50
Dermatology for the Primary Care Physician Sandy Baumberger, MD Assistant Professor Dept. of Family Medicine
| Date post: | 03-Jun-2018 |
| Category: |
Documents |
| Upload: | benny-pojer |
| View: | 223 times |
| Download: | 0 times |
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 1/50
Dermatology for the Primary CarePhysician
Sandy Baumberger, MD Assistant Professor
Dept. of Family
Medicine
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 2/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 3/50
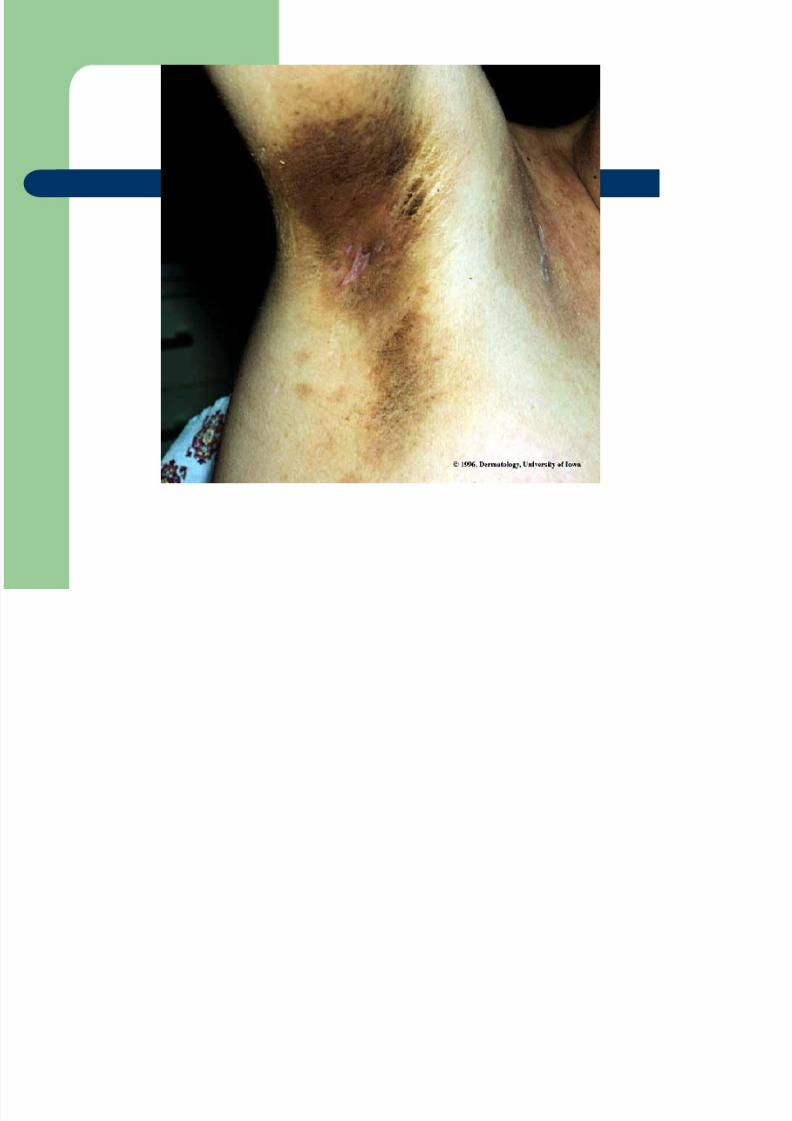
Acanthosis Nigricans
Diffuse velvety thickening & hyperpigmentation ofthe skin. Most often the axilla, other body folds
May be associated with factors of heredity, obesity,endocrine disorders (metabolic syndrome), drugadministration (Nicotinic acid), and malignancy(adenocarcinoma, lymphoma)
May be caused by hypersecretion of pituitary peptide
or non-specific growth-promoting effect ofhyperinsulinemia
No specific treatment. May resolve with resolution ofcausative agent (drug) or weight loss

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 4/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 5/50
Allergic Contact Dermatitis
Acute, subacute, or chronic inflammation of theepidermis and dermis caused by external agents,
toxicity, or an allergic reaction characterized bypruritis or burning of the skin
Caused by a type IV hypersensitivity reaction causedby sensitized lymphocytes (T cells) after contact withan antigen. Tissue damage occurs from cytotoxicityby T cells and release of lymphokines
Treatment involves removing the offending agent,corticosteroid creams, and oral prednisone forreactions over large body surfaces

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 6/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 7/50
Atopic Dermatitis
Acute, subacute, usually chronic pruritic inflammation of theepidermis and dermis occurring in association of personal orfamily history of hay fever, asthma, rhinitis, or Atopic dermatitis
Type I (IgE mediated) hypersensitivity reaction occurring as aresult of the release of mast cells and basophils that have beensensitized by the interaction of the antigen with IgE.Colonization of Staph aureus of nares and/or involved skin isoften seen
Emotional stress worsens. Treatment with antihistamines to
decrease scratching and secondary infection. Topicalcorticosteroids are the mainstay of treatment. Occasionalsystemic steroids may be needed. Avoid superinfection withHSV and/or Staph aureus-treat if infection noted

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 8/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 9/50
Basal Cell Carcinoma
Most common type of skin cancer. Rarely metastasizes butmay invade deeply (especially in the “danger zones” near eyes,nasolabial folds, ear canal, and in posterior auricular sulcus.
Caused by sun exposure and or other radiation exposure Lesions appear as papule or nodule. May appear “pearly” with
a rolled edge. Fine telangiectasia may be seen. Variablecolors
Dermatopathology shows proliferating atypical basal cells(deep blue staining on H&E but with little anaplasia and
infrequent mitoses) Treatment involves excision with primary closure, skin flaps, or
grafts. Lesions in the danger zone should be removed viaMohs surgery. Radiation may be used in cases where severedisfigurement may occur with surgery

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 10/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 11/50
Candidiasis
Superficial mycotic infection occurring on moist cutaneous sitesand mucosal surfaces. Patients may have altered immunityfrom moisture at site of infection, diabetes, antibiotic therapy, oralteration in systemic immunity.
Microscopic sampling of skin or mucosal scraping shows C.albicans
Many sites potentially infected: mucosa, vulvovaginitis, diapercandidiasis, intertriginous, follicular, and chronic cutaneous
candidiasis Treatment involves topical or systemic treatment with antifungal
creams/tablets. Prevention includes procedures to avoidconstant skin contact with moisture
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 12/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 13/50
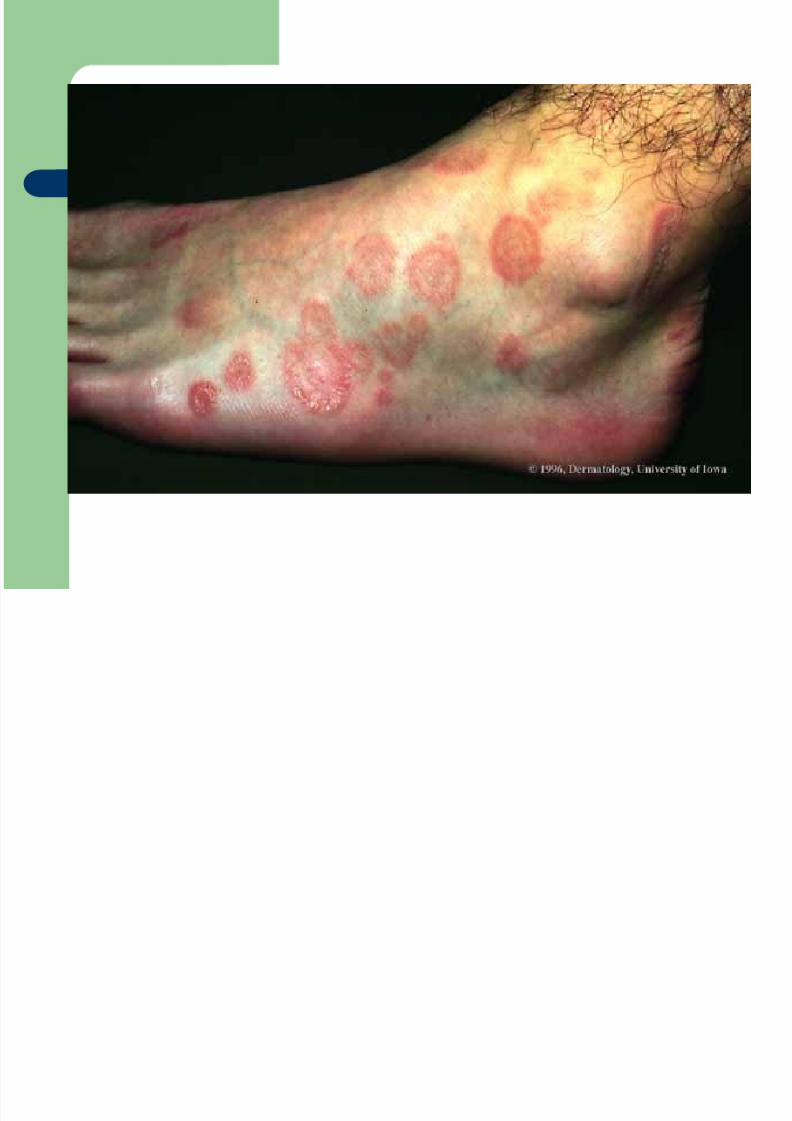
Erythema Multiforme
Reaction pattern of blood vessels in the dermis with secondaryepidermal changes with characteristic erythematous iris-shapedpapules and vesicobullous lesions. Typically involves withpalms, soles, and mucous membranes. May be pruritic orpainful
Dermatopathology shows inflammation characterized byperivascular mononuclear infiltrate, edema of upper dermis,and eosinophilic necrosis of keratinocytes if bulla formation
Treatment is symptomatic. If severely ill, doses of prednisone(50-80 mg/day). Control of Herpes Simplex outbreaks usingoral Acyclovir may prevent development of recurrent erythemamultiforme

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 14/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 15/50
Granuloma Annulare
Self-limited chronic inflammation of the dermis that
exhibits papules in an annular arrangement
Dermatopathology shows foci of chronic
inflammatory and histiocytic infiltrations in the
superficial and mid-dermis surrounded by a wall of
palisading histiocytes and multinuclear giant cells
Treatment with intralesional triamcinolone acetonide3.0 mg/ml or topical corticosteroids with occlusion
may be useful. May recur.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 16/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 17/50
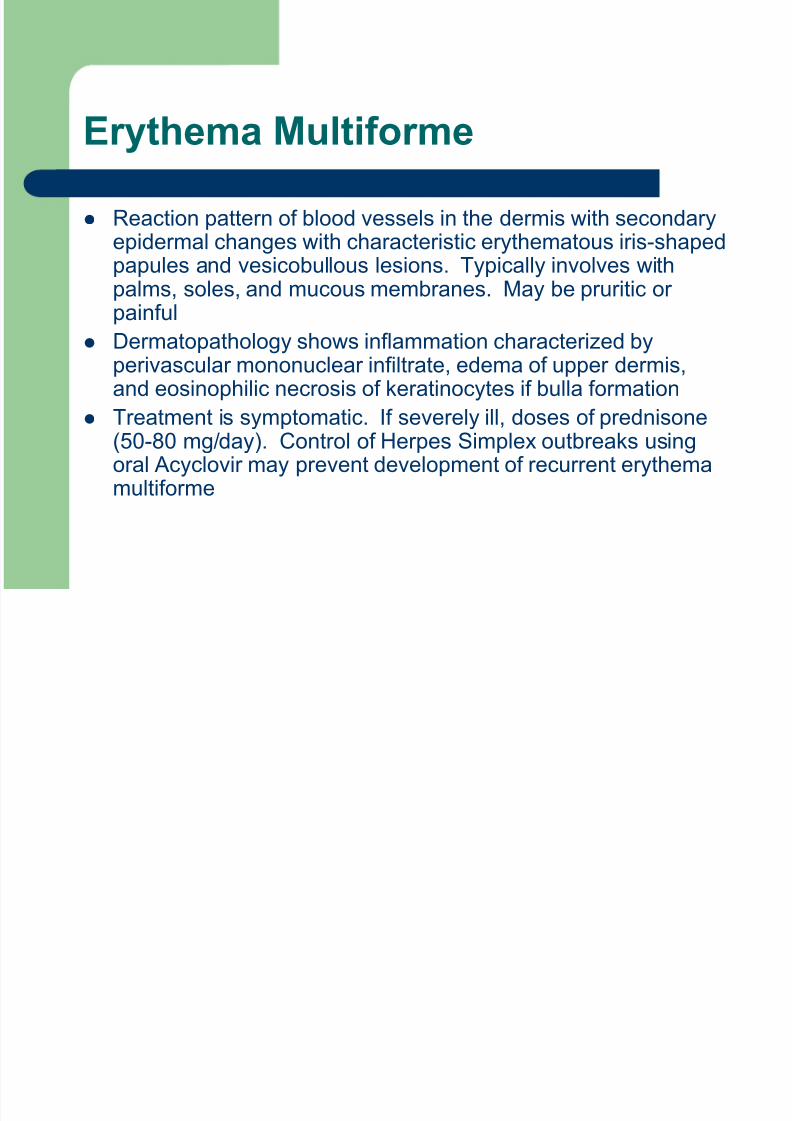
Herpes Simplex
Cutaneous infection caused by HSV 1 and 2 virus types. Type1 usually occurs above the waist/Type 2 below the waist.Lesions to mucous membranes are first umbilicated and thenevolve into punched-out lesions. Secondary infections withStaph aureus are common.
Wright’s stain of vesicular fluid shows multinucleated giantcells. Skin infection positive for HSV and may grow Staph.
Treatment with acyclovir 200 mg 5x daily for 5-10 days. Treat
staph infections with sensitive antibiotics. People with atopic dermatitis are at high risk, also people with
burns, and decreased immune states are at high risk.

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 18/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 19/50
Herpes Zoster
Acute localized infection caused by varicella-zoster virus (VZV)and is characterized by unilateral pain and vesicular or bullouseruption limited to a dermatome innervated by a corresponding
sensor ganglion. During the varicella virus, VZV travels to the sensory ganglion
and establishes latent infection. When humoral and cellularimmunity ebbs, viral replication occurs. The virus then travelsdown the sensory nerve causing pain first, then skin lesionsoccur.
Treatment with high dose Acyclovir (800 mg 5x daily for 10days) hastens healing of acute lesion. The risk of postherpeticneuralgia in patients over 60 years old is >50%. Disseminationmay occur, and motor paralysis may occur if the virus involvesthe cranial nerves.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 20/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 21/50
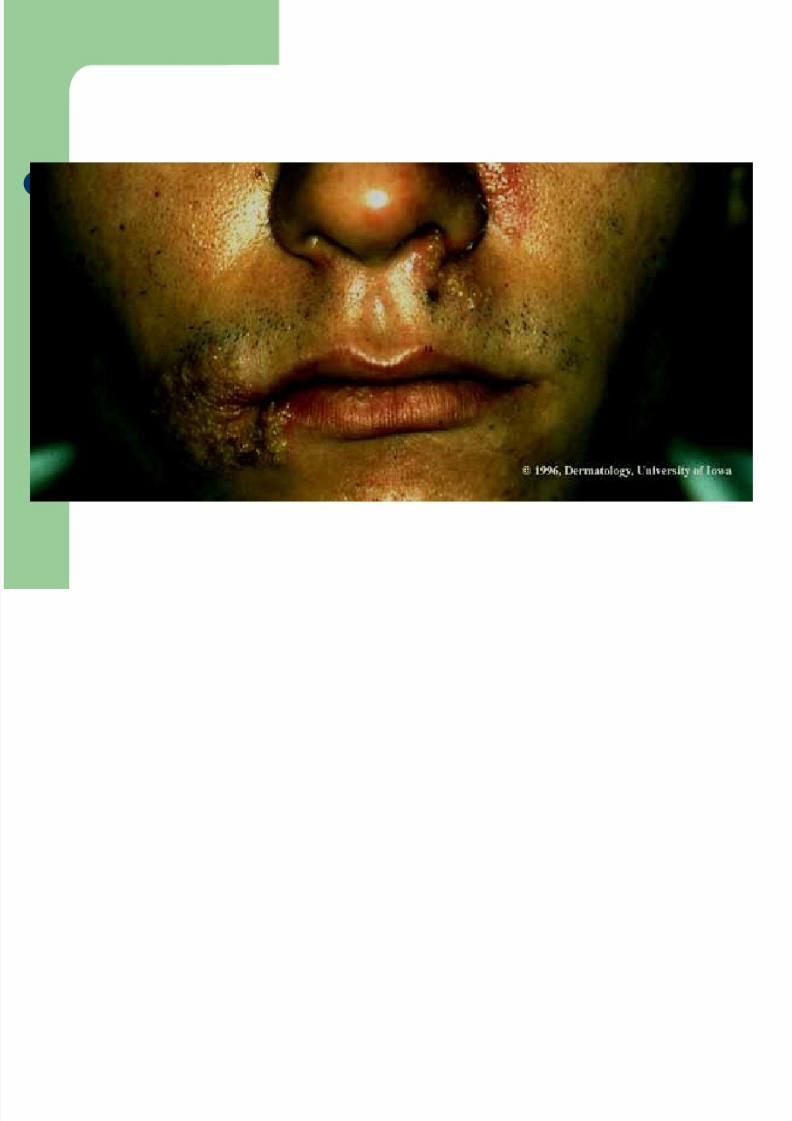
Impetigo
An acute purulent infection which is at first vesicular and
later crusted-a very superficial infection of the epidermis
affecting mostly young children and young adults. Very contagious
Most often due to Staph aureus or group A B-hemolytic
streptococci
Treatment: wash crusts off - topical mupirocin 2%ointment. Systemic antibiotic therapy may be necessary
with sensitive antibiotics if extensive lesions are present.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 22/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 23/50
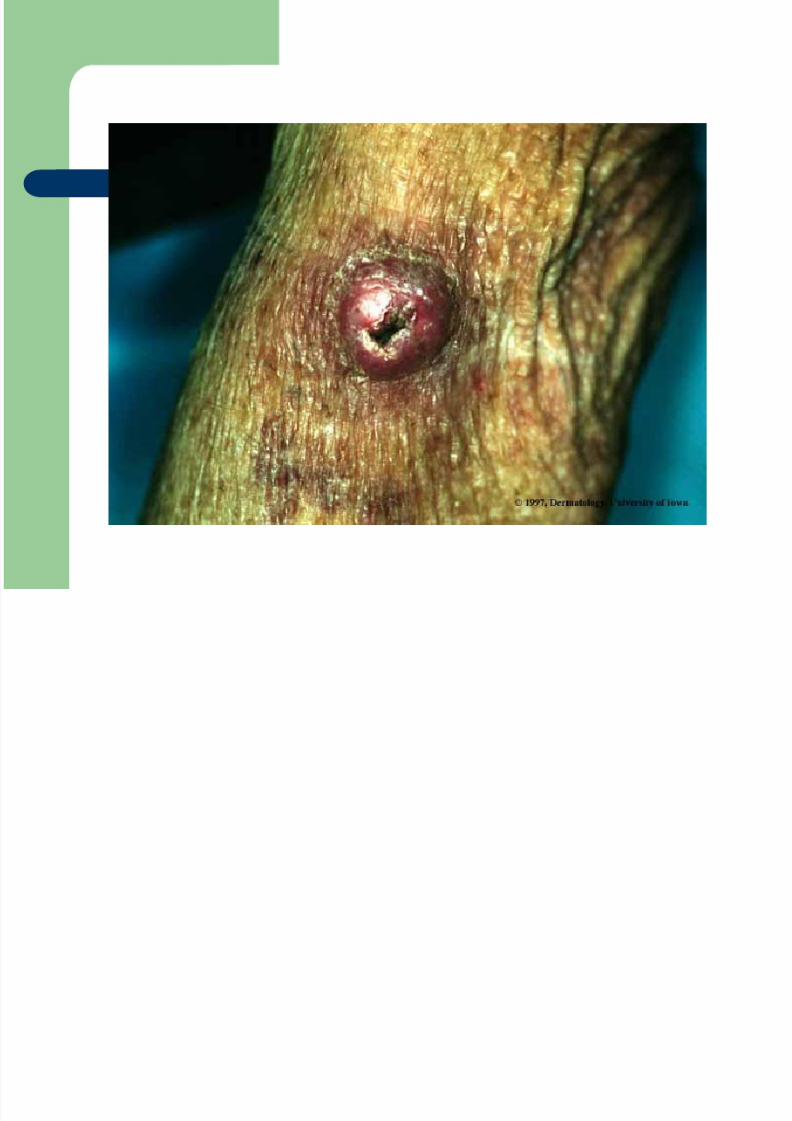
Keratocanthoma
Self-healing, rapidly developing epithelial neoplasmthat mimics squamous cell carcinoma. May grow to
2.5 cm diameter in six weeks. HPV has been identified in some lesions. Other
etiologic factors include ultraviolet radiation andchemical carcinogens (industrial).
Spontaneous regression in 2-6 months, sometimes 1year. No specific treatment. May result indisfiguring scar. May need to biopsy-as lesion canmimic squamous cell carcinoma.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 24/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 25/50
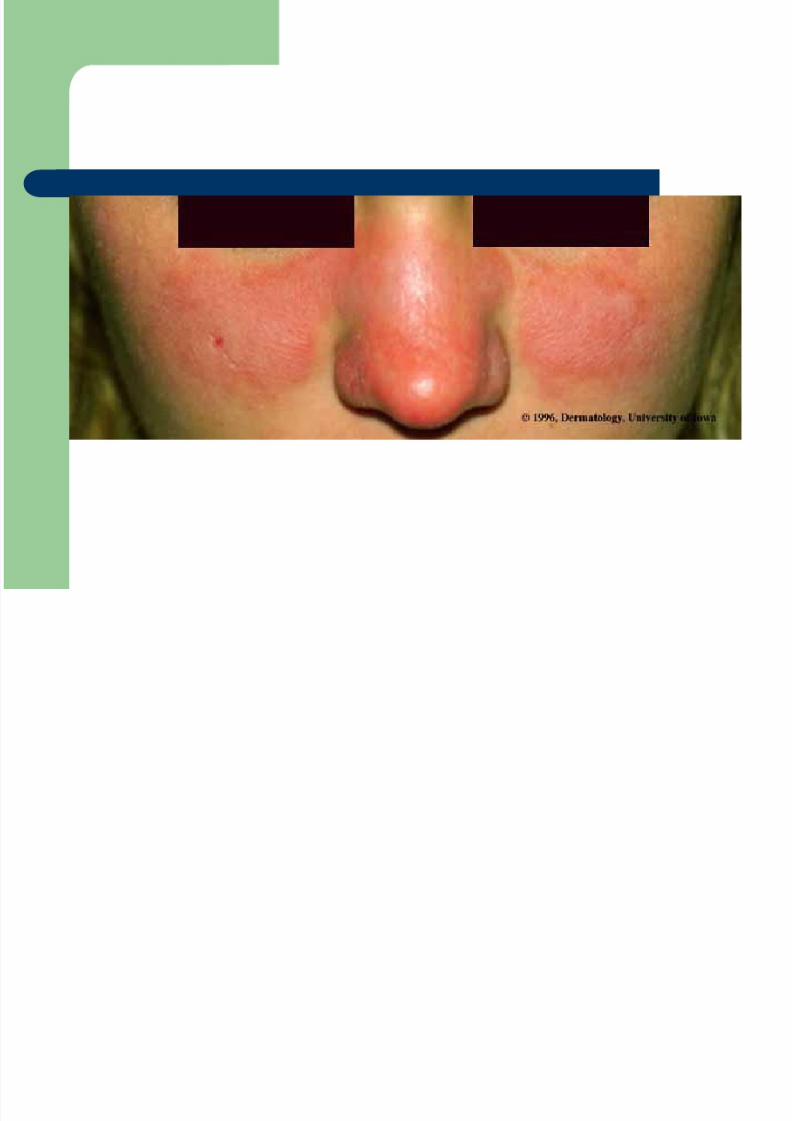
Systemic Lupus Erythematosus
Serious multisystem disease involves connective tissue andblood vessels. Clinical manifestations include fever, skinlesions, arthritis, renal, cardiac, and pulmonary disease.
Lesions may appear in “butterfly” pattern to face. Well-demarcated regions.
Dermatopathology shows atrophy of epidermis, dermalinflammatory infiltrate with lymphocytes, and fibrinoiddegeneration of the connective tissue and walls of the bloodvessels.
Treatment involves rest, avoidance of sun exposure.Prednisone is used for treatment of systemic symptoms.Chloroquine sulfate or other antimalarials are sometimes usefulin the treatment of skin lesions, but do not reduce the need forprednisone
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 26/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 27/50
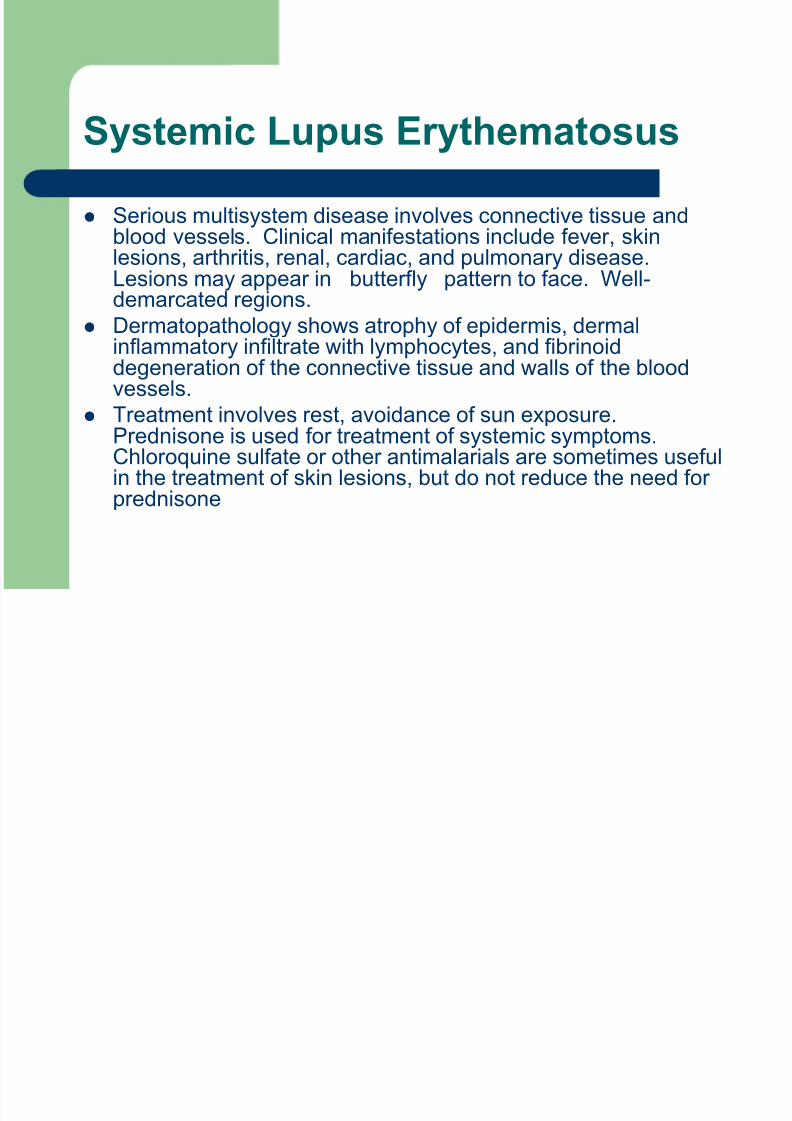
Malignant Melanoma (nodular type)
One type of primary melanoma that arises quite rapidly (4 mosto 2 years) from normal skin or a melanotic nevus. 15-30% ofmelanoma in the US. Family history, light skin color, excessive
sun exposure, history of melanocytic nevus important. Appear on upper back in males, lower legs in females, and
other sites. Arises at the dermoepidermal junction and extendslaterally in the dermis. Eventually invades the dermis and thenmay continue to spread. Malignant melanoma is the type ofskin cancer most likely to metastasize.
Excisional or punch biopsy acceptable. Depth of lesion is moreimportant than diameter. Nodal biopsy only needed if >1.7 mmthickness or suspicion of node involvement. Skin grafts may beneeded for large areas

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 28/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 29/50
Molluscum contagiosom
Discrete, umbilicated, pearly-white papulescaused by a poxvirus and occur in both
children and adults that develop over 2-3months. Not symptomatic.
Dermatopathology reveals “molluscumbodies” (inclusion bodies)
Usually spontaneous remission. May usecurettage, liquid nitrogen, or lightelectrocautery
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 30/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 31/50
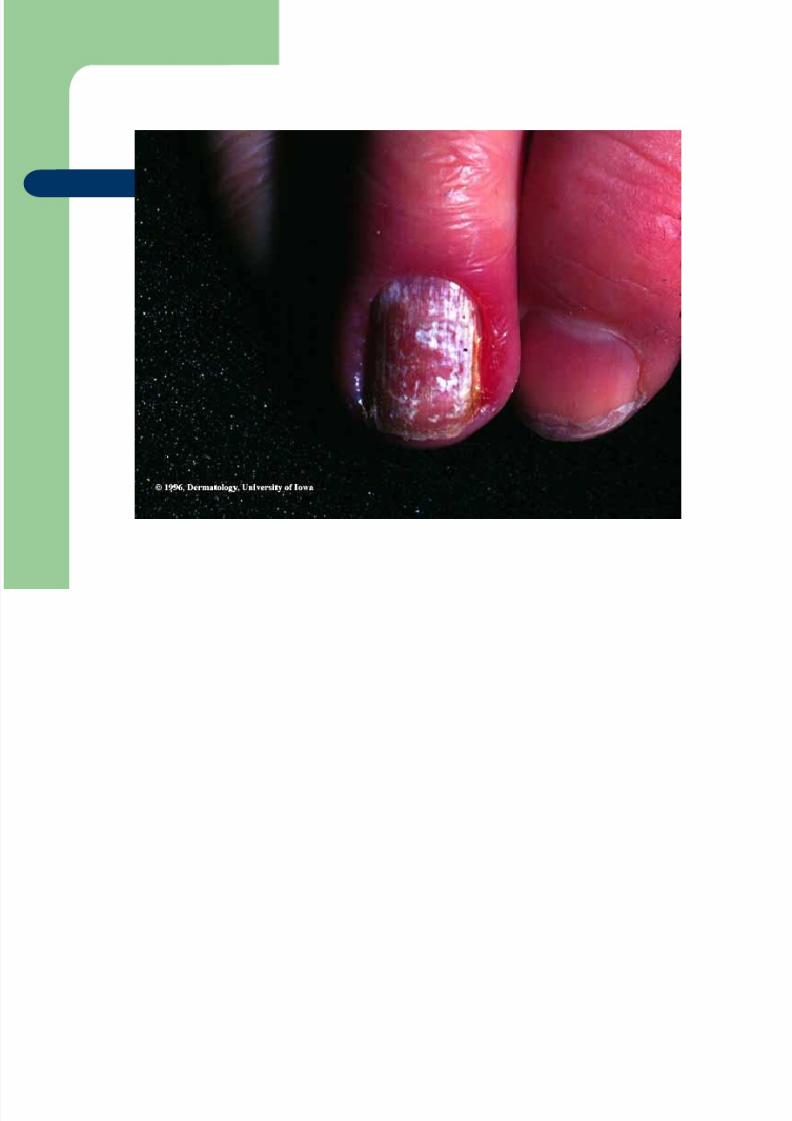
Onychomycosis
Dermatophyte infection of the nail plate. The termonychomycosis includes infections caused by both fungus andyeasts.
May occur due to reduction in blood flow with age or peripheralnerve injury. Mechanical pressure by footwear can also causeinjury and increase susceptibility of nail keratin todermatophytic infections.
Oral antifungals such as Terbinafine 250 mg 1x daily for 6-12
weeks or Sporanox 200mg 2x daily for 1 week and then 3weeks off, then retreat x1 week. Need to watch liver functions.

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 32/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 33/50
Pediculosis Captitis (Head Lice)
Infestation of the scalp by the head louse. It feedson the scalp and neck, and deposits eggs on the
hair. Minimal symptoms. Pediculus humanus capitis-transmitted via shared
caps, brushes, combs, head-to-head contact.
Treatment with Permethrin 1% cream. Apply toscalp after washing hair. Leave on scalp x 10minutes, rinse. Remove nits with fine tooth comb.Repeat after 7 days if living lice still present.Wash/dry-clean clothes/bedding as appropriate.

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 34/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 35/50
Pityriasis Rosea
Exanthematous, maculopapular, red, scalingeruption that occurs mainly on the trunk.
Causes pruritis for some-may be severe. “herald patch” precedes the exanthematous
phase. The exanthem develops over aperiod of 1-2 weeks. Thought to be caused
by an unknown infectious agent.
Regression is usually spontaneous. May useUVB treatments, antihistamines for pruritis.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 36/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 37/50
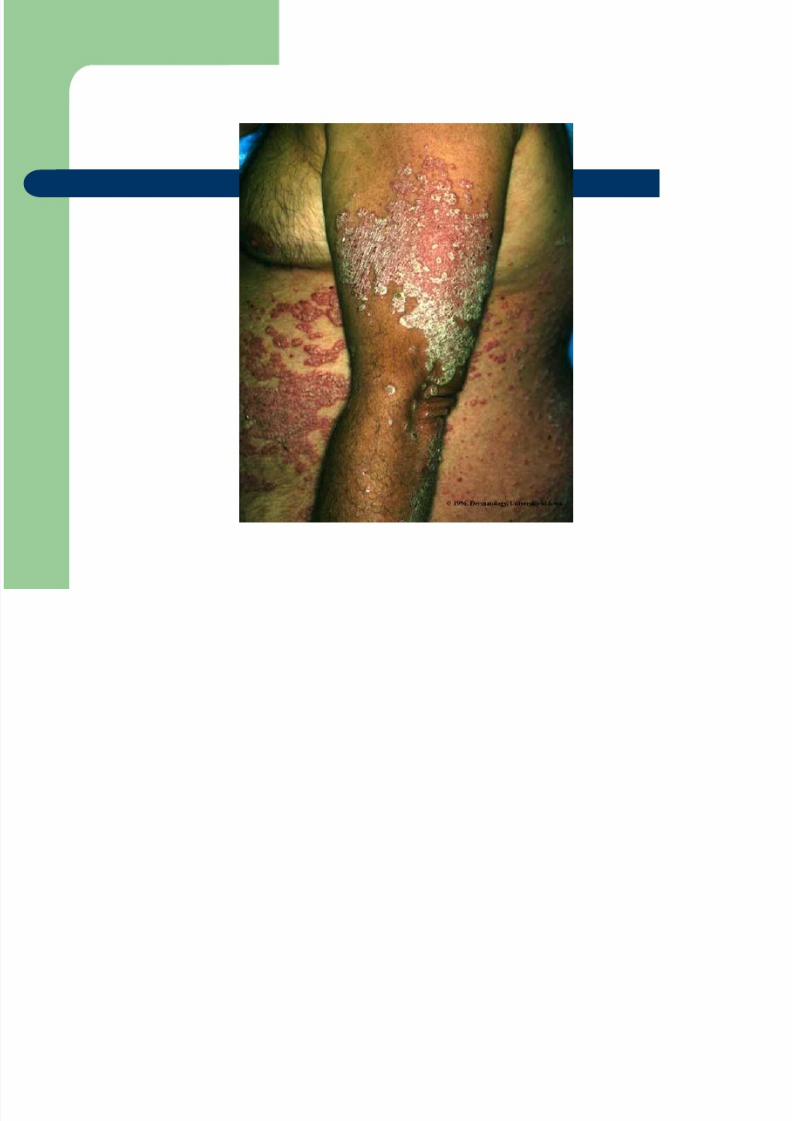
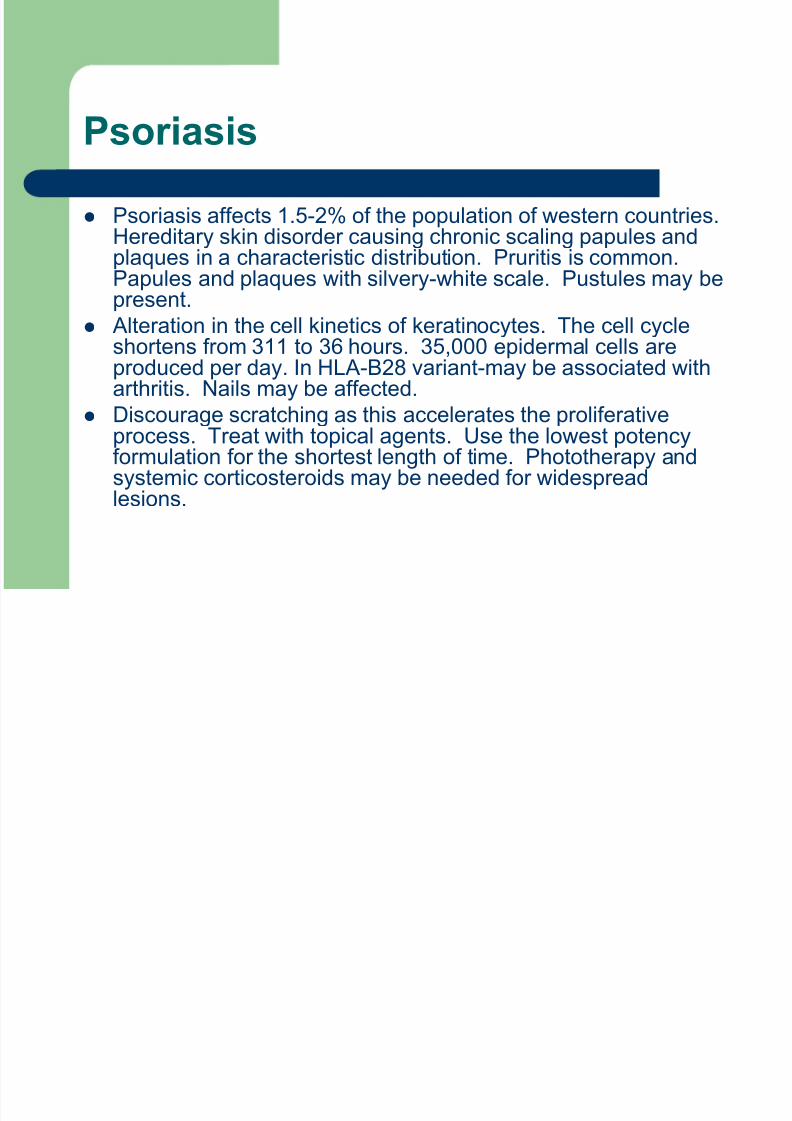
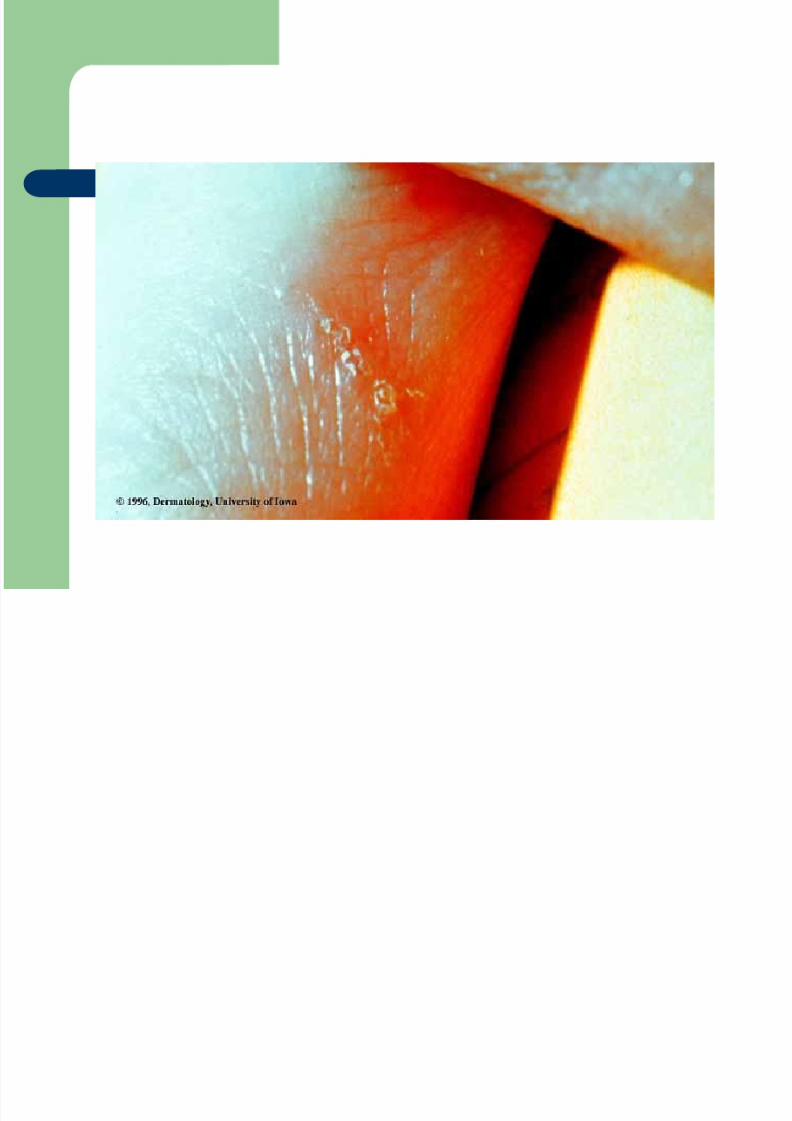
Psoriasis
Psoriasis affects 1.5-2% of the population of western countries.Hereditary skin disorder causing chronic scaling papules andplaques in a characteristic distribution. Pruritis is common.
Papules and plaques with silvery-white scale. Pustules may bepresent.
Alteration in the cell kinetics of keratinocytes. The cell cycleshortens from 311 to 36 hours. 35,000 epidermal cells areproduced per day. In HLA-B28 variant-may be associated witharthritis. Nails may be affected.
Discourage scratching as this accelerates the proliferativeprocess. Treat with topical agents. Use the lowest potencyformulation for the shortest length of time. Phototherapy andsystemic corticosteroids may be needed for widespreadlesions.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 38/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 39/50
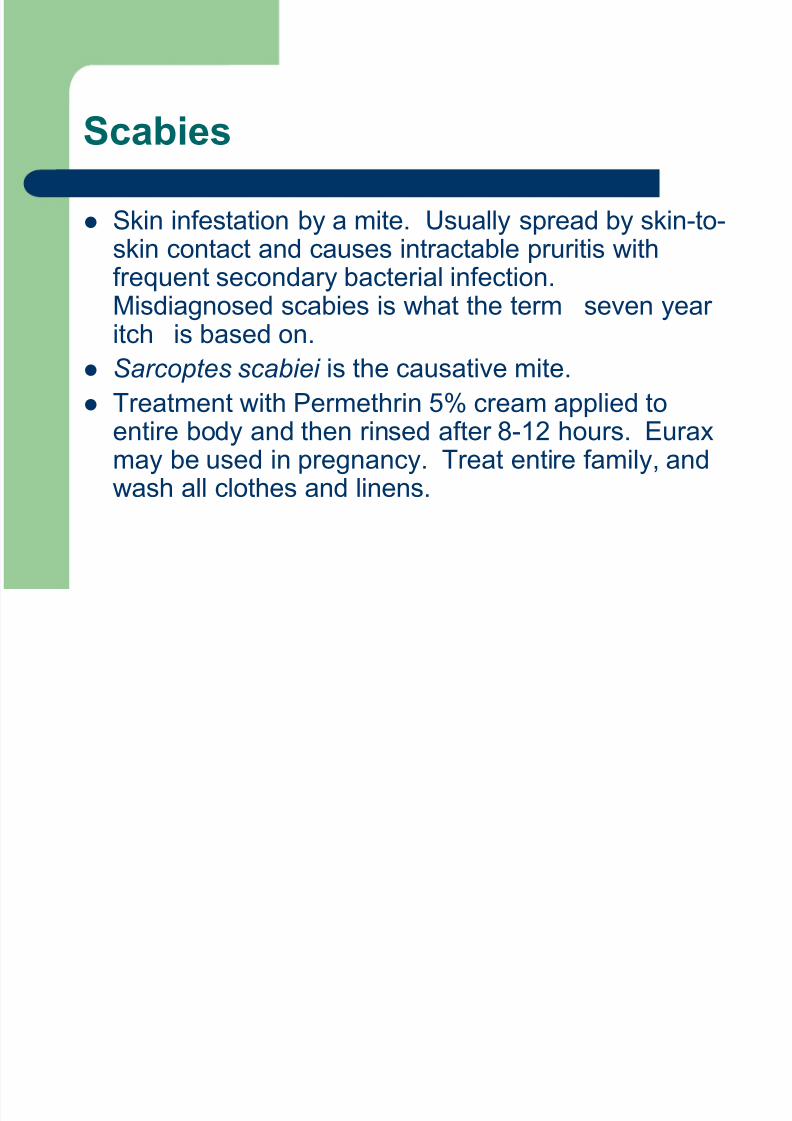
Scabies
Skin infestation by a mite. Usually spread by skin-to-skin contact and causes intractable pruritis with
frequent secondary bacterial infection.Misdiagnosed scabies is what the term “seven yearitch” is based on.
Sarcoptes scabiei is the causative mite.
Treatment with Permethrin 5% cream applied toentire body and then rinsed after 8-12 hours. Euraxmay be used in pregnancy. Treat entire family, andwash all clothes and linens.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 40/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 41/50
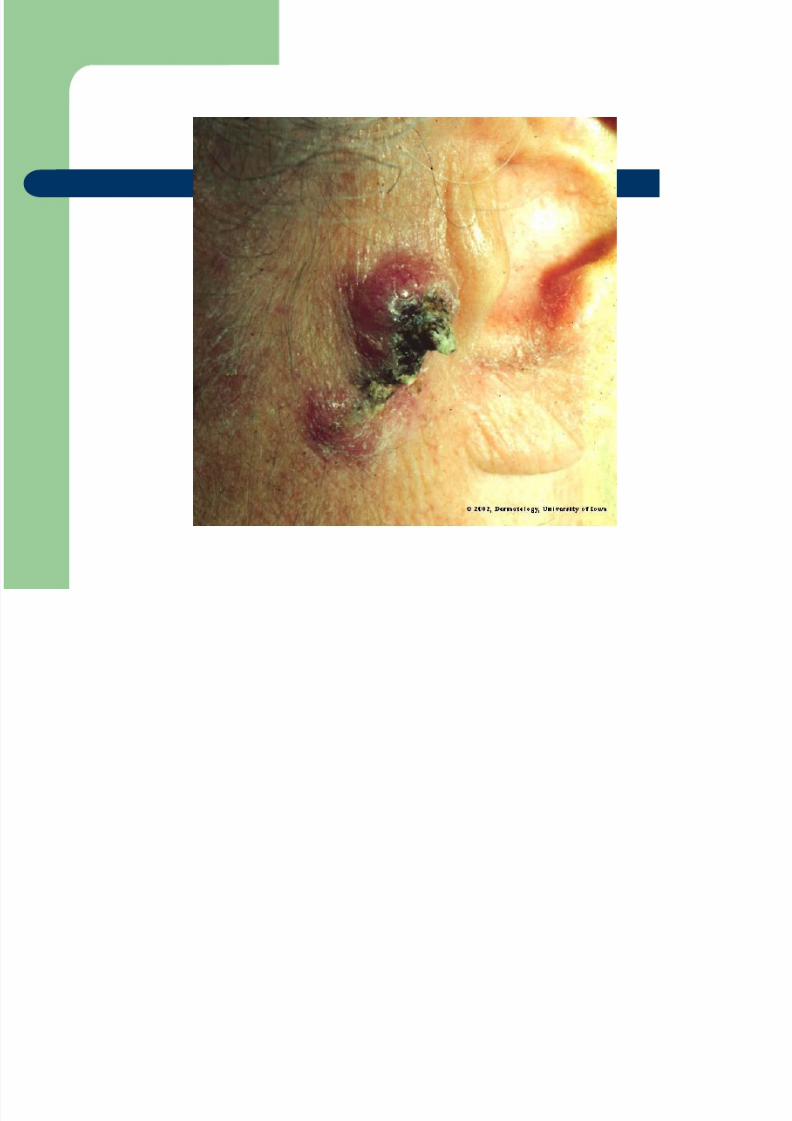
Squamous Cell Carcinoma
Malignant tumor of epithelial keratinocytes. Arises as a resultof exogenous carcinogens (sunlight exposure, exposure toionizing radiation, & other causes). Persons who work outdoors
and have fair skin at higher risk.
Dermatopathology shoes proliferating anaplastic cells thatextend in broad masses into the dermis and SQ tissue.
Treatment involves wide excision. SCC has an overallremission rate after therapy of 90%. Lesions from ionizing
radiation or in an old burn scar are more likely to metastasize.Low rate of metastasis overall. Patients outdoors often need touse sunscreen with high SPF and protective clothing. Avoidtanning beds.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 42/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 43/50
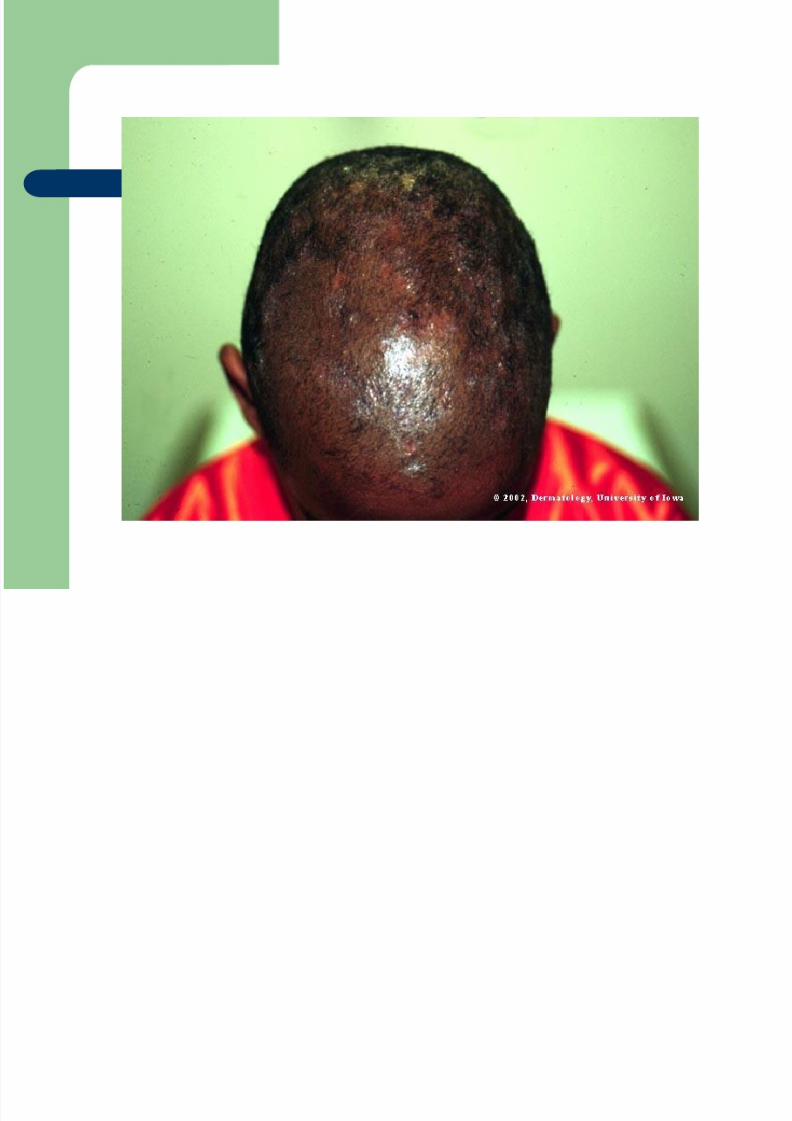
Tinea Capitis
Dermatophytic infection of the scalp. Acute infectioncharacterized by follicular inflammation with painful, boggynodules which drain pus and result in scarring alopecia.
Scaling alopecia is seen in chronic infection.Lymphadenopathy may be seen.
Microsporum audouini, M. canis, Trichophyton tonsurans arecausative agents. May be transmitted person-to-person, or pet-to-person, or via hats, barber utensils.
Treatment with Griseofulvin orally for 1-2 months usuallyneeded. Watch liver functions if on drug for several months.Infection may recur.

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 44/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 45/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 46/50
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 47/50
Varicella
Highly contagious primary infection characterized bysuccessive crops of pruritic vesicles which evolve topustules, crusts, and at times scars. Mildconstitutional symptoms. Known as “Chickenpox”.
Caused by Varicella Zoster virus
Varicella vaccine given routinely now-required forschool admission. Treatment is usuallysymptomatic. Adults may require treatment with
Acyclovir 800 mg 4x daily for 5 days within 24 hoursof illness. May give VZIG to immunocompromisedpatients if exposed to VZV.
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 48/50

8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 49/50
Verruca Vulgaris (Common Wart)
A discrete benign epithelial hyperplasia
manifested by papules and plaques caused
by viral infection.
Caused by human wart viruses of the papova
group, HPV.
Treatment using salicylic acid, liquidnitrogen, curettage with local anesthesia, or
laser surgery
8/11/2019 Dermatology Memory - Answers
http://slidepdf.com/reader/full/dermatology-memory-answers 50/50
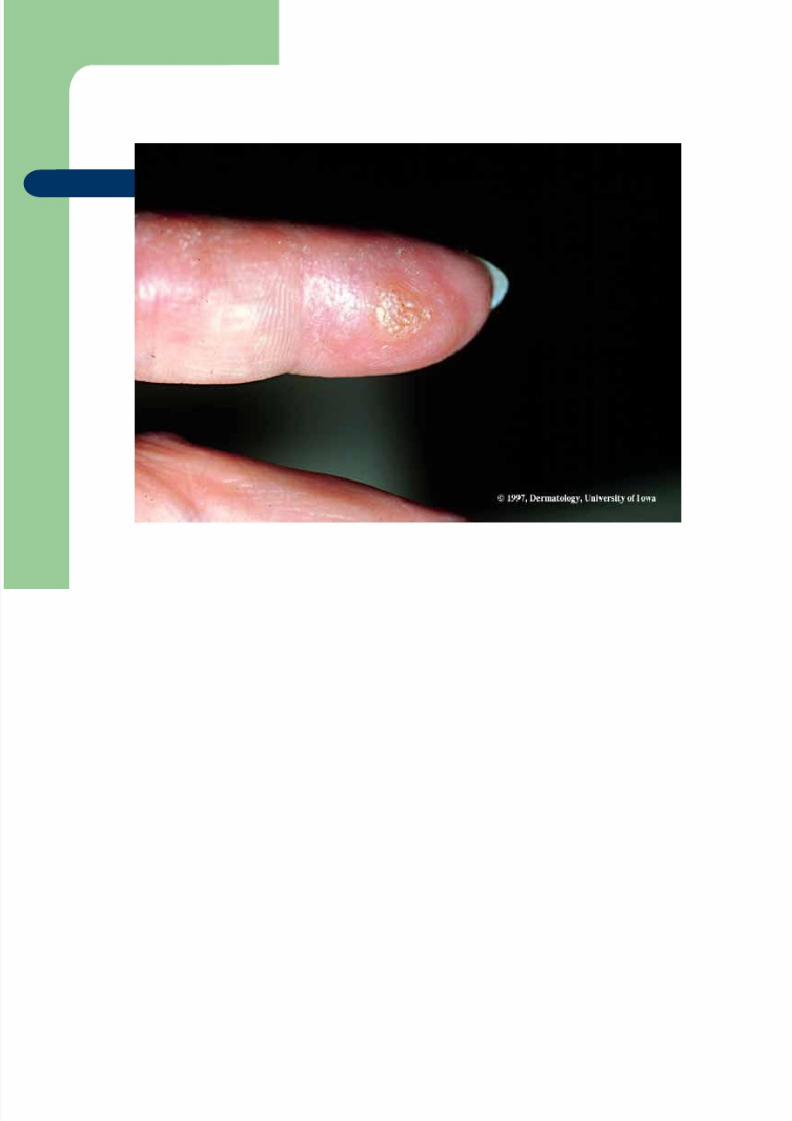
Cellulitis
Cellulitis is a spreading infection of the skinextending to involve the subcutaneous tissues.
The most common causes are group A ß -haemolytic streptococci (GABHS) andStaphylococcus aureus.
Predisposing factors include skin abrasions,lacerations, burns, eczematous skin, etc,
although the portal of entry of organisms is oftennot seen.
Treat with flucolaxacillin

















