51
LATE RESULTS OF ESOHAGOMYOTOMY IN PATIENTS WITH ACHALASIA PROFESSOR AND CHAIRMAN, DEPARTMENT OF SURGERY, UNIVERSITY OF CHILE DEPARTMENT OF SURGERY UNIVERSITY HOSPITAL
| Date post: | 26-Sep-2018 |
| Category: |
Documents |
| Upload: | truongnguyet |
| View: | 218 times |
| Download: | 1 times |

LATE RESULTS OF ESOHAGOMYOTOMY IN
PATIENTS WITH ACHALASIA
PROFESSOR AND CHAIRMAN,DEPARTMENT OF SURGERY,
UNIVERSITY OF CHILE
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
Which are the late results of oesophagomyotomy in patients with achalasia, usually young adults (40 to 50 years age) with a life expectancy of more than 30 years?
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

There are many articles dealing with surgical treatment of patients with achalasia.
• The majority with follow up less than 5 years• Very few with follow up longer than 10 years• None with follow up longer than 20 years.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

LATE RESULTS IN ACHALASIA SUBMITTED TO OESOPHAGOMYOTOMY
Started 1972 n = 81Closed 1998Follow up ended in 2004 (32 years)Lost from follow up 14 (19%)Included in follow up 67 (81%)- Group I follow up 119 months (15)- Group II follow up 120-239 months (35)- Group III follow up longer to 240 months (17)
Csendes A, Ann. Surg. 2006;243:196.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

ESOPHAGOMYOTOMY IN ACHALASIA
Surgical details.- Good exposure GE junction- Section proximal short vessels- 6 to 7 cms length myotomy in esophagus- 10 to 15 mm on stomach-Dor, partial fundoplication
Csendes A, 2010
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

DETAILS OF ESOPHAGOMYOTOMY
- To assure completeness of myotomy.-To prevent later healing or approximation of muscular bordes of the myotomy.- To avoid too radical myotomy that might result in development of G-E reflux.
Csendes A, 2010
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
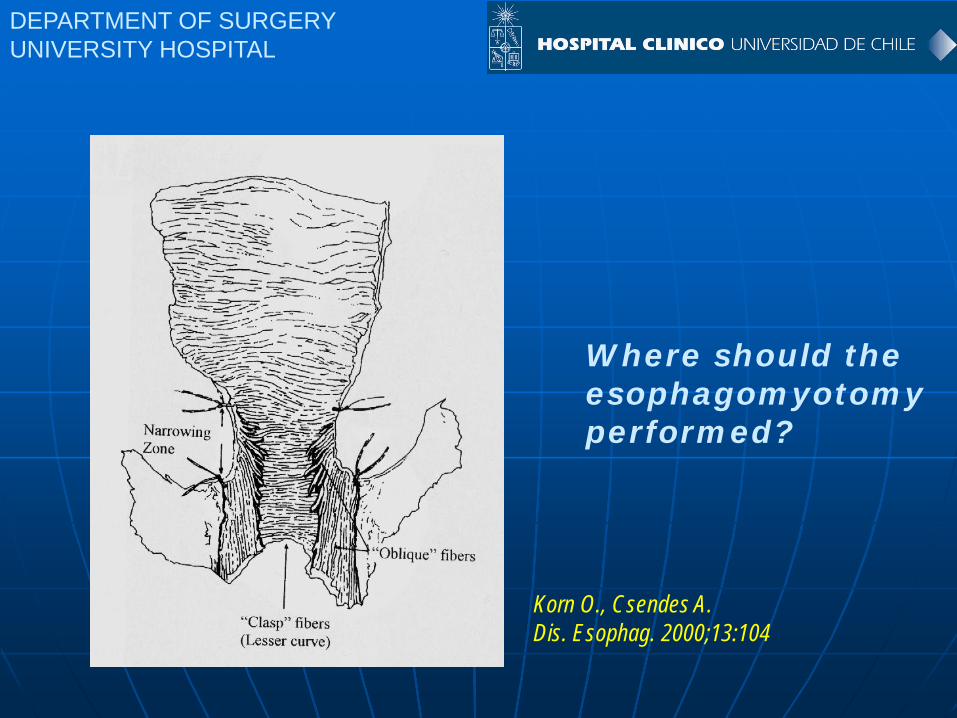
Where should the esophagomyotomyperformed?
Korn O., Csendes A. Dis. Esophag. 2000;13:104

Korn O, Csendes A, Dis. Esoph. 2000;13:104
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

HOW LONG IS THE MYOTOMY AT GASTRIC SIDE?
121 followed 85 months after surgery.- 24% reflux 1 year after surgery.- 48% reflux 10 years after surgery.
Extension of the incision at the stomach more than 2 cms = 100% incidence of reflux.
Jara F., M. Arch. Surg. 1979;114:935-936.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

Dor´s anterior hemifundoplication
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

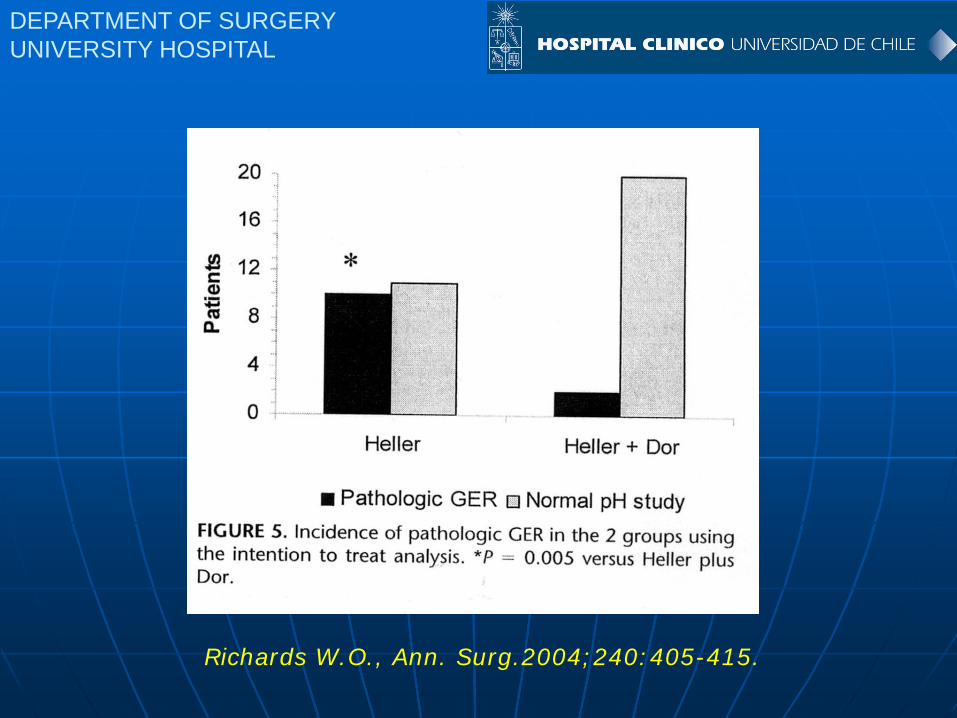
ESOPHAGOMYOTOMY ALONE AND MYOTOMY PLUS PARTIAL DOR FUNDOPLICATION
Prospective ramdomized study:Myotomy alone Myotomy plus Dor
LESP(mmHg) 13.7 13.9 n.s.
24-hrs pH 47.6% 9.1% <0.001
Richards W. O. Ann. Surg. 2004;240:405-415.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
Richards W.O., Ann. Surg.2004;240:405-415.

COMPLICATIONS OF ESOPHAGOMYOTOMY
1.- Mucosal tear, usually at the distal portion.
2.- Not recognized burning of the mucosa.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

LATE RESULTSN = 67
- 3 patients (45%) developed epidermoid carcinoma 8, 9 and 15 years after surgery.
- 64 patients were alive and followed by subjective and objective evaluations.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
CLINICAL AND LABORATORY EVALUATIONS IN ALL PATIENTS N = 64
- Clinical questionnaire 100%- Endoscopic evaluation 100%- Radiological studies 100%- Histological analysis 100%- Manometric evaluation 192 times
(3 times each)- 24 h pH studies 100%
Csendes A, Ann. Surg. 2006;243:196.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

CLINICAL FEATURES OF PATIENTS WITH ACHALASIA SUBMITTED TO OESOPHAGOMYOTOMY
Group I Group II Group III
Follow up (mo) 88 173 281Heartburn 30% 38% 37% n.s.Dysphagia 15% 32% 30% n.s.Gain of weight 100% 97% 94% n.s.
Csendes A, Ann. Surg. 2006;243:196.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
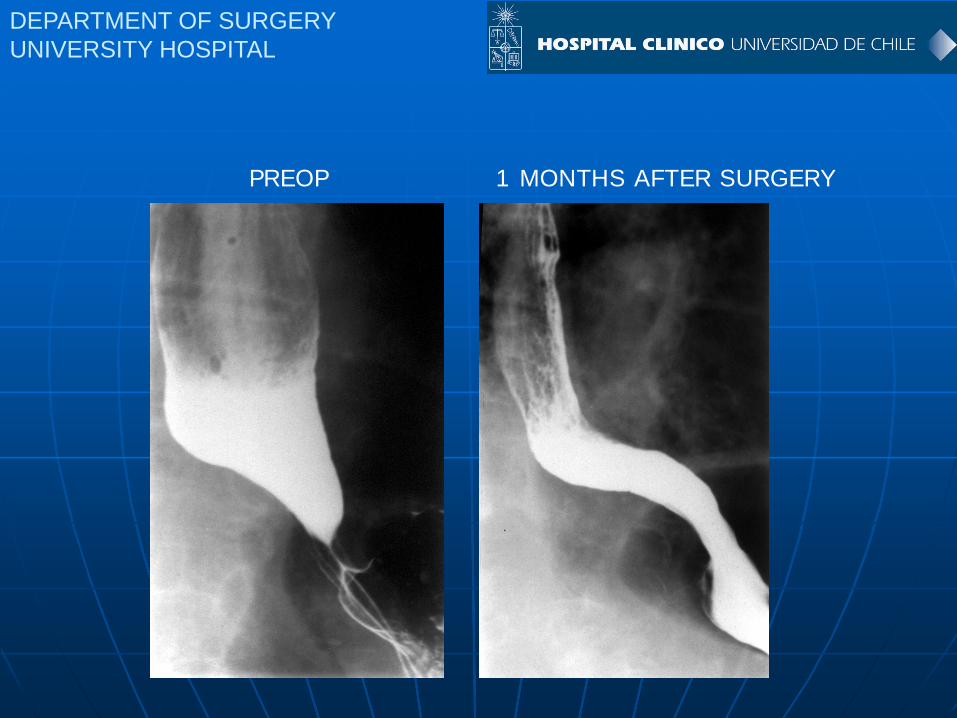
PREOP 1 MONTHS AFTER SURGERY

RADIOLOGICAL EVALUATIONS BEFORE AND 1 MONTH AFTER SURGERY
Internal diameterGO junction
Internaldiametermiddlethirdoesophagus (mm)
0
2
4
6
8
10
12
BeforeOperation
1 monthsafter surgery
P <0.001
P <0.001
05
101520253035404550
BeforeOperation
1 monthsafter surgery
Csendes A, Ann. Surg. 2006;243:196.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

ENDOSCOPIC EVALUATION LATE AFTER OESOPHAGOMYOTOMY
Group I Group II Group IIIn = 13 n = 34 n = 17
Oesophagitis 7.7%(1) 5.9%(2) 29.4%(5) n.s.
Barrett´s Oesophagus 7.7%(1) 17.6%(6) 29.4%(5) n.s.
Carcinoma 15.4%(2) 2.9%(1)
Csendes A, Ann. Surg. 2006;243:196.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

FIG. 1. LOWER ESOPHAGEAL SPHINCTER PRESSURE BEFORE OPERATION AND 1 YEAR AND AT LATE
CONTROL AFTER SURGERY
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
AFTER OPERATIONS
n.s.
P < 0.001 9

05
10152025303540
Preop Lateafter
surgery
mm
Total length L.O.S. Abdominal length L.O.S.
0
5
10
15
Preop Lateafter
surgery
mmn.s.
n.s.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
Csendes A. Ann. Surg. 2006;243:196.

MANOMETRIC FEATURES OF OESOPHAGEAL BODY LATE AFTER OESOPHAGOMYOTOMY
Group I Group II Group IIIn = 13 n = 34 n = 17
Amplitude (mmHg)Preop 19 15 20Postop 38 25 35
% peristalsisPreop 0 0 12%Postop 15 0 17%
Csendes A, Ann. Surg. 2006;243:196.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

% PATIENTS WITH ABNORMAL 24-H pH STUDIES
05
101520253035404550
Group I n =13
Group II n= 34
Group III n= 17
Csendes A, Ann. Surg. 2006;243:196.
n.s n.s
P < 0.05%ofpatients
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
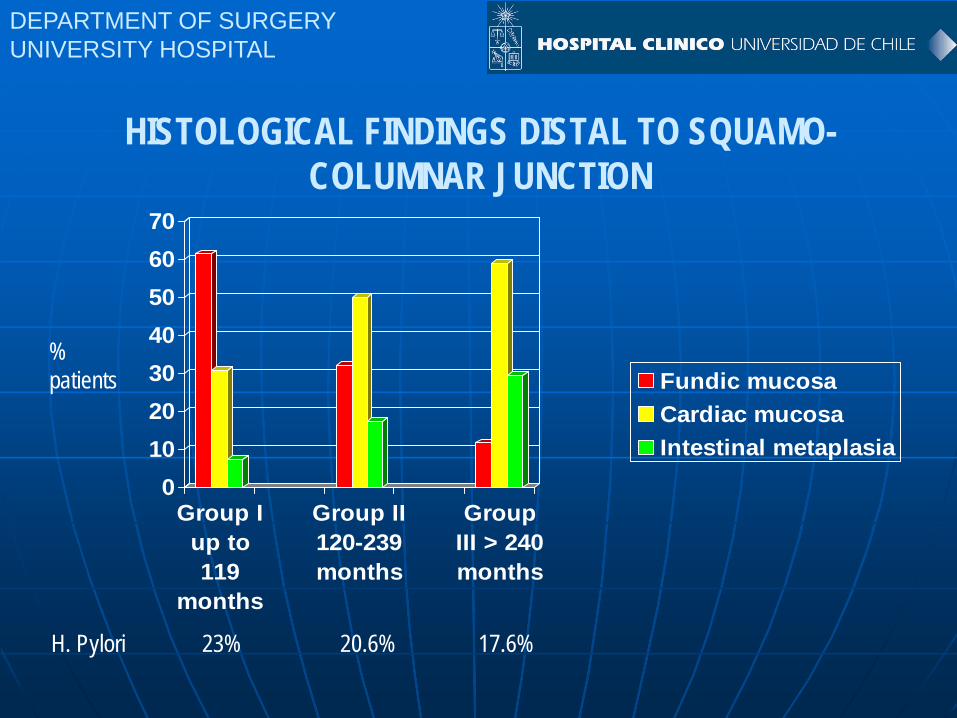
HISTOLOGICAL FINDINGS DISTAL TO SQUAMO-COLUMNAR JUNCTION
%patients
H. Pylori 23% 20.6% 17.6%
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
010203040506070
Group Iup to119
months
Group II120-239months
GroupIII > 240months
Fundic mucosaCardiac mucosaIntestinal metaplasia

24 H pH STUDIES ACCORDING TO THE LENGTH OF BARRETT OESOPHAGUS
N = 12
A.- Short-segment BO: n = 9 (75%)15-25 mm = 17.2%
B.- Long-segment BO: n = 3 (25%)35-40 mm = 24.3%
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
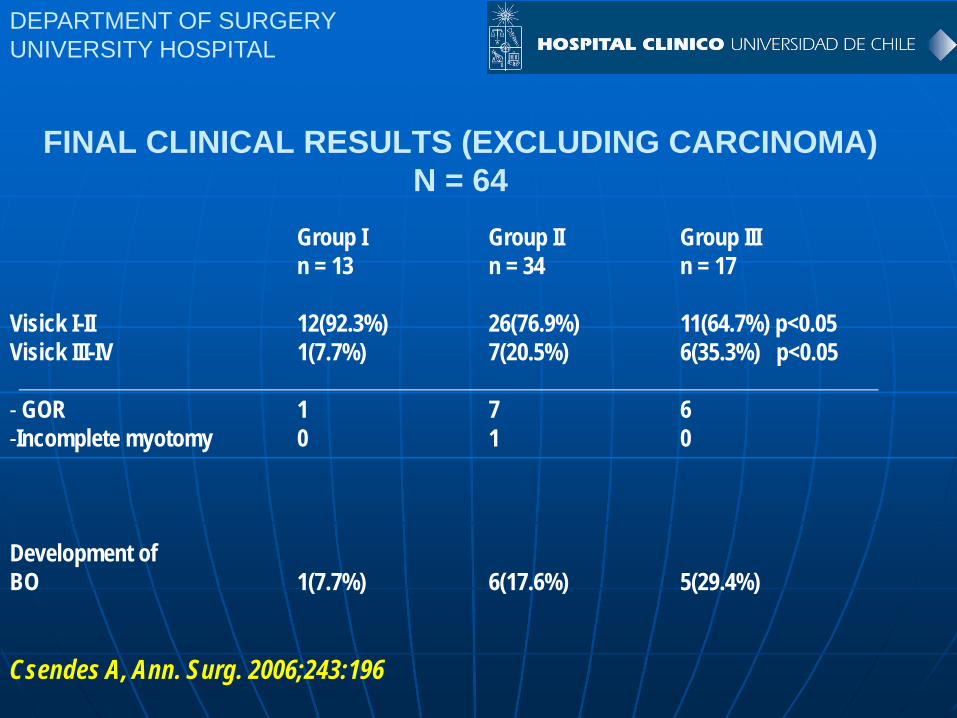
Group I Group II Group IIIn = 13 n = 34 n = 17
Visick I-II 12(92.3%) 26(76.9%) 11(64.7%) p<0.05Visick III-IV 1(7.7%) 7(20.5%) 6(35.3%) p<0.05
- GOR 1 7 6-Incomplete myotomy 0 1 0
Development ofBO 1(7.7%) 6(17.6%) 5(29.4%)
Csendes A, Ann. Surg. 2006;243:196
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
FINAL CLINICAL RESULTS (EXCLUDING CARCINOMA)N = 64

LATE RESULTS IN SURGICALLY MANAGED OESOPHAGEAL ACHALASIA
Pearson G., Ann. Thorac. Surg. 1994;58:1343.
Visick I-II 95% 1 year68% 10 year67% > 20 year
Deterioration of initially good results due to late development of disabling reflux disease.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

LATE RESULTS OF ESOPHAGOMYOTOMY FOR ACHALASIA (FOLLOW UP > 100 MONTHS)
Author n Follow up Improvement GER(months)
Jaakola (1991) 26 104 46% 39%Picciocchi (1993) 101 114 89% 11%Malthaner (1994) 22 120 67% 35%Mineo (2004) 39 107 90% 8%Mathioli (2006) 123 105 88% 8%Csendes (2006) 67 190 73% 25%
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

RESULTS AFTER LAPAROSCOPIC ESOPHAGOMYOTOMY IN ACHALASIA
39 authors3086 patientsFollow up 35 monthsImprovement 89%GE reflux a.- With antireflux surgery 8.8%
b.- Without antireflux surgery 31.5%
Campos G., Ann. Surg. 2009;249:45-57.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
CONCLUSIONS I
1.- Lower oesophageal sphincter pressure remains in a similar low value (near 10 mmHg) along the follow up.
2.- There is no recovery of peristalsis at the late follow up.
3.- Pathologic acid reflux increases significantly as follow up is longer (more than 20 years).
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
CONCLUSIONS II
4.- Intestinal metaplasia at the distal oesophagus appears almost exclusively in patients with abnormal acid reflux.
5.- The prevalence of intestinal metaplasia (Barrett´s oesophagus) increases parallel to the length of follow up.
6.- There is a progressive deterioration of good results if the follow up is very long.
<10 years 92% of Visick I-II> 20 years 65% of Visick I-II
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
“DIFFICULT” ACHALASIAS
N° patients
- With epiphrenic diverticula 4
- “Sigmoid shape” esophagus 6
- Peptic strictures with Barrett´s esophagus 12
- Failed esophagomyotomy 5
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

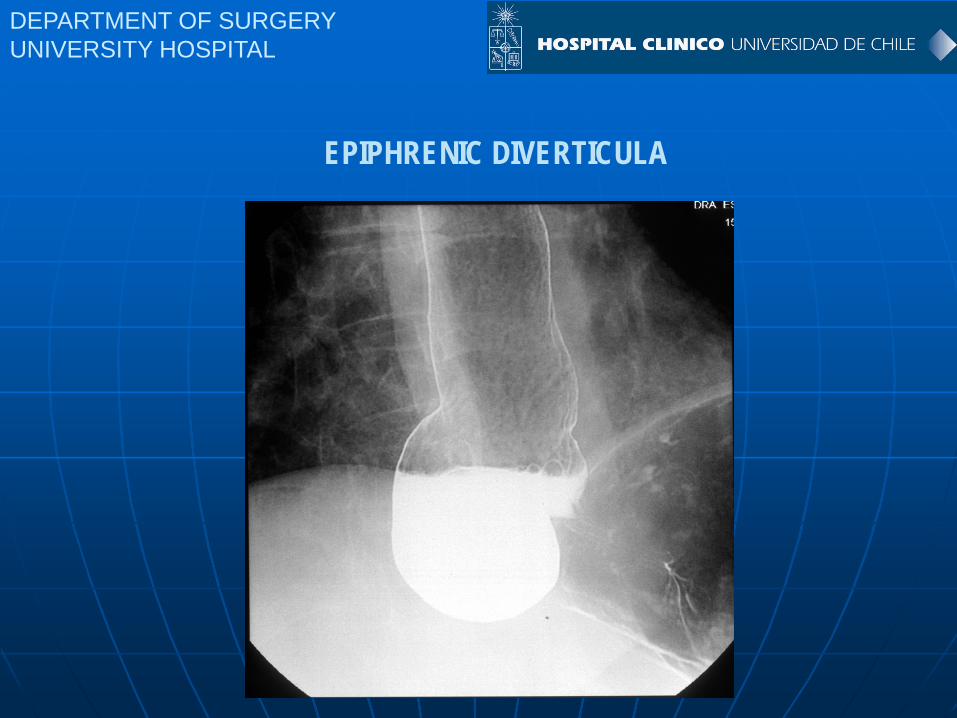
EPIPHRENIC DIVERTICULA
- Laparoscopic approach
- Pinotti´s maneuver
- Extensive dissection of GE junction and distal esophagus
- Resection of diverticula with EndoGIA and placing a bougie 36 inside the lumen.
- Esophagomyotomy plus Dor fundoplication
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
EPIPHRENIC DIVERTICULA

DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
EPIPHRENIC DIVERTICULA

DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
POSTOPERATIVE APPEARANCE

“SIGMOID SHAPE” ESOPHAGUS
- Classic esophagomyotomy = only partial results in 50%.
- Laparoscopic esophaguectomy and gastric ascensus by posterior mediatinum.a.- Complex operationb.- Hemotorax in 2 patients
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
SIGMOID SHAPE ESOPHAGUS

ACHALASIA OF THE ESOPHAGUS: CLASSIFICATION
Type IV Severe:Dilatation > 10 cm(mega-esophagus, sigmoïd)
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

PEPTIC STRICTURES OF THE ESOPHAGUS WITH BARRETT´S ESOPHAGUS
- Laparotomic or laparoscopic approach.
- Inverted cardioplasty+ antrectomy and Roux-en-Y anastomosis.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
Braghetto I, Csendes A., Dis. Esoph. 1998;11:58-61.
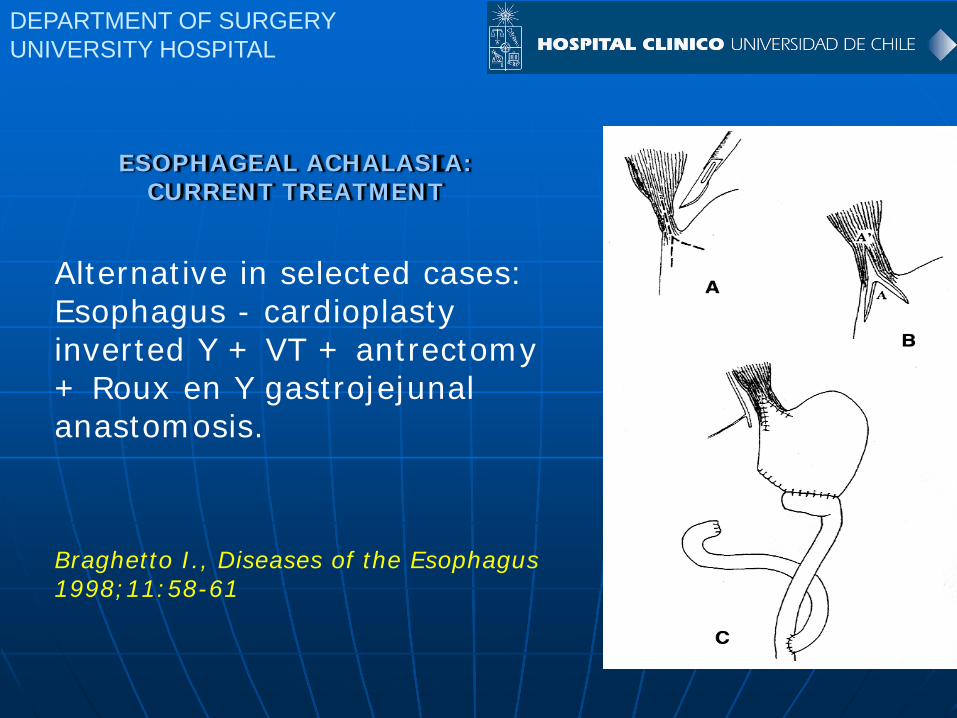
ESOPHAGEAL ACHALASIA:CURRENT TREATMENT
Alternative in selected cases: Esophagus - cardioplastyinverted Y + VT + antrectomy+ Roux en Y gastrojejunalanastomosis.
Braghetto I., Diseases of the Esophagus1998;11:58-61
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
POSTOPERATIVE GASTROESOPHAGEAL REFLUX

DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
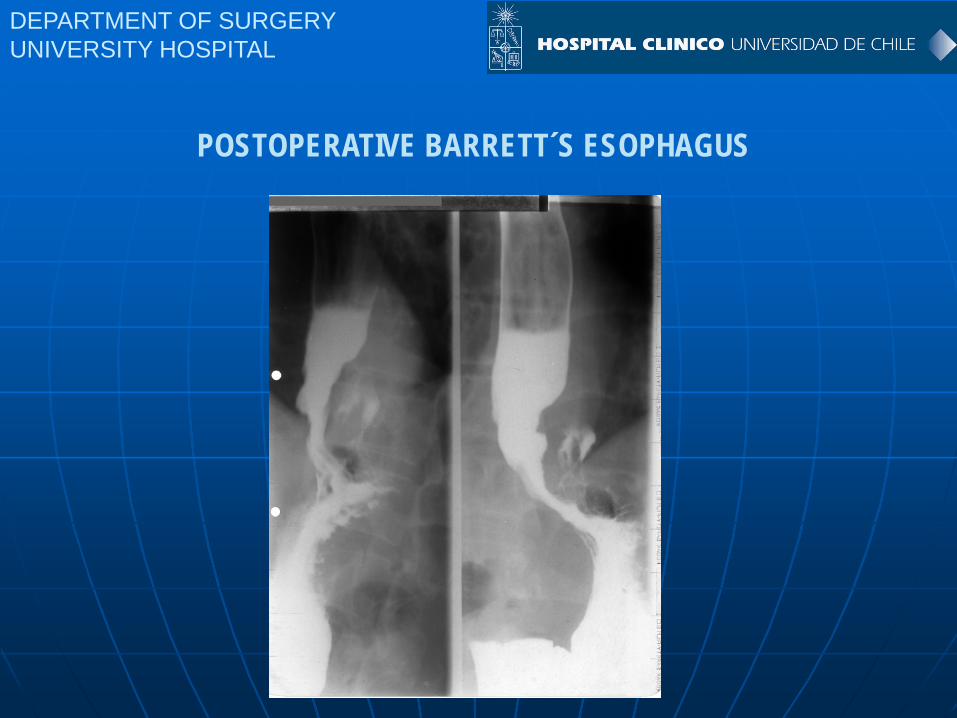
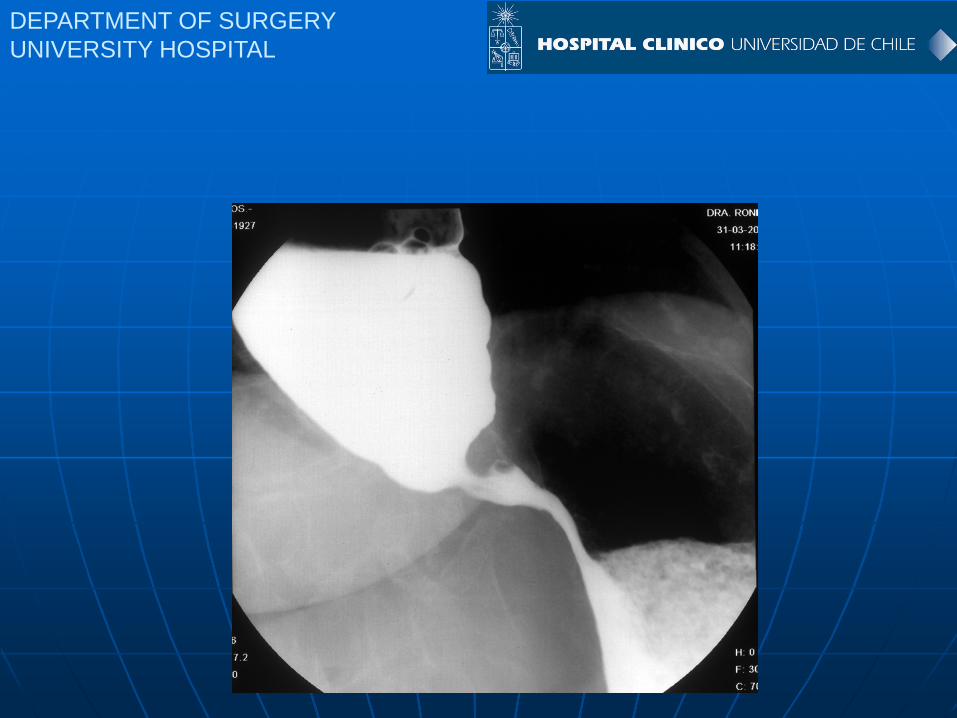
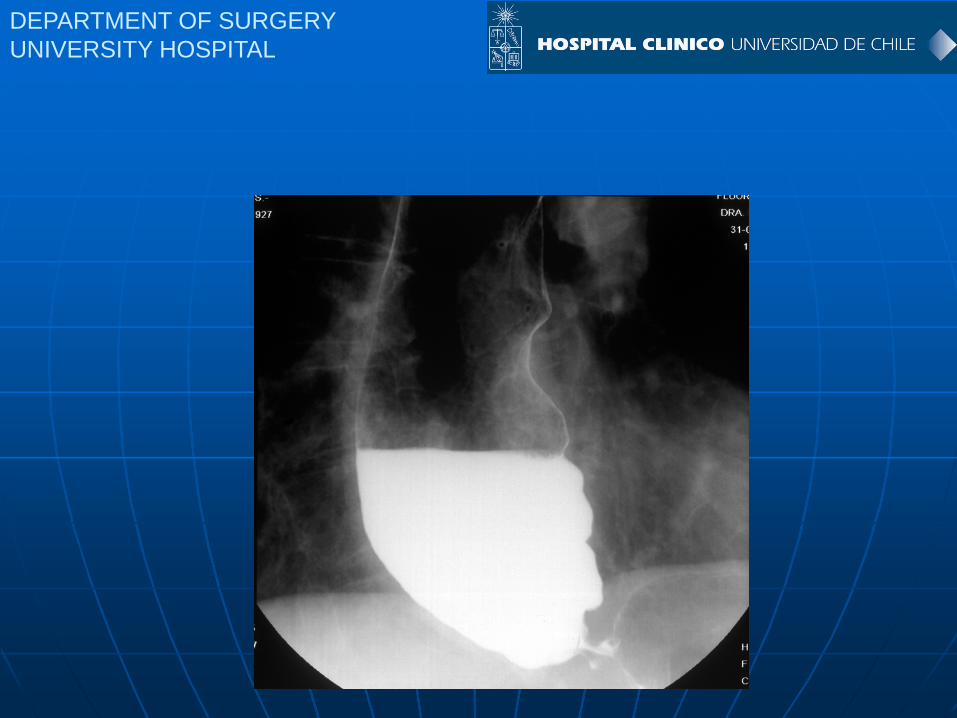
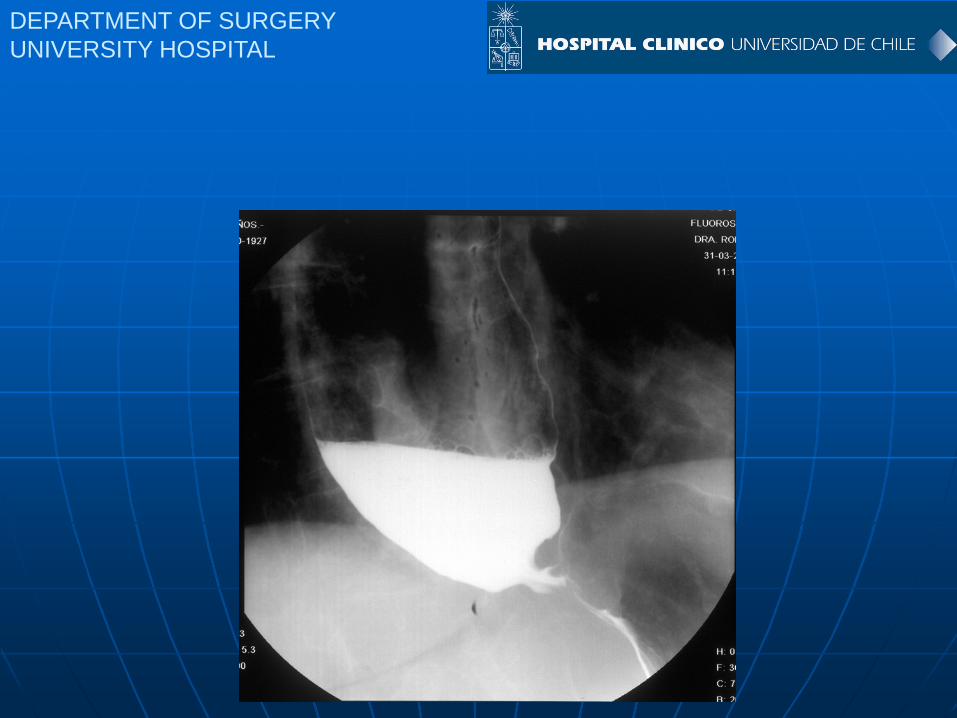
POSTOPERATIVE BARRETT´S ESOPHAGUS
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
POSTOPERATIVE BARRETT´S ESOPHAGUS

CAUSES FOR FAILED ESOPHAGOMYOTOMY
- Short and insufficient esophagomyotomy
- Incomplete myotomy (intact circular fibers)
- Fibrous healing of myotomy.
- Very tight fundoplication.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

FAILED ESOPHAGOMYOTOMY
- Laparotomic reoperation.
- Stricture at the distal end of GE junction.
- Re-myotomy until 15 mm to the stomach and Dor fundoplication.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

WHY A PREVIOUS ENDOSCOPIC THERAPY INCREASES COMPLICATIONS DURING ESOPHAGOMYOTOMY.
1.- With Botox: severe fibrotic reaccion at the GE junction, making difficult to separate muscular layer from mucosa.
Patti M., Dig. Dis. Sci. 1999;44:2270-2276.Horgan S., Surg. Endosc. 1999;13:576-579.
2.- With pneumatic dilatation: It produces hematoma and fibrosis at the GE junction.
Morino M., Surg. Endosc. 1997;11:359-361.Vantrappen G., Gut 1971;12:268-277.West RL., Dig. Dis. Sci. 1998;43:1973-1974.
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

LESSONS LEARNED AFTER 40 YEARS TREATING PATIENTS WITH ACHALASIA.
154 patients laparotomic172 patients laparoscopica.- Abdominal approach is better than thoracic approach.b.- Laparoscopic approach is ideal.c.- Esophagomyotomy at least 6 cms and 10 to 15 mm at the stomach. d.- Partial fundoplication decreases postop. reflux.
Csendes A., 2010
DEPARTMENT OF SURGERYUNIVERSITY HOSPITAL

















