 190 Adult 80 - 190 mg/dL
C4 Adult 10 - 50 Adult 10 - 50 mg/dL
Carotene Adult 0.2 - 1.6 Adult 0.2 - 1.6 umol/L
Ceruloplasmin Adult 175 - 450 Adult 175 - 450 mg/L
Chloride Adult 98 - 108 Adult 98 - 108 mmol/L
Cholesterol Please see Canadian dyslipidemia guidelines.
CK
4 days 30 - 1200
14 days 80 - 700
Adult 42 - 396
4 days 30 - 1200
14 days 80 - 700
Adult 24 - 240
U/L
Creatinine
12 months 5 - 30
16 years 0 - 0
54 years 55 - 110
>54 years 55 - 120
12 months 5 - 30
16 years 0 - 0
54 years 40 - 85
>54 years 45 - 95
umol/L
Ferritin Adult 15 - 350 Adult 15 - 300 ug/L
GGT
4 months 1 - 147
10 years 1 - 90
Adult 1 - 50
4 months 1 - 147
10 years 1 - 90
Adult 1 - 40
U/L
Glucose (random) Adult 3.9 - 11 Adult 3.9 - 11 mmol/L
(fasting) Adult 3.9 - 5.5 Adult 3.9 - 5.5 mmol/L
HbA1c
Adult 0.048 - 0.06 Adult 0.048 - 0.06
HDL Please see Canadian dyslipidemia guidelines.
Ionized Calcium Adult 1.2 - 1.35 Adult 1.2 - 1.35 mmol/L
Iron Adult 14 - 29 Adult 14 - 29 umol/L

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 27
Lactic Acid on ice
Adult 0.5 - 2.5 Adult 0.5 - 2.5 mmol/L
LDH
4 days 290 - 775
10 days 545 - 2000
24 months 180 - 430
12 years 110 - 295
Adult 110 - 220
4 days 290 - 775
10 days 545 - 2000
24 months 180 - 430
12 years 110 - 295
Adult 110 - 220
U/L
LDL Please see Canadian dyslipidemia guidelines.
Lipase Adult 0 - 60 Adult 0 - 60 U/L
Magnesium
4 days 0.6 - 0.9
5 months 0.65 - 1.05
6 years 0.71 - 0.95
12 years 0.69 - 0.87
20 years 0.67 - 0.89
Adult 0.7 - 1.23
4 days 0.6 - 0.9
5 months 0.65 - 1.05
6 years 0.71 - 0.95
12 years 0.69 - 0.87
20 years 0.67 - 0.89
Adult 0.7 - 1.23
mmol/L
Osmolarity Adult 280 - 300 Adult 280 - 300 mOsm/kg
Phosphorus
10 days 1.45 - 2.91
24 months 1.45 - 2.16
12 years 1.45 - 1.78
14 years 1.05 - 1.8
16 years 0.9 - 1.55
Adult 0.7 - 1.45
10 days 1.45 - 2.91
24 months 1.45 - 2.16
12 years 1.45 - 1.78
14 years 0.9 - 1.55
16 years 0.9 - 1.55
Adult 0.7 - 1.45
mmol/L
Potassium
12 months 3.5 - 6.5
5 years 3.6 - 6.2
Adult 3.5 - 5.5
12 months 3.5 - 6.5
5 years 3.6 - 6.2
Adult 3.5 - 5.5
mmol/L
Prealbumin Adult 0.11 - 0.41 Adult 0.11 - 0.41 g/L
Sodium Adult 134 - 144 Adult 134 - 144 mmol/L
Saturation Adult 0.15 - 0.5 Adult 0.15 - 0.5
TIBC Adult 52 - 72 Adult 52 - 72 umol/L
Total Protein
1 weeks 44 - 76
7 months 46 - 74
1 years 51 - 73
Adult 60 - 80
1 weeks 44 - 76
7 months 46 - 76
1 years 51 - 73
Adult 60 - 80
g/L
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 28
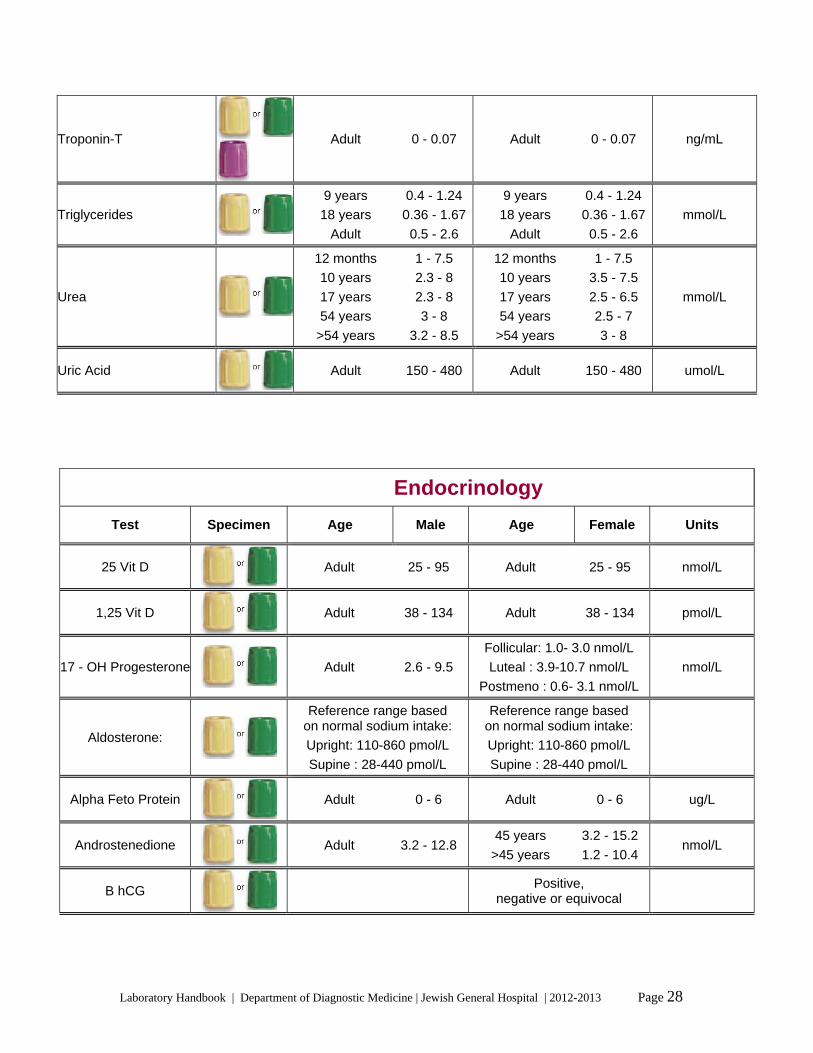
Troponin-T
Adult 0 - 0.07 Adult 0 - 0.07 ng/mL
Triglycerides
9 years 0.4 - 1.24
18 years 0.36 - 1.67
Adult 0.5 - 2.6
9 years 0.4 - 1.24
18 years 0.36 - 1.67
Adult 0.5 - 2.6
mmol/L
Urea
12 months 1 - 7.5
10 years 2.3 - 8
17 years 2.3 - 8
54 years 3 - 8
>54 years 3.2 - 8.5
12 months 1 - 7.5
10 years 3.5 - 7.5
17 years 2.5 - 6.5
54 years 2.5 - 7
>54 years 3 - 8
mmol/L
Uric Acid Adult 150 - 480 Adult 150 - 480 umol/L
Endocrinology
Test Specimen Age Male Age Female Units
25 Vit D
Adult 25 - 95 Adult 25 - 95 nmol/L
1,25 Vit D
Adult 38 - 134 Adult 38 - 134 pmol/L
17 - OH Progesterone
Adult 2.6 - 9.5
Follicular: 1.0- 3.0 nmol/L
Luteal : 3.9-10.7 nmol/L
Postmeno : 0.6- 3.1 nmol/L
nmol/L
Aldosterone:
Reference range based on normal sodium intake:
Upright: 110-860 pmol/L
Supine : 28-440 pmol/L
Reference range based on normal sodium intake:
Upright: 110-860 pmol/L
Supine : 28-440 pmol/L
Alpha Feto Protein
Adult 0 - 6 Adult 0 - 6 ug/L
Androstenedione
Adult 3.2 - 12.8 45 years 3.2 - 15.2
>45 years 1.2 - 10.4 nmol/L
B hCG
Positive,
negative or equivocal

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 29
CA 125
Adult 0 - 35 Adult 0 - 35 U/mL
CEA
Adult 0 - 3 Adult 0 - 3 ug/L
DHEA-S
4 years 0.2 - 0.6
7 years 0.1 - 5
9 years 0.3 - 2.6
11 years 0.4 - 2
12 years 0.5 - 4.1
13 years 0.5 - 9.3
14 years 0.6 - 6.6
15 years 0.5 - 7.8
16 years 1.6 - 8.4
17 years 1.3 - 9.7
18 years 2.8 - 9.3
20 years 2.9 - 12
30 years 7.6 - 17.4
40 years 3.3 - 14.1
50 years 2.6 - 14.4
60 years 1.9 - 8.4
70 years 1.1 - 7.9
80 years 0.8 - 4.7
>80 years 2.2 - 15.2
4 years 0.2 - 2.1
7 years 0.2 - 1
9 years 0.4 - 1.8
11 years 0.4 - 4.3
12 years 0.3 - 2.7
13 years 0.8 - 4.8
14 years 0.6 - 4.5
15 years 0.9 - 8.2
16 years 1.1 - 7.8
17 years 1.6 - 9.6
18 years 2.6 - 10.8
20 years 3.9 - 10.7
30 years 1.8 - 10.3
40 years 1.2 - 7.3
50 years 0.9 - 6.5
60 years 0.7 - 5.4
70 years 0.4 - 3.5
80 years 0.5 - 2.4
>80 years 0.9 - 11.7
umol/L
Estradiol
Prepubertal: 0-130
Adult male : 55-165
Prepubertal: 0- 130
Early follicular: 90- 715
Preovulatory: 240-1510
Luteal : 147- 950
Menopausal: 0- 145
pmol/L
FSH
Adult 1.6 - 11
Follicular : 3.3-11.3 U/L
Pre-ovul.: 5.0-16.0 U/L
Ovulation: 5.2-20.4 U/L
Luteal: 1.8-8.2 U/L
Menopausal: 48.6-143.9 U/L
U/L
Insulin
16 years 0 - 0
65 years 40 - 100
16 years 0 - 0
65 years 40 - 100 pmol/L
LH
Adult 0.8 - 6.1
Follicular: 1.6- 7.9 U/L
Pre-ovulation: 7.7-23.1 U/L
Ovulation:13.2-82.7 U/L
Luteal: 0.7- 9.9 U/L
Menopausal:13.2-45.7 U/L
U/L
PTH
Adult 10 - 70 Adult 10 - 70 ng/L
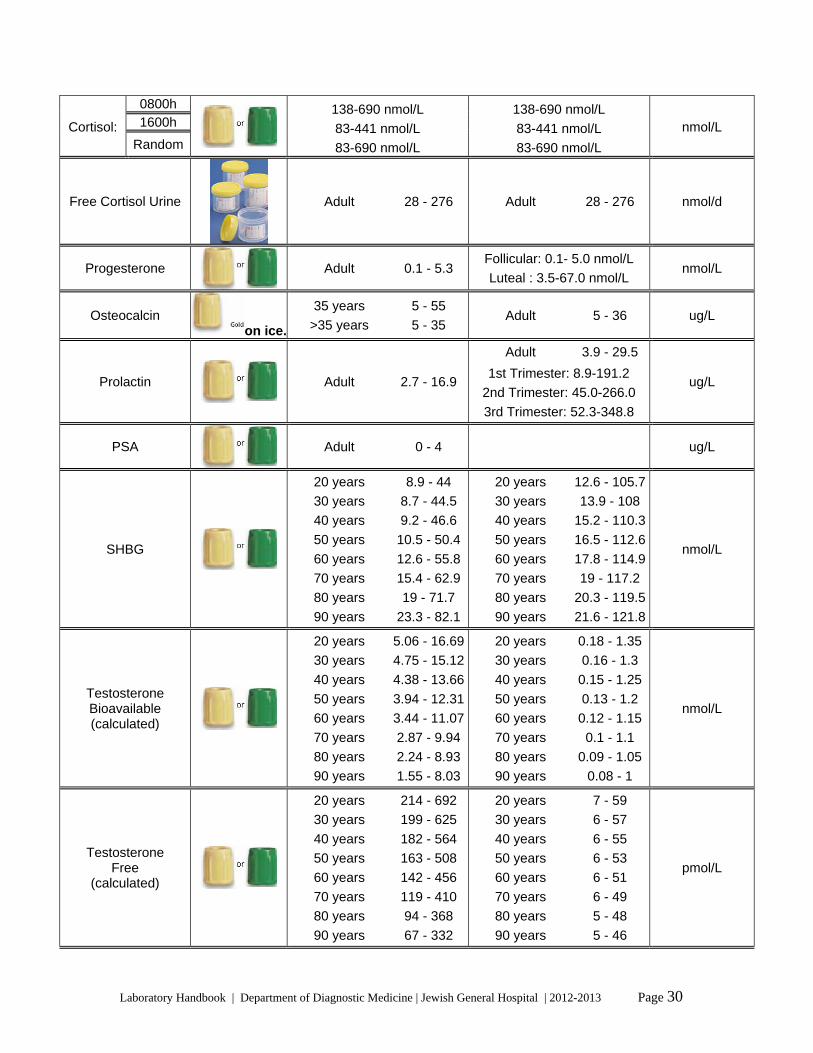
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 30
0800h 1600h Cortisol:
Random
138-690 nmol/L
83-441 nmol/L
83-690 nmol/L
138-690 nmol/L
83-441 nmol/L
83-690 nmol/L
nmol/L
Free Cortisol Urine
Adult 28 - 276 Adult 28 - 276 nmol/d
Progesterone
Adult 0.1 - 5.3 Follicular: 0.1- 5.0 nmol/L
Luteal : 3.5-67.0 nmol/L nmol/L
Osteocalcin on ice.
35 years 5 - 55
>35 years 5 - 35 Adult 5 - 36 ug/L
Prolactin
Adult 2.7 - 16.9
Adult 3.9 - 29.5
1st Trimester: 8.9-191.2
2nd Trimester: 45.0-266.0
3rd Trimester: 52.3-348.8
ug/L
PSA
Adult 0 - 4 ug/L
SHBG
20 years 8.9 - 44
30 years 8.7 - 44.5
40 years 9.2 - 46.6
50 years 10.5 - 50.4
60 years 12.6 - 55.8
70 years 15.4 - 62.9
80 years 19 - 71.7
90 years 23.3 - 82.1
20 years 12.6 - 105.7
30 years 13.9 - 108
40 years 15.2 - 110.3
50 years 16.5 - 112.6
60 years 17.8 - 114.9
70 years 19 - 117.2
80 years 20.3 - 119.5
90 years 21.6 - 121.8
nmol/L
Testosterone Bioavailable (calculated)
20 years 5.06 - 16.69
30 years 4.75 - 15.12
40 years 4.38 - 13.66
50 years 3.94 - 12.31
60 years 3.44 - 11.07
70 years 2.87 - 9.94
80 years 2.24 - 8.93
90 years 1.55 - 8.03
20 years 0.18 - 1.35
30 years 0.16 - 1.3
40 years 0.15 - 1.25
50 years 0.13 - 1.2
60 years 0.12 - 1.15
70 years 0.1 - 1.1
80 years 0.09 - 1.05
90 years 0.08 - 1
nmol/L
Testosterone Free
(calculated)
20 years 214 - 692
30 years 199 - 625
40 years 182 - 564
50 years 163 - 508
60 years 142 - 456
70 years 119 - 410
80 years 94 - 368
90 years 67 - 332
20 years 7 - 59
30 years 6 - 57
40 years 6 - 55
50 years 6 - 53
60 years 6 - 51
70 years 6 - 49
80 years 5 - 48
90 years 5 - 46
pmol/L
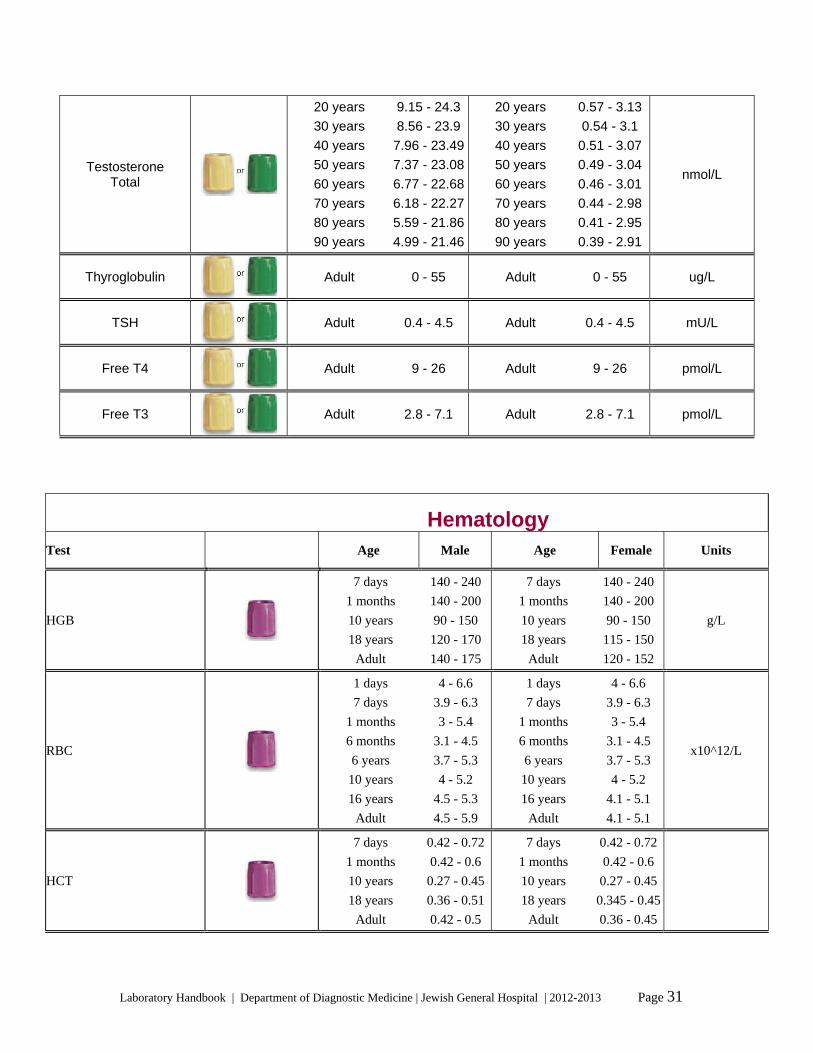
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 31
Testosterone Total
20 years 9.15 - 24.3
30 years 8.56 - 23.9
40 years 7.96 - 23.49
50 years 7.37 - 23.08
60 years 6.77 - 22.68
70 years 6.18 - 22.27
80 years 5.59 - 21.86
90 years 4.99 - 21.46
20 years 0.57 - 3.13
30 years 0.54 - 3.1
40 years 0.51 - 3.07
50 years 0.49 - 3.04
60 years 0.46 - 3.01
70 years 0.44 - 2.98
80 years 0.41 - 2.95
90 years 0.39 - 2.91
nmol/L
Thyroglobulin
Adult 0 - 55 Adult 0 - 55 ug/L
TSH
Adult 0.4 - 4.5 Adult 0.4 - 4.5 mU/L
Free T4
Adult 9 - 26 Adult 9 - 26 pmol/L
Free T3
Adult 2.8 - 7.1 Adult 2.8 - 7.1 pmol/L
Hematology
Test Age Male Age Female Units
HGB
7 days 140 - 240 1 months 140 - 200 10 years 90 - 150 18 years 120 - 170
Adult 140 - 175
7 days 140 - 240 1 months 140 - 200 10 years 90 - 150 18 years 115 - 150
Adult 120 - 152
g/L
RBC
1 days 4 - 6.6 7 days 3.9 - 6.3
1 months 3 - 5.4 6 months 3.1 - 4.5 6 years 3.7 - 5.3 10 years 4 - 5.2 16 years 4.5 - 5.3
Adult 4.5 - 5.9
1 days 4 - 6.6 7 days 3.9 - 6.3
1 months 3 - 5.4 6 months 3.1 - 4.5 6 years 3.7 - 5.3 10 years 4 - 5.2 16 years 4.1 - 5.1
Adult 4.1 - 5.1
x10^12/L
HCT
7 days 0.42 - 0.72
1 months 0.42 - 0.6 10 years 0.27 - 0.45
18 years 0.36 - 0.51
Adult 0.42 - 0.5
7 days 0.42 - 0.72
1 months 0.42 - 0.6 10 years 0.27 - 0.45
18 years 0.345 - 0.45
Adult 0.36 - 0.45

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 32
MCV
1 days 95 - 121 7 days 88 - 126
1 months 85 - 123 6 months 74 - 108 4 years 70 - 88 6 years 75 - 87 10 years 77 - 95 16 years 78 - 98
Adult 80 - 96
1 days 95 - 121 7 days 88 - 126
1 months 85 - 123 6 months 74 - 108 4 years 70 - 88 6 years 75 - 87 10 years 77 - 95 16 years 78 - 102
Adult 80 - 96
fL
MCH
1 days 31 - 37 1 months 28 - 40 6 months 25 - 35 4 years 23 - 31 6 years 24 - 30 10 years 25 - 33 16 years 25 - 35
Adult 27 - 33
1 days 31 - 37 1 months 28 - 40 6 months 25 - 35 4 years 23 - 31 6 years 24 - 30 10 years 25 - 33 16 years 25 - 33
Adult 27 - 33
pg
MCHC
1 days 290 - 370 7 days 260 - 380
1 months 290 - 370 16 years 300 - 360
Adult 310 - 370
1 days 290 - 370 7 days 260 - 380
1 months 290 - 370 16 years 300 - 360
Adult 310 - 370
g/L
RDW
7 days 13 - 18 4 years 11.5 - 16 10 years 11.5 - 15
Adult 11.5 - 14.5
7 days 13 - 18 4 years 11.5 - 16 10 years 11.5 - 15
Adult 11.5 - 14.5
c/v
WBC
1 days 9.4 - 34 7 days 5 - 21
1 months 6 - 19.5 1 years 6 - 17.5 4 years 6 - 17 6 years 5.5 - 15.5 8 years 5 - 14.5 10 years 4.5 - 13.5 16 years 4.5 - 13
Adult 4 - 11
1 days 9.4 - 34 7 days 5 - 21
1 months 6 - 19.5 1 years 6 - 17.5 4 years 6 - 17 6 years 5.5 - 15.5 8 years 5 - 14.5 10 years 4.5 - 13.5 16 years 4.5 - 13
Adult 4 - 11
x10^9/L
LYMP%
1 years 60 - 67 Adult 25 - 45
1 years 60 - 67 Adult 25 - 45
%
MONO%
Adult 2 - 12 Adult 2 - 12 %
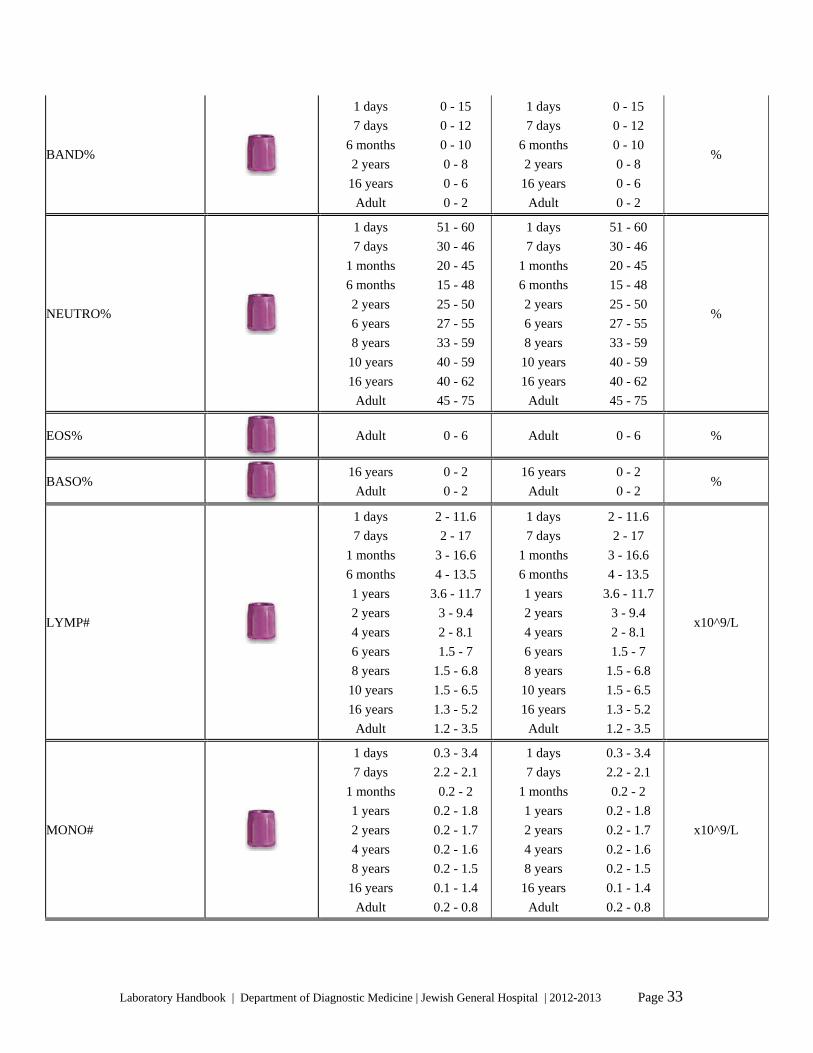
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 33
BAND%
1 days 0 - 15 7 days 0 - 12
6 months 0 - 10 2 years 0 - 8 16 years 0 - 6
Adult 0 - 2
1 days 0 - 15 7 days 0 - 12
6 months 0 - 10 2 years 0 - 8 16 years 0 - 6
Adult 0 - 2
%
NEUTRO%
1 days 51 - 60 7 days 30 - 46
1 months 20 - 45 6 months 15 - 48 2 years 25 - 50 6 years 27 - 55 8 years 33 - 59 10 years 40 - 59 16 years 40 - 62
Adult 45 - 75
1 days 51 - 60 7 days 30 - 46
1 months 20 - 45 6 months 15 - 48 2 years 25 - 50 6 years 27 - 55 8 years 33 - 59 10 years 40 - 59 16 years 40 - 62
Adult 45 - 75
%
EOS%
Adult 0 - 6 Adult 0 - 6 %
BASO%
16 years 0 - 2 Adult 0 - 2
16 years 0 - 2 Adult 0 - 2
%
LYMP#
1 days 2 - 11.6 7 days 2 - 17
1 months 3 - 16.6 6 months 4 - 13.5 1 years 3.6 - 11.7 2 years 3 - 9.4 4 years 2 - 8.1 6 years 1.5 - 7 8 years 1.5 - 6.8 10 years 1.5 - 6.5 16 years 1.3 - 5.2
Adult 1.2 - 3.5
1 days 2 - 11.6 7 days 2 - 17
1 months 3 - 16.6 6 months 4 - 13.5 1 years 3.6 - 11.7 2 years 3 - 9.4 4 years 2 - 8.1 6 years 1.5 - 7 8 years 1.5 - 6.8 10 years 1.5 - 6.5 16 years 1.3 - 5.2
Adult 1.2 - 3.5
x10^9/L
MONO#
1 days 0.3 - 3.4 7 days 2.2 - 2.1
1 months 0.2 - 2 1 years 0.2 - 1.8 2 years 0.2 - 1.7 4 years 0.2 - 1.6 8 years 0.2 - 1.5 16 years 0.1 - 1.4
Adult 0.2 - 0.8
1 days 0.3 - 3.4 7 days 2.2 - 2.1
1 months 0.2 - 2 1 years 0.2 - 1.8 2 years 0.2 - 1.7 4 years 0.2 - 1.6 8 years 0.2 - 1.5 16 years 0.1 - 1.4
Adult 0.2 - 0.8
x10^9/L

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 34
NEUTRO#
1 days 4.8 - 20.4 7 days 1.5 - 9.7
1 months 1.2 - 8.8 6 months 0.9 - 8.4 4 years 1.5 - 8.5 8 years 1.5 - 8 16 years 1.8 - 8.1
Adult 1.8 - 7.5
1 days 4.8 - 20.4 7 days 1.5 - 9.7
1 months 1.2 - 8.8 6 months 0.9 - 8.4 4 years 1.5 - 8.5 8 years 1.5 - 8 16 years 1.8 - 8.1
Adult 1.8 - 7.5
x10^9/L
EOS#
1 days 0 - 1.4 1 months 0 - 0.8 2 years 0 - 0.7 6 years 0 - 0.6 16 years 0 - 0.5
Adult 0 - 0.5
1 days 0 - 1.4 1 months 0 - 0.8 2 years 0 - 0.7 6 years 0 - 0.6 16 years 0 - 0.5
Adult 0 - 0.5
x10^9/L
BASO#
10 days 0 - 0.7 10 years 0 - 0.4 16 years 0 - 0.3
Adult 0 - 0.2
10 days 0 - 0.7 10 years 0 - 0.4 16 years 0 - 0.3
Adult 0 - 0.2
x10^9/L
PLAT
Adult 150 - 400 Adult 150 - 400
Adult 150 - 400 Adult 150 - 400
x10^9/L
MPV
Adult 9.9 - 11.8 Adult 9.9 - 11.8 fL
B2-microglobulin
Adult 0 - 2.2 Adult 0 - 2.2 mg/L
RCV Adult 24 - 32 Adult 22 - 28 mL/kg TBV Adult 55 - 69 Adult 56 - 66 mL/kg
Blood volume
Plasma volume
By appointment only
Adult 30 - 38 Adult 32 - 40 mL/kg
Blood viscosity
Adult 3.6 - 5.4 Adult 3.6 - 5.4
Cryoglobulin
Send at 37 degrees Negative Negative
Folate (Serum/plasma)
Adult 11 - 46 Adult 11 - 46 nmol/L
Haptoglobin
Adult 0.3 - 2 Adult 0.3 - 2 g/L
Heat stability test
Adult 0 - 5 Adult 0 - 5
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 35
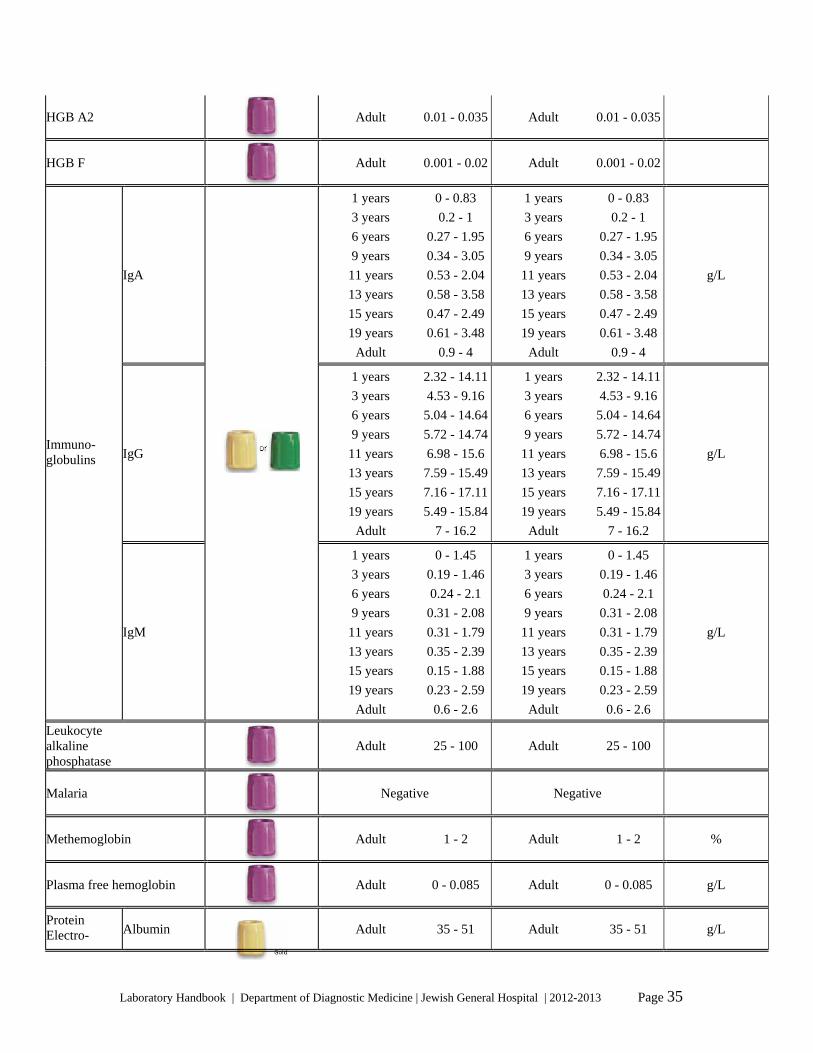
HGB A2
Adult 0.01 - 0.035 Adult 0.01 - 0.035
HGB F
Adult 0.001 - 0.02 Adult 0.001 - 0.02
IgA
1 years 0 - 0.83 3 years 0.2 - 1 6 years 0.27 - 1.95
9 years 0.34 - 3.05
11 years 0.53 - 2.04
13 years 0.58 - 3.58
15 years 0.47 - 2.49
19 years 0.61 - 3.48
Adult 0.9 - 4
1 years 0 - 0.83 3 years 0.2 - 1 6 years 0.27 - 1.95
9 years 0.34 - 3.05
11 years 0.53 - 2.04
13 years 0.58 - 3.58
15 years 0.47 - 2.49
19 years 0.61 - 3.48
Adult 0.9 - 4
g/L
IgG
1 years 2.32 - 14.11
3 years 4.53 - 9.16
6 years 5.04 - 14.64
9 years 5.72 - 14.74
11 years 6.98 - 15.6
13 years 7.59 - 15.49
15 years 7.16 - 17.11
19 years 5.49 - 15.84
Adult 7 - 16.2
1 years 2.32 - 14.11
3 years 4.53 - 9.16
6 years 5.04 - 14.64
9 years 5.72 - 14.74
11 years 6.98 - 15.6
13 years 7.59 - 15.49
15 years 7.16 - 17.11
19 years 5.49 - 15.84
Adult 7 - 16.2
g/L Immuno- globulins
IgM
1 years 0 - 1.45 3 years 0.19 - 1.46
6 years 0.24 - 2.1 9 years 0.31 - 2.08
11 years 0.31 - 1.79
13 years 0.35 - 2.39
15 years 0.15 - 1.88
19 years 0.23 - 2.59
Adult 0.6 - 2.6
1 years 0 - 1.45 3 years 0.19 - 1.46
6 years 0.24 - 2.1 9 years 0.31 - 2.08
11 years 0.31 - 1.79
13 years 0.35 - 2.39
15 years 0.15 - 1.88
19 years 0.23 - 2.59
Adult 0.6 - 2.6
g/L
Leukocyte alkaline phosphatase
Adult 25 - 100 Adult 25 - 100
Malaria
Negative Negative
Methemoglobin
Adult 1 - 2 Adult 1 - 2 %
Plasma free hemoglobin
Adult 0 - 0.085 Adult 0 - 0.085 g/L
Protein Electro- Albumin Adult 35 - 51 Adult 35 - 51 g/L

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 36
Alpha 1 Adult 1 - 3 Adult 1 - 3 g/L
Alpha 2 Adult 5 - 10 Adult 5 - 10 g/L
Beta Adult 6 - 11 Adult 6 - 11 g/L
phoresis
Gamma Adult 6 - 15 Adult 6 - 15 g/L
Retics
Adult 7 - 31 Adult 7 - 31 x-10^3
Without Intrinsic factor
Adult 8 - 50 Adult 8 - 50 % Schilling test
With Intrinsic factor
By appointment only
Adult 8 - 50 Adult 8 - 50 %
Sed. rate (Westergren)
Adult 0 - 15 Adult 0 - 20 mm/h
Serum free hemoglobin
Adult 0 - 0.085 Adult 0 - 0.085 g/L
Serum muramidase
Adult 5 - 15 Adult 5 - 15 mg/L
Serum viscosity
Adult 1 - 2 Adult 1 - 2
Sickle cell
Negative Negative
Sulphemoglobin
Adult 0 - 2.2 Adult 0 - 2.2 %
Urine eosinophil
Negative Negative
Urine free hemoglobin
Negative Negative
Urine hemosiderin
Negative Negative

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 37
Urine muramidase
Adult 0 - 2 Adult 0 - 2 mg/L
Vitamin B12
Adult 140 - 700 Adult 140 - 700 pmol/L
Coagulation
Test Specimen Age Male Age Female Units
APTT
Adult 27 - 35 Adult 27 - 35 s
PT
Adult 11.5 - 14.5 Adult 11.5 - 14.5 s
INR
Therapeutic INR: 2.0-3.0 (Metallic valves: 2.5-3.5)
Therapeutic INR: 2.0-3.0 (Metallic valves: 2.5-3.5)
Fibrinogen
Adult 2 - 4.5 Adult 2 - 4.5 g/L
Thrombin time
Adult 13 - 18 Adult 13 - 18 s
D-dimer
Adult 0 - 0 Adult 0 - 0 ug FEU/L
Factor II
Adult 0.7 - 1.1 Adult 0.7 - 1.1
Factor V
Adult 0.7 - 1.6 Adult 0.7 - 1.6
Factor VII
Adult 0.6 - 1.55 Adult 0.6 - 1.55
Factor VIII
Adult 0.5 - 2 Adult 0.5 - 2
Factor IX
Adult 0.65 - 1.4 Adult 0.65 - 1.4
Factor X
Adult 0.7 - 1.4 Adult 0.7 - 1.4
Factor XI
Adult 0.6 - 1.35 Adult 0.6 - 1.35
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 38
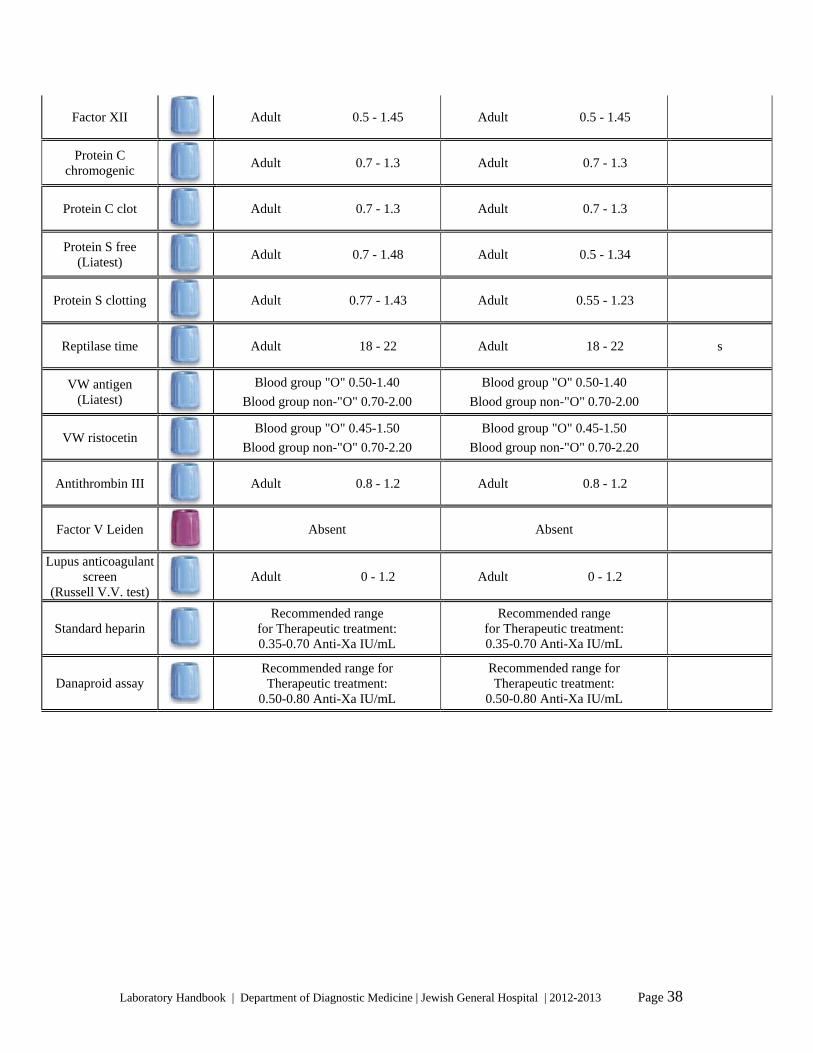
Factor XII
Adult 0.5 - 1.45 Adult 0.5 - 1.45
Protein C chromogenic
Adult 0.7 - 1.3 Adult 0.7 - 1.3
Protein C clot
Adult 0.7 - 1.3 Adult 0.7 - 1.3
Protein S free (Liatest)
Adult 0.7 - 1.48 Adult 0.5 - 1.34
Protein S clotting
Adult 0.77 - 1.43 Adult 0.55 - 1.23
Reptilase time
Adult 18 - 22 Adult 18 - 22 s
VW antigen (Liatest)
Blood group "O" 0.50-1.40 Blood group non-"O" 0.70-2.00
Blood group "O" 0.50-1.40 Blood group non-"O" 0.70-2.00
VW ristocetin
Blood group "O" 0.45-1.50 Blood group non-"O" 0.70-2.20
Blood group "O" 0.45-1.50 Blood group non-"O" 0.70-2.20
Antithrombin III
Adult 0.8 - 1.2 Adult 0.8 - 1.2
Factor V Leiden
Absent Absent
Lupus anticoagulant screen
(Russell V.V. test) Adult 0 - 1.2 Adult 0 - 1.2
Standard heparin
Recommended range for Therapeutic treatment:0.35-0.70 Anti-Xa IU/mL
Recommended range for Therapeutic treatment: 0.35-0.70 Anti-Xa IU/mL
Danaproid assay
Recommended range forTherapeutic treatment:
0.50-0.80 Anti-Xa IU/mL
Recommended range for Therapeutic treatment:
0.50-0.80 Anti-Xa IU/mL

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 39
Dalteprin peak (3-4 hours)
Recommended range for therapeutic treatment with Dalteparin
a) Treatment dosage = 100 IU/Kg Q12H:0.40 - 0.80 Anti-Xa IU/mL
b) Treatment dosage = 120 IU/Kg Q12H:0.60 - 1.20 Anti-Xa IU/mL
c) Treatment dosage = 200 IU/Kg Q24H:0.80 - 1.60 Anti-Xa IU/mL Recommended range for
therapeutic treatment with Enoxaparin a) Treatment dosage = 1.0 mg/Kg Q12H:
0.60 - 1.00 Anti-Xa IU/mL b) Treatment dosage = 1.5 mg/Kg Q24H:
1.00 - 1.60 Anti-Xa IU/mL
Recommended range for therapeutic treatment with Dalteparin
a) Treatment dosage = 100 IU/Kg Q12H:0.40 - 0.80 Anti-Xa IU/mL
b) Treatment dosage = 120 IU/Kg Q12H:0.60 - 1.20 Anti-Xa IU/mL
c) Treatment dosage = 200 IU/Kg Q24H:0.80 - 1.60 Anti-Xa IU/mL Recommended range for
therapeutic treatment with Enoxaparin a) Treatment dosage = 1.0 mg/Kg Q12H:
0.60 - 1.00 Anti-Xa IU/mL b) Treatment dosage = 1.5 mg/Kg Q24H:
1.00 - 1.60 Anti-Xa IU/mL
Dalteprin trough
For Dalteparin Recommended range for
therapeutic treatment: 0.20-0.40 Anti-Xa IU/mL Recommended range for prophylactic treatment:
0.10-0.30 Anti-Xa IU/mL For Enoxaparin
Recommended ranges not established
For Dalteparin Recommended range for
therapeutic treatment: 0.20-0.40 Anti-Xa IU/mL Recommended range for prophylactic treatment:
0.10-0.30 Anti-Xa IU/mL For Enoxaparin
Recommended ranges not established
IgG
Adult 0 - 21 Adult 0 - 21 GPL u/mL Anticardiolipin
antibody IgM
Adult 0 - 19 Adult 0 - 19 MPL u/mL

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 40
Various tests requiring special collection
Container Test Comments
Pre-chilled
ACTH
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable in whole blood; must be received in the laboratory within 30 min of collection.
Pre-chilled
ADH (Vasopressin)
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable in whole blood; must be received in the laboratory within 30 min of collection.
Ammonia
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable in whole blood; must be received in the laboratory within 15 min of collection.
Beta Hydroxybutyric Acid
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable in whole blood; must be received in the laboratory within 30 min of collection.
CA 15-3
Ideally, collect on wet ice. Send to lab ASAP with sufficient ice.
CA 19-9
Ideally, collect on wet ice. Send to lab ASAP with sufficient ice.
Calcium ionized
Collect on wet ice. Avoid having the patient make a fist. The tourniquet must not be applied for greater then one minute. Do not expose the specimen to air at any time during collection or transport. Stable in whole blood at 4C for 4 hours. Do not freeze the sample tube.
Calcitonin
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable in whole blood; must be received in the laboratory within 30 min of collection.
Carotene
Protect from light. Wrap specimen in aluminum foil.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 41
Pre-chilled
Catecholamines (Plasma)
This is not a routine assay and must be discussed with the Biochemist on-call before requesting. Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable, must be received in the laboratory within 30 min of collection.
C-peptide
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Must be separated from cells within 6 hours of collection.
Collect 2 red top tubes
Cryoglobulins Must be kept warm (37C) from time of collection until arrival in the laboratory.
C-telopeptide
12 hours fasting. Sample must be collected before 10:00am. Offsite: please collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted.
Free erythrocyte protoporphyrin
Protect from light. Wrap specimen container in aluminum foil.
Gastrin
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted.
Growth hormone
Fasting 8 hours and 30 min at rest before collection. Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted.
Homocysteine
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable in whole blood; must be received in the laboratory within 60 min of collection.
Lactate
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable, must be received in the laboratory within 15 min of collection.
Methotrexate
Protect from light. Wrap specimen in aluminum foil. Collect on wet ice. Send STAT.
Methylmalonic acid
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 42
Osteocalcin
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable, must be received in the laboratory within 60 min of collection.
Porphyrin (Plasma)
Protect from light. Wrap specimen container in aluminum foil.
Random urine
PBG/ALA- random urine
Protect from light. Wrap specimen container in aluminum foil.
Random stool
Porphyrin screen- fecal
Protect from light. Wrap specimen container in aluminum foil.
Random urine
Porphyrin screen- urine
Protect from light. Wrap specimen container in aluminum foil.
Pre-chilled
Renin
Collect on wet ice. Send to lab ASAP with sufficient ice. Sample will be rejected if ice has fully melted. Analyte is highly unstable in whole blood; must be received in the laboratory within 60 min of collection.
Vitamin A
Protect from light. Wrap specimen container in aluminum foil.
Vitamin E
Protect from light. Wrap specimen container in aluminum foil.
AC = Fasting (at least 6 hrs); PC = 2 hours postprandial
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 43
Glucose tolerance test (GTT or OGTT)
What is the glucose tolerance test? The glucose tolerance test measures the body's ability to metabolize glucose. Why is this test performed? The oral glucose tolerance test is generally performed to diagnose diabetes mellitus when fasting blood glucose is difficult to interpret. How to prepare for the OGTT? The test is generally performed 8 to 14 hours after an overnight fast. We suggest fasting from 22h00 and then present to the test center the following morning at 08h00. The test must be performed before 10:00 am for proper interpretation. We recommend bringing along a good book or other reading material, as you will be required to remain seated for 2 hours during the test. What does fasting mean? No caloric intake for at least 8 hours before your first blood sample is taken. During this period only water may be taken. Can I drink other liquids? You may drink only water (no tea, coffee, or other beverages) Can I take my medication? A number of medications can affect the test results, therefore, it is important to inform your health professional of all medications you are currently taking. You may be instructed to stop certain medications prior
to the test. When can I resume eating? The standard glucose tolerance takes 2 hours from the 1st blood sample. You will be able to eat after the last blood sample. What other precaution must be taken prior to test? You should maintain an unrestricted diet and activity for at least three days prior to the test. Do not engage in strenuous exercise for 8 to 14 hours before the first blood sample is taken. How is the test done? On the day of test, the following steps will be done: 1. A blood sample will be collected after
you arrive and register at the test center. 2. You will be asked to drink a sweet liquid
containing 75 g of glucose. It should be drunk slowly over 5 min.
3. You should remain seated at the test center during the test, without smoking.
4. A second blood sample will then be collected after 2 hours.
5. You may then eat and drink. What affects the Test? 1. Acute stress (surgery, infection,
emotional cause, or fever) or Vigorous exercise
2. Certain medications, as well as alcohol. 3. Low carbohydrates diet in the days just
before the test. 4. Vomiting during the test may also cause
inaccurate results.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 44
Patient Instructions for a Clean-Catch Urine Collection
Container: sterile container - orange top
Notes: To ensure that the urine specimen you are submitting is of good quality and not
contaminated with other germs:
1. Never collect urine from a bedpan or urinal
2. Thoroughly clean the genital area prior to collection procedures to ensure that the
specimen obtained is not contaminated with skin bacteria.
3. Transport specimen to the laboratory within 2 hours of collection. If this is not possible,
the urine specimen should be refrigerated and transported to the lab within 24 hours.
Make sure your specimen is clearly labelled with your name and information.
Procedure:
Clean-Catch urine specimens (female)
1. Sit comfortably on the toilet, and swing one knee to the side as far as you can.
2. Spread yourself with one hand, and hold yourself spread while you clean yourself
and then collect the specimen.
3. Using antibacterial soap or regular soap, wipe your vaginal area as carefully as
you can from front to back between the folds of skin.
4. After washing, rinse well with a water moistened pad or with a damp face cloth
with the same front to back motion. Use each pad only once and then discard it.
5. Hold the cup with your fingers on the outside; do not touch the rim. First, pass a
small amount of urine into the toilet, and then pass enough urine into the cup to fill
it half full.
6. Place the lid back on the cup and make sure it is closed tightly.
Clean-Catch urine specimen (Male)
1. Retract the foreskin (if uncircumcised), and clean the glans (head of the penis)
Follow steps 3 to 6 above for cleaning yourself and collecting the urine.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 45
Patient instructions for 24-Hour urine collection
NOTE: PLEASE USE URINE CONTAINERS PROVIDED BY THE HOSPITAL. URINE COLLECTED IN ANY OTHER CONTAINER WILL NOT BE ACCEPTED. 1. On the morning that you start collecting your urine, (eg. 9:00A.M.), empty your
bladder in the toilet and discard the urine. Note: The collection starts with an empty bladder.
2. At the start of the collection, record the start date and time on the label attached to
the container. At the end of the collection, record the finish date and time as well. 3. Collect ALL the urine for the rest of the morning, afternoon, evening and night, in the
container provided. 4. Make sure the lid is tightly closed and the spout is snapped in to avoid any spillage. 5. Take the container with you if you go out. 6. Keep the container in a cold place whenever you can. 7. The following morning, (ex. 9:00 A.M. the next day), empty your bladder and collect
the urine. This is the last urine to be collected. 8. Bring in all your collected urine, along with the requisition, to the
Test Centre (Room E-102), or to the Department of Diagnostic Medicine Department (Room D-136).
If you have any questions, please call 340-8222 extension 5094. REMEMBER: You will have to start again if any urine is missed during the 24 hour collection OR if the requisition does not accompany the collection upon delivery. CAUTION: The bottles marked CORROSIVE contain acid. In order to avoid acid burns, empty your bladder in a measuring cup first and then transfer the urine to the bottle. Rinse the measuring cup with water only after each usage. Do not wash with soap or detergent. Keep the container upright to avoid acid spillage or contamination of the bottle cap. In case of skin contact with acid, wash immediately with water (5 minutes).
We do not provide the measuring cup; one can be purchased at any grocery store, pharmacy or a dollar store.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 46
24-Hour urine collection bottles
Test Special Conditions Plain Bottle
Acid Bottle
Metal-free Bottle
ALA (or PBG) √ Aldosterone √ Amino acids √ Amylase √ Arsenic √ Bence Jones (protein) √ Calcium √ (to acidify) √ Catecholamines (Epinephrine + Nor-Epinephrine)
√
Chloride Acid unacceptable √ Citrates √ (to acidify) √ Copper √ Cortisol √ Creatinine, including creatinine clearance
Serum creatinine required for clearance
√ √
Cysteine √ Electrolytes Acid unacceptable √ 5-HIAA Special instructions
for patient (see P&P) √
Hydroxyproline √ Lead √ Magnesium √ (to acidify) √ Mercury √ Metanephrines √ Microalbumin √ Nitrogen sulphate √ Osmolality √ Oxalates √ (to acidify) √ Phosphate (Phosphorus) √ (to acidify) √ Porphyrins √ Potassium Acid unacceptable √ Protein √ Protein electrophoresis √ Sodium Acid unacceptable √ Trace elements √ Urea √ √ Urea nitrogen profile (TPNU) √ Uric acid √ Zinc √
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 47
Patient instructions for sputum collection
Container: sterile- orange top
Procedure: (Bacterial Culture)
1. If possible, rinse your mouth and gargle with water prior to sputum collection. If you have
dentures, remove them prior to specimen collection.
2. Cough deeply to produce a good sputum specimen. Expectorate this into the sterile
container provided. Do not cough spit or post nasal discharge into the container.
Procedure: (Tuberculosis)
1. Collect sputum as instructed above, but collect specimen as soon as you wake up in the
morning.
2. Collect a sample on 3 consecutive days for a total of 3 specimens.
Sputum should be brought to the laboratory as soon as possible the same day. If a delay of 1-2
hours is anticipated, refrigerate the specimen prior to bringing it to the lab.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 48
Patient instructions for stool collection
(routine culture and Clostridium difficile)
Container: Sterile orange top
Sterile white container with spoon
To ensure that the best quality specimen is collected:
1. Stool must not be contaminated with urine or water from the toilet bowl.
2. The stool must be collected in the manner described below. Do not use toilet paper to
collect the stool sample.
3. The following medications might interfere with the results of the stool test, therefore you
should wait seven days before providing a specimen if you have taken any of the
following:
o Bismuth
o Magnesium ( e.g. Some antacids)
o Mineral oil
o Barium meal or Barium enema test
Procedure:
Collect the stool in the following manner;
1. Pass the stool sample directly into a sterile, wide mouth, leakproof container with a tight
fitting lid.
2. To prevent stool from mixing with water, place either an aluminum pie plate in the toilet
bowl, or place saran wrap over the toilet seat to collect stool sample.
3. With a cardboard stick or with the spoon provided in the white top container provided,
spoon out an egg sized portion and place it into the sterile container.
4. It is important to bring the stool specimen to the lab the same day, and preferably within 2
hours after collection. If a delay of more than 2 hours is anticipated, place the specimen
in your refrigerator prior to bringing it to the lab.
If your Doctor asks you to collect two or three specimens, these should be collected on
separate days.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 49
Patient instructions for stool O&P collection
Container: yellow top container with liquid and spoon. DO NOT empty liquid out.
To ensure that the best quality specimen is collected:
1. Stool must not be contaminated with urine or water from the toilet bowl. 2. The stool must be collected in the manner described below. Do not use toilet paper to
collect the stool sample. 3. The following medications might interfere with the results of the stool test, therefore you
should wait seven days before providing a specimen if you have taken any of the following:
o Bismuth o Magnesium ( e.g. Some antacids) o Mineral oil o Barium meal or Barium enema test
Procedure:
Collect the stool in the following manner;
1. Pass the stool sample directly into a sterile, wide mouth, leakproof container with a tight fitting lid.
2. To prevent stool from mixing with water, place either an aluminum pie plate in the toilet bowl, or place saran wrap over the toilet seat to collect stool sample.
3. With a cardboard stick or with the spoon provided in the white top container provided, spoon out an egg sized portion and place it into the sterile container.
4. It is important to bring the stool specimen to the lab the same day, and preferably within 2 hours after collection. If a delay of more than 2 hours is anticipated, place the specimen in your refrigerator prior to bringing it to the lab.
5. The liquid in this container is poisonous. DO NOT drink this and keep away from children. 6. If your Doctor asks you to collect 2 or 3 stools, wait 48 hours between specimens.
o Since the stool is well preserved in the liquid, you can bring all 3-stool specimens to the lab on the same day.
If you are collecting stool for both culture and O&P, you can collect stool for bacterial culture and O&P at the same time and bring all specimens to the lab the day the last specimens are collected.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 50
The following protocol is to be used for diagnosing Influenza. Influenza is diagnosed by viral culture or antigen detection.
Influenza is NOT diagnosed by a blood test.
The best specimen for viral detection in adults is a throat gargle. If this cannot be done (i.e.
intubated patients, patients with no gag reflex, patients with decreased level of consciousness or
severe dementia or unable to cooperate), then a deep nasal swab should be done.
Procedure for obtaining a throat gargle for Influenza virus detection
1. Use 2 mL of non-bacteriostatic saline (available in pink plastic unidose ampoules OR 2
mL can be aspirated from a single-dose vial of non-bacteriostatic saline for injection;
discard vial after use).
2. Place saline into sterile orange-topped specimen container
3. Ask patient to gargle with saline for 5 seconds (i.e. "count slowly to five") and then to spit
saline back into the container. Close container tightly.
4. Label specimen. Send specimen without delay to Microbiology, accompanied by a single
blue Microbiology requisition, and check off "viral culture" (specimen: throat gargle) and
also write in "Rapid Influenza Assay".
Procedure for obtaining a deep nasal swab for Influenza virus detection
1. Use the regular culture swabs.
2. Moisten culture swab first by placing it into the accompanying culture tube, which is
already filled with transport liquid in a mini-sponge. Leave swab in contact with mini-
sponge for 5-10 seconds.
3. Remove swab from culture tube, and place into posterior nostril of patient. Press against
nostril wall in a circular motion 3-5 times. Remove and place into other nostril and rotate
against nostril wall another 3-5 times. Place swab back into culture tube and close tightly
by pressing into place.
4. Label specimen. Send specimen without delay to Microbiology, accompanied by a single
blue Microbiology requisition, and check off "viral culture" (specimen: nasopharyngeal
swab) and also write in "Rapid Influenza Assay".

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 51
Fecal occult blood screening - Patient information
PURPOSE OF TEST To detect colorectal bleeding. HOW? By detecting blood in the stool that is invisible to the eye, but can be detected by a simple chemical reaction. WHAT TO DO? 2 easy steps: 1. For a period of 48 hours, and until all
stool specimens are collected, do not eat red meat, radishes, turnips, melons or horseradish. You may eat small quantities of chicken and tuna. For the same period of time take no aspirin or vitamin C. All these substances may contain blood-like material or cause the appearance of blood in the stool, and produce false results. During this testing period, eat plenty of cooked fruits and vegetables and whole grain cereals such as “All Bran.” These foods encourage bowel movements.
2. After a full 48 hours on the above diet, collect pieces of stool from the first 3 bowel movements. First Collection 1. Flip open slide 1 2. Use one stick to collect a sample from
stool 3. Apply a thin layer of stool on the
rectangle labelled A
4. Apply a second layer of stool on the rectangle labelled B
5. Close the cover flap 6. Discard the stick Second Collection 1. Flip open slide 2 2. Use one stick to collect a sample from
stool 3. Apply a thin layer of stool on the
rectangle labelled A 4. Apply a second layer of stool on the
rectangle labelled B 5. Close the cover flap 6. Discard the stick Third Collection 1. Flip open slide 3 2. Use one stick to collect a sample from
stool 3. Apply a thin layer of stool on the
rectangle labelled A 4. Apply a second layer of stool on the
rectangle labelled B 5. Close cover flap 6. Discard the stick NOTE: 1. Do not apply more than a thin smear,
the test result may be invalid 2. Do not expose slides to the heat,
sunlight, or fluorescent light. Keep it in cool, dark place.
3. Do not collect specimens during menstruation or hemorrhoidal bleeding.
3. Return the test card to the Test Centre.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 52
Labeling of cytology specimens
1. All specimens must have a label affixed, pre-printed or handwritten, which supplies the following information: • Patient’s full name • Patient’s unique identifying number (RAMQ or MRN) • Site of specimen • Time of immersion into fixative. 2. To avoid mislabeled specimens, proper identification of the patient is necessary at the point of collection. Carefully verify the information on the admitted patient’s bracelet at bedside just prior to specimen collection. All outpatients are identified by asking the individual to pronounce his full name and date of birth. The information provided by the patient must exactly match the physician request, the laboratory requisition, and the specimen label prior to collection. 3. No collection containers should be pre-labeled. Containers should be
labeled directly at the patient-side immediately following collection. Immediately discard any unused labels to avoid mislabeling of the next patient. 4. Proper containers and fixatives for collection must be used. Using a wrong container or fixative may lead to erroneous results. 5. Where there is uncertainty in the identification of the primary sample or its condition, the laboratory may choose to process the sample after the requesting physician or person responsible for the primary sample collection takes the responsibility for identifying and accepting the sample, or for providing proper information, or all these. In such an instance, the signature of that person taking responsibility for the primary sample identification should be recorded on the request form and in the final report.
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 53
Procurement of cytology specimens
Please note: All specimens are to be sent accompanied with a properly completed requisition.
1. Body Fluids (Ascetic, Peritoneal, Pericardial, etc.)
• A fresh specimen is sent to the cytology laboratory in a sterile urine cup container or vacutainer.
• The specimens must be labeled as required.
• Containers must be securely tightened to avoid any leakage.
• The specimen should be delivered to the laboratory ASAP!
• If a delay is anticipated, the specimen should be refrigerated.
• DO NOT send drainage apparatus, needles or syringes to the laboratory.
2. Bronchial/Gastric Brushings
• The specimens are to be submitted in a sterile container containing 95% alcohol.
• The complete brush or slide must be immersed in the Cytolyt solution and gently shaken.
• The specimens must be labeled as required.
• Containers must be securely tightened to eliminate any leakage.
• The specimen should be send to cytology ASAP.
• If a delay is anticipated, the specimen should be refrigerated.
3. Bronchial / Gastric Washings
• A fresh specimen is submitted in a sterile specimen container.
• The specimens must be labeled as required.
• Containers must be securely tightened to eliminate any leakage.
• The specimen should be send to cytology ASAP.
• If a delay is anticipated, the specimen should be refrigerated.
4. Cerebrospinal Fluid (CSF)
• The specimen is submitted fresh in a sterile specimen container.
• Containers must be securely tightened to eliminate any leakage.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 54
• The specimen should be send to cytology ASAP.
• If a delay is anticipated, the specimen should be refrigerated.
• If the preliminary diagnosis is leukemia or lymphoma, a second sample is required for Flow Cytometry.
5. Pap Test
• The PAP smear is to be fixed in alcohol and delivered to the cytology laboratory with properly completed requisition.
• The slide has to be labeled in pencil and should have the patient’s full name and RAMQ or MRN.
6. Fine needle Aspirations: this procedure may yield a Cytopathology specimen, a tissue specimen or both.
• The tissue core specimen must be placed in formalin container and be delivered to pathology.
• The cytopathology specimen should be smeared on a slide and fixed in alcohol or cytospray.
• The specimens must be labeled as required.
7. Sputum
• The specimen is submitted in a sterile urine cup with no preservative.
• A series of three early morning deep cough specimens is the most sensitive. It is recommended that patients should clean teeth and mouth prior to obtaining specimen.
• The specimens must be labeled as required.
• Containers must be securely tightened to eliminate any leakage.
• The specimen should be send to cytology ASAP.
• If a delay is anticipated, the specimen should be refrigerated.
8. Urine
• The specimen is submitted in a urine cup with no preservative.
• A series of three morning urines from consecutive days have to be collected.
• First morning specimens should NOT be used the second morning specimen is recommended.
• The specimens must be labeled as required.
• Containers must be securely tightened to eliminate any leakage.
• The specimen should be send to cytology ASAP.
• If a delay is anticipated, the specimen should be refrigerated.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 55
Transfusion service
Starting November 19th 2007, Transfusion Service will introduce a new requisition (F161 REV 09-07 - see attached).which will replace and incorporate our present 3 requisitions (F160, 161 and 162). On the above start date, the new requisitions will be available in Stores, your old requisitions are to be discarded and the new requisition put in place. In order to meet this CCHSA requirement, it is mandatory for both the requisition and specimen to include (see attached examples):
1) Patient Identification – label, addressograph or handwritten (Full Name/Hospital # or RAMQ (date of birth if RAMQ not available))
2) Date 3) Time 4) Phlebotomist’s initials
In order to facilitate the introduction of these mandatory requirements, there will be a transition period of one month. During this time, Transfusion Service will call the location stating that a notification form (see attached) is being faxed for the charge nurse. This notification form will indicate what mandatory information the patient’s requisition and/or specimen were missing. IMPORTANT: It should be noted that the mandatory information not indicated on the notification form is already enforced. If the requisition and/or specimen are received with any of the above information missing:
1) Specimen: If the patient’s name or number is missing the specimen will be rejected. Missing collection date and time can be completed however, the phlebotomist must come to the Transfusion Service to complete this or the specimen will be rejected. If there is an urgent need for blood, the protocol for uncrossmatched blood will be applied.
2) Requisition: if only the requisition is missing mandatory information, the phlebotomist must complete another requisition and have it hand delivered to Transfusion Service or the specimen will be rejected. If there is an urgent need for blood, the protocol for uncrossmatched blood will be applied.

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 56
TRANSFUSION SERVICE REQUEST
1
2
3 4 5
6
7
RENSEIGNEMENT NÉCESSAIRE DU PROCÉDÉ NECESSARY PROCESS INFORMATION
2) INFORMATION NÉCESSAIRE– NECESSARY INFORMATION 3) TYPE D’ÉCHANTILLON – TYPE OF SPECIMEN 4) ANALYSES - TESTS 5) PRODUIT/QUANTITÉ - PRODUCT/AMOUNT 6) COMMENTAIRES - COMMENTS 7) POUR L'USAGE DU LABO SEULEMENT- LAB USE ONLY
RENSEIGNEMENT OBLIGATOIRE MANDATORY INFORMATION
NOM COMPLET – FULL NAME #DOSSIER OU RAMQ (DDN) - HOSPITAL# OR RAMQ (DOB)
INITIALES DU (DE LA) PHLÉBOTOMISTE –
PHLEBOTOMIST’S INITIALS DATE – DATE HEURE – TIME
1
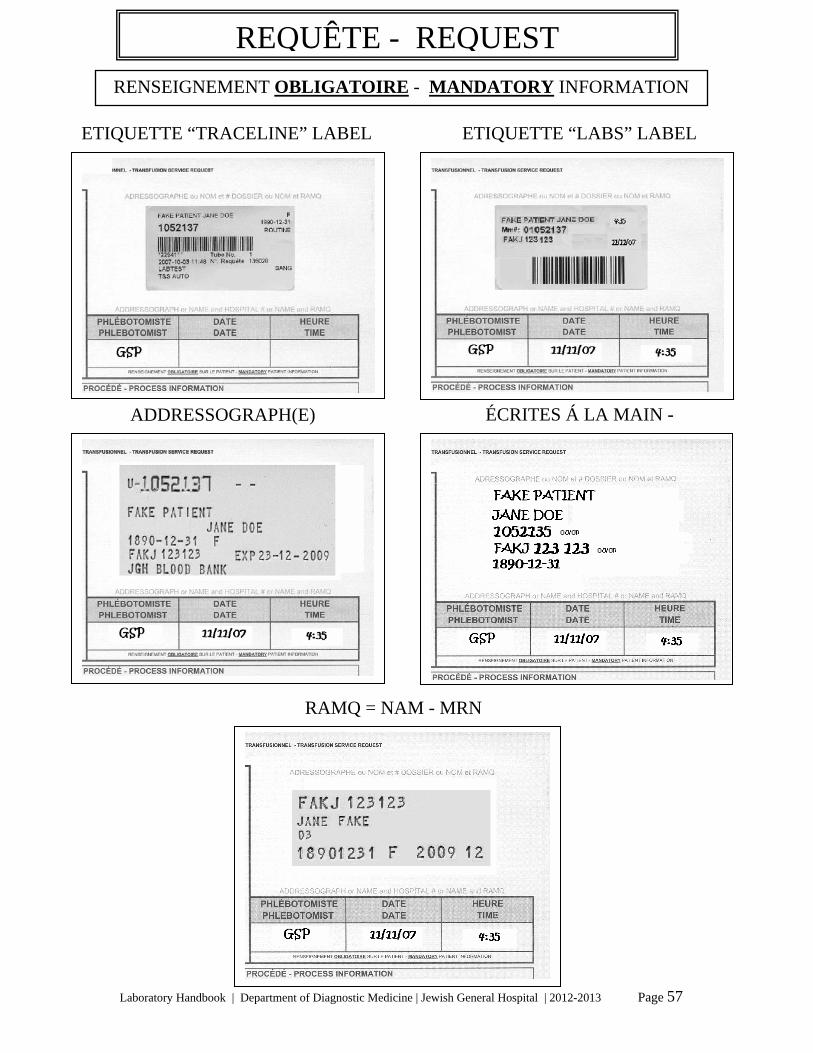
Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 57
ETIQUETTE “TRACELINE” LABEL ETIQUETTE “LABS” LABEL
ADDRESSOGRAPH(E) ÉCRITES Á LA MAIN -
REQUÊTE - REQUEST
RENSEIGNEMENT OBLIGATOIRE - MANDATORY INFORMATION
RAMQ = NAM - MRN

Laboratory Handbook | Department of Diagnostic Medicine | Jewish General Hospital | 2012-2013 Page 58
ETIQUETTE “TRACELINE” LABEL ETIQUETTE “LABS” LABEL
12
3 4 5
RENSEIGNEMENT OBLIGATOIRE - MANDATORY INFORMATION
1) NOM COMPLET – FULL NAME 2) #DOSSIER OU RAMQ - HOSPITAL# OR RAMQ 3) DATE – DATE 4) HEURE – TIME 5) INITIALES DU (DE LA) PHLÉBOTOMISTE -
PHLEBOTOMIST’S INITIALS
ÉCHANTILLON - SPECIMEN
FAKE PATIENT JANE DOE
1052135 OU/OR FAKJ 123 123 OU/OR 1890-12-31 11/11/07 4:35 GSP
ADDRESSOGRAPH(E) ÉCRITES Á LA MAIN - HANDWRITTEN
GSP GSP
GSP
11/11/07
11/11/07
4:35
4:35
RAMQ NAM - MRN
GSP 11/11/07 4:35

















