[1] 1. INTRODUCTION. Diseases of the heart and blood vessels are the largest cause of mortality across the globe. They are the principle cause of dis ability and death in all industrialized nations. Currently, in US A it causes about 700000 deaths annually which is almost 40% of total mortality. Furthermore, these disease processes cause much suffering because of pain, disability and limb l oss due to peripheral vascular disease (PVD). In the brief history of modern cardiovascular medicine, it has not been uncommon for scientists, researchers and clinicians to join forces in an effort to dramatically change the development and treatment of a specific pathology. The introduction of coronary arteriography, bypass surgery, angioplasty and now, drug-eluting stents has positively influenced the care of patients suffering from lifestyle-limiting anginal symptoms due to obliterative coronary artery disease. In each of these and many other areas currently under study, the common denominator for success has been the ability to create a specific focal point where every available element of laboratory information is translated into a potential broad clinical app lication. About four categories of cardiac illnesses account for 85-90% of the deaths due to cardiac diseases. They are 1. Ischemic Heart diseases. (Diseases due to less blood supply to heart musculature) 2. Hypertensive and pulmonary hypertensive hear t diseases. 3. Congenital heart diseases. (Birth defects like VSD, ASD, T etrology of Fallot) 4. Valvular diseases of heart.
Diseases of the heart and blood vessels are the largest cause of mortality across the
globe. They are the principle cause of disability and death in all industrialized
nations. Currently, in USA it causes about 700000 deaths annually which is almost
40% of total mortality. Furthermore, these disease processes cause much suffering
because of pain, disability and limb loss due to peripheral vascular disease (PVD).
In the brief history of modern cardiovascular medicine, it has not been
uncommon for scientists, researchers and clinicians to join forces in an effortto dramatically change the development and treatment of a specific pathology.
The introduction of coronary arteriography, bypass surgery, angioplasty andnow, drug-eluting stents has positively influenced the care of patients suffering
from lifestyle-limiting anginal symptoms due to obliterative coronary artery
disease.
In each of these and many other areas currently under study, the common
denominator for success has been the ability to create a specific focal point where
every available element of laboratory information is translated into a potential broad clinical application.
About four categories of cardiac illnesses account for 85-90% of the deaths due to
cardiac diseases. They are
1. Ischemic Heart diseases. (Diseases due to less blood supply to heart
musculature)
2. Hypertensive and pulmonary hypertensive heart diseases.
3. Congenital heart diseases. (Birth defects like VSD, ASD, Tetrology of Fallot)
The etiology, pathology and different treatment modalities involved be it medical
or surgical in treating these diseases is beyond the scope of this discussion since
our interest lies in the knowhow of materials, technicalities and researches going
on in the field of development of newer biomaterials which become a part of
cardiovascular system either as prostheses or become ingenious and help inregeneration of lost cardiac or vascular tissue.
Regardless of the arena of options available to treat the cardiovascular diseases, no
technique has been rated as giving 100% cure and safety. The potential risks
involved in treating the cardiac diseases are many- few of which are restenosis,
thrombosis, prolonged bleeding postsurgicaslly, infection and graft rejection and so
on. Therefore the requirement of the day lies in designing and dispensing of newer materials which to some extent helps in overcoming these problems.
During the last few decades, man – made materials and devices have beendeveloped to the point at which they can be used to replace parts of living systems
in the human body. These special materials, which are able to function in intimatecontact with living tissue, with minimal adverse reaction or rejection by the body
are called biomaterials.
“Biomaterial is any substance (other than a drug) or combination of substances,synthetic or natural in origin, which can be used for a period of time, as a whole or
as a part of a system which treats, augments or replaces any tissue, organ or function in the body”.
Two main parameters have to be considered in choosing the biomaterial for a
certain application:
1. In order to choose the right Standard design, some physical and mechanical
features such as strength and deformation, fatigue and creep, friction and wear resistance, flow resistance and pressure drop, and other characteristics which may be engineered with the material, must be considered.
2. Compatibility, or biocompatibility, characterizes a set of material specifications
and constraints which refer to the material – tissue interactions. These
characteristics have to be specified according to the intended device application,
and have to be tested and evaluated in a set of in – vitro and in – vivo experiments.
Biocompatibility evaluation
In order to evaluate the material‟s suitability for the cardiovascular application for long term implantation, the biocompatibility criteria have to include the following
host reactions to the biomaterial which focus on toxicity, carcinogenicity and biostability: Foreign body reaction, Inflammatory reaction, Thrombosis,
Hemolysis, Adaptation, Infection and sterilization, Carcinogenesis,Hypersensitivity and systemic effects, Long term stability, and Fatigue tests.
These studies are designed according to ISO 10993 standards.
Large number of materials has been tested to suit the requirements which include a
variety of natural, synthetic and semi synthetic fibers, polymers, metals and also
the tissue engineered materials.
In the beginning let us place our interest on grafting of cardiac tissues, some
A graft i s a biological material which replaces the indigenous missing tissue with
the same type of tissue der ived from self, other donor or syntheticall y prepared in
a laboratory which best sui ts and simulates the structur e and function of the
tissue being replaced.
The grafts used in human body in general can be classified in following ways.
1. Autografts-Taken from one‟s own body.
2. Allograft-Taken from another donor living or dead.3. Xenograft-Taken from an animal source. (commonly bovine)
4. Synthetic-Commercially prepared in laboratory.
NEED FOR CARDIOVASCULAR TI SSUE GRAFTING:
Diseases of heart and its valves are the major cause of death and deformityglobally. The majority of surgical techniques available so far involves harvesting
of the long saphenous vein from the leg or even the cephalic and basilic veins fromthe arm of the patient. However, in about a third of patients this proves inadequate
or unsuitable. Therefore need for artificial materials which mimic the nature to
maximum extent is always in demand by surgeon. In fact surgeons have alreadysuccessfully tried on materials like polyethylene terephthalate (Dacron),
polytetrafluoroethylene (PTFE), expanded PTFE (ePTFE) and polyurethane.
Another important field which requires extensive research and development of new
materials is the replacement of heart valves.
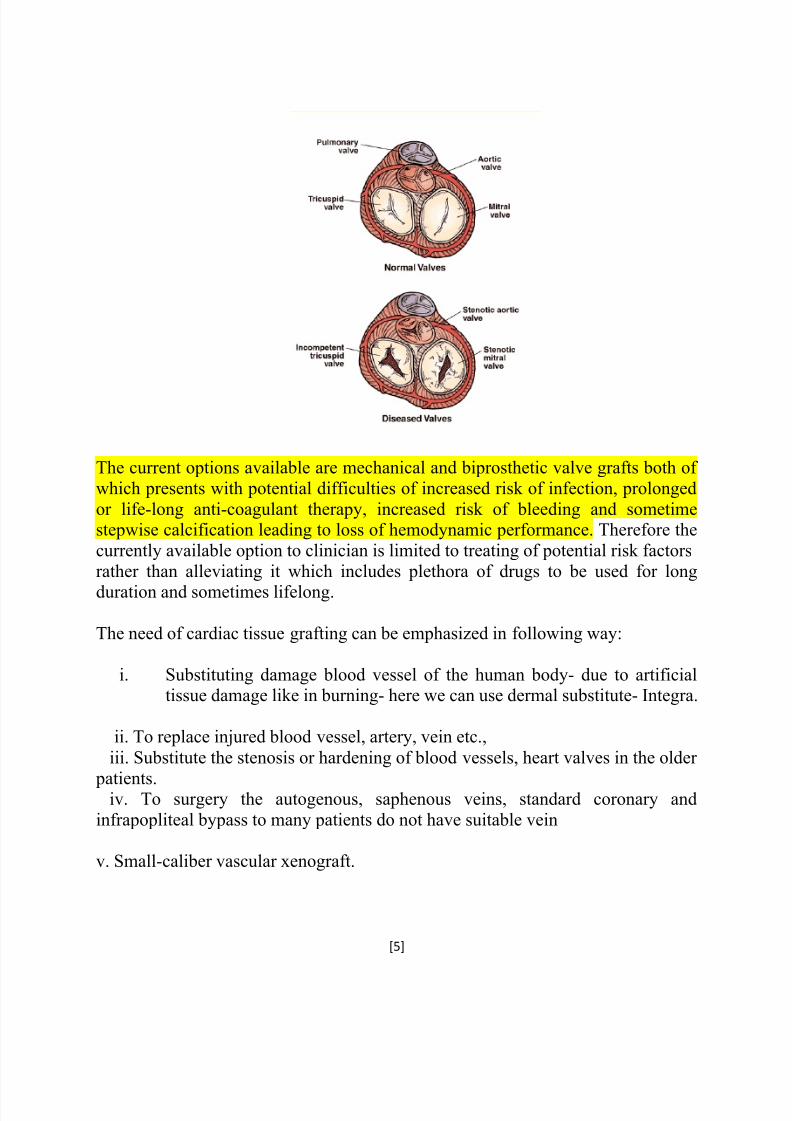
Heart valves are nothing but gateways for the entry and exit of blood vessels into
the chambers (atria and ventricles) of the heart. The specialty of the valves is thatthey open unidirectional, always toward the ventricles so that the regurgitation of
blood to atria will never occur. The left atria-ventricles are guarded by tricuspid
valve, right atria-ventricle guarded by mitral valve. The opening to pulmonaryartery is guarded by pulmonary valve and aorta is guarded by aortic valve.
The current options available are mechanical and biprosthetic valve grafts both of
which presents with potential difficulties of increased risk of infection, prolonged
or life-long anti-coagulant therapy, increased risk of bleeding and sometimestepwise calcification leading to loss of hemodynamic performance. Therefore the
currently available option to clinician is limited to treating of potential risk factors
rather than alleviating it which includes plethora of drugs to be used for long
duration and sometimes lifelong.
The need of cardiac tissue grafting can be emphasized in following way:
i. Substituting damage blood vessel of the human body- due to artificialtissue damage like in burning- here we can use dermal substitute- Integra.
ii. To replace injured blood vessel, artery, vein etc.,
iii. Substitute the stenosis or hardening of blood vessels, heart valves in the older
patients.iv. To surgery the autogenous, saphenous veins, standard coronary and
infrapopliteal bypass to many patients do not have suitable vein
The characteristics of the ideal graft have to fit the following requirements which
are divided into three main parts: mechanical, biocompatibility and handling:
* It must be durable, withstanding after implantation the dual threats of biodegradation and mechanical fatigue.
* The ideal graft should have and maintain the same compliance as a normal
artery: It should be flexible, maintaining its contour and have kinking resistance,
bending without partial occlusion – as it crosses joints.
* The graft must not harm the host in anyway.
* Its luminal surface must interact with blood elements in a minimally traumatic,nonthrombogenic fashion.
* It should be resistant to infection.
* It must be capable of sterilization without graft alteration. The ideal graft should
have an optimal porosity, allowing for good incorporation without causingunmanageable bleeding following implantation.
* Finally, from the handling point of view, it must be readily available in multiplelengths and sizes, and its handling characteristics should include an ease of
Vascular graft mater ials : The synthetic graft market is currently dominated by
three major materials: Polyethylene Terephthalate (PET), Polytetrafluoroethylene(PTFE) and Polyurethanes. As mentioned above, vascular grafts should be
chemically stable and resistant to degradation and to toxic or inflammatory by products. They have to be biocompatible and hemocompatible. Their structure has
to be porotic to an extent that there won‟t be blood leakage. Polyester (Dacron or PET) and PTFE are chemically stable after implantation.
Dacron:
Dacron : There are woven Dacron (not porous), knitted Dacron (porous), crimpedgrafts and newer knitted Dacron which have velour construction on their inner and
outer surfaces that are thought to facilitate tissue incorporation.
In order to reduce the blood loss, knitted grafts sometimes should be pre – clotted
prior to insertion. The pre – clotting procedure is less frequently used in woven grafts because of much smaller pores produced in this technique. Dacron grafts have
recently been manufactured coated with protein (collagen/albumin) to reduce the
blood loss and antibiotics to prevent graft infection.
Expanded PTFE (e-PTFE) : e – PTFE is considered a non textile technique. This is
a fluorocarbon polymer, formed into sheets by a paste extrusion process, producinga porous material that has solid nodes interconnected by fine fibrils.
The intranodal distance can be varied to change the graft porosity. The grafts inclinical use are impervious to blood, resistant to dilatation, and are chemically
inert, highly electronegative and highly hydrophobic. ePTFE is considered to be better than Dacron for venous reconstruction if autogenous vein is not available.
GORE-TEX is the newest vascular graft offering good performance by reducing
kinking and compression. It is the lowest profile, radially supported graft available
today.
The e-PTFE are used to repair occluded arteries and veins and blood vessels in the peripheral artery.
The second use of e-PTEF material is it can be used for dialysis treatment of
chronic renal failure patients. These materials exhibit superior thrombo-resistencewhich leads to prevention of smaller blood vessels getting occluded.
ePTFE grafts- the potential role of fibrin
As we know that fibrin is the most important vascular endothelium growth factor
(VEGF) of the blood vessels. So in this case we use a preteated heparin or fibrinseeded cells on an ePTFE or Dacron for a particular animal. Ongoing platelet
activation provides high concentrations of granule products like platelet factor 3,fibrinogen and von Willebrand factor as well as dense granule contents such as
calcium. At the same time, graft surfaces are continually rinsed by blood with itsundiminishing concentrations of fibrinogen and other clotting factors- like TCF-β
(Thrombin Growth Factor). Thus, the fibrin generated on the inner surface of
vascular prostheses has a particularly high level of fibrinogen – hence excellent
healing properties.
Polyurethanes: Polyurethanes were first introduced
to the medical device market in the earliest 50s as composites foam breast
prosthesis. Since then, a lot of work and development was done to improve their characteristics and biostability. Polyurethanes‟ advantages include a very smooth
non – thrombogenic inner surface, a thin walled graft with some compliance andimproved handling characteristics.
Graft made by synthetic protein polymers cross-linked by γ-rays- new
generation biopolymers:
Synthetic protein polymers cross-linked by γ- irradiation represent a newgeneration of biopolymers. Preliminary reports suggest that they have similar
elasticity as arteries, with a controllable rate of degradation. This recent trendillustrates the limitations of PTFE and Dacron at lower flow rates and stresses the
need for alternative biomaterials. Materials such as PTFE and Dacron have little potential for micro-vessel grafts due to their poor haemodynamics caused by lack
of arterial compliance. This results in thrombogenicity to the extent that in low-flow applications (as is the care for microvessels) below 4mm their usage is
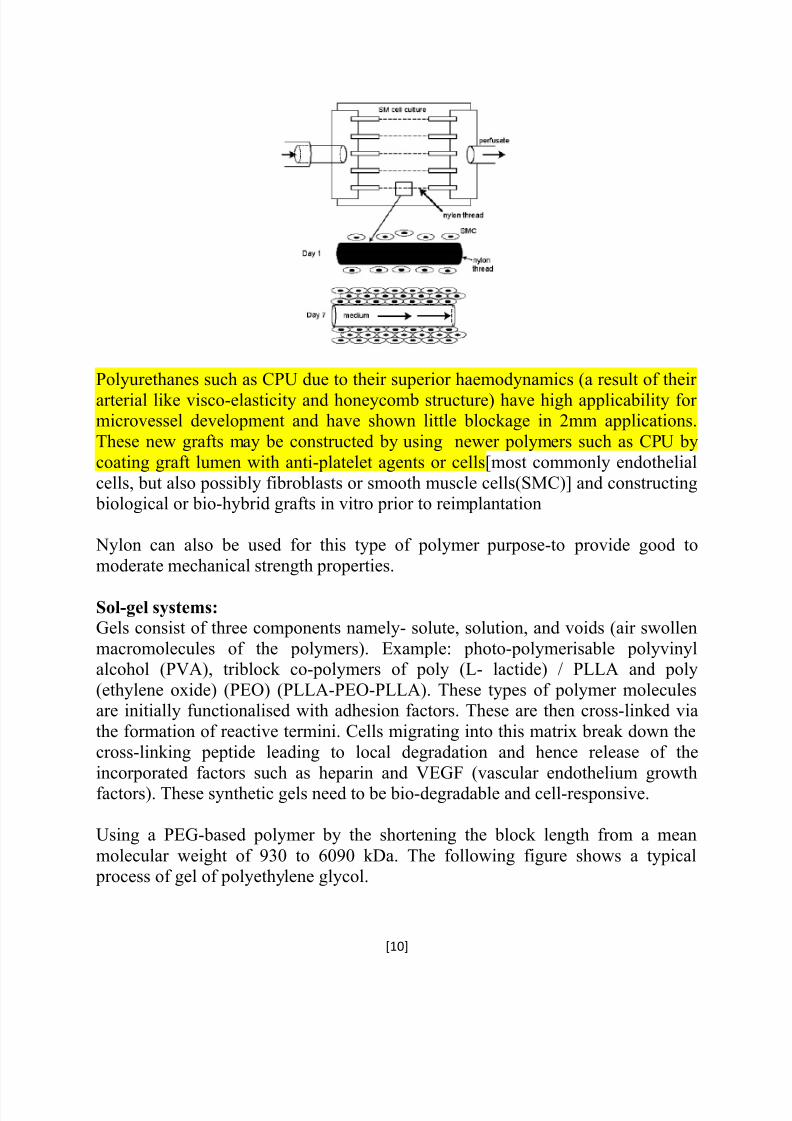
Polyurethanes such as CPU due to their superior haemodynamics (a result of their
arterial like visco-elasticity and honeycomb structure) have high applicability for microvessel development and have shown little blockage in 2mm applications.
These new grafts may be constructed by using newer polymers such as CPU by
coating graft lumen with anti-platelet agents or cells[most commonly endothelial
cells, but also possibly fibroblasts or smooth muscle cells(SMC)] and constructing biological or bio-hybrid grafts in vitro prior to reimplantation
Nylon can also be used for this type of polymer purpose-to provide good to
moderate mechanical strength properties.
Sol-gel systems:
Gels consist of three components namely- solute, solution, and voids (air swollen
macromolecules of the polymers). Example: photo-polymerisable polyvinylalcohol (PVA), triblock co-polymers of poly (L- lactide) / PLLA and poly
(ethylene oxide) (PEO) (PLLA-PEO-PLLA). These types of polymer moleculesare initially functionalised with adhesion factors. These are then cross-linked via
the formation of reactive termini. Cells migrating into this matrix break down the
cross-linking peptide leading to local degradation and hence release of the
incorporated factors such as heparin and VEGF (vascular endothelium growthfactors). These synthetic gels need to be bio-degradable and cell-responsive.
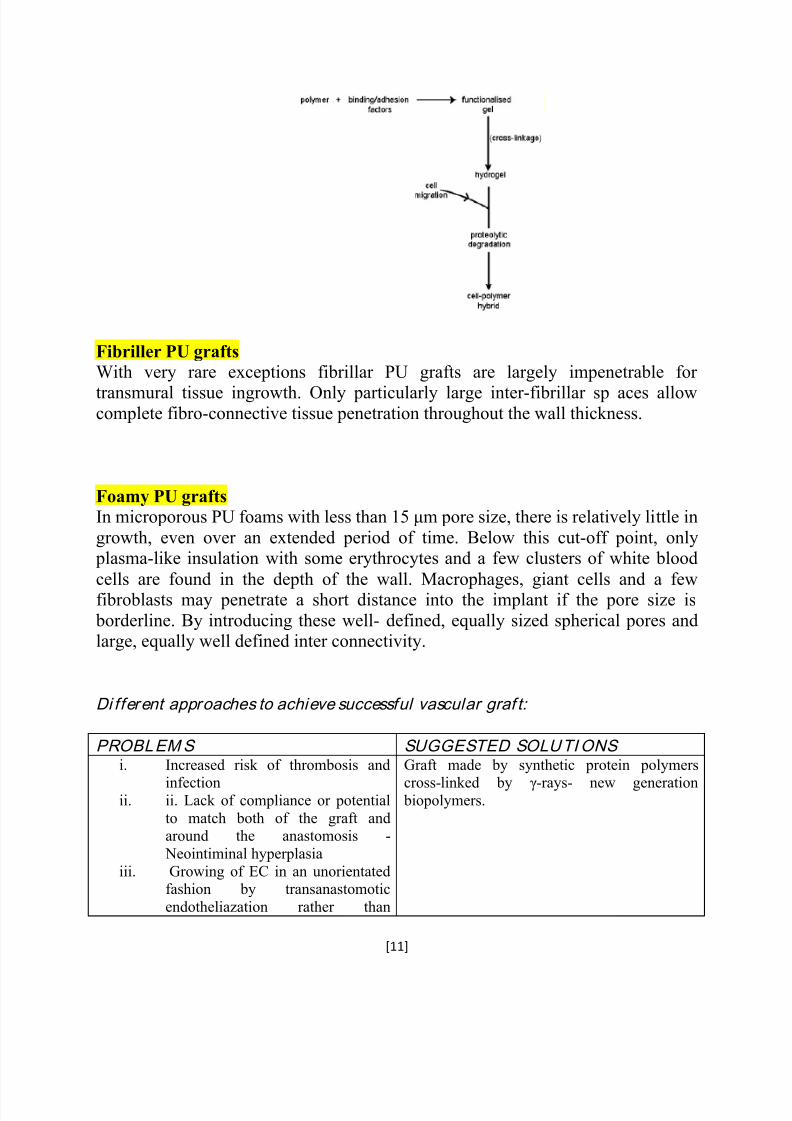
Using a PEG-based polymer by the shortening the block length from a mean
molecular weight of 930 to 6090 kDa. The following figure shows a typical process of gel of polyethylene glycol.
With very rare exceptions fibrillar PU grafts are largely impenetrable for
transmural tissue ingrowth. Only particularly large inter-fibrillar sp aces allowcomplete fibro-connective tissue penetration throughout the wall thickness.
Foamy PU grafts
In microporous PU foams with less than 15 μm pore size, there is relatively little in
growth, even over an extended period of time. Below this cut-off point, only plasma-like insulation with some erythrocytes and a few clusters of white blood
cells are found in the depth of the wall. Macrophages, giant cells and a fewfibroblasts may penetrate a short distance into the implant if the pore size is
borderline. By introducing these well- defined, equally sized spherical pores andlarge, equally well defined inter connectivity.
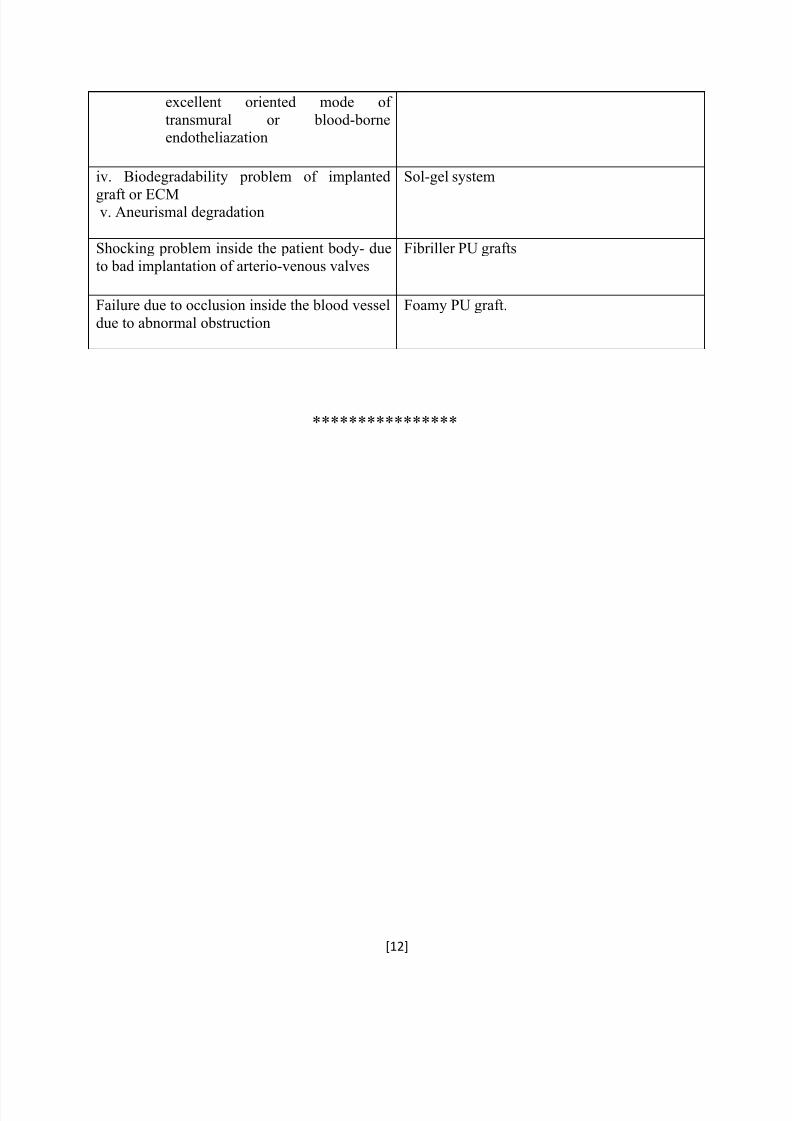
Di fferent approaches to achieve successful vascular graf t:
PROBLEMS SUGGESTED SOLUTIONS i. Increased risk of thrombosis and
infectionii. ii. Lack of compliance or potential
to match both of the graft andaround the anastomosis -
Neointiminal hyperplasia
iii. Growing of EC in an unorientatedfashion by transanastomotic
endotheliazation rather than
Graft made by synthetic protein polymers
cross-linked by γ-rays- new generation biopolymers.
Revolutionary advances in nanotechnology propose novel materials with superior
properties for biomedical application. One of the most promising nonmaterial for biomedical application is polyhedral oligomericsilsesquioxane (POSS), an amazing
nanocage consisting of an inner inorganic framework of silicon and oxygen atomsand an outer shell of organic groups. The unique properties of this nanoparticle has
led to the development of a wide range of nanostructured copolymers withsignificantly enhanced properties including improved mechanical, chemical, and
physical characteristics. Since POSS nanomaterials are highly biocompatible,
biomedical application of POSS nanostructures has been intensely explored. Oneof the most promising areas of application of POSS nanomaterials is the
development of cardiovascular implants. The incorporation of POSS into
biocompatible polymers has resulted in advanced nanocomposite materials withimproved hemocompatibility, antithrombogenicity, enhanced mechanical andsurface properties, calcification resistance, and reduced inflammatory response,
which make these materials the material of choice for cardiovascular implants.
Currently, application of POSS containing polymers in the development of new
generation cardiovascular implants including heart valve prostheses, bypass grafts,and coronary stents is under intensive investigation, with encouraging outcomes.
Surface modification of biomaterials used in cardiovascular grafts or implants isvery much necessary since they modulate the platelet responses by directly
modulating the thrombogenic proteins or by inducing antithrombogenic biomolecules.
Nanotechnology is recognising a great role in such surface modification of
cardiovascular implants through bio-functionalization of polymers and peptides innanocomposites and through nanofabrication of polymers which will pave the way
for finding a closer blood match through haemostasis when developing
cardiovascular implants with a greater degree of patency.
Silver nanoparticles or nanosilver (NS) are recognized for efficient antibacterial
properties. This study aims to determine the influence of NS integrated POSS-PCUon thrombogenicity. Silver nitrate was reduced with dimethylformamide and
stabilized by the inclusion of fumed silica nanoparticles to prevent aggregation of NS and were incorporated into POSS-PCU to form a range of POSS-PCU-NS
concentrations (by weight); 0.20%, 0.40%(NS32), 0.75%(NS64), and
1.50%(NS128). Surface wettability was determined with sessile-drop water contactangles. Platelets were introduced onto test samples and Alamar Blue (AB),
mitochondrial-activity assay, quantified the degree of platelet adhesion whilst
platelet-factor-4 (PF4) ELISA quantified the degree of platelet activation.Thromboelastography (TEG) determined the profiles of whole blood kinetics while
hemolysis assay demonstrated the degree of blood compatibility. Increasing levelsof NS induced greater hydrophilicity. A concentration dependant decrease in
platelet adhesion and activation was observed with AB and PF4 readings,respectively.
5. TECHNICAL CONSIDERATION OF CARDIOVASCULAR GRAFTS
1. Microvascular grafts:
Human micro vasculature begins with arteries dividing consecutively into smaller branches like meta-arterioles (80 –100μm) until finally forming capillaries (10–
15μm). These vessels serve to redistribute blood and its nutrients whilst lowering
the pressure head. This allows blood to perfuse the tissue, allowing more efficientexchange of metabolites.
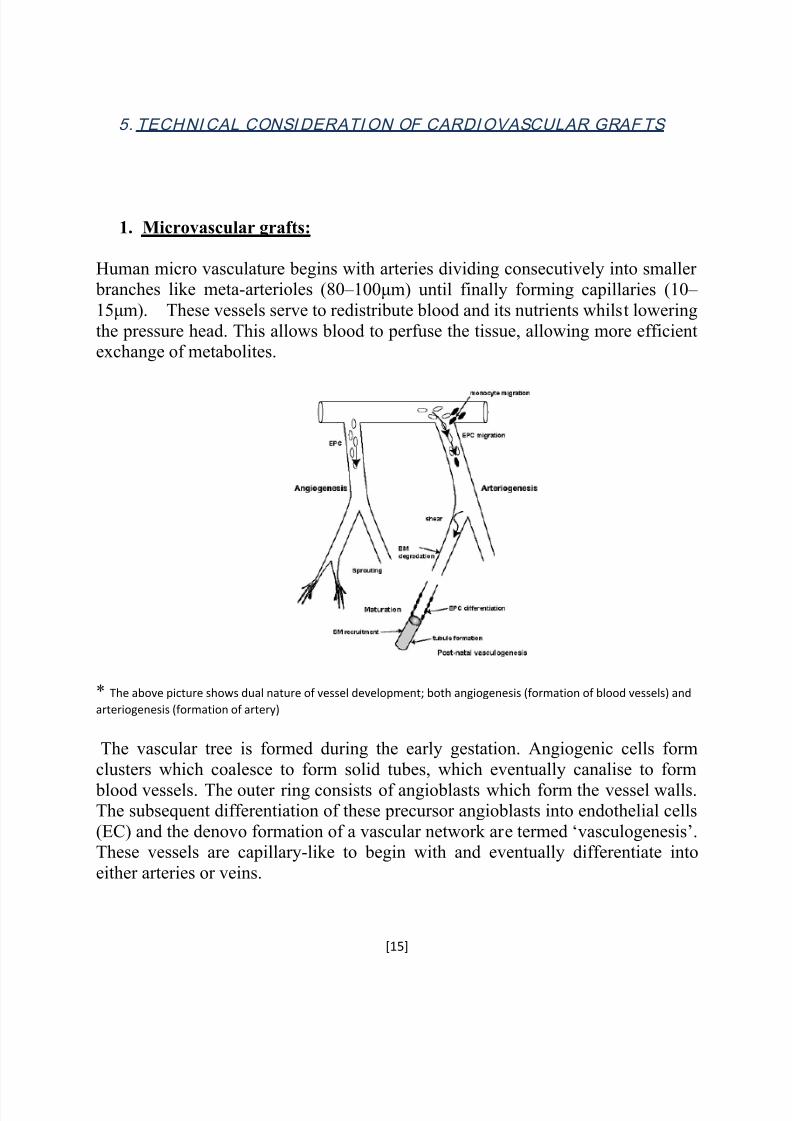
* The above picture shows dual nature of vessel development; both angiogenesis (formation of blood vessels) and
arteriogenesis (formation of artery)
The vascular tree is formed during the early gestation. Angiogenic cells form
clusters which coalesce to form solid tubes, which eventually canalise to form
blood vessels. The outer ring consists of angioblasts which form the vessel walls.The subsequent differentiation of these precursor angioblasts into endothelial cells
(EC) and the denovo formation of a vascular network ar e termed „vasculogenesis‟.These vessels are capillary-like to begin with and eventually differentiate into
The adult vascular network remodels itself by arteriogenesis with the opening up
and then the subsequent enlargement of existing collaterals (so-called collateralenlargement), as well as the formation of completely new vessels from the already
existing vessels (so-called arterialisation). Micro-vascular remodelling is a
mechanistic process delineated to the specific tissue type and specific stimuli.Therefore, with the exceptions of skeletal muscle responding to exercise and the
female menstrual cycle itself, micro-vascular remodelling is limited solely to pathological situations, in particular inflammation, wound healing, ischemia.
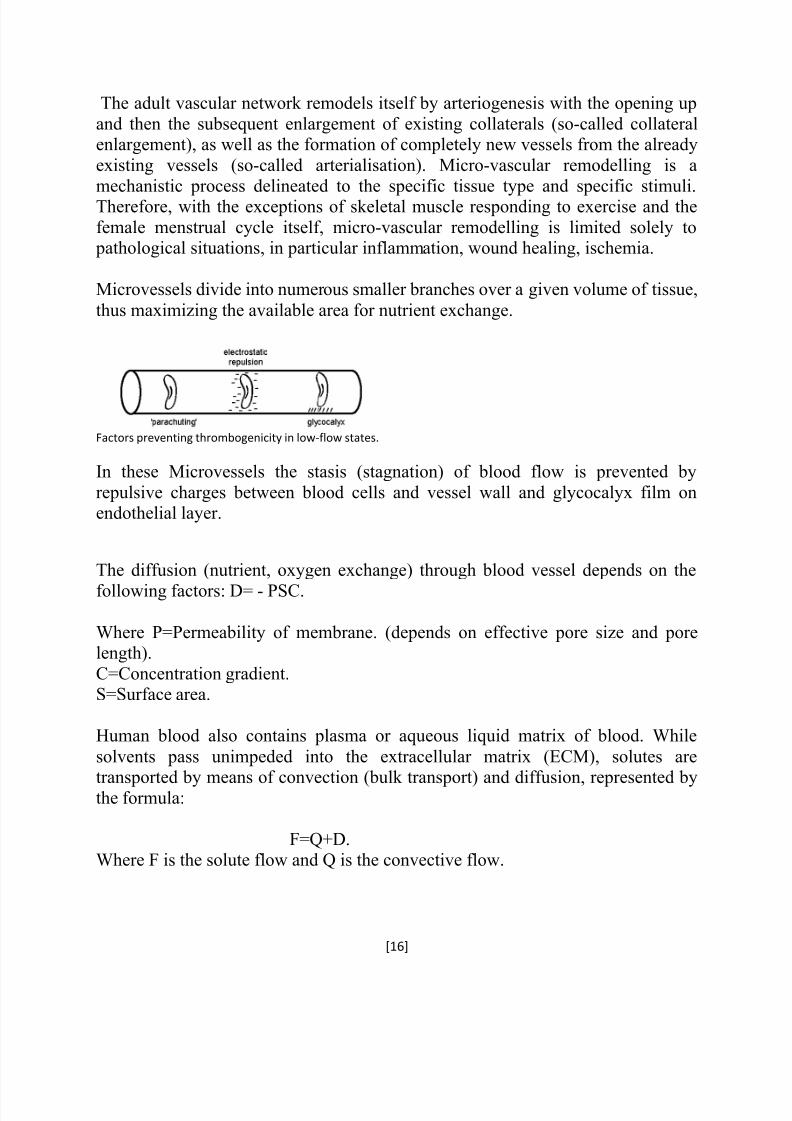
Microvessels divide into numerous smaller branches over a given volume of tissue,
thus maximizing the available area for nutrient exchange.
Factors preventing thrombogenicity in low-flow states.
In these Microvessels the stasis (stagnation) of blood flow is prevented by
repulsive charges between blood cells and vessel wall and glycocalyx film onendothelial layer.
The diffusion (nutrient, oxygen exchange) through blood vessel depends on the
following factors: D= - PSC.
Where P=Permeability of membrane. (depends on effective pore size and porelength).
C=Concentration gradient.S=Surface area.
Human blood also contains plasma or aqueous liquid matrix of blood. While
solvents pass unimpeded into the extracellular matrix (ECM), solutes are
transported by means of convection (bulk transport) and diffusion, represented bythe formula:
F=Q+D.Where F is the solute flow and Q is the convective flow.
Solute efflux is dependent on the rate of solvent transfer within the medium.
Solutes like glucose are transported via convection with water (solvent)
Some recent studies have shown that the nutrient exchange depends on balance
between the hydrostatic pressure, osmotic pressure and interstitial pressure in amicrovessel.
The configuration of Microvessels is something like this: The microvessels with a
cross-sectional density of 1300 per mm2 and inter capillary distance of 34 μm toform a rich perfusing network.
Based on the above configuration the size of the microvascular grafts have internaldiameter of 1mm or less and may be classified into conducting arterial and
distributing capillary blood vessel.
The construction of arterial conduits is based on small-calibre vascular grafttechnology. These new grafts may be constructed by using (a) newer polymers
such as CPU (b) by coating graft lumen with anti-platelet agents or cells[most
commonly endothelial cells, but also possibly fibroblasts or smooth muscle cells(SMC)] and (c) constructing biological or bio-hybrid grafts in vitro prior to
reimplantation. Although the autologous vein grafts the current gold standard for
micro-vascular repairs, are compliant and non-thrombogenic, they are limited bythe need for additional vein-harvesting procedures. Furthermore, the construction
of artificial vascularised tissue requires an inherent vascular network. Vein grafts
are not suitable for this purpose as it is technically impossible to dissect out acapillary bed in its entirety.
Materials used in microvascular grafts: Polyester, polyethylene terepthalate,
polyurethane etc. Poly (carbonate-urea) urethane (CPU) can also be used as the
vascular graft with advanced effect of physiological shear stress. However, these prosthetic materials prove to be inferior to autologous conduits, especially when
the vessel diameter is less than 5mm. The problems include increased risk of
thrombosis and infection, limited durability, lack of compliance both of the graftand around the anastomosis, and failure due to restenosis, thus necessitating further
interventions. Currently several groups are working towards the development of
Macrovascular grafts account for the blood vessels whose diameter is more than 1
mm. The materials used in microvascular grafts have also been successfully used
in grafting bigger vessels of which Dacron and PTEF are clinically moreacceptable for peripheral bypass grafts where the patency is significantly lower in
grafts smaller than 6 mm in diameter.
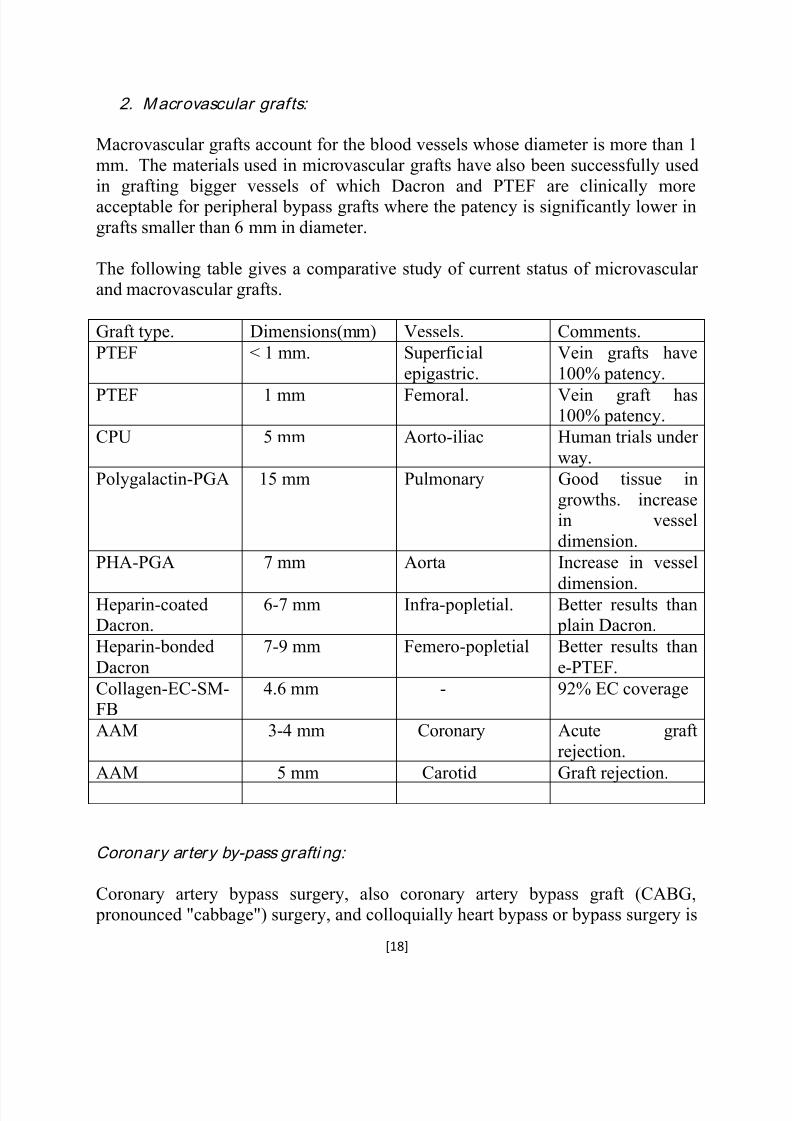
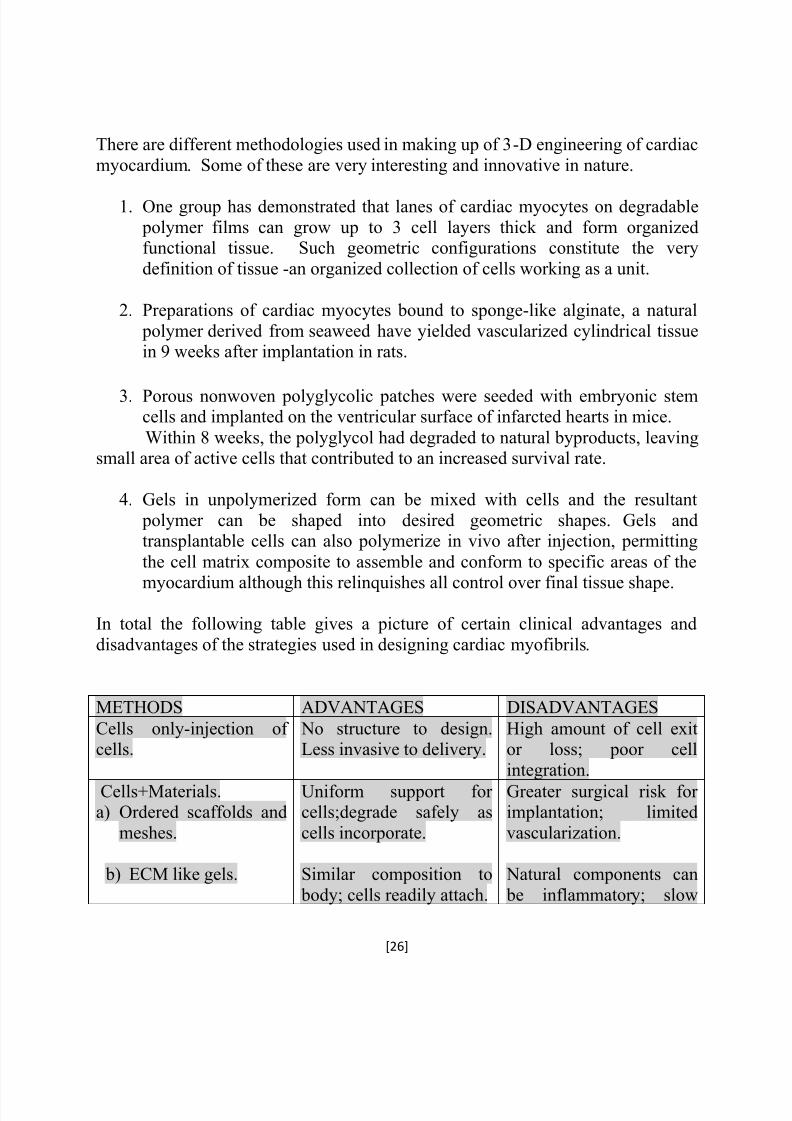
The following table gives a comparative study of current status of microvascular and macrovascular grafts.
Graft type. Dimensions(mm) Vessels. Comments.
PTEF < 1 mm. Superficial
epigastric.
Vein grafts have
100% patency.
PTEF 1 mm Femoral. Vein graft has100% patency.
CPU 5 mm Aorto-iliac Human trials under
way.
Polygalactin-PGA 15 mm Pulmonary Good tissue in
growths. increasein vessel
dimension.
PHA-PGA 7 mm Aorta Increase in vessel
dimension.Heparin-coatedDacron.
6-7 mm Infra-popletial. Better results than plain Dacron.
Heparin-bonded
Dacron
7-9 mm Femero-popletial Better results than
e-PTEF.
Collagen-EC-SM-FB
4.6 mm - 92% EC coverage
AAM 3-4 mm Coronary Acute graft
rejection.
AAM 5 mm Carotid Graft rejection.
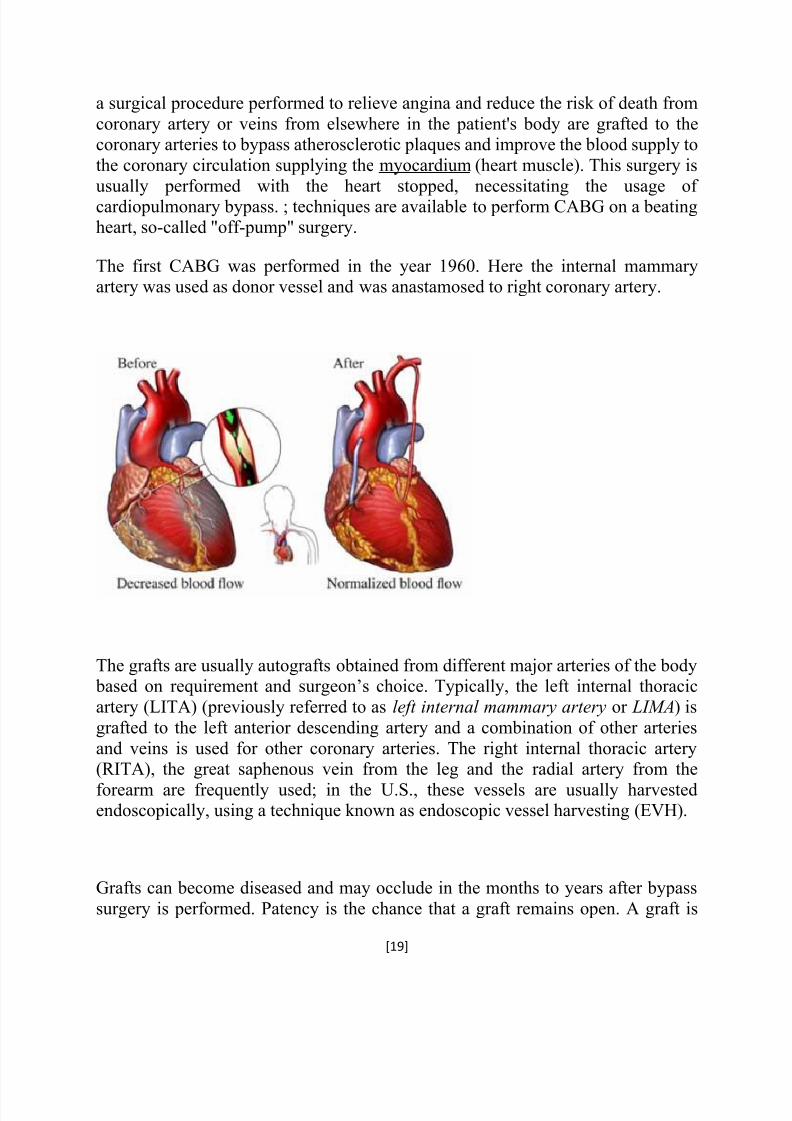
Coronary artery by-pass grafti ng:
Coronary artery bypass surgery, also coronary artery bypass graft (CABG, pronounced "cabbage") surgery, and colloquially heart bypass or bypass surgery is
a surgical procedure performed to relieve angina and reduce the risk of death from
coronary artery or veins from elsewhere in the patient's body are grafted to thecoronary arteries to bypass atherosclerotic plaques and improve the blood supply to
the coronary circulation supplying the myocardium (heart muscle). This surgery is
usually performed with the heart stopped, necessitating the usage of cardiopulmonary bypass. ; techniques are available to perform CABG on a beatingheart, so-called "off-pump" surgery.
The first CABG was performed in the year 1960. Here the internal mammaryartery was used as donor vessel and was anastamosed to right coronary artery.
The grafts are usually autografts obtained from different major arteries of the body based on requirement and surgeon‟s choice. Typically, the left internal thoracic
artery (LITA) (previously referred to as left internal mammary artery or LIMA) is
grafted to the left anterior descending artery and a combination of other arteries
and veins is used for other coronary arteries. The right internal thoracic artery(RITA), the great saphenous vein from the leg and the radial artery from the
forearm are frequently used; in the U.S., these vessels are usually harvestedendoscopically, using a technique known as endoscopic vessel harvesting (EVH).
Grafts can become diseased and may occlude in the months to years after bypass
surgery is performed. Patency is the chance that a graft remains open. A graft is
considered patent if there is flow through the graft without any significant (>70%diameter) stenosis in the graft.
Graft patency is dependent on a number of factors, including the type of graft used(internal thoracic artery, radial artery, or great saphenous vein), the size or the
coronary artery that the graft is anastomosed with, and, of course, the skill of thesurgeons performing the procedure.
However the existing materials have not been proved successful in replacing
smaller diameter blood vessels. Tissue engineering offers the potential of providingvessels that can be used to replace diseased and damaged native blood vessels.
The cardiovascular diseases are becoming a major fear in the present era all over
the globe. The cardiovascular tissue engineering (TE) can become an ideal
substitute to replace all of these cardiac problems like: cardiovascular grafting,valves, micro vessel construction, aorta and vein formation.
Damage to heart muscle, acute or chronic, has long been considered a tipping pointfor individual health outlook and progression to heart failure. The problem is that
adult heart muscle cells, the cardiac myocytes cannot divide to replace the injured
cells. Thus despite a limited population of resident cardiac stem cells the heartcannot repair itself by any native processes. Instead, a scar tissue develops over
regions of damaged myocardium. Such scar tissue keeps the organ intact butcannot contract. The ideal clinical intervention would either avoid such scar
formation or simply replace formed scar tissue with functioning cardiac muscletissue.
In recent years, the emerging cardiac tissue engineering provides a new therapeutic
method for heart diseases. And in the tissue engineering, the scaffold material
which can mimic the structure of the extracellular matrix properly is a key factor.
The rapid expansion of nano-scaffolds during the past ten years has led to new perspectives and advances in biomedical research as well as in clinical practice.
The requirement of the field would include a material which will replace the
damaged cardiac tissue to the fullest extent and at the same time exhibit all the properties necessary for the cardiac muscle activity namely contraction and
conduction of electrical impulses. Therefore the purpose of tissue engineering in
general and cardiac muscles in particular is that it has to create a viable cellular environment through the use of biologically acceptable materials. The idea is that
transplantable cells can be contained and organized in so called engineering
scaffolds. Such scaffolds with contained cells can then be sued to treat or replace a
part of the body, say the cardiac tissue. Empty fabricated structures can also beimplanted in vivo in providing a structure to condition stem cells already present.
Therefore the purpose of such design is to make a livable structure. In case of
cardiac tissue, healthy and functional cardiac myocytes would be the idealinhabitants.
The purpose of cardiac tissue engineering is to replace or repair injured heart
muscle effectively. Supporting materials to create habitable spaces can provide the
basic requirements of cardiac muscle cells. The design of such supportingmaterials influences the behavior of cells; the shape, dimensions, and chemistry of
substrates affect such processes as attachment, cell signaling, and differentiation.As cardiac muscle cells flourish in artificial environments, they may become
functional tissue with clinical value.
I DENTI FYING THE BASIC CELL RESPONSES
Simulation of host-cell environment to its closest is of a great importance in
selecting and designing any biomaterial. A tissue engineered material when takenas a scaffold for impregnation of myocytes should support the cardiac cells 3-
dimensionally and also effectively mimic the local microenvironment.
Slight changes beyond a uniformly flat state can affect cardiac myocytes. Collagen,
the most abundant constituent of the extracellular matrix, has a bundle diameter
measured in the nanometer rangeV100 to 1,000 times smaller than the micrometer average cardiac myocyte diameter. Just as cells are influenced by extracellular
proteins like collagen, so also are they capable of responding to artificial
structures in the same size range. Meshes of electro spun nanofibers supportcardiac myocyte adhesion and spontaneous contraction.
Stimuli other than surface topography can also have robust cellular consequences.Mechanical forces, either generated from cell contraction or sensed from
external sources, have pronounced effects on differentiation, growth, and survivalof myocardial cells. For instance, experimentally exposing cardiac myocytes
to repeated stretching in specific directions alters amounts of contractile proteins.
when material or matrix stiffness is tuned to the range of native muscle rigidity
(bearing a Young‟s modulus a measure of resistance to deformation between 8 and17 kPa), mesenchymal stem cells are induced to differentiate into a myogenic
lineage. The clinical implications of controlling stiffness can be appreciated when
it is recognized that collagen, a primary component of scar tissue that isoverproduced in heart failure, has a relatively high stiffness. Although designing
around forces and stiffnesses may seem rudimentary, the interplay of these 2 physical elements has great significance for cardiac tissue engineering.
Before getting into the actual designing of cardiac muscle tissue it is imperative toknow the anatomy of the cardiac musculature. The musculature or the muscles of
the body has been divided into 3 major categories based on the functionality of thetissue.
They are as follows:1. Voluntary muscles.(Skeletal Muscles).
The cardiac muscle is again an involuntary muscle but classified and considered
separately because of the specialized function it performs, the conduction of electrical impulses across the heart which leads to the rhythmic contraction of heart.
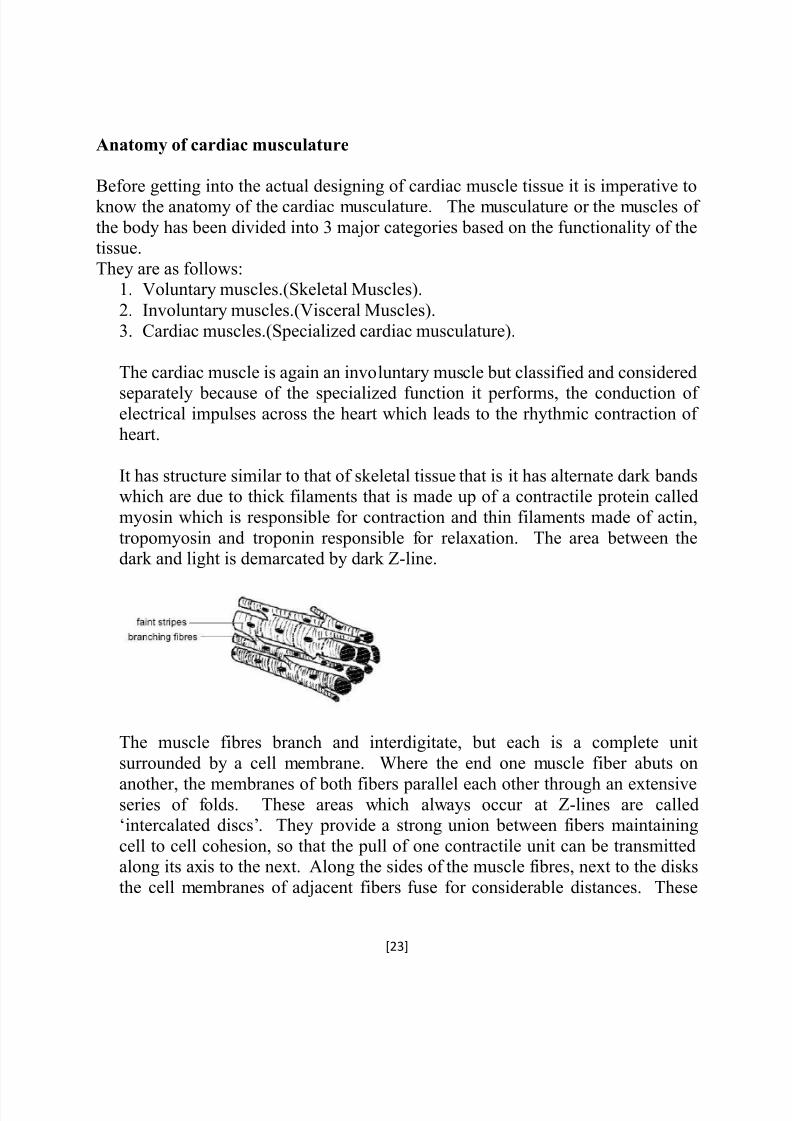
It has structure similar to that of skeletal tissue that is it has alternate dark bandswhich are due to thick filaments that is made up of a contractile protein called
myosin which is responsible for contraction and thin filaments made of actin,
tropomyosin and troponin responsible for relaxation. The area between thedark and light is demarcated by dark Z-line.
The muscle fibres branch and interdigitate, but each is a complete unit
surrounded by a cell membrane. Where the end one muscle fiber abuts on
another, the membranes of both fibers parallel each other through an extensiveseries of folds. These areas which always occur at Z-lines are called„intercalated discs‟. They provide a strong union between fibers maintaining
cell to cell cohesion, so that the pull of one contractile unit can be transmittedalong its axis to the next. Along the sides of the muscle fibres, next to the disks
the cell membranes of adjacent fibers fuse for considerable distances. These
gap junctions provide low-resistance bridges for the spread of excitation from
one fiber to another.
Mechanical properties of cardiac muscles:
Contractile response : The contractile response of cardiac muscle begins just
after the start of depolarization (loss of excitation) and lasts about one and half times as long as action potential. The Calcium ion extracellular fluid as well as
sarcoplasmic reticulum (network of protective fibres around muscles)contributes for contraction.
Isoforms: The cardiac muscle is slow and the fibers are dependent on oxidativemetabolism and hence on a continuous supply of Oxygen.
Corr elation between muscle fiber length and tension: The relation betweeninitial fiber length and total tension in cardiac muscle 1is similar to skeletalmuscle; there is resting length at which the tension developed upon stimuli is
maximal.
Metabolism: Mammalian hearts have an abundant blood supply, numerous
mitochondria and a high content of myoglobin a muscle pigment that may function
as an oxygen storage mechanism.
Pacemaker tissue: The pacemaker tissue is a specialized bundle of heart
muscle fibers which have the potentiality to initiate repetitive action potential.It makes up the conduction system that normally spreads impulses throughout
the heart. The pacemaker is characterized by an unstable membrane potential.
Much of cardiac tissue engineering involves the struggle to perfect cellular
organization without sacrificing tissue vascularization. The in vivo myocardiumhas a very dense layout, with overlapping arrays of muscle cells arranged in
different circumferential orientations. Individual branched cardiac myocytes inthe heart are linked to others at both ends through intercalated discs (containing
gap junctions and other adherent sites) that help to transfer both molecular
signals (eg, electrical coupling) and forces of contraction. Replicating this cellular
organization of the myocardium has proved very difficult.
Therefore the complexity of engineered tissue increases from 2-D to 3-D. Here,levels of diffusion determine the degree of nutrient delivery and metabolic waste
removal available to cells in the construct interior. The thickness of normal,diastolic left ventricular myocardium is a little more than 1 cm in the human heart,
but there is a 200-2m tissue depth limit for the diffusion of oxygen. Therefore,cell survival in 3D cardiac tissue constructs depends on angiogenesis and
functional vascular integration to serve the remaining 95% of the heart wall.
Therefore certain general factors are always considered while designing materials
for cardiac conditions. They are
1. MATERIALS AND DEGRADATION-Besides non-inflammatory incomposition the material should degrade steadily over the time as native
supports are built around the cell.
2. ATTACHMENT: Cardiac myocytes are anchorage-dependent i.e., for
proper functioning their surface attachment is very important.
3. DIFFUSION AND POROSITY: Cells contained in 3-D constructs risks
poor diffusion of vital nutrients and gases while porosities can shape the
capacity for the vascularization.4. STIFNESS: The rigidity of cell substrate affects cardiac myocyte
morphology and commitment of stem cells to lineage.
5. FORCES: Just as in regular heart beating the cardiac myofibrils are
sensitive to mechanical forces, both in magnitude and frequency.
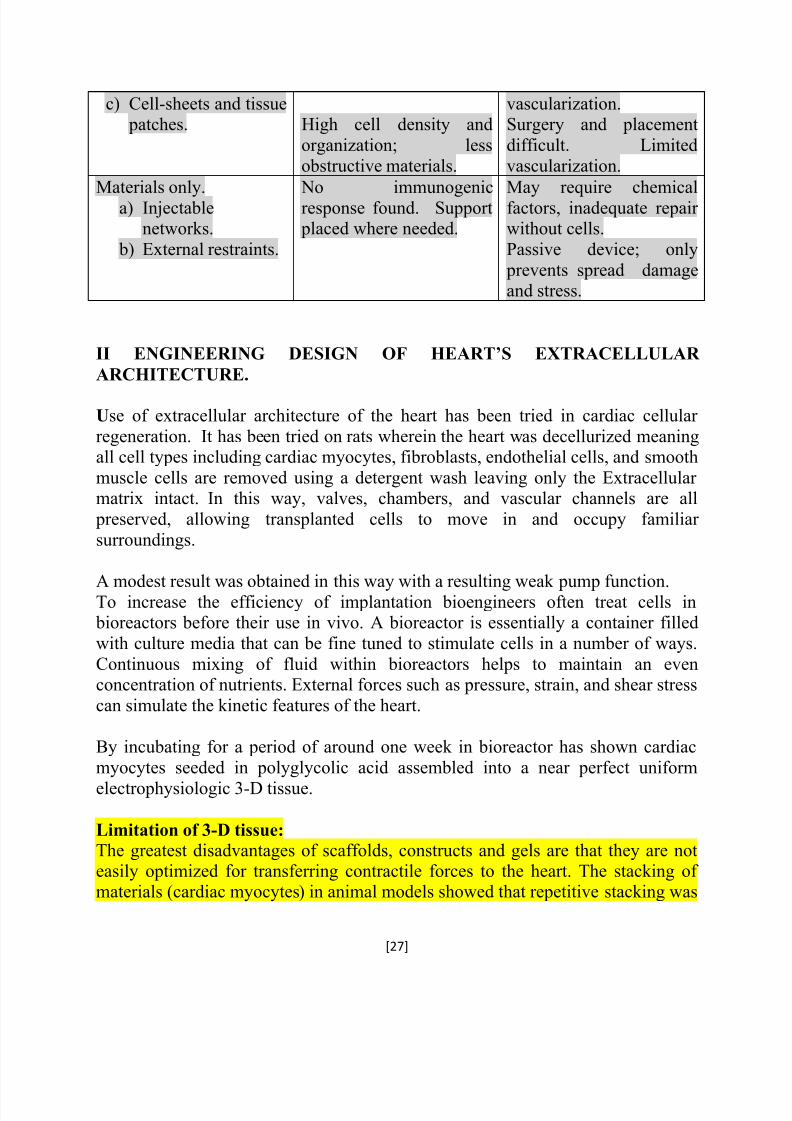
c) Cell-sheets and tissue patches. High cell density and
organization; less
obstructive materials.
vascularization.Surgery and placement
difficult. Limited
vascularization.
Materials only.a) Injectablenetworks.
b) External restraints.
No immunogenicresponse found. Support placed where needed.
May require chemicalfactors, inadequate repair without cells.
Passive device; only
prevents spread damageand stress.
II ENGINEERING DESIGN OF HEART’S EXTRACELLULAR
ARCHITECTURE.
Use of extracellular architecture of the heart has been tried in cardiac cellular
regeneration. It has been tried on rats wherein the heart was decellurized meaningall cell types including cardiac myocytes, fibroblasts, endothelial cells, and smooth
muscle cells are removed using a detergent wash leaving only the Extracellular matrix intact. In this way, valves, chambers, and vascular channels are all
preserved, allowing transplanted cells to move in and occupy familiar
surroundings.
A modest result was obtained in this way with a resulting weak pump function.To increase the efficiency of implantation bioengineers often treat cells in bioreactors before their use in vivo. A bioreactor is essentially a container filled
with culture media that can be fine tuned to stimulate cells in a number of ways.
Continuous mixing of fluid within bioreactors helps to maintain an evenconcentration of nutrients. External forces such as pressure, strain, and shear stress
can simulate the kinetic features of the heart.
By incubating for a period of around one week in bioreactor has shown cardiac
myocytes seeded in polyglycolic acid assembled into a near perfect uniform
electrophysiologic 3-D tissue.
Limitation of 3-D tissue:
The greatest disadvantages of scaffolds, constructs and gels are that they are noteasily optimized for transferring contractile forces to the heart. The stacking of materials (cardiac myocytes) in animal models showed that repetitive stacking was
It is interesting to note that the number of patients requiring heart valvereplacement will increase by 2 folds in next three decades. Currently available
valves does not replace the nativity of the tissue to 100%. Heart valve tissueengineering is a promising technology to overcome these problems.
Currently available heart valve prostheses are categorized into mechanical and
bioprosthetic value. Mechanical valves offer excellent structural durability butinherently prone to thromboemolic events due to high physiologic stress.
Therefore the patients have to be on life-long thrombolytic drug therapy.
Bioprostheses are more susceptible structural wall degradation.
There are three approaches to achieving the goal of an engineered tissue heartvalve: (1) cell seeding of biodegradable synthetic scaffolds, (2) cell seeding of
processed tissue scaffolds, and (3) in-vivo repopulation by circulating endogenous
cells of implanted substrates without prior in-vitro cell seeding.
Advantages of an engineered tissue heart valve would likely include
nonthrombogenicity, infection resistance, and cellular viability.
Goal of engineering tissue heart valves:
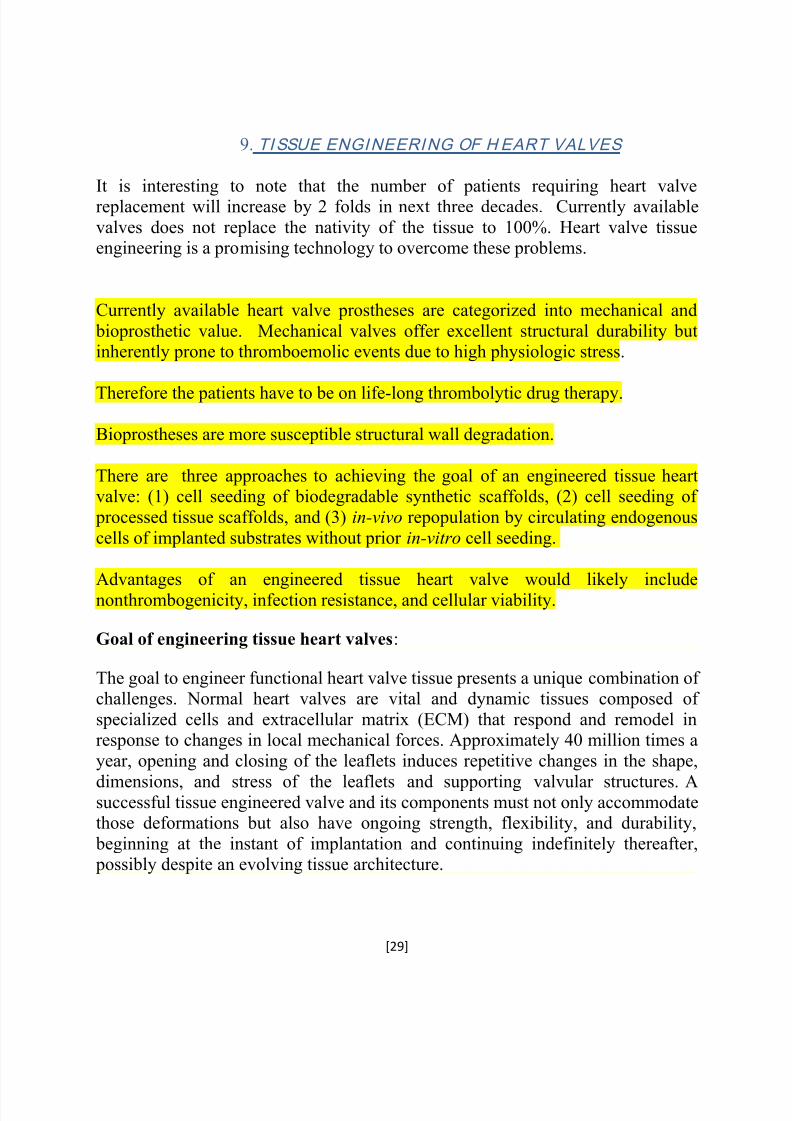
The goal to engineer functional heart valve tissue presents a unique combination of challenges. Normal heart valves are vital and dynamic tissues composed of
specialized cells and extracellular matrix (ECM) that respond and remodel inresponse to changes in local mechanical forces. Approximately 40 million times a
year, opening and closing of the leaflets induces repetitive changes in the shape,
dimensions, and stress of the leaflets and supporting valvular structures. Asuccessful tissue engineered valve and its components must not only accommodatethose deformations but also have ongoing strength, flexibility, and durability,
beginning at the instant of implantation and continuing indefinitely thereafter, possibly despite an evolving tissue architecture.
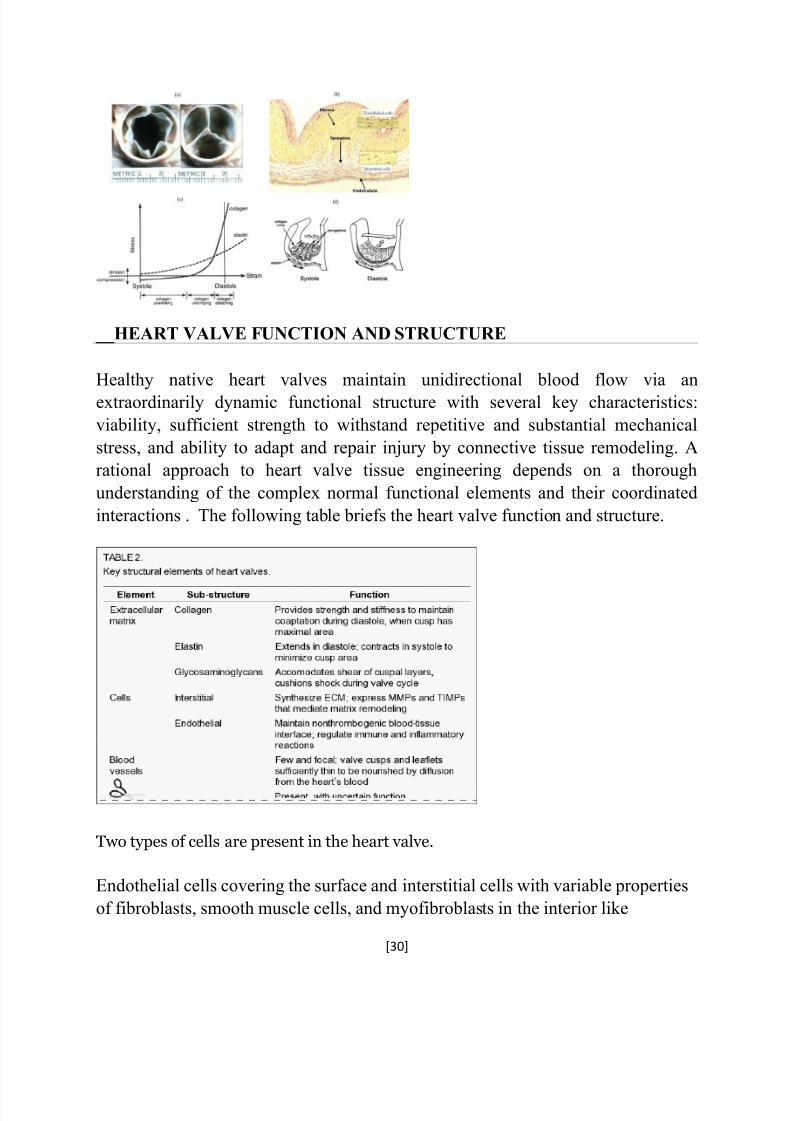
endothelial cells elsewhere in the circulation, valvular endothelial cells (VEC)
maintain a nonthrombogenic blood-tissue interface and regulate immune and
inflammatory reactions. VEC, the most numerous valvular cell type, synthesize
ECM and express matrix degrading enzymes, metalloproteinases (MMPs), and
their inhibitors (TIMPs) that mediate matrix remodeling.
CLINICAL STUDIES USING ENGINEERED MATRICES AS HEART
VALVES
One study used a decellularized pulmonary allograft seeded with autologous
endothelial cells and conditioned in bioreactor to reconstruct the right ventricular
outflow tract of adults undergoing the Ross procedure. According to the
investigators, based on a one-year follow-up, seeded endothelial cells remained on
the construct and were fully functional and the construct mechanical strength wasmaintained. There was no calcification and/or thrombogenesis. However, whether the seeded cells contributed to valve function is yet uncertain.
Despite promising results in animal experiments using decellularized xenograft
scaffolds, translation to humans has been difficult. Clinical applications of
implanted decellularized xenograft tissue heart valves have been largelyunsuccessful. Histological examination of decellularized porcine aortic SynerGraft
valves (Cryolife Inc.) implanted for 6 months in sheep without in-vitro preseeding
suggested some growth of host cells on intact leaflets and showed a lack of calcification.
The decellularized valves were not seeded or conditioned in a bioreactor before
implant with the hope that the unseeded scaffold could attract endogenous cells.These valves had a high rate of failure; examination of failed valves revealed
incomplete initial decellularization, lack of cell repopularization, lack of endothelialization, severe inflammation, fibrous sheath formation, calcification and
severe degeneration of both leaflets and wall.
Challenges for the futuristic clinical applications:
Heart valve tissue engineering has exciting potential but many unanswered
questions and challenges remain before human implantation can be considered. Asuccessful tissue engineered valve must be vital, complex, dynamic, composed of
10. ROLE OF NANOTECHNOLOGY IN CARDIOVASCULAR TISSUE
ENGINEERING.
The basic strategy of the tissue engineering is the construction of a biocompatible
scaffold to replace, re-generates or repairs damaged cells or tissues. In cardiactissue engineering, the ideal scaffold should mimic the structure of the extracellular
matrix (ECM), which is very important for the proliferation and differentiation of the seeding cells. So, to seek the bionic myocardial extracellular matrix material in
the myocardial tissue engineering for the cultured myocardial cells is a key factor for the translation from the tissue engineering into clinical practice. Now the
common used scaffold materials include traditional scaffold material, nanometer
scaffold material, and composited scaffold material. The nano-scaffolds have manyunique advantages in the field of cardiac tissue engineering.
Traditional scaffold materials
The scaffold materials which serve as temporary 3D substrates, provide a proper
microenvironment for seeding cells, and they have been shown to actively regulate
cellular responses including attachment, proliferation,differentiation and matrixdeposition [3-5]. The ECM-mimicking microenvironment is the place of getting
nutrition, waste excretion, gas exchange and metabolism for seeding cells.
Biological scaffold materials
Biological scaffold materials include fibrin, collagen, hyaluronic acid and sodium
alginate and so on. These natural polymers retained the normal grid structure,and they have a good biocompatibility, and they are beneficial to cell adhesion,
proliferation and differentiation. The biological material is widespread, andthe price is relatively cheap. Base on the advantages of good biocompatibility and
cheap price, the biological material became one of the earliest applications
of the scaffold materials in cardiac tissue engineering. In the laboratory, with
collagen as the basis researchers have fabricated the three-dimensional myocardialmodel which contains a variety of extracellular matrix proteins and growth factors
successfully, and by using of the model, they cultivate regeneration myocardial
cells which show good differentiation like the normal myocardial cells in vivoenvironment.
Synthetic material:
Synthetic materials include polyesters§elastomers and so on. The polyesters such
as polylactic acid (PLA) and polyglycolic acid (PGA) are common used for myocardial tissue engineering. The reasons why they are popular are mostly
depended on the good biocompatible of their degradation products, their
mechanical properties and simple to manufacture.
Nano-scaffolds:
Nanotechnology is defined by the size of a material (generally 1-100 nm) or
manipulation on the molecular level, and the 3 D space of the nano-scaffold should be at least one dimensional in nanometer level. The electrospinning process
produced polymer fibers in the nanometer range with an approximate diameter of 100 nm.
The nanoscaffold has a better specific effect of bulk and surface advantages, which
is much superior than millimeter and micrometer scaffold materials. The collagenfibers with diameters in the nanometer and submicron range are the major
component of the ECM, so fabricating the nanoscaled scaffold becomes the
pursuits of the researchers. While some studies have found that the smallest fibers(near 100 nm) produced by electrospining are superior. Others have concludedthat slightly larger, submicron fibers (near 400 nm) offer the best performance.
In contrast with traditional scaffold materials, thee 3-D nanofibrous scaffolds
provide a superior microenvironment for promoting cell functions. Since
nanofibrous scaffolds have nanometer pore sizes, cells are unable to penetrate bythemselves, so the seeding cells must be incorporated into the scaffold during
fabrication to ensure proper cell distribution.
Technologies for generating nanofibrous biomaterials
At present there is several major technologies for fabricating nanofibrous
biomaterials, including phase separation, self-assembly, electrospinning and so on.Phase separation techniques have been used to prepare porous polymer membranes
for purification and separation purposes. In laboratory, researchers havegenerated Nano fibrous structures by manipulating the phase separation process.
Nanocomposites in cardiac tissue engineering
Recently, the function of nanocomposites in cardiac tissue engineering causes a hotdiscussion among the researchers. The key limitation of porous matrix used for cardiac tissue engineering is that their pore walls limit the interaction of cells, and
delay electrical signal propagation. The 3D nanocomposites of gold nanowireswithin macroporous alginate scaffolds have been developed to bridge the non-
conducting pore walls, and this can increase electrical signal propagation