35
Jugdeep Dhesi & Jason Cross Dept of Ageing and Health Guy’s and St Thomas’ , London

Jugdeep Dhesi & Jason Cross Dept of Ageing and Health
Guy’s and St Thomas’ , London
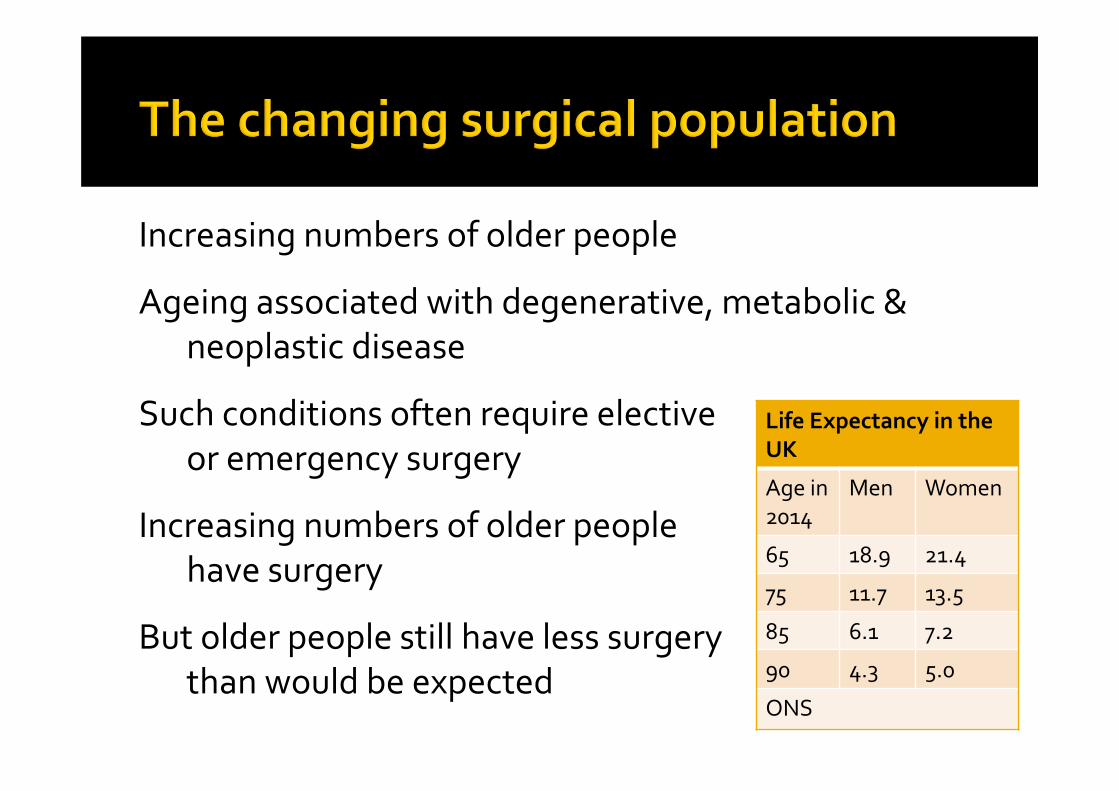
Life Expectancy in the UK
Age in 2014
Men Women
65 18.9 21.4
75 11.7 13.5
85 6.1 7.2
90 4.3 5.0
ONS
Increasing numbers of older people
Ageing associated with degenerative, metabolic & neoplastic disease
Such conditions often require elective or emergency surgery
Increasing numbers of older people have surgery
But older people still have less surgery than would be expected
Clinician reported outcomes Morbidity Mortality
Patient reported outcomes Recovery (change in trajectory of disease/disability) Experience, satisfaction
Process related outcomes Harm and complaints LOS, readmissions Cost (in‐hospital, rehab, formal and informal )

Assess risk factors
Not ‘fit’ for surgery’
V
Fit for surgery
Admit to SAL/Sx wardSurgical ward
Discharge to community HDU/ITU

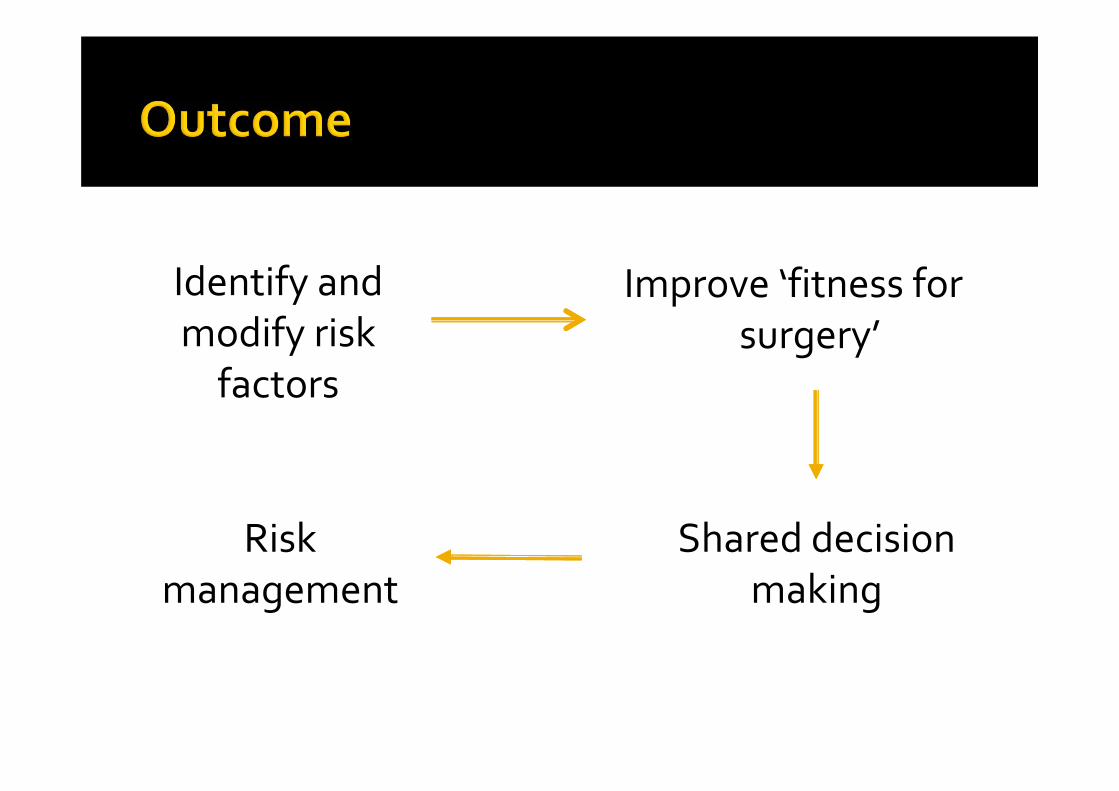
Identify and modify risk factors
Improve ‘fitness for surgery’
Shared decision making
Risk management

Identify risk factors
Modify risk factors
Make patient fitter
Less complications, managed better
Improve outcomes

Clinical pathway
Skeletal muscle
conditioning Cardiopul fitness
Frailty
Anaemia
Manage comorbidity
Nutrition

Medical complications Rehabilitation Discharge Follow up

74 yrs old FLiving aloneNo support‘Difficult’ historian
OsteoarthritisDiabetesHypertensionSOB ?cause
Anaemia
No surgeryHbA1c 8.2%BP 170/88ECG NADCXR NADHb 100g/l
Elective colorectal cancer (orthopaedic/vascular/gynae/any) surgery

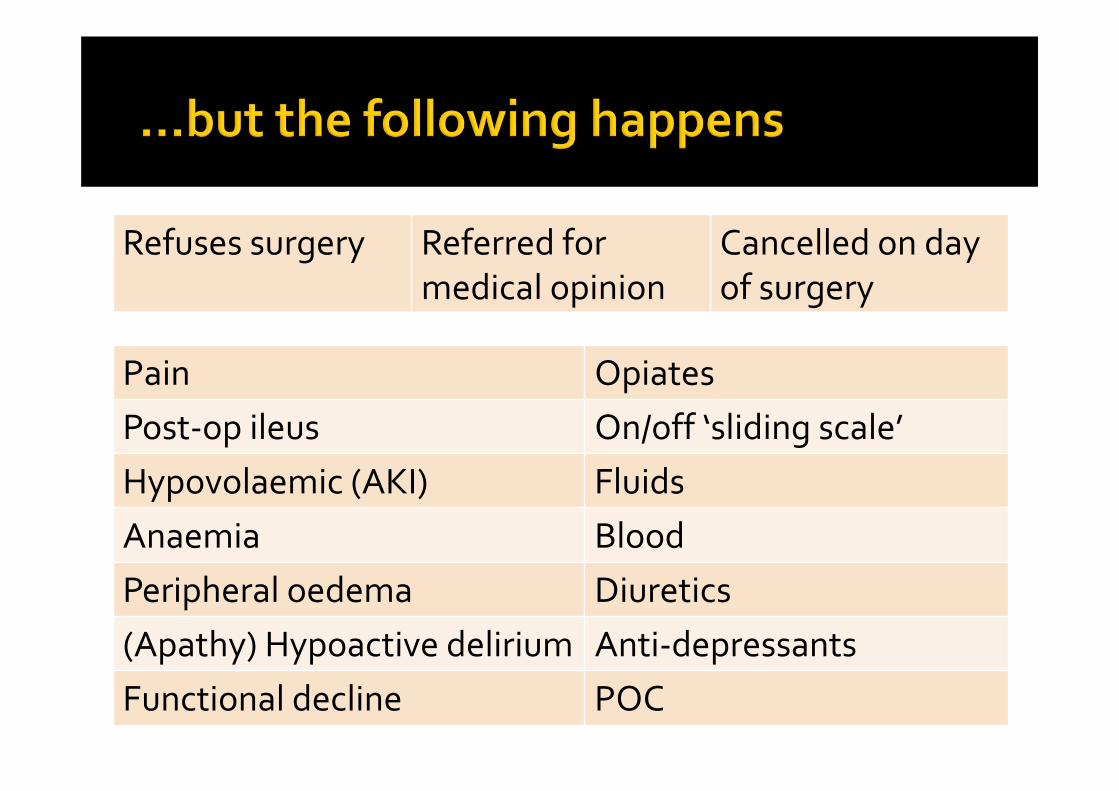
Pain Opiates Post‐op ileus On/off ‘sliding scale’Hypovolaemic (AKI) FluidsAnaemia BloodPeripheral oedema Diuretics(Apathy) Hypoactive delirium Anti‐depressantsFunctional decline POC
Refuses surgery Referred for medical opinion
Cancelled on day of surgery

• 4 in 5 high risk patients to general ward
• Management on wards by junior staff
• Poor recognition of medical problems
• Reliance on on‐call staff
• Multiple medical team involvement

Knowledge Assessment, optimisation, post‐op medical care, rehabilitation, discharge planning
Behaviours Reactive approach Unstandardised and uncoordinated medical management
Attitudes Cultural, traditional, silos of care
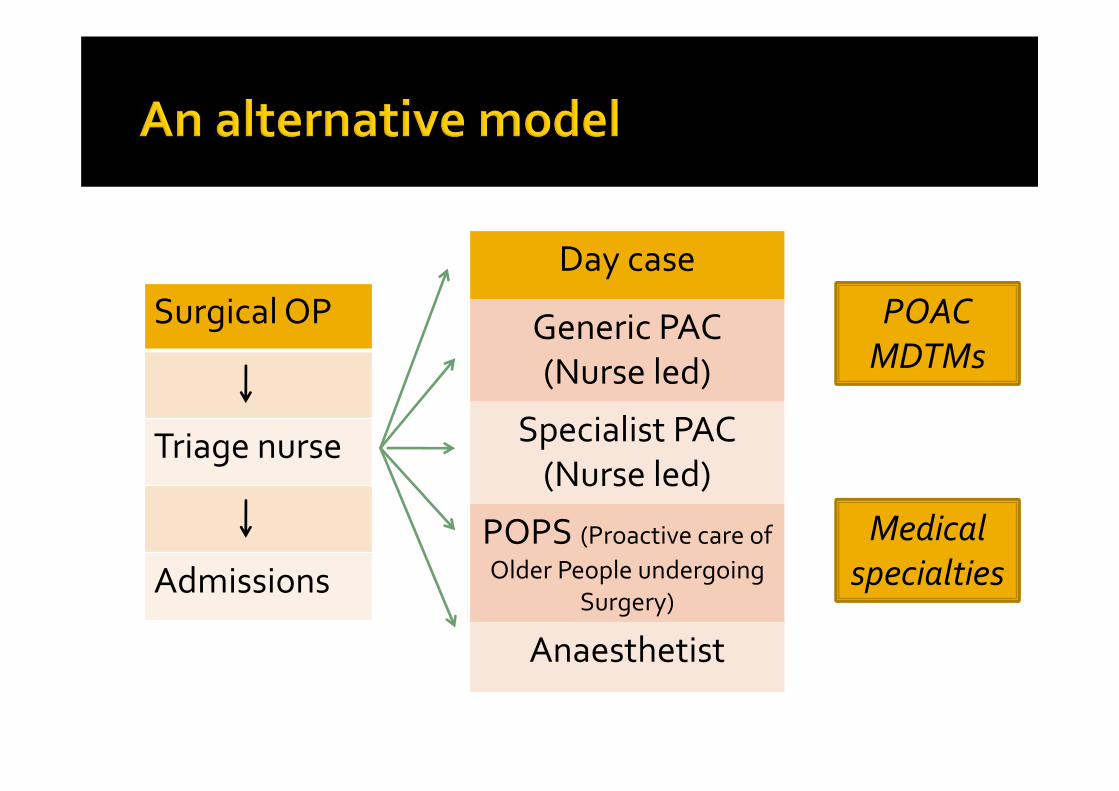
Medical specialties
Day case
Generic PAC (Nurse led)
Specialist PAC (Nurse led)
POPS (Proactive care of Older People undergoing
Surgery)
Anaesthetist
Surgical OP
Triage nurse
Admissions
POAC MDTMs

Surgical OP/PACReferrals• Screening criteria• ‘Medically unfit’ • Support required for decision making
Pre‐op CGAConsultantCNSOTSocial worker
Hospital AdmissionWard roundsMDMsCase conferencesEducation and training
Post DischargeIntermediate CarePrimary careSocial careSpecialist clinics
LiaisonPatientSurgical teamAnaesthetistsGPCommunity service
The POPS model

Comprehensive geriatric assessment (CGA)
Holistic, multidimensional, interdisciplinary assessment of an individual
Formulation of a list of needs and issues to tackle an individualised care and support plan tailored to an individual’s needs, wants and priorities
Risk assessment Recognition of known comorbidity Identification of unrecognised disease, disability, frailty Assessment of functional reserve
Optimisation Medical, functional, psychological & social condition Application of organ specific guidelines Use of multidisciplinary interventions

Collaborative decision making Risk/harm versus benefit Consent, capacity, advance directives Communication
Risk management Prediction of post operative complications Planning of postoperative care promoting Early identification of medical complications Standardised mx of medical complications
Prediction of support required on discharge


OADiabetesHTNSOB ?cause‘Difficult’ historian
PainHbA1c 8.2%BP 170/88Ischaemic ECG AnaemiaDeconditioningCog impair’tSocial issues
Treat/physioTreat/planABPM/treatMedical optimisationIv ironExercise programmeDelirium risk/mxEquipment/POCPsychological supportDischarge planning

Admission on day of surgeryDetailed info to anaesthetist
Planned individualised intraoperative care
Proactive standardised mx of ileus, diabetes, fluid balance by joint team
Appropriate discharge plans
POPS Letter

Pre and post studyOrtho elective, Age and Ageing, 2007;36:190‐196
Randomised controlled trial Single centre elective aortic & lower limb
vascular 40% reduction in LOS No increase in readmission Predominantly due to ▪ reduction in medical complications ▪ streamlining of process (reduction in SD of LOS)
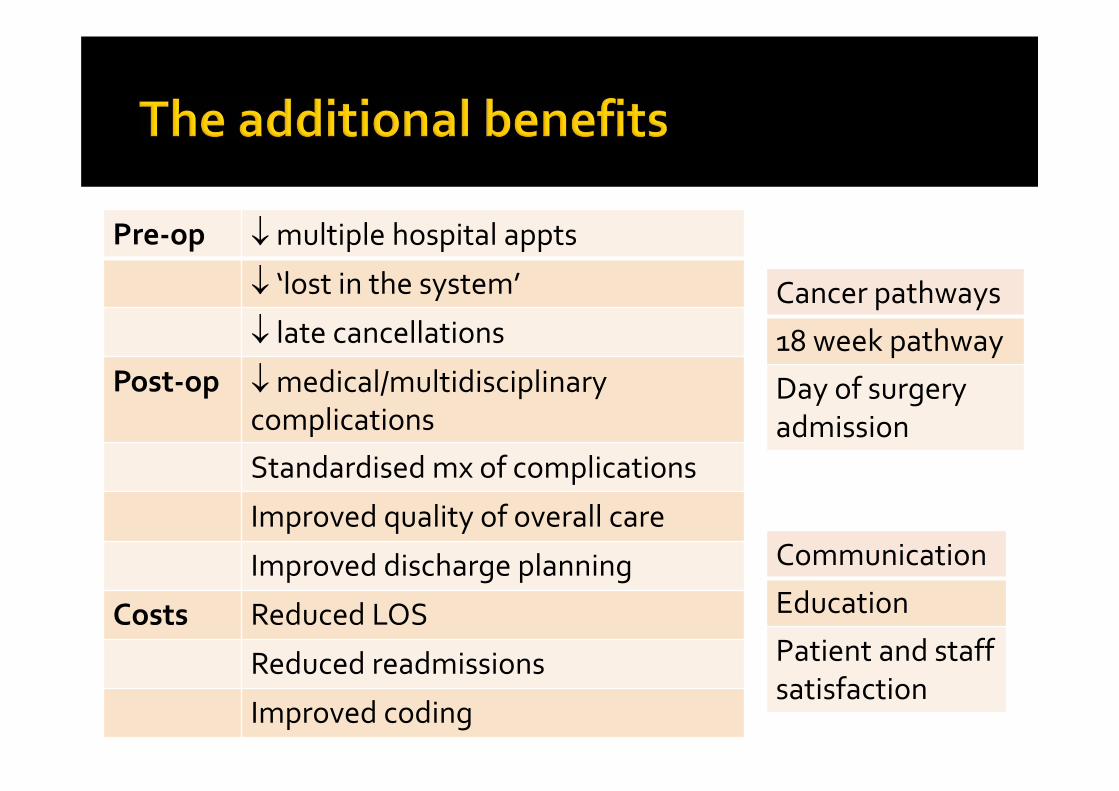
Pre‐op multiple hospital appts
‘lost in the system’
late cancellations
Post‐op medical/multidisciplinary complications
Standardised mx of complications
Improved quality of overall care
Improved discharge planning
Costs Reduced LOS
Reduced readmissions
Improved coding
Cancer pathways
18 week pathway
Day of surgery admission
Communication
Education
Patient and staff satisfaction

Guys St Thomas’
Orthopaedic – electiveUrologyHead and NeckENT
Orthopaedic – traumaUpper GI/Lower GIVascularPlastics
Elective – known to POPS
Elective – not known to POPS
Non‐ElectiveWard based MDTMs
POPS Clinic
Joint surgical ward rounds
CPOAC MDTMs
Amputee Rehab Unit

Jason Cross ANP – POPS team
Putting it into practice – case studies

IHD
PPM
CKD 4
DM
MCI
Falls
Continue aspirin
Arranged / site OK
No contrast confirmed / risk discussed
Pre op plan
Counselled / info given
POPS OT
Stable / BNP 450
Requires check as >6 months
Stable with risk of AKI & dialysis
Referral to specialist / Hba1c >10%
MoCA 21/30 / High Delirium risk
Multi‐factorial / risk of f/decline
Issue Assessment Intervention
77 year old elective / Fem distal bypass for PVD Direct referral from consultant

High surgical risk
Morbidity 97%Mortality 56%
Patient symptomatic
Requiresintervention
Patient concern over risk
Unsure of options
Risk discussed with surgery / POPS presence
Less invasive procedure
Angioplasty and stent
Good symptomatic relief
CommunicationVerbal
EmailClinic letter
Identify and modify risk factors
Improve ‘fitness for surgery’
Shared decision making
Risk management

Multimorbidty
Abdominal pain
No surgical issues / requesting transfer to
elderly care
Nurses report patient has care needs / daughter
struggling
Proactive case finding with expedited assessment
89 year old lady / on admissions ward

Constipation
Frail with f/decline
Social care
Laxatives prescribed / advice
OT referral and assessment
Discussed / advice / community ref
Faecal loading on imaging
Risk of falls / increased care
Living with daughter / requesting care input
Issue Assessment Intervention
Patient home after bowels
opened
Proactive case funding with
holistic assessment
Admission avoidance with appropriate community referral
76 year old gentleman Incarcerated hernia Requires emergency surgery Discussed at EGS handover meeting Concerns raised Nursing home resident Patient confused ‘has dementia’ Would palliative care be more appropriate

AF
Warfarin
Anaemia
Immobility
High Surgical risk
Confusion
Consent
Plan detailed / IV Digoxin
Discussed / Vitamin K
Haematinics obtained
Air mattress
Discussion
Delirium pathway / advice
• Best interest discussion• Family involved • Documentation• Consent form 4 • Proceeds to surgery
Rate controlled
INR high (2.4)
Hb 11 / stable for surgery
High risk PA breakdown
Morbidity 81%, Mortality 14%
Delirium NOT dementiaMild cognitive impairment
• Lacks capacity (delirium)• Collateral history • Good QOL• Living independently
Issue Assessment Intervention

Ileus
AF
AKI
Delirium
Functional decline
Dietetic reviewTPN
IV Digoxin / advice / pathway
Fluid resus / AKI pathway
Haloperidol (not used) / pathway
Early therapy Rehab referral
Albumin droppingNBM prolonged
Fast rate
Baseline 3a 20% cr rise
Acute / multi‐factorial
Global weaknessDeconditioned
Issue Assessment Intervention
Delirium resolves at day 5
14 day hospital stay
Early therapy referral to rehab
unity
4 week stay at rehab then home

Surgical OP/PACReferrals• Screening criteria• ‘Medically unfit’ • Support required for decision making
Pre‐op CGAConsultantCNSOTSocial worker
Hospital AdmissionWard roundsMDMsCase conferencesEducation and training
Post DischargeIntermediate CarePrimary careSocial careSpecialist clinics
LiaisonPatientSurgical teamAnaesthetistsGPCommunity service
The POPS model


















