GHENT UNIVERSITY FACULTY OF PHARMACEUTICAL SCIENCES ACADEMIC YEAR 2016 - 2017 DEPRESCRIBING OF PSYCHOTROPIC DRUGS IN PATIENTS ADMITTED TO ORTHOGERIATRIC AND GERIATRIC WARDS Saïn VANDEPOELE INTERUNIVERSITY PROGRAMME: MASTER OF SCIENCE IN HOSPITAL PHARMACY SUPERVISOR KATY VERHELLE, PharmD ANNE VERHAEGHE, PharmD ACADEMIC PROMOTER PROF. ANNEMIE SOMERS, PharmD, PhD
Transcript
GHENT UNIVERSITY
FACULTY OF PHARMACEUTICAL SCIENCES
ACADEMIC YEAR 2016 - 2017
DEPRESCRIBING OF PSYCHOTROPIC DRUGS IN PATIENTS ADMITTED TO ORTHOGERIATRIC AND GERIATRIC WARDS
Saïn VANDEPOELE
INTERUNIVERSITY PROGRAMME: MASTER OF SCIENCE IN HOSPITAL PHARMACY
SUPERVISOR
KATY VERHELLE, PharmD
ANNE VERHAEGHE, PharmD
ACADEMIC PROMOTER
PROF. ANNEMIE SOMERS, PharmD, PhD
GHENT UNIVERSITY
FACULTY OF PHARMACEUTICAL SCIENCES
ACADEMIC YEAR 2016 - 2017
DEPRESCRIBING OF PSYCHOTROPIC DRUGS IN PATIENTS ADMITTED TO ORTHOGERIATRIC AND GERIATRIC WARDS
Saïn VANDEPOELE
INTERUNIVERSITY PROGRAMME: MASTER OF SCIENCE IN HOSPITAL PHARMACY
In this research, the mean number of drugs taken at admission was 10.7± 3.8. The number of drugs in
community dwelling persons with an age over 80 years, reported in a Belgian study of Wauters et al.,
was 5.4 (7) and the presence of polypharmacy and excessive polypharmacy was 57.7% and 9.1%
respectively. Our observation was that 58.3% of the patients took 10 drugs or more which is higher
compared to findings of Wauters et al. A retrospective analysis of patients at geriatric wards in Sydney
observed polypharmacy for 60% of the patients and excessive polypharmacy for 11% of the patients
(44). Another study of Somers et al. which was performed at the geriatric wards of the Ghent university
hospital found an average of 5.9 drugs at admission (17).
It is clear that the number of drugs at admission, revealed in this study, was higher compared to findings
in the literature. This can be explained by several reasons. First, one of the requirements for inclusion
was the minimum intake of 5 drugs. In fact, the complete population of this research was dealing with
‘polypharmacy’ (intake of ≥ 5 drugs). Further, not only regular or chronic medications were taken into
account but also acute and temporary drugs (topical, dermatological, ophthalmological, supplements).
However, some studies reported higher number of drugs. In a study of Page et al., residents of
residential age care facilities were taking an average of 9.3 medicines (18) and in a RCT of Potter et al.
an average of 9.6 regular medicines per patient was found. This may be due to the origin of the patient
(nursing home resident) and the fact that the majority of the patients lived with dementia which can
contribute to a higher number of drugs. In a study of Perehudoff et al. 80% of the patients took 5
medicines or more which is a similar result compared to the findings in this study. The high presence of
polypharmacy could be due to the selection method of the patients. Patients for whom a consultation
with the geriatric liaison team was requested, were included (53).
From our study it can be concluded that the mean number of drugs was higher in women than men.
This result was confirmed by a study in the US in which the number of medications increased with age
and female gender (54).
The mean number of drugs taken at discharge was 11.5 ± 3.6. There was an increase in medicines of
0.8 from admission to discharge. Similar findings were reported in other studies. A study in the US found
an increase of 2.9 drugs on an acute medical service. An increase of 6.0 to 6.2 was reported in an older
population of a Slovakian study and an increase of 4.1 to 4.7 in an older Australian population at
admission (54).
5.1.2. Use of (psychotropic) drugs
The mean ACB score, calculated by the anticholinergic cognitive burden scale by Boustani et al., was
1.3. 26.7% of the included patients had an ACB-score higher than 3. A Belgian health survey of 2013
reported that 7% of the patients, aged over 75 and hospitalized in geriatric departments, had an ACB
score higher than 3 (32). Since it is not clear from this latter survey which anticholinergic rating scale
was used, comparisons are difficult to make. In a similar research, a prevalence of 17.9% was detected
40 | DISCUSSION
when the anticholinergic risk scale (ARS) was used (23). However, it is difficult to extrapolate these
results. The ARS listed only 49 medicines compared to 88 medicines listed in the ACB scale and the
rating score of certain drugs (i.e. quetiapine) was different between the rating scales.
In our study, medicines contributing to anticholinergic burden were not registered. According to Best et
al. patients are most exposed to SSRIs, antipsychotics, opioid receptor agonists, anticonvulsants (44).
Wilson et al. reported similar drug classes which attributed to anticholinergic burden (45).
It was shown that a higher anticholinergic burden was associated with cognitive impairment in older
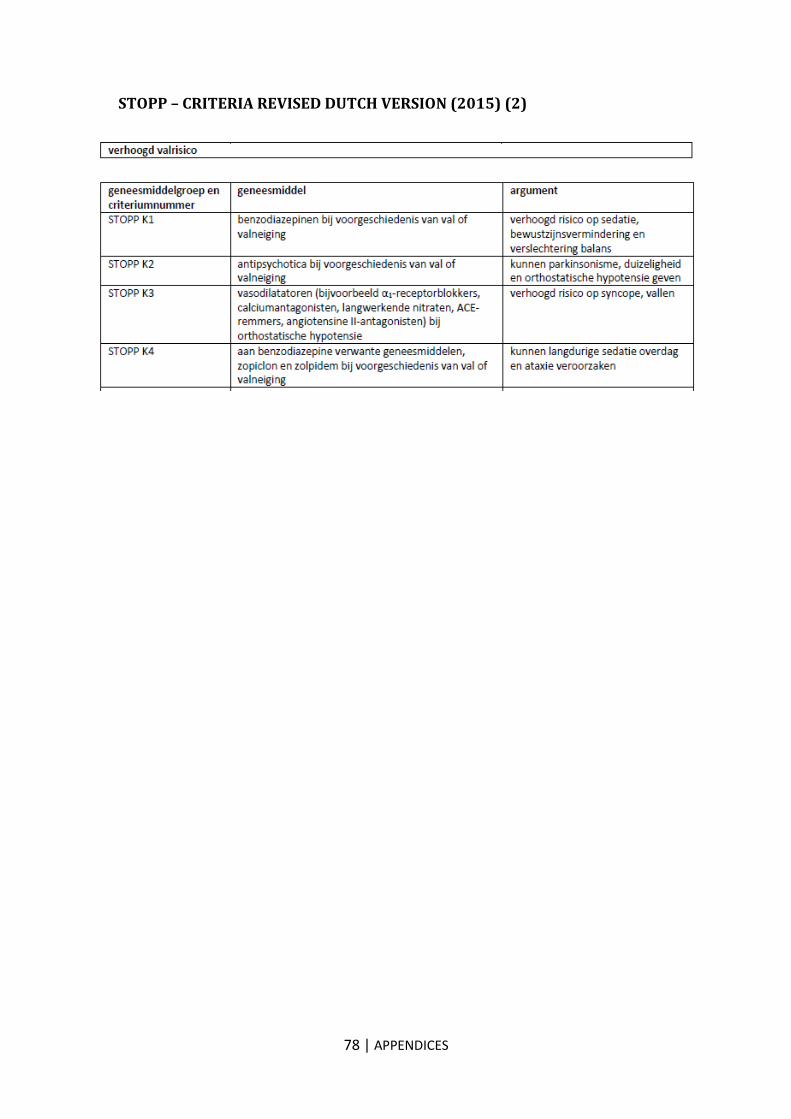
people (33), with delirium related hospital admission (44) and fall incidents (45).
However, is it useful to calculate anticholinergic burden knowing that risk scales seem to simplify
pharmacological mechanisms and do not take into account dose-dependency of anticholinergic adverse
effects and possible synergic and antagonistic effects of medicines (33)?
This study showed a mean vitamin D level in serum of 18.4 µg/L. In a research of Broe et al., the effect
of vitamin D supplement doses in elderly nursing home residents on fall risk was determined. The mean
vitamin D level was similar for this population: 19.5 µg/L. A higher dose of vitamin D was not associated
with a lower risk of falls. However, it was shown that patients taking 800IU cholecalciferol per day had
fewer fall incidents compared to the placebo group. Similar findings were reported in a Swiss and
Australian randomized trial (55). In a meta-analysis of RCTs, it was concluded that a supplementation
of 800 IU vitamin D per day reduced the risk of hip and nonvertebral fractures both for ambulatory and
institutionalized elderly persons. The importance of vitamin D in elderly with bone loss, was attributed
to the beneficial effect on muscle strength and balance (47).
Nevertheless, a British clinical trial found no association between the vitamin D level and the risk on
falls. The explanation was that serum concentrations of vitamin D were higher in healthy patients, which
resulted in fewer falls (55).
In this study, the prevalence of the START criterion ‘vitamin D deficiency in patients with a fracture or
osteoporosis’ had not been documented. Knowing that 72.8% of the patients with inadequate vitamin D
levels (< 30 µg/l) took no vitamin D supplements at admission, the measurement of the prevalence of
this START criterion would be beneficial. In a study of Wauters et al. the absence of vitamin D and
calcium supplements in patients with known osteoporosis or fragility fractures was 9.1% (56) and
according to Dalleur et al. 13.9% (57). This percentages proved the importance of applying the START-
criterion in daily practice.
However, for 120 patients prescribing of vitamin D was suggested by the clinical pharmacist in training.
The effect of this proposed intervention was clear by the shift of drug class with ATC code A on discharge
(Figure 7). The drug distribution at discharge showed an increase of 7% in drugs of the alimentary tract
and metabolism, which contained vitamins such as vitamin D supplements. The high level of acceptance
by the geriatricians was partly due to results revealed by the Belgian health care report. It was revealed
that only 16.2% of geriatric patients in AZ Groeninge stayed with vitamin D during hospitalization. This
was a poor result compared to the national mean of this report in which 50% of the patients stayed with
vitamin D (32). This has convinced the geriatricians to monitor the vitamin D content closely.
In this research 80.4% of the patients were benzodiazepine users. This high percentage may be due to
the predetermined inclusion criteria. Based on the distribution of drug classes by ATC code the
proportion of nervous system drugs was 27.5%. This latter percentage represented a part of all
41 | DISCUSSION
consumed drugs and did not represent the intake per patient. In addition, this distribution was plotted
for all patients during the second study period, including those who did not meet the inclusion criteria.
34% of the patients took psychotropic medications in a retrospective study cohort of patients staying at
the day clinic of geriatrics in Utrecht (58). On the other hand, the Belgian health care report 2013
mentioned a national average of BDZ use of 18% (32). This report seems to underestimate the BDZ use
in the geriatric population compared to other findings.
In this study research, no relationship between the intake of benzodiazepines and fall incidents (p-value
= 0.411) was found. This was against all expectations. The absence of statistical significance may be
due to the low number of non-BDZ users in the study. Secondly, it may be due to the selection of the
patients. 49% was admitted via orthogeriatrics in which the incidence of fall incidents and fractures is
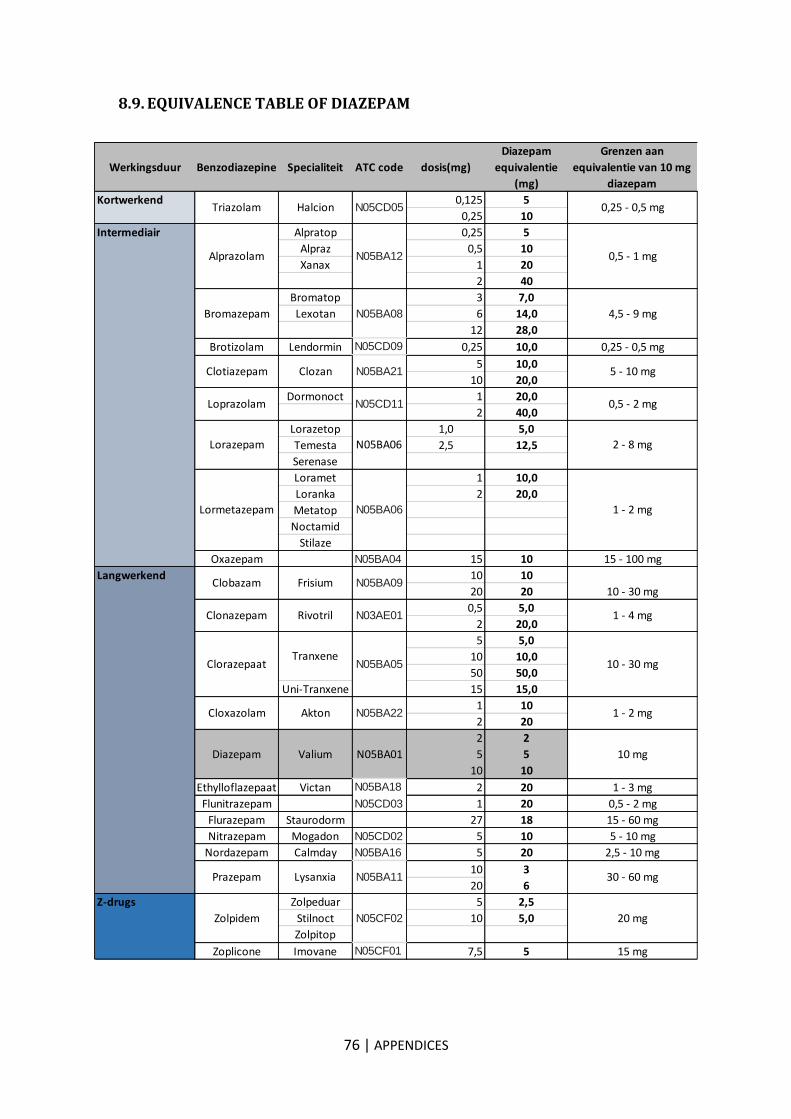
high. Better results would be obtained if diazepam equivalents were linked to fall incidents, rather than
the use of benzodiazepines.
Nevertheless, in a systematic review by Leipzig et al., the relation between fall risk and psychotropic
drugs was investigated. Several studies found an association between falls and the intake of
psychotropic medication such as antidepressants, neuroleptics and benzodiazepines (15; 59).
However, in a study of Van Strien et al. distinction was made between incidental falls and recurrent falls.
In this latter study, only an association between the intake of psychotropic medication and multiple falls
was found. The reason of a single fall was attributed to an underlying cause, but for patients with
recurrent falls the link with psychotropic medication was more obvious.
The effect of antipsychotics on falls was attributed to drug effects on gait and stability. Tapering
antipsychotic medication was found to improve the mobility of geriatric patients (58).
In addition, taking benzodiazepines, including short-and long-acting molecules, would contribute to more
fall incidents. However, it had been concluded that only long-acting benzodiazepines had a higher risk
on fall incidents. This effect can be explained because half-lives of benzodiazepines may seem longer
due to reduced hepatic drug clearance in the elderly (58).
Finally, the link of fall incidents with antidepressants, mainly SSRIs, was demonstrated. These drugs
were described as having a direct effect on fall incidents through their sedative and orthostatic effects.
Next, Strien et al. found significant differences in living situation and sex between psychotropic and non-
psychotropic users. The group of psychotropic users had more females and more patients lived in long
term care facilities or had professional help. A similar result was confirmed in this study, female patients
were more likely to take benzodiazepines (p < 0.001). However the link between benzodiazepine use
and residence in a nursing home could not be confirmed.
Moreover, Strien et al. found that psychotropic medication users took an average of 8.8 medications
compared to 5.1 medicines among non users (58).
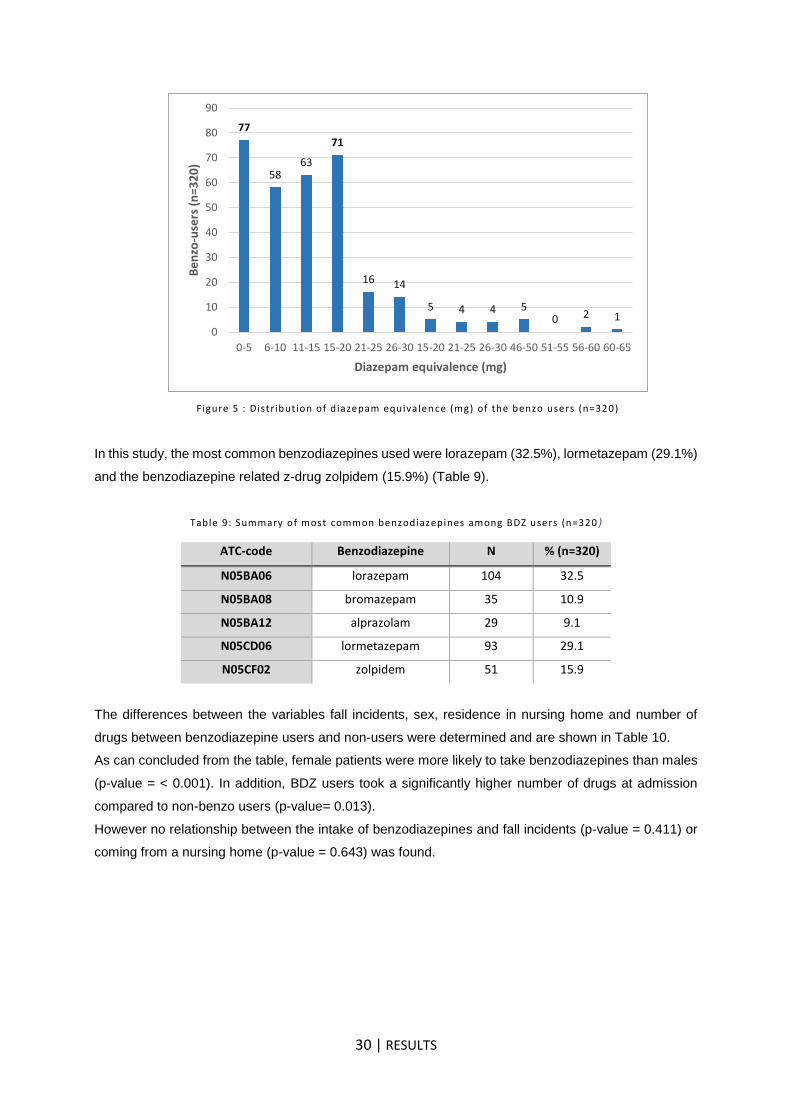
In this research, the largest group of BDZ users had a diazepam equivalent between 0 and 5 or between
15 and 20 mg. The mean diazepam equivalent was 13.5 mg. No similar study reported consumption
data of diazepam equivalents in the elderly. However, in a study of Ray et al. an association between
diazepamequivalents and the rate of falls was reported. A higher risk of falls was associated with higher
diazepam doses (60). The link between diazepam doses and risk on falls was not investigated in this
research.
In this study the most common taken benzodiazepines among benzo-users were lorazepam (32.5%),
lormetazepam (29.1%) and zolpidem (15.9%). Also Wayne et al. observed that the most frequent
intermediate-acting benzodiazepine was lorazepam (64.7% of all benzodiazepine use) (60). The INCB
42 | DISCUSSION
reported a high manufacture of alprazolam, diazepam and lorazepam during the period 2006-2015
which followed the overall trend in consumption. According to a report of ‘The Order of Pharmacists’ in
France, the most consumed benzodiazepines were alprazolam, zolpidem and bromazepam.
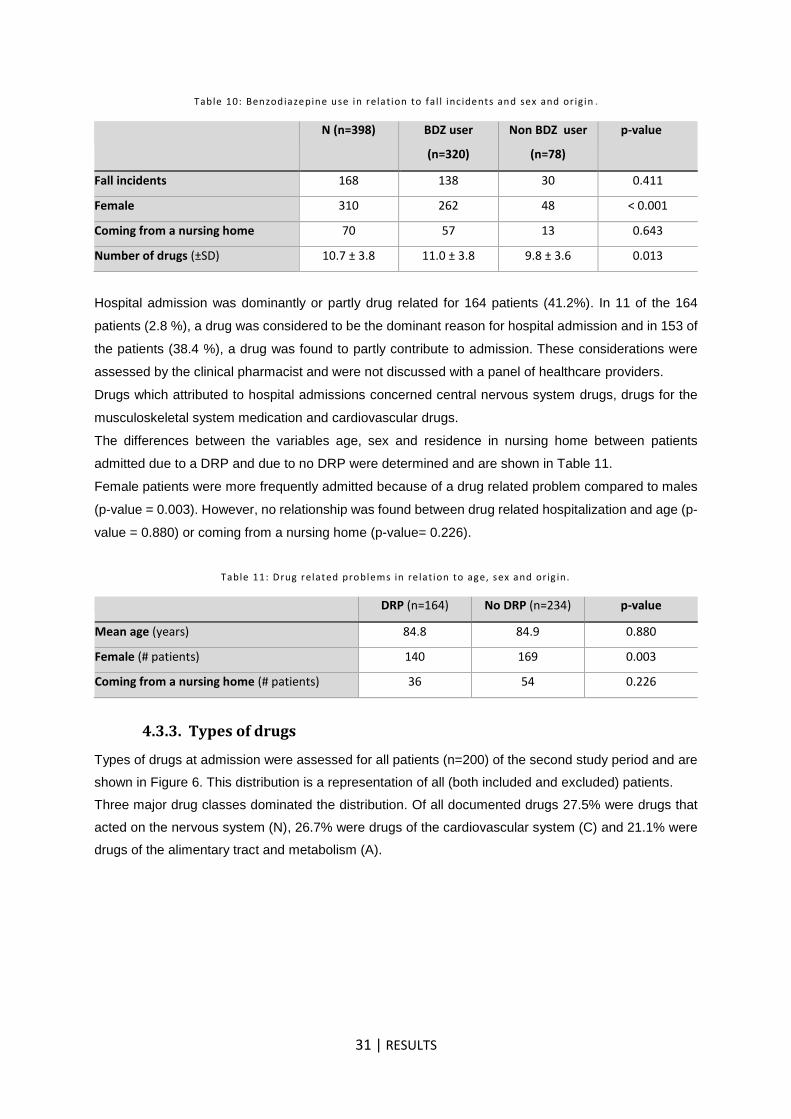
In this study 41.2 % of the admissions were attributable to drug related problems, in which 2.8 % were
considered to be the dominant reason for hospital admission and 38.4% were found to partly contribute
to admission. This percentage was high compared to a study of Somers et al. in which 20.9% of the
patients presented with a drug related admission. Additionally, patients admitted due to a DRP took a
higher number of drugs compared to patients who were admitted because of other reasons. No
relationship between DRPs and residence in nursing home or sex was found according to Somers et al.
(17). No association between DRPs and nursing home residents was found (p-value = 0.226) according
to our study. However, female patients were found to be more admitted because of drug related
problems compared to men (p-value = 0.003).
In a review of Beijer et al, the prevalence of HARMs varied from 0.4 to 41.3%. This variation was
attributed to a large number of studies which reported a lower percentage of ADR related hospital
admissions compared to smaller studies. Moreover, it was shown that the percentage among elderly
was 4 times higher than in the younger population: 16.6% compared to 4.1%. And if hospitalizations
were prevented, 7 times more elderly could be kept out of hospital than non-elderly. A high amount of
money seems to be wasted, thinking of all these preventable hospitalizations (61).
In this study, no relationship between the prevalence of DRPs and age was found. However, patients
admitted due to a DRP were younger compared to patients admitted for another reason according to
Somers et al. Despite the large sample size, the method used to detect DRPs in our study was not well
substantiated. Considerations concerning DRPs were not discussed with other healthcare providers and
the causality of the DRP was not evaluated. Probably this attributed to a higher prevalence of DRPs and
insignificance between the variables.
5.1.3. Types of drugs
The main drug classes at admission were the nervous system drugs (27.5%), cardiovascular drugs
(26.7%) and drugs of the alimentary tract and metabolism (21.1%)
Compared to a study of Perehudoff et al., in which the relationship between discrepancies and potential
clinical outcomes was assessed for patients admitted to non-geriatric wards at the Ghent University
Hospital, the 3 main classes were identical. These consisted of 30% cardiovascular drugs, 19% central
nervous drugs and 16% alimentary tract drugs (53). In a study of Dalleur et al. at the University Hospital
St-Luc in Brussels, the most frequent drugs prescribed in community dwelling older patients were 38.8%
of psycholeptics (N05), 24.3% drugs for acid related disorders (ATC code A02), 23.1% of
psychoanaleptics (N06) and 20.3% of cardiac therapy (ATC code CO1) (57).
In this study, the ATC codes of drugs were not always documented at the time of discharge from the
hospital. For example, medication changes conducted on another ward than geriatric wards were not
documented when the patient was transferred before discharge.
Differences between ATC distribution at admission and discharge are discussed below. In this study the
increase of alimentary tract drugs was one of the largest differences between admission and discharge.
This increase may be due to prescribing of vitamin D and drugs for constipation during hospitalization.
In addition, considering the focus of this project, it is surprising that the subclass A02 only decreased
43 | DISCUSSION
from 99 to 95 drugs. This can be explained by the fact that mostly the dose was reduced (i.e. Pantomed®
40 mg to 20 mg) which had no effect on the ATC code. The ATC code is a classification system and
does not take into account the assumed average maintenance dose per day.
Another remarkable change was the decrease of the proportion of cardiovascular drugs. This reduction
was mainly due to a decrease of cardiac drugs (antiarrhythmics and cardiac glycosides) and a decrease
of lipid modifying agents. The latter drug class was probably stopped during hospitalization because
primary prevention did not benefit from life expectancy.
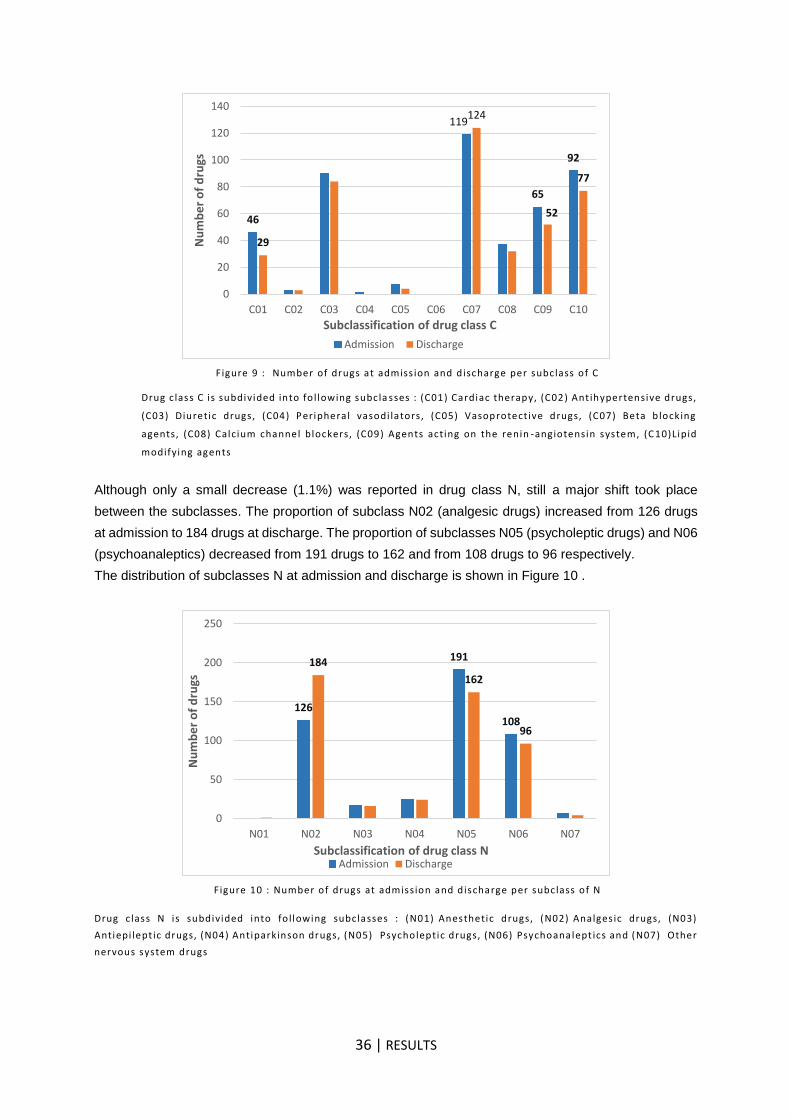
Although the slight decrease (1.1%) of ATC class N compared to admission, the shift of subclasses N
was an important observation in this study. The distribution of the subclasses showed that the proportion
of analgesic drugs had increased strongly (from 126 to 184 drugs). The increase of pain medication was
expected because many patients were recovering from a fall incident and underwent surgery of a knee
or hip replacement. In addition, the increase of oral laxatives could be attributed to the increased
prescription of opioid analgesics at discharge. Although, the association of laxatives with the regular use
of opioids was absent in 10.7% of the cases according to a study of Wauters et al (56). A measurement
of the prevalence of START criteria beyond the scope of this research.
The proportion of psycholeptics (N05) and psychoanaleptics (N06), on the other hand, had decreased
from 191 at admission to 162 drugs at discharge and from 108 to 96 respectively. It would have been
better to distinguish between patients in which only a dose reduction occurred compared to patients in
which a tapering schedule was initiated and the medication was ceased. The ATC code remained the
same for patients who were discharged with a reduced dose of a drug and the proportion of that drug
class did not decrease at discharge. A possibility in the future is to take into account the defined daily
dose (DDD). The defined daily dose is the considered average maintenance dose per day for a drug
used for its main indication in adults. In a study of Tjagvad et al., benzodiazepine prescriptions and
factors associated with increasing amounts of benzodiazepines were studied in patients aged between
18 and 67 years. For each prescription, the numbers of DDD dispensed were measured. In addition,
patients were classified into 2 groups depending on whether they took more (high dose) or less
(moderate dose) than 584 DDD per year. Tjagvad et al. concluded that 30% of the patients was
prescribed more than 365 DDD per year, which indicated a therapeutic amount of benzodiazepine in its
main indication per day or in other words 1 DDD per day. This number indicates an inappropriate use
of benzodiazepines (62). A DDD measurement can detect dose reductions and provides better insight
into drug changes at discharge.
The distribution of the ATC drug classes at discharge was similar to findings in the Belgian health report
2013. In this survey, the prevalence of patients, who had been discharged with psychotropic medication
and PPIs, was 26% and 21% respectively.
These results corresponded to findings reported in the study of Potter et al. in which the most commonly
prescribed new medications were laxatives, analgesics and vitamins in addition to eye drops and topical
antifungal agents (63). Also a study of Somers et al. (2010) showed a decrease in the use of
psychotropic medication and an increase in the use of laxatives (17).
44 | DISCUSSION
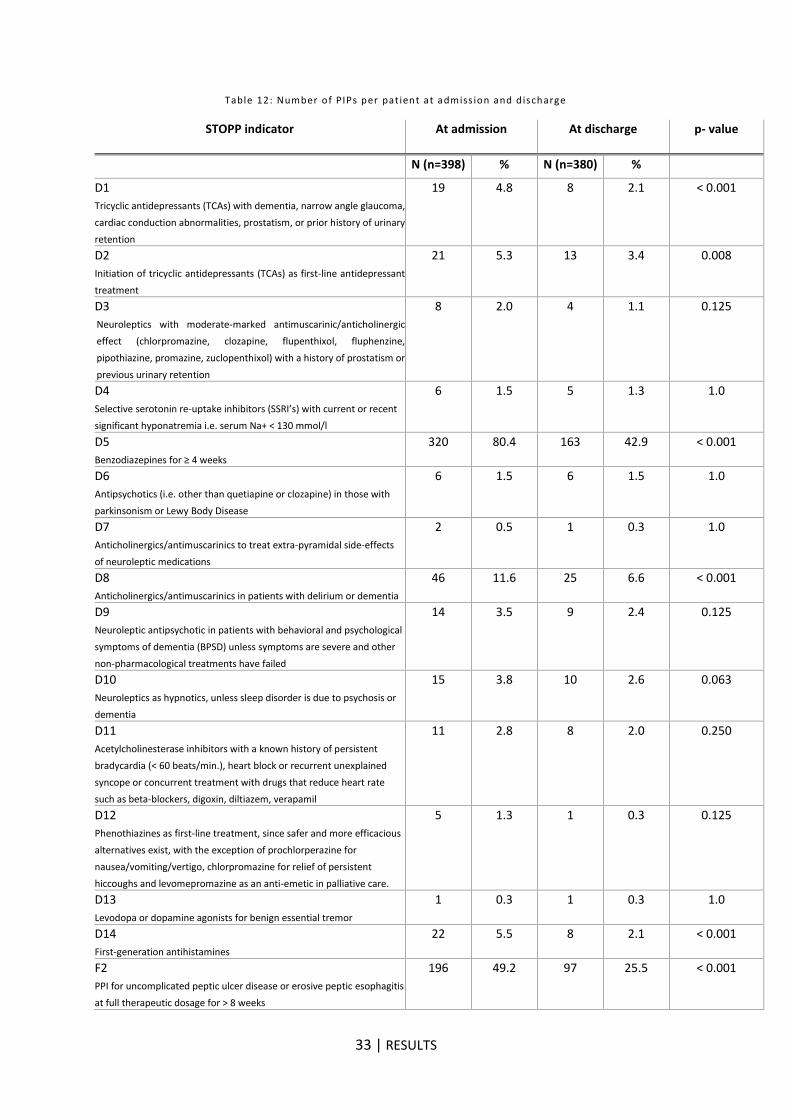
5.1.4. Prevalence of PIPs according to STOPP D
The PIP prevalence of the STOPP criteria category D, observed in this study, was very high: 94.0% at
admission and 66.8% at discharge. A limitation of the registration of PIPs at discharge was that PIPs
resolved without requirement of pharmacist involvement, may not have been documented.
The Mc Nemar test showed that the STOPP indicators D1, D2, D5, D8, D14 and F2 were significantly
different at discharge. The absence of statistical significance in the remaining documented STOPP
indicators may be due to the low incidence in patients.
In a systematic literature review of Tommelein et al. that aimed to determine the prevalence and type of
PIPs for community dwelling patients, the overall PIP prevalence was 22.6% (64). In an investigation of
older patients admitted to six European hospitals, the PIP prevalence was determined by using the
STOPP criteria and was 51.3% (65). The large difference in PIP prevalence could be attributed to
different living situations: community dwelling patients compared to acute sick patients in the hospital.
However, a cross sectional study of a cohort of older Belgian patients in primary care found a PIP
prevalence of 41% (57). Prevalences may vary depending on the selected STOPP criteria and the way
of applying and interpreting the tools by various healthcare providers. Recommendations to improve the
validity and applicability of explicit tools are suggested in the study of Dalleur et al. The validity of explicit
criteria could be improved by mentioning contraindications for criteria and by avoiding contradictions
and overlaps. The applicability of explicit criteria on the other hand, could be improved by clearly
describing the conditions, drug categories and diseases, by suggesting tips and possible alternatives
(57).
The high PIP prevalence of 94% in this study research is probably due to the high number of benzo
users (80.4%) at admission. The STOPP criterium D5 (use of benzodiazepines longer than 4 weeks)
was met for all benzo users and therefore a high overall prevalence was detected.
The most frequently drugs involved in PIPs were anxiolytics, antidepressants and NSAIDs according to
a study of Tommelein et al (64). In our study, the most common drugs involved at admission were
benzodiazepines (80.4%), PPIs (49.2%), anticholinergics (11.8%) and antidepressants (7%). The
prevalence of all these drugclasses was significantly reduced at discharge. A strong decrease of PPI
users and BDZ users took place, from 80.4% to 45.5% and from 49.2% to 25.0% respectively.
The most common contributing STOPP criteria were benzodiazepines and neuroleptic drugs in older
patients with recurrent fall incidents (15.2%) and prolonged prescription of high-dose proton pump
inhibitors (8.2%) according to Gallagher et al. (65). In a research of Wauters et al., in which the impact
of inappropriate prescribing in people aged over 80 years was studied, the most common criterion for
misuse was the intake of benzodiazepines for longer than 4 weeks (35%). In addition, the absence of
vitamin D and calcium supplements in patients with known osteoporosis was 9.1% (56).
A study of Dalleur et al. reported a PIP prevalence of 4.9% for long-acting benzodiazepines (57). The
large difference can be explained by the fact that every intake of a (short or long-acting) benzodiazepine
for more than 4 weeks was recorded in our study. The prevalence of benzodiazepines and neuroleptic
drugs in older patients with recurrent falls was not measured.
45 | DISCUSSION
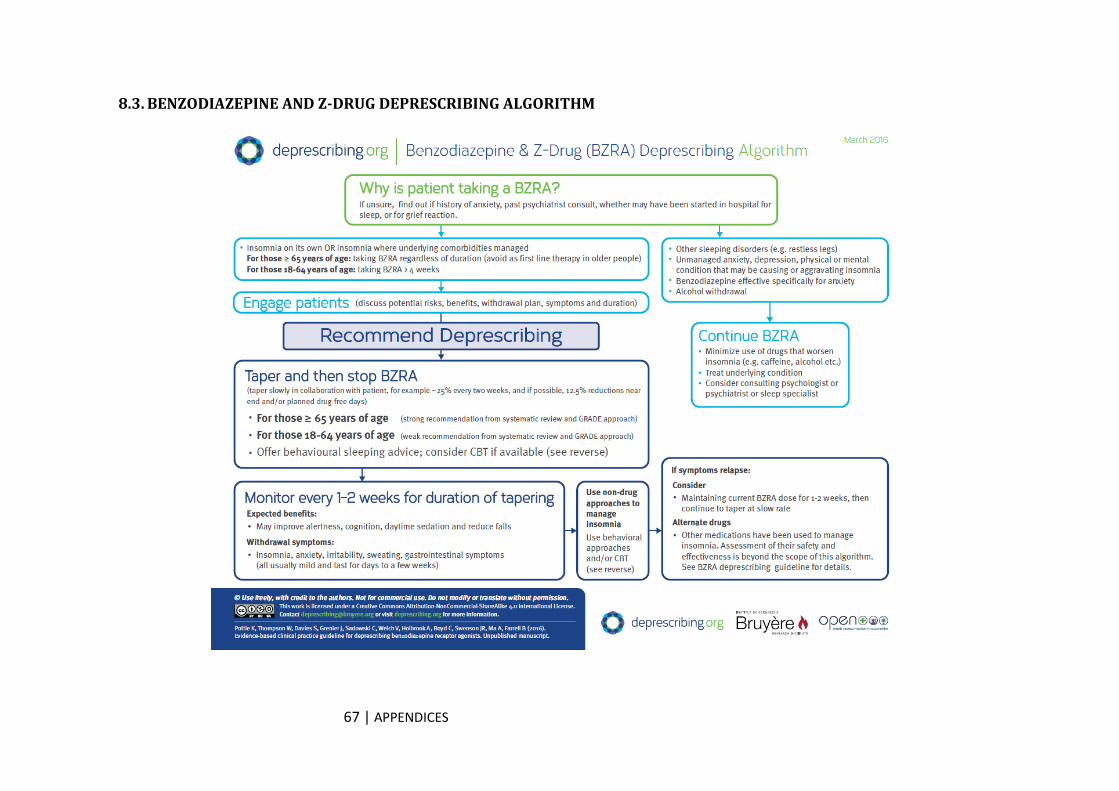
5.2. Deprescribing
In this study 656 drugs or 15.2% of all drugs at admission (n= 4298) were suggested to deprescribe. In
a study of Page et al. even 271 drugs or 58% of all drugs (n=464) of the residents were targeted to
deprescribe (18). Page et al. performed a complete medication review for each resident and thus more
drugs were targeted to deprescribe.
For 75.6% of the patients in this study at least one recommendation was accepted, which is lower
compared to a randomized controlled trial of Potter et al. in which at least 1 drug was tapered in 89% of
the participants. Also in a RCT of Gallagher et al. the acceptance rate was high; 91% of STOPP
recommendations and 97% of START recommendations were accepted and implemented (26). In a
study of Klopotowska et al.in which the participation of a hospital pharmacist in reducing prescribing
errors and HARMs was investigated on ICU, 71% of the recommendations were accepted by the ICU
physicians.
The lower degree of acceptance in our study may be due to the drug classes that were targeted. On the
other hand, no complete appropriateness check of the medication scheme at admission was performed
and less drugs were proposed to deprescribe. Finally in 31 (20.9%) patients was no cessation attempted
since the willingness to cease a medication was absent. In a study of Reeve et al., the patients
willingness to stop medications was checked by administering questionnaires and was found to be 89%
in older patients. However, the real-life acceptance rate of this withdrawal attempt was expected to be
lower (66). In several studies, different acceptances rates are found. For example in a RCT of
community-dwelling older patients with polypharmacy, only 1.5 drugs of the 4.5 recommended drugs
were stopped (67). In a study of Garfinkel al. in which the Good Palliative-Geriatric Practice algorithm
was applied, the success rate for discontinuation was very high (82%) (68). Difference in populations
on the one hand (palliative versus community-dwelling patients) and the types of drug classes that were
targeted on the other hand, can explain the varied degrees of acceptance.
Similar findings were mentioned in a study of Potter et al. in which antidepressants, PPIs and
benzodiazepines had a lower withdrawal success rate compared to other classes such as
biphosphonates, aspirin and iron supplements. It can be concluded that risk-modifying drugs (statins,
aspirin, vitamins) were more successfully tapered than symptom-modifying drugs (analgesics,
antidepressant, hypnotics) (63). The focus of this study is on psychotropic medication and PPIs, which
can explain the lower withdrawal success rate.
In addition, several problems were recurring for certain BDZ users.
A first example was the almost impossible reduction of Flunitrazepam®, a long-acting benzodiazepine
that was equated to narcotic drugs by the Belgian government. Almost all users, included in this study,
refused the withdrawal of this drug. In the past, the addiction to Flunitrazepam®, was already recognized
by the International Narcotics Control Board (INCB). The INCB was concerned about the sale of this
molecule on the illicit market in frequent diversions (69). In this research, telephone conversations with
GPs revealed that this molecule is not frequently prescribed nowadays, only for elderly patients who
took it for years.
A second common problem is the intake of multiple benzodiazepines in alcohol addicts admitted to
hospital. When a patient with problematic alcohol use suddenly stops or reduces drinking, withdrawal
symptoms may occur. Benzodiazepines appear to be the most appropriate therapy to treat alcohol
withdrawal. They act on neurotransmission pathways and have cross-tolerance with ethanol. The
preference is given to long-acting benzodiazepines (Valium®, Tranxene®) because increased
46 | DISCUSSION
compliance and reduced morbidity (due to less pronounced withdrawal symptoms) is expected (70).
Kosten et al. referred to a study in which a significant reduction of withdrawal symptoms was found with
benzodiazepines compared to the placebo group (71). However, for patients with a problematic
benzodiazepine use in combination with a problematic alcohol use, the administration of long-acting
benzodiazepines is contraindicated because of risk on oversedation. But when do we speak of a
problematic benzodiazepine use? Should we substitute all benzodiazepines to an equivalent dose of
diazepam? And if we should add another benzodiazepine, do we run the risk that these patients will get
used to this higher dose? (70; 72). The article of Kosten et al. refers to studies in which carbamazepine
seemed effective in patients undergoing benzodiazepine withdrawal.
One last consideration is the position of alternative medication therapies in the treatment of sleeping
disorders. Considering the increase in the number of prescriptions for psychotropic drugs in Belgium,
we may ask questions about the adequacy of these prescriptions. A number of patients are prescribed
psychotropic drugs while an alternative is possible.
Fytotherapy could be one of the possible alternatives. Herbs such as Passiflora, Valerian and Kava
(pyrones) are often incorporated into plant preparations. The latter is an extract of a pepper plant, but
should cause liver failure and it is not permitted in Belgium. Passiflora preparations are commercialized
and are known under the brand names Sedinal®, Sedistress® and Valdispert®. Valerian is used in
Dormiplant®, Sedistress sleep®, Valdispert®,.. (73) Usually these phytopreparates are not included into
the hospital's formularium and thus alternatives are not systematically presented during the counseling
of the patient. However, the addition of these preparations to a withdrawal scheme of benzodiazepines
could be an option for patients who are convinced they need ‘a sleeping pill’.
Another possible alternative is the use of the hormone melatonin. In Belgium only 1 drug has been
registered, known under the brand name Circadin® at a dose of 2 mg melatonine (73). However,
variable ranges of doses are available in herb shops. The use of this agent was investigated for jet lag,
but according to the SPC this agent has only indications for short-term primary insomnia in people aged
over 55 (74).
And finally, the use of trazodone in low doses (between 25 and 100 mg) is common in the elderly.
Trazodone is used for its sedative side effects, but actually it is indicated for depression in doses
between 150 and 300 mg. The addition of Trazolan® to the patients therapy next to the use of
benzodiazepines is often seen in patients with complaints of insomnia.
5.3. Follow-up
In this study, the follow-up after hospitalization revealed that for 31.1% of the patients the withdrawal
attempt failed. In a review of Reeve et al., some approaches to optimize the patients’ willingness to
cease medications are represented. This includes: presenting deprescribing in a way that does not
provoke stress or fear and does not affect the relationship with the prescriber, by clarifying that the
advice is formulated to achieve therapeutic goals and by making clear the steps of the reduction process.
Furthermore, it is important to consider every adult individually for deprescribing and to mention that
deprescribing is a trial (75; 66).
In a systematic review of 31 studies was found that diuretics, antihypertensives and psychotropic
medication could be discontinued without problems. Especially psychotropic medication had a high risk
of relapse (63).
47 | DISCUSSION
In several articles, the need for follow-up after discharge was emphasized in which the patients
preference was a face-to-face conversation over a telephone call (75). However, in a study of Haynes
et al., which objective was to determine the role of a pharmacist in improving care transitions, also follow-
up calls were performed. These post-discharge calls were conducted by non-healthcare professionals,
making this follow-up less time-consuming and less expensive than when performed by a pharmacist.
However, some pharmacists preferred to conduct the follow-up call personally (39).
On the other hand, in a study of Gujral et al. the impact of CPs on discussing patients’ belief about their
myocard infarct drugs did not improve the medication adherence at 12 months. In this latter study, a
face-to-face conversation by the researcher 5 to 6 weeks after discharge preceded the telephone call
conducted by the CP 3 months after discharge (76). However according to a review by Nazar et al., in
which the contribution of CPs in improving transfer of care was studied, CPs could play a role in the
identification of DRPs. The interventions of CPs in the reviewed studies were characterized by home
visits within a certain period of time after discharge, reporting discrepancies in the prescribed drugs after
comparison with the medication schedule at discharge or by a medical review a few months post-
discharge (37). It is clear that in also in our study the follow-up after discharge was an added value.
However, the interviewer did not use a standardized questionnaire that determined sleep quality and
possible withdrawal symptoms. In a study of Baldwin et al. the association between sleeping disorders
and the effect on quality of life (QOL) was investigated by using the short form (SF) – 36 questionnaire.
This was a measurement for health-related quality of life including questions about physical and social
activities, pain, mental health, emotional problems, vitality and general health perceptions. Another
example of a questionnaire which focused specifically on sleep habits was the Sleep Habits
Questionnaire (SHQ) which was completed by patients in the study of Baldwin et al (77). There are
plenty of ways to measure sleep quality or quality of life, which is also recommended to be used in future
research when conducting a follow-up call post discharge.
5.4. Strengths and limitations of the project and future perspectives This was a single center observational prospective study. In ideal circumstances, a prospective
multicenter randomized controlled trial would have been performed. To determine if the results are
generalizable, this study should be performed in several care settings including those in primary care
and nursing home care. In addition, this study was only performed on geriatrics, while geriatric patients
were spread throughout the hospital. It would be an opportunity to extend this project hospital-wide with
the focus on non-psychiatric patients with long-term benzodiazepine use.
The full potential of interventions would be more appreciated if there was a comparison with a control
group rather than comparison with uncontrolled ‘usual care’. According to Thompson and Schoenfeld,
the use of a usual care-arm is appropriate in two-armed randomized controlled trials for drug and devices
and for non-pharmacological interventions lying well outside usual-care practices (37).
Medication reconciliation was found to be the key factor in improving care transitions according to
Haynes et al. Benefits that were cited were: clarifying certain drug therapies for the patient and enabling
communication with the doctors (39). Also in this study research, discrepancies or recent therapy
changes in the medication scheme were often revealed which took extra time when making
recommendations in the EMR. Medication reconciliation is certainly an added value but was beyond the
scope of this project, considering the amount of time required.
48 | DISCUSSION
Furthermore, factors as potential drug-drug or drug-disease interactions and adherence but also
outcome parameters such as life expectancy, future risk of ADRs and quality of life were not assessed
in this research and would be beneficial. The addition of a pharmaco economic analysis would be
opportune (75).
In future studies, deprescribing should be applied for all categories of the STOPP criteria when detecting
inappropriate prescriptions. In addition, also the START criteria should be screened because the effect
of misuse and underuse is often omitted. According to a study of Wauters et al., it was demonstrated
that patients with a high underuse (3 drugs or more) have a 3.3 fold higher risk of mortality and a 2.8
fold higher risk of hospitalization compared to patients without underuse. The effect of misuse was
associated with a higher risk for hospitalization, but not for mortality (56).
Another future perspective would be the counseling of patients at discharge. This session, led by a
clinical pharmacist, can help patients understand their new medication regimen and can anticipate
barriers to noncompliance. A teach-back method, which is mostly not performed by nurses due to lack
of time, could improve understanding medication related problems (39).
Finally, the information exchange should occur between all healthcare actors, with the necessary
information security and protection. An electronic platform of healthcare, called eHealth, was established
by the Belgian government in 2008. This allows an electronic exchange of health data through different
systems. One of the systems is called Vitalink; this platform includes a vaccination platform (Vaccinet),
an exchange platform for medication schemes and includes sumEHR (Summarized Electronic Health
Record). The latter is an encrypted and structured file which is accessible for GPs, for specialists in the
hospital and for the patient but not for (hospital) pharmacists. Nevertheless, these applications are still
in development and are faced with problems such as inadequate usability in software packages (41).
1. HUGHES SG. Prescribing for the elderly patient : why do we need to exercise caution ? 46, London: Br J Clin Pharmacology, 1998.
2. MANGONI AA, JACKSON SHD. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. London : British Journal of Clinical Pharmacology, 2003.
3. GARFINKEL D, ILHAN B, BAHAT G. Routine deprescribing of chronic medications to combat polypharmacy. Israel: Ther. Adv. Drug Saf, 2015.
4. PAGE RL. Inappropriate prescribing in the hospitalized elderly patient= Defining the problem, evaluation tools and possible solutions. Colorado: Clinical Interventions in Aging, 2010.
5. KONRAT C, BOUTRON I. Underrepresentation of Elderly People in Randomised Controlled Trials. The Example of Trials of 4 Widely Prescribed Drugs. Parijs: PLoS ONE, 2012.
6. SALZMAN SL. Medication compliance in the elderly.: J Clin Psychiatry. , 1995.
7. WAUTERS M, ELSEVIERS M. Polypharmacy in a Belgian cohort of community dwelling oldest old (80+). Ghent: International Journal of Clinical and Laboratory Medicine, 2016.
8. WASTESSON JW, CANUDAS-ROMO V, LINDAHL JACOBSEN R, JOHNELL K. Remaining Life Expectancy With and Without Polypharmacy: A Register-Based Study of Swedes Aged 65 Years and Older . Denmark: Elsevier, 2015.
9. LIU ML. Deprescribing: An Approach to Reducing Polypharmacy in Nursing Home Residents. Waltham: The journal for nurse practitioners, 2014. 136-139.
10. SCOTT IA, JAYATHISSA S. Quality of drug prescribing in older patients: is there a problem and can we improve it? Australia: Internal Medicine Journal, 2010.
11. SCOTT IA., GRAY LC, MARTIN JH. Deciding when to stop: towards evidence-based deprescribing of drugs in older populations. 18, Australia: Evid Based Med, 2013. 4.
12. MARTIN L, WILLIAMS L, HASKARD KB. The challenge of patient adherence. California: Therapeutics and clinical risk management, 2005.
13. MAHER RL, HANLON JT, HAJJAR ER. Clinical consequences of Polypharmacy in elderly. Pittsburgh: NIH-PA, 2014.
14. SHOBHA S. Prevention of falls in older patients. Texas: American Academy of Family Physicians, 2005.
15. LEIPZIG RM, CURNRNING RG. Drugs and Falls in Older People: A Systematic Review and meta-analysis I : Psychotropic drugs. New York: The American Geriatric Society, 1999.
16. BAYÓNA AR, SAMPEDRO FG. Inappropriate treatments for patients with cognitive decline. Santiago de compostela: Elsevier, 2012.
17. SOMERS A., ROBAYS H, VANDER STICHELE R. Contribution of drug related problems to hospital admission in the elderly. Ghent: JNHA, 2010.
18. PAGE AT, ETHERETON BEER CD, CLIFFORD RM, BURROWS S. Deprescribing in frail older people – Do doctors and pharmacists agree?. Australia: Elsevier, 2015.
52 | REFERENCES
19. FARRELL B. What are priorities for deprescribing for elderly patients ? Capturing the voice of practiioners : a modified Delphi process. Sweden: Plos One, 2015.
20. GNJIDIC D, LE COUTEUR D, KOULADJIAN L, HILMER NS. Deprescribing Trials: Methods to Reduce Polypharmacy and the Impact on Prescribing and Clinical Outcomes . Clinics in Geriatric Medicine Elsevier, 2012.
21. MAIR A, FERNANDEZ-LLIMOS F. Polypharmacy management programmes: the SIMPATHY project. Edinburgh: European Journal of Hospital Pharmacy, 2017, Vol. 24.
22. ROCHON PA. Drug prescribing for older adults. www.uptodate.com. [Online] https://www.uptodate.com/contents/drug-prescribing-for-older-adults.
23. ROGGE A. Medicatiebegeleiding bij ontslag uit de geriatrische afdeling van het ziekenhuis en overdracht van het medicatieschema naar de openbare apotheek. Gent: Universiteit Gent, 2016.
24. BJERRE LM, HALIL R, CATLEY C. Potentially inappropriate prescribing (PIP) in long-term care (LTC) patients: validation of the 2014 STOPP-START and 2012 Beers criteria in a LTC population—a protocol for a cross sectional comparison of clinical and health administrative data. BMJ OPEN, 2015.
25. CULLINAN S. Use of a frailty index to identify potentially inappropriate prescribing and adverse drug reaction risks in older patients. Age and ageing, Cork : Oxford University, 2015.
26. GALLAGHER PF, O’CONNOR MN, O’MAHONY D. Prevention of Potentially Inappropriate Prescribing for Elderly Patients: A Randomized Controlled Trial Using STOPP/START Criteria89, Ireland: Clinical pharmacoly and therapeutics, 2011. 6.
27. OPONDO D, ESLAMI S, VISSCHER S. Inappropriateness of Medication Prescriptions to Elderly Patients in the Primary Care Setting: A Systematic Review. Amsterdam: PLOS one, 2012.
28. VANDENHOVEN J. Polyfarmacie bij ouderen: toepasbaarheid van de Nederlandse multidisciplinaire richtlijn Polyfarmacie bij ouderen in België. Gent: Universiteit Gent, 2015.
29. PANEL AMERICAN GERIATRICS SOCIETY 2015 BEERS CRITERIA UPDATE EXPERT. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. JAGS, 2015.
30. GOKULA M, HOLMES HM. Tools to reduce polypharmacy. USA: Clin Geriatr Med, 2012.
31. WILMA KNOL, MONIQUE M, VERDUIJN. Onjuist geneesmiddelgebruik bij ouderen opsporen : de herziene STOPP- en START criteria. Nederland: Nederlands tijdschrift Geneeskunde, 2015.
32. Prescription of 10 (+1) drugs in the Belgian geriatric wards. RIZIV : Rijksinstituut voor ziekte- en invaliditeitsverzekering. [Online] [Cited: 1 28, 2017.] http://www.riziv.fgov.be/SiteCollectionDocuments/symposium_polymedication_poster07.pdf.
33. SALAHUDEEN MS, DUFFULL SB. Anticholinergic burden quantified by anticholinergic risk scales and adverse outcomes in older people: a systematic review. P.S. New Zealand: BMC Geriatrics, 2015.
34. HANEVELD, KLEIN H. Psychiatrienet.nl. [Online] De tijdstroom. [Cited: januari 20, 2017.]
35. CASSELS A. 'Can I stop even one of these pills?' The development of a tool to make deprescribing easier. Canada: European journal of hospital pharmacy, 2017, Vol. 24.
36. MC CORMACK J. www. Medstopper.com. Medstopper. [Online] [Cited: januari 20, 2017.]
53 | REFERENCES
37. NAZAR H. A systematic review of the role of community pharmacists in improving the transition from secondary to primary care. United Kingdom: British Journal of Clinical Pharmacology, 2015.
38. KRIPALANI S. Promoting Effective Transitions of Care at Hospital Discharge: A Review of Key Issues for Hospitalists.. Georgia: Journal of Hospital Medicine, 2007.
39. HAYNES KT. Pharmacists’ Recommendations to Improve Care Transitions The Annals of Pharmacotherapy , 2012.
40. KRIPALANI S. Effect of a Pharmacist Intervention on Clinically Important Medication Errors After Hospital Discharge. Boston: Annals of Internal Medicine, 2012, Vol. 157.
41. STORMS H, MARQUET K, NELISSEN K, HULSHAGEN L, LENIE J, REMMEN R, CLAES N. Implementing an electronic medication overview in Belgium.. Belgium: BMC, 2014.
42. FARMAKA. GENEESMIDDELENBRIEF : Deprescribing deel 2. Farmaka, 2015.
43. PAGE AT, POTTER K, CLIFFORD R Deprescribing in older people. Australia: Elsevier, 2016.
44. BEST O. Investigating polypharmacy and drug burden index in hospitalized older people. Australia: Internal Medicine Journal, 2006.
45. WILSON NM. Associations Between Drug Burden Index and Falls in Older People in Residential Aged Care. Sydney: The American Geriatrics Society, 2011.
46. YU EW. Proton pomp inhibitors and risk of fractures: a meta-analysis of 11 international studies. Boston: NIH, 2011.
47. BISCHOFF-FERRARI BH. Fracture prevention with vitamin D supplementation. Journal American Medical Association(JAMA), 2005.
48. MINISTRY OF HEALTH AND CANCER SOCIETY OF NEW ZEALAND. Vitamin D. New Zealand: Clinical Pharmacist, 2013.
49. KLOPOTOWSKA JE, KUIPER R. On-ward participation of a hospital pharmacist in a Dutch intensive care unit reduces prescribing errors and related patient harm : an intervention study.. Amsterdam: Biomed Central, 2010.
51. Benzodiazepinen, schema afbouw. Medpsy. [Online] juni 13, 2013. [Cited: februari 10, 2017.] https://medpsy.wordpress.com/2013/06/13/benzodiazepinen-schema-afbouw/.
52. Ontwenningschema en omrekentabel. Novadic Kentron/Nieuwe Kansen. [Online] Leonard B2B Communicatie, 2016. [Cited: 02 10, 2017.] https://www.novadic-kentron.nl/verwijzers-en-professionals/kennisbank-verwijzers/benzodiazepines/ontwenningsschema-en-omrekentabel/.
53. PEREHUDOFF K. Medication discrepancies in older patients admitted to non-geriatric wards : An exploratory study. Gent: Elsevier, 2014.
54. DUERDEN M, AVERY T, PAYNE R. Polypharmacy and medicines optimization. London: The King's fund, 2013.
55. BROE KE. A higher dose of vitamin D reduces the risk of falls in nursing home residents : a randomized, multiple-dose study. Boston: The American Geriatrics Society, 2007.
54 | REFERENCES
56. WAUTERS M, ELSEVIERS M. Too many, too few, or too unsafe? Impact of inappropriate prescribing on mortality, and hospitalization in a cohort of community dwelling oldest old.. 82, Gent: British journal of clinical pharmacology, 2016.
57. DALLEUR O, BOLAND B. Detection of potentially inappropriate prescribing in the very old: cross-sectional analysis of the data from the BELFRAIL observational cohort study.. Leuven : Biomed Central, 2015.
58. VAN STRIEN A, VAN MARUM RJ. Psychotropic medications, including short acting benzodiazepines, strongly increase the frequency of falls in elderly. Utrecht: Elsevier, 2013.
59. DIAZE-GUTIERREZ J. Relationship between the use of benzodiazepines and falls in older adults : A systematic review. Monica. Spain: Elsevier, 2017.
60.RAY WA, PURUSHOTTAM BT. Benzodiazepines and the risk of falls in nursing home residents. Tennessee : American Geriatrics Society, 2000.
61. BEIJER HJM, BLAEY CJ. Hospitalisations caused by adverse drug reactions (ADR): a meta-analysis of observational studies. Pharmacy World & Science, 2002.
62. TJAVAD. Benzodiazepine prescription for patients in treatment for drug use disorders: nationwide cohort study in Denmark. Denmark: BMC Psychiatry, 2016.
63. POTTER K, FLICKER L, PAGE A. Deprescribing in frail older people : A Randomized Controlled Trial. Glasgow : Plos One, 2016.
64. TOMMELEIN E, MEHUYS E, PETROVIC M. Potentially inappropriate prescribing in community-dwelling older people across Europe: a systematic literature review. et. Gent: European Journal Clin. Pharmacol., 2015.
65. GALLAGHER P, LANG PO. Prevalence of potentially inappropriate prescribing in acutely ill population of older patients admitted to six European hospitals. Ireland : European J. Clinical Pharmacology, 2011.
66. REEVE E. People's attitudes, beliefs, and experiences regarding polypharmacy and willingness to deprescribe.. Queensland: The American Geriatrics Society, 2013.
67.WILLIAMS The Short-Term Effect of Interdisciplinary Medication Review on function and cost in Ambulatory Elderly People. Virginia: The American Geriatrics Society, 2004.
68. GARFINKEL D. Feasibility study of a systematic approach for discontinuation of multiple medications in older adults: American Medical Association, 2010.
69. INCB ( INTERNATIONAL NARCOTICS CONTROL BOARD). Psychotropic Substances. New York: United Nations, 2016.
70. MILLER NS. Management of Withdrawal Syndromes and Relapse Prevention in Drug and Alcohol Dependence. Chicago: Am Fam Physician, 1998.
71. KOSTEN T, O'CONNOR PG. Management of drug and alcohol withdrawal. Yale: The new England journal of medicine, 2003.
72. TITECA. Zorgpad Alcohol AZ Groeninge. Kortrijk.
73. CHRISTIAENS T. Gecommentarieerd Geneesmiddelenrepertorium. [Online]. www.bcfi.be.
74. BCFI. SKP van Circadin®. 2015.
55 | REFERENCES
75. REEVE E. Review of deprescribing processes and development of an evidence-base, patient-centered deprescribing process. Australia: British Journal of Clinical Pharmacology, 2014.
76. GUJRAL G, WINCKEL K, NISSEN LM. Impact of community pharmacist intervention discussing patients beliefs to improve medication adherence. Australia, 2013.
77. BALDWIN C, GRIFFITH KA, NIETO FJ. The association of sleep-disordered breathing and sleep symptoms with quality of life in the sleep hearth health study. Arizona: Sleep, 2000.
78. LIU LM. Deprescribing : an approach to reducing polypharmacy in nursing home residents: The journal of nurse practioners, 2014.
79. SCOTT IA, GRAY LC, MARTIN JH. Deciding when to stop: towards evidence-based deprescribing of drugs in older populations. Australia: Evidence Based Medicine, 2012.
80. KOPER D, KAMENSKI G, FLAMM M. Frequency of medication errors in primary care patients with polypharmacy. Austria: Family practice, 2013.
81. REICH O. Potentially Inappropriate Medication Use in older Patients in Swiss Managed Care Plans : prevalence, determinants and association with hospitalization. Switzerland: PLOS ONE, 2014.
82. WAUTERS M. Too many, too few, or too unsafe? Impact of inappropriate prescribing on
mortality, and hospitalization in a cohort of community-dwelling oldest old. Gent: British Journal of




































































![Chronic dizziness in older people 6.pdf · Dames en heren, Bijna 10% van de ouderen bezoekt minimaal 1 keer per jaar de huisarts vanwege duizeligheid [1]. De diagnostiek van duizeligheid](https://static.documents.pub/doc/80x56/5ec1d31710202250766a1a01/chronic-dizziness-in-older-people-6pdf-dames-en-heren-bijna-10-van-de-ouderen.jpg)















