35
Department of Otorhinolaryngology
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | jeremy-washington |
| View: | 231 times |
| Download: | 4 times |

Department of Otorhinolaryngology
CHOLESTEATOMA
Chronic Suppurative Otitis Media Attico-Antral Type
Cholesteatoma
• Is epidermal cyst of the middle ear and/or Temporal bone with a squamous epithelial lining.
• Contain keratin and desquamated epithelium.• Can be congenital or acquired• Natural history is progressive growth with erosion of
surrounding bone due to pressure effects and osteoclast activation.
It is skin in wrong place

Cholesteatoma
It erodes bone by: 1.Enzymatic activity. 2.Pressure necrosis (expansion of the
sac). This may open pathways for spread of
infection (Bony or Unsafe type o CSOM)

Pathogenesis of Cholesteatoma
Congenital Cholesteatoma: Arises from embryonic epithelial tissue in the
temporal bone ( may be in ME cavity or temporal bone especially the petrous apex).
Epidermal cysts usually present in the anterior superior quadrant of the middle ear near the Eustachian tube orifice.
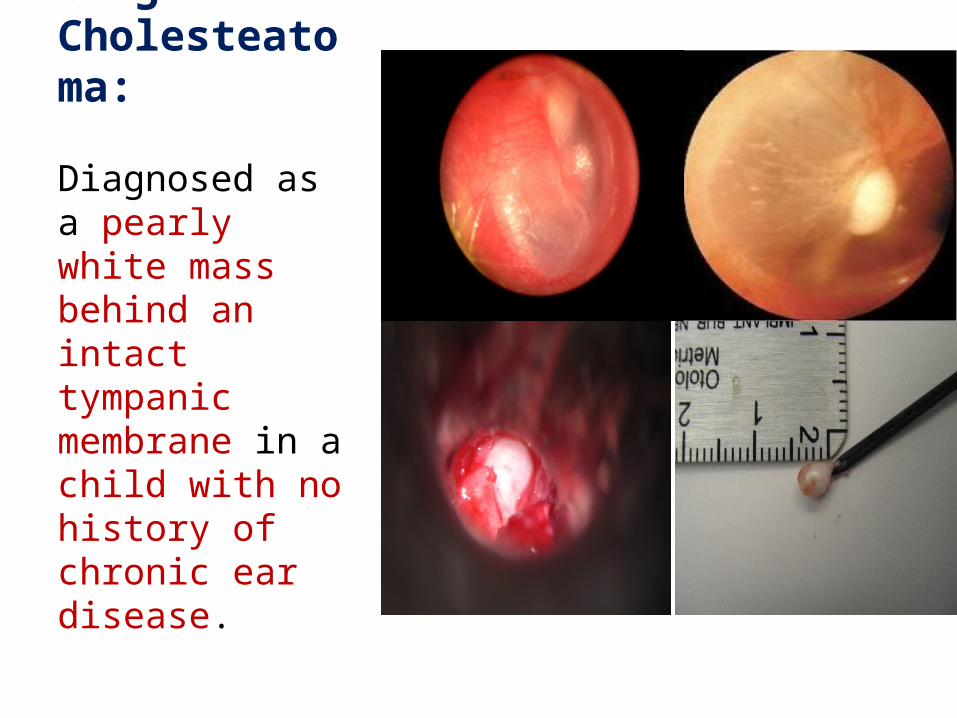
Congenital Cholesteatoma:
Diagnosed as a pearly white mass behind an intact tympanic membrane in a child with no history of chronic ear disease.

Acquired Cholesteatoma
PathogenesisSquamous epithelium may be found in the
middle ear as a result of:
• Invagination• Migration (through a perforation)• Squamous metaplasia
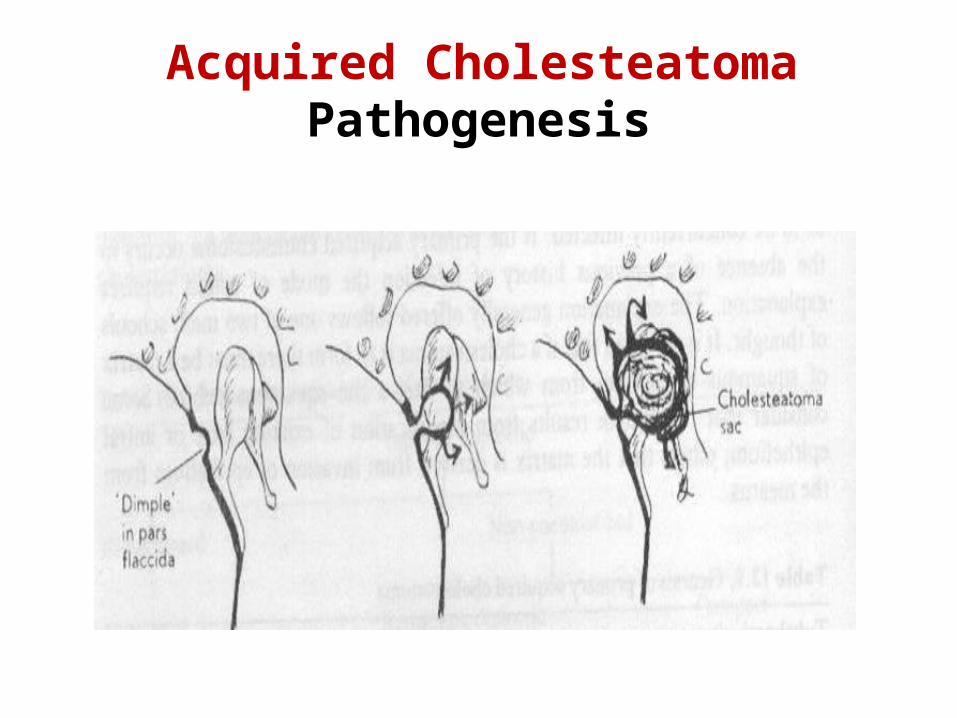
Acquired Cholesteatoma Pathogenesis
Acquired Cholesteatoma
1) Invagination Theory ( primary acquired ) Prolonged ET obstruction creates negative
ME pressure leading to retraction of pars flaccida (or the superior part of the membrana tensa) which becomes an invaginated into the ME (retraction pocket) and gradually distend with accumulated keratin and later on separate from the drum membrane.


Primary acquired cholesteatoma
Normal TM Primary acquired (M Flaccida)
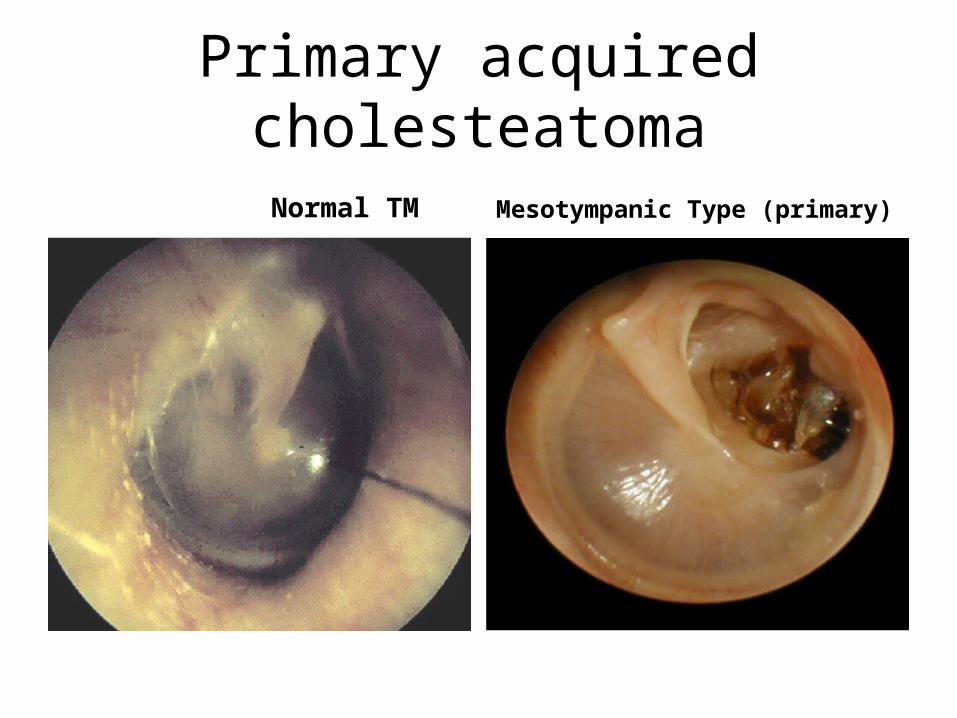
Primary acquired cholesteatoma
Normal TM Mesotympanic Type (primary)
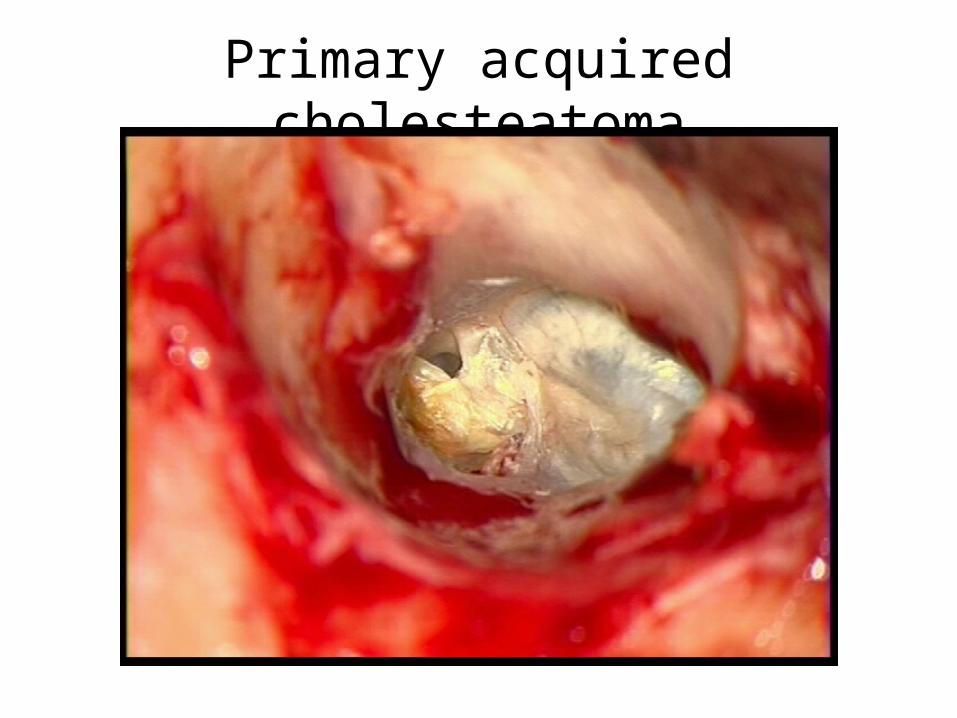
Primary acquired cholesteatoma
Pathogenesis Of Cholesteatoma (cont.)
2) Migration Theory (Secondry acquired)The stratified squamous epithelium of the deep
external auditory meatus grows through a marginal perforation into the middle ear cavity.
3) Metaplasia Theory Long standing suppuration can stimulate metaplasia
of the simple squamous epithelium of the middle ear to stratified squamous epithelium.

Secondary Acquired Cholesteatoma
• Migration Theory – most accepted • Originates from a tympanic membrane perforation• As the edges of the TM try to heal, the squamous
epithelium migrates into the middle ear
Clinical Picturesymptoms 1) Hearing loss (marked) and tinnitus. Sometimes HL is minimal as the sac may
bridges the gap between the necrosed ossicles.
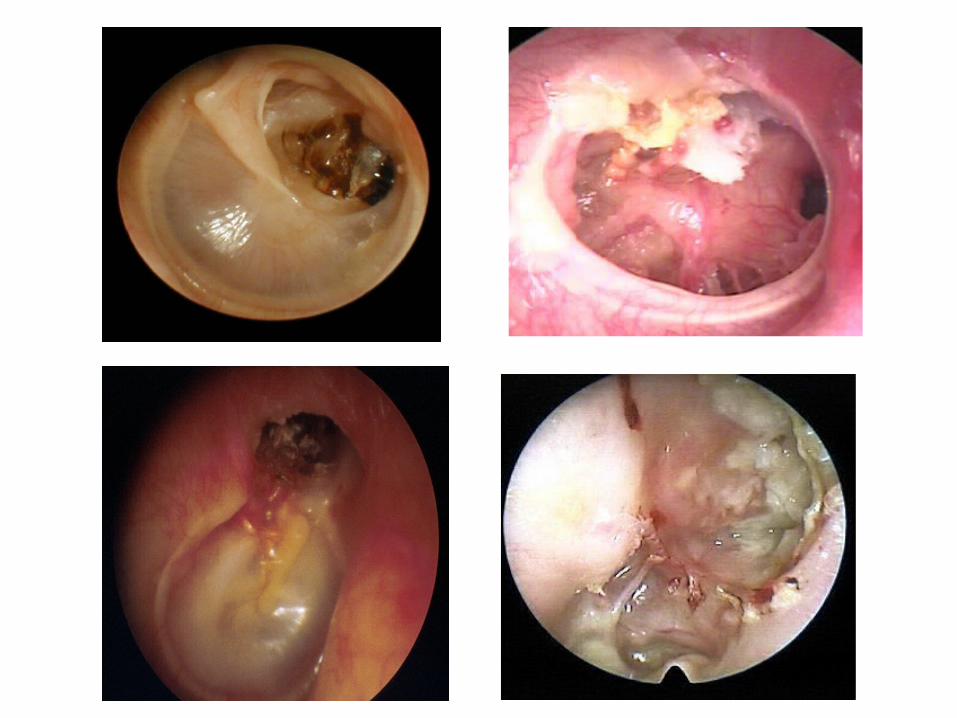
2) Foul smelling ear discharge.Signs1- Fetid scanty purulent ear discharge2- Perforated DM with cholesteatoma debris3- Conductive or mixed HL

Clinical Picture
• Mass behind intact tympanic membrane in cases of congenital cholesteatoma
• Sometimes the first presentation is with one of complications e.g. facial nerve paralysis or lateral sinus thrombophlebitis
• Granulation tissue or aural polyp may fill the ear canal with bloody ear discharge

Investigations
1- Culture and Sensitivity: of the ear discharge.
2- Audiological assessment - CHL, mixed HL or dead ear3- Imaging of the temporal bone: Only in
cases with - Suspected or presence of complications, - Congenital cholesteatoma or - History of previous ear surgery

Imaging of Temporal
Axial Section Coronal Section
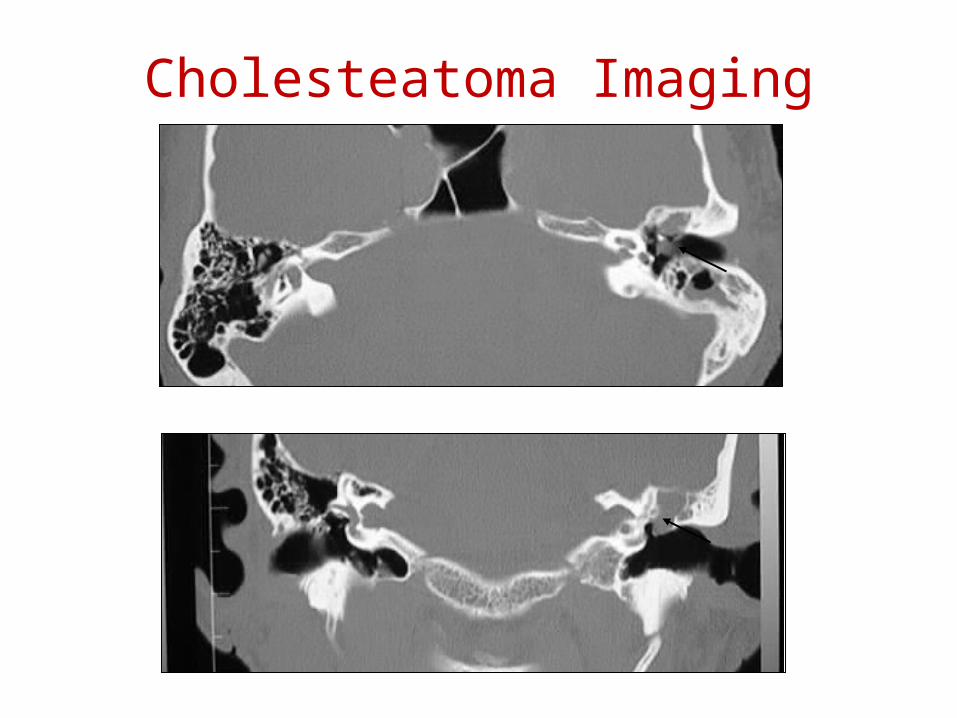
Cholesteatoma Imaging
Treatment of Cholesteatoma
Is Surgical, No role for medical treatment except for active ear infection (ototopical drops)
Tympanoplasty with Mastoidectomy is the standard surgical procedure
In cases with total HL radical mastoidectomy is indicated
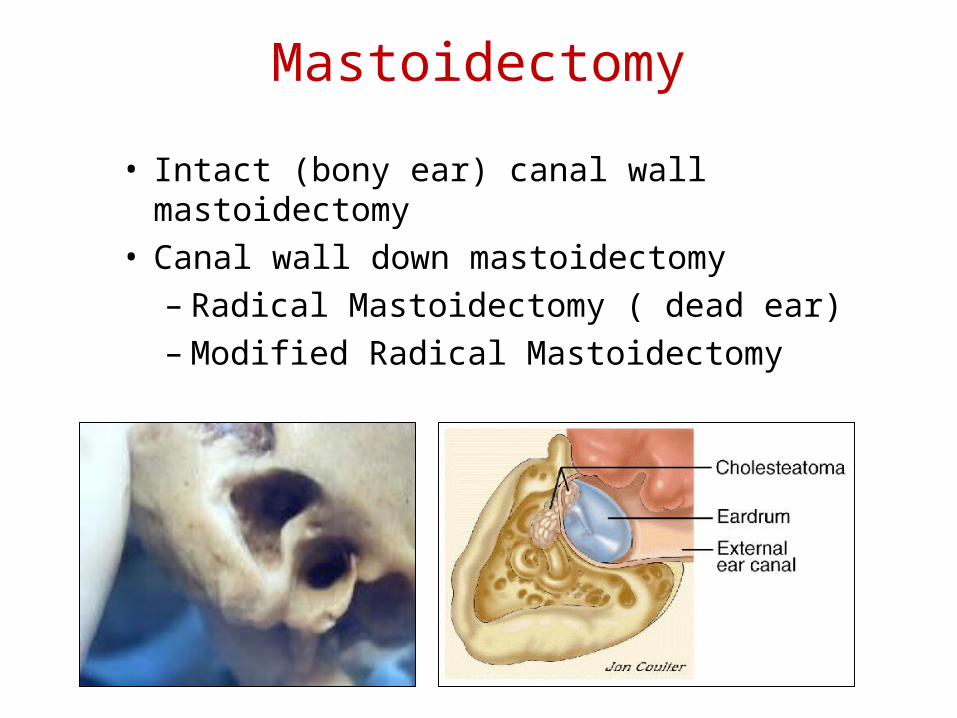
Mastoidectomy
• Intact (bony ear) canal wall mastoidectomy
• Canal wall down mastoidectomy– Radical Mastoidectomy ( dead ear)– Modified Radical Mastoidectomy

Cholesterol Granuloma
CGs, first reported in the mastoid and middle ear in 1894, may occur anywhere in the air cell system of temporal bone when eustachian tube obstruction, mucosal edema, temporal bone fracture, cholesteatoma, chronic otitis media or any another process blocks the air cell tracts.

Cholesterol Granuloma
• Cholesterol granuloma is a histological term used for the description of a tissue response to a foreign body such as cholesterol crystals released by the breakdown of blood and local tissue.
• It may arise any portion of the pneumatized temporal bone but most frequently involves the petrous apex
Cholesterol Granuloma
CG can be a perfectly localized and isolated mass in any pneumatized area in the temporal bone, the middle ear cavity, mastoid antrum, external auditory canal and the petrous apex.
Cholesterol Granuloma
Cholesterol granuloma (CG) of the middle ear typically presents with a conductive hearing loss and a blue eardrum; those at the petrous apex either manifest with side-effects from bony erosion (with sensorineural hearing loss, tinnitus, vertigo or cranial nerve impairment), or are identified as incidental findings .
OTORRHOEA
Definition: Discharge of abnormal material
through the external ear canal
Ear Wax is considered as normal external ear secretion not discharge

OTORRHOEA
Description Amount: Scanty or profuseNature: Watery, mucoid (& muco-purulent), purulent or
bloody (sanginous) Smell: Cholesteatoma & external otitis
OTORRHOEA
The source of ear discharge:1- External ear2- Middle ear3- Intracranial (CSF)

WATERY OTORRHOEA
CSF Otorrhoea: Mostly traumatic- Skull base fracture (commonly the
longitudinal type)- Iatrogenic (post-operative)- Rarely, malignant neoplasm eroding the skull
base
Bloody Otorrhoea
• Traumatic: Trauma of the external, middle ear and skull
base• Inflammatory: Bullous myringitis, acute and chronic otitis
media• Neoplastic:
glomus , carcinoma of external or middle ear

Mucopurulent Otorrhoea
Always from middle ear; Acute and chronic otitis mediaPulsating ear discharge:Acute or acute on top of chronic suppurative
otitis media with small perforation of drum membrane
Intra-cranial complications of suppurative otitis media ( extra-dural abscess)
Muc-opurulent Otorrhoea
Reservoir Sign:Rapid recollection of discharge in the external
ear canal which indicates coalescent mastoiditis

PURULENT OTORRHOEA
External otitis and cholesteatomaUsually smelly (fetid)
Management of cases of ear discharge is according to the cause
N.B. No packing of external ear in suspected cases of CSF otorrhoea.

















