Nanomedicine: Nanotechnology, Biology, and Medicinexx (2013) xxx–xxx
nanomedjournal.com
Design and development of nanocomposite scaffolds forauricular reconstruction
Leila Nayyer, PhDa, Martin Birchall, MD, FRCS, FMed Scib,c,Alexander M. Seifalian, PhDa,d,⁎, Gavin Jell, PhDa
aCentre for Nanotechnology & Regenerative Medicine, UCL Division of Surgery & Interventional Science, University College London, London, UKbUCL Ear Institute, University College London, London, UK
cRoyal National Throat Nose and Ear Hospital, University College London, London, UKdDepartment of Plastic and Reconstructive Surgery, Royal Free London NHS Foundation Trust Hospital, London, UK
Ear deformity can have a significant psychological impact. Itcan occur as a result of trauma (67,000 patients have eardeformities caused by burns/year in the US),1 cancer (malignantlesion of the ear account for approximately 13% of all head andneck melanomas)2 or congenital abnormalities such as microtiaand anotia (undeveloped and absence of pinna respectively, 2 per10,000 live births in the EU).3,4 The gold standard for totalauricular reconstruction is a lengthy (up to 9 h) two-stagereconstruction procedure using sculpted autologous costalcartilage and re-arrangement of the soft tissue with complexflaps and skin grafts for coverage.5 This approach has many
The authors have no financial interests to declare in relation to thecontent of this paper. No outside funding was received.
⁎Corresponding author: UCL Division of Surgery & InterventionalScience, University College London, London, UK.
Please cite this article as: Nayyer L., et al., Design and development of nanocoxx:1-12, http://dx.doi.org/10.1016/j.nano.2013.06.006
complications including cartilage donor site sequelae such asscarring, and possible complications such as infection, pain andbleeding. Acquisition of the surgical techniques required toobtain aesthetically excellent results is a long and specializedprocess, so this skill set is not common even in plastic andreconstructive surgery.6–8
The use of synthetic biomaterials offers a number ofadvantages for auricular reconstruction. They may be personal-ized or mass produced in predetermined shapes and sizes,making “off-the-shelf” products possible. There is little or nodonor site morbidity, and a shortened operating time andimplantation would be open to many more surgeons and centers.Synthetic materials such as silicone, and porous polyethylenehave been used for auricular reconstruction. At present, non-biodegradable porous high-density polyethylene (HDPE: Med-por®; Porex Surgical, Newnan, GA, USA) is the most popularsynthetic material because of its stability, non-toxicity andplasticity. However extrusion and infection lead to failure ratesof 14.8%.9
mposite scaffolds for auricular reconstruction. Nanomedicine: NBM 2013;
2 L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
Material elastic modulus mismatch with the native tissue,inadequate cellular adhesion and delayed fibrovascular ingrowthinto the porous implant may all contribute to failure rates.10 Thedevelopment of new implantable biomaterial for auricularreconstruction more closely matching the mechanical propertiesof human ears and promoting desirable cellular interactions mayincrease biomaterial–tissue integration and thereby preventmicro-movement and extrusion.
Recent advances in the field of material science andnanotechnology have allowed the development of biomaterialswith controllable mechanical and surface properties, allowingbiomaterials to more closely mimic human tissues. The use ofnanotechnology, particularly the use of nanoparticles incorporatedinto 3D polymer matrixes, may enable even greater control oversurface properties and consequently protein adsorption and tissueformation.11 Ideal biomaterial scaffolds for auricular reconstruc-tion should have structural stability, match the mechanicalproperties of the native tissue and have porosity to enablevascularization and host tissue integration.12 Substrate stiffnessalso affects cellular behavior, including migration, growth anddifferentiation, through various mechanotransductive processes.13
We described the development of a non-biodegradablenanocomposite scaffold based on incorporating polyhedraloligomeric silsesquioxane (POSS) nanocage into polycarbon-ate-based urea–urethane (PCU, UCL-Nano™).14,15 Tissuesand organs composed of POSS-PCU have been successfullyused in first-in-human applications for replacement of coronaryarteries, lacrimal ducts, and the world's first synthetictrachea.16–18 We hypothesize that this material could also besuitable for auricular reconstruction. As opposed to morecomplicated and costly tissue engineering approaches involvingcondrocytic production of ECM to provide suitable mechanicalproperties, our simple approach is to create a biomaterial thatalready matches the mechanical properties of the ear cartilage.In this approach fibrotic cell integration and preventingmodular mismatch between the dermis tissue and the implantare the primary concerns to preventing extrusion rates. Theaims of this study were to design and manufacture ear-shapedconstructs based on POSS-PCU using two fabrication process-es solvent evaporation/porogen leaching (POSS-PCUs) andphase-separation (coagulation)/porogen leaching (POSS-PCUc), to evaluate the physiochemical properties of thesecandidate materials to Medpor®, and third, to evaluate thebiological activity of these scaffolds in terms of effects onproliferation, morphology, collagen production and migrationof applied fibroblasts.
Materials and methods
Nanocomposite polymer synthesis
POSS-PCU nanocomposite polymer was synthesised asdescribed previously. 15 Briefly, polycarbonate polyol,2000mwt and trans-cyclohexanechloroydrinisobutyl-silses-quioxane (Hybrid Plastics Inc) were placed in a 500-ml reactionflask equipped with mechanical stirrer and nitrogen inlet. Themixture was heated in order to dissolve the POSS cage into thepolyol and then cooled to 70 °C. Flake 4,4′-methylenebis(phenyl
isocyanate) (MDI) was added to the polyol blend and thenreacted, under nitrogen, at 75 °C–85 °C for 90 min to form apre-polymer. Dimethylacetamide (DMAC) was added slowly tothe pre-polymer to form a solution; the solution was cooled to40 °C. Chain extension of the pre-polymer was carried out by thedropwise addition of a mixture of ethylenediamine anddiethylamine in DMAC to form a solution of POSS-modifiedpolycarbonate urea–urethane in DMAC. Micro thin sheets microthin Medpor® sheets medical grade high-density porouspolyethylene (HDPE) (Porex Surgical, Newnan, GA, USA)were used as comparison.
Ear mould design
A custom-made ear-shaped 3D negative glass mould(Glossary Co., UK) was fabricated from positive 3D printingof a 3D scan obtained from the external part of the human ear,and used to manufacture a polymeric POSS-PCU auricle ofappropriate size and morphology (Figure 1, A-B). The 3Dprinting or additive layer manufacturing (ALM) of auricleframework was created by a ZPrinter® system (3D SystemsCorporation, USA) based on powder bed and inkjet 3D printingtechniques. ALM software was used to slice the 3D computermodel (standard triangulate language [STL] files format) intothinner horizontal layers of powder which is solidified by abinder. The 3D printing auricle was then fabricated layer bylayer via rapid tooling (RT) process from computer sliced data toprint the mould for the ear model (Figure 1, C). The 3D negativeglass mould was then created from the 3D printing ear modeland acted as a rigid cast for shaping and discharging of twodifferent polymeric auricle POSS-PCU nanocomposites pro-cessed by solvent evaporation/porogen leaching (POSS-PCUS)and phase-separation (coagulation)/porogen leaching (POSS-PCUC; Figure 1, D-E).
Fabrication of scaffold
POSS-PCU auricular nanocomposite scaffolds were fabricat-ed by combining porogen leaching with either solvent casting orcoagulation techniques. In all procedures, sodium chloride(NaCl) was dissolved in an 18 wt% solution of POSS-PCU inDMAC containing Tween-20 surfactant. Prior to this, theporogen particles were sieved using stainless steel sieves (FisherScientific) in order to achieve an average particle size of 140-150 μm. The viscous slurry of NaCl/POSS-PCU was producedby dispersing and degassing of the mixture using a Thinky AER250 mixer (Intertonics, Kidlington, UK). The weight ratio ofNaCl to POSS-PCU was controlled to 3:7.
In the solvent evaporation/porogen leaching POSS-PCUS
method, the negative mould was coated with a layer of the NaCl/POSS-PCU slurry and left in the air-circulating oven at 65 °C for4–5 h until all the solvent evaporated. This procedure wasrepeated four times until the polymer was adequate thickness.The ear construct was then carefully removed from the glassmould and submerged in deionized water to dissolve out theporogen to form the porous polymeric scaffold. The constructwas continuously washed with frequent water changes, usingpure deionized water, for a period of 72 h to ensure the completeremoval of NaCl. In the phase-separation (coagulation)/porogen
Figure 1. Auricular design and manufacturing. Human-sized glass mould design using a 3D printing ear as positive mould that created based on 3D scan data to fabricate a porous auricular scaffold made from POSS-PCU. 3D scan image of the external part of a human ear model (A) and negative glass mould fabricated (B) from positive 3D printing auricle mould (C) using additive layer manufacturing (ALM) based on powderbed and inkjet 3D printing. Porous polymeric auricular POSS-PCU NC scaffold produced by solvent evaporation/porogen leaching (POSS-PCUS) (D) and by phase-separation (coagulation)/porogen leaching(POSS-PCUC) techniques (E).
3L.Nayyer
etal
/Nanom
edicine:Nanotechnology,
Biology,
andMedicine
xx(2013)
xxx–xxx
4 L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
leaching (POSS-PCUC) method the slurry mixture was,however, cast onto the mould and immediately immersed indeionized water for an initial period of 24 h. This processresulted in the formation of a coagulated porous auricularscaffold via DMAC exchange with deionized water and leachingof NaCl. The construct was continuously washed with frequentwater changes, using pure deionized water, for a period of 72 hto ensure the complete removal of NaCl and DMAC. Thephysicochemical properties of the auricular scaffolds werethen characterized.
Scaffold sheets of dimensions 8 × 8 cm, with a thicknessof 700-800 μm were also fabricated by POSS-PCUS andPOSS-PCUC procedures using stainless steel plates similarto the preparation methods described above. The poroussheets of polymer were then cut into 16-mm diameter disksfor use in 24-well plates and autoclaved for all cell cultureexperiments.
Auricular nanocomposite scaffold characterization
Scanning electron microscopy (SEM)Surface and cross sections of the POSS-PCU NC samples
(n = 4) were evaluated under scanning electron microscopy(SEM) to assess pore size, shape and distribution. Briefly, thesample was post-fixed using 1% osmium tetroxide (Merck, UK),washed with distilled water and dehydrated at room temperaturein a series of acetone solutions. Following dehydration, thesample was transferred to tetramethylsilane for 5 min and thenallowed to air dry. The sample was attached to aluminium stubswith double-sided sticky tabs (TAAB Laboratories Equipment,UK) and coated with gold using a sputter coater (SC500EMScope) prior to SEM examination (Philips 501, Eindhoven,the Netherlands). The samples were observed at ×10, ×80, and×160 magnifications at 25 kV. Average pore size data wereobtained using ImageTool software on three 25 × 104-μm2
surface areas (×80 magnification) for each of the preparedsamples (n = 4).
The open-pore structure of Medpor® meant that it wasimpossible to measure discrete pore sizes, using this methodol-ogy. The manufacture's data were therefore used as comparisonwith a stated pore size of N100 μm.
Porosity measurementThe porosity of the micro-porous POSS-PCU samples
(n = 4) was calculated using the formula described in Eqs. 1and 2 below.19 The thickness and dimensions of the sampleswere measured to obtain the volume of the scaffold and thenweighed. The mass of the scaffold was divided by thevolume of the scaffold to obtain the apparent density usingEq. 1.
Apparent density g=cm3� � ¼ scaffold mass gð Þ
scaffold volume cm3ð Þ ð1Þ
The bulk density of scaffold was eventually divided by theapparent density of the non-porous pure POSS-PCU polymer(p = 1.15 g/cm3) to obtain the porosity using Eq. 2 below.The porosity is expressed as a percentage. The manufacture's
data for the porosity of Medpor® were 50% and this was usedas a comparison.
Porosity %ð Þ¼ 1−
scaffold apparent density g=cm3ð ÞPOSS−PCU polymer density g=cm3ð Þ
of POSS-PCU scaffolds, Medpor® and human auricular cartilagesamples (n = 6) were characterized using an Instron-5565 tensiletester. This was under uniaxial tension with dog bone-shapedsamples of dimension 20 × 4 mm, with loading speed of50 mm/min. Each sample had its mean thickness calculated byan electronic micrometer. Data such as maximum tensilestrength, elongation at break and Young's modulus werecollected with a stretching ratio of 0% to 25%. The Young'smodulus of Medpor® sample was obtained from an elongation ofless than 2.5%, due to sample fracture above this elongation %(because of the stiffer/less elastic nature of Medpor®).
Contact angle measurementsThe hydrophilicity/hydrophobicity of the hydrated POSS-
PCU NC and Medpor® surfaces, which are highly porous, wasexamined through captive bubble contact angle measurementsusing a DSA100 instrument (KRÜSS, Germany), in conjunctionwith axisymmetric drop shape analysis profile (ADSA-P) indistilled water. A curved needle was placed directly beneath thecenter of the sample surface in a water chamber from which anair bubble was dispensed. Measurements were taken on threefurther occasions for each of the prepared surfaces (n = 4). Atthis point, the angle the bubble made upon contact with thepolymer was measured using a circular algorithm technique,implemented in the KRÜSS drop shape analysis software.Values N90°θ are considered hydrophilic, and values b90°θ areconsidered hydrophobic in captive bubble technique.
Atomic force microscopy (AFM)The POSS-PCU NC and Medpor® surface topography were
examined using an atomic force microscope (Bruker Dimension3100) operating in contact mode. The samples were placed on ametallic disk and magnetically mounted in the AFM chamber.Measurements were taken on three further occasions for each ofthe prepared surfaces (n = 4). Surface images for quantitativeanalysis were obtained from 15 × 15-μm scans at a scan rate of1 Hz. The root mean square surface roughness (Rq) values werecalculated from the scans using the NanoScope® analysissoftware (Bruker Corporation) version 1.40.
Biological activity evaluation on auricularnanocomposite scaffold
Fibroblast cultureMouse fibroblast cells (3 T3 cell line, European Collection of
Cell Culture, UK) were cultured in Dulbecco's modified Eagle’smedium (DMEM) supplemented with 10% foetal bovine serum(FBS) and 1% antibiotic (50 μg/ml streptomycin, 50 U/mlpenicillin) solutions (all from Invitrogen, UK) and incubated at37 °C. The 16-mm polymer disks were autoclaved and washed
5L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
in sterile phosphate-buffered saline (PBS). Each polymer disk(n = 4) was seeded with cells at a density of 4 × 104 cells/cm2 in1 ml of cell culture medium. Wells containing tissue cultureplastic (TCP) without test polymer were used as positivecontrols. Media were replaced every 2 days. Cell proliferationand matrix deposition were measured on days 2, 6 and 10 asdescribed below. On days 10 and 14, fibroblast morphologyand migration were also determined by SEM and histologyanalysis, respectively.
Fibroblast proliferationThe metabolic activity of cultured fibroblasts was monitored
using the tetrazole MTT (3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (Sigma, UK), as previouslydescribed.20 Briefly, 50 ml of a 5-mg/ml solution of MTT inphosphate-buffered saline (PBS) was added to the culture mediaof the cell-seeded polymer disks 3 h prior to the end of cellculture (2, 6, and 10 days). Formazan was solubilized in DMSO(dimethyl sulfoxide; Sigma, UK) and the absorbance read on acolorimetric plate reader (Anthos 2020 microplate reader,Biochrome Ltd, UK) at 592 nm.
Extracellular collagen productionThe amount of extracellular secreted collagen from fibro-
blasts was measured using the Picrosirius Red method aspreviously described.21 Briefly, the supernatant (100 μl) (n = 4)was dispensed into 96-well plates and incubated at 37 °C for 16-24 h until dry. After rinsing three times per well with distilledwater (200 μl), 100 μl of 0.2% (wt/vol) Sirius Red (Sigma) insaturated picric acid was placed in each well for 30 min at roomtemperature. The plates were washed with 200 μl of 0.5%NaOH. The absorbance eluted stain was measured at 540 nm in amicroplate reader (Anthos 2020 microplate reader, BiochromeLtd) and the amount of soluble collagen estimated.
Fibroblast morphology via scanning electronmicroscopy (SEM)
Following 10 days cell culture, cell-seeded polymer disks(n = 4) were harvested, washed with PBS (×2) and fixed with1.5% glutaraldehyde for 2 h at 4 °C. Following three rinses withdistilled water, the samples were dehydrated through a series ofgraded ethanol solutions and then freeze-dried. Dry constructswere sputter coated with gold and observed by SEM at ×80 and×640 magnifications (Philips 501).
Fibroblast ingrowth via histological analysisThe migration of cultured fibroblasts within the scaffolds
was determined using histology. Following 14-day cell culture,cell-seeded polymer disks (n = 4) were harvested, washed withPBS (×2) and fixed with 10% neutral-buffered formalin (NBF)(Sigma Aldrich) for 24 h at 4 °C. Following dehydrationthrough a series of graded ethanol solutions, the samples wereparaffin embedded and horizontally cross sectioned (2-4 μm);sections from the middle area (~depth 250 μm from top) wereanalyzed with hematoxylin and eosin (H&E) staining. Thestained samples were observed by stereoscope microscopyimaging system (Nikon, SMZ 1500) fixed with a digital camera(INFINITY2-1C) at ×20 magnification. Average cell countingdata were obtained on three 24 × 104 μm2 field of view areas
(×20 magnification) for each of the prepared slice samples(n = 4).
Statistical analysis
All quantitative data are presented as means ± standarddeviation (SD). The differences between samples duringrepeated-measures testing was calculated by one-way analysisof variance (ANOVA) using Tukey's post hoc test withsignificance accepted at the 5% level using IBM® SPSS®Statistics version 20.
Results
Preparation of auricular nanocomposite scaffolds
The glass mould system allowed the manufacture ofcustomized auricular scaffold with a POSS-PCU nanocompositepolymer (using POSS-PCUS and POSS-PCUC fabricationtechniques). This reproduces the anti-helix, helix, and otherkey structural features (Figure 1,D-E). The POSS-PCUc scaffoldwas considerably easier to remove from the glass mouldcompared to that made from POSS-PCUs.
Physicochemical characterization of auricularnanocomposite scaffolds
Pore sizeThe scaffold made using POSS-PCUC contained a less open
macro-pores on the surface compared with that made fromPOSS-PCUS (Figure 2). The cross-section SEM image of bothscaffolds revealed a heterogeneous porous structure (Figure 2).The average pore sizes of POSS-PCUS and POSS-PCUC
scaffolds were 142.13 ± 15.36 μm and 151.85 ± 17.39 μm,respectively, and related to the leachable NaHCO3 particle size(Table 1). No significant differences in the internal pore sizeswere noted between scaffolds prepared via different fabricationmethods. There were, however, considerable differences in the“open”-pore structure of Medpor® compared with less “open”-nanocomposite-pore structure (Figure 2).
PorosityPOSS-PCUC scaffolds were significantly more porous than
those made from POSS-PCUS (85.21% ± 1.19% vs. 63.47% ±1.35%, P b 0.001). Porosity correlated with decreasing scaffolddensity (Pearson's rank correlation) as expected (Table 1).
Mechanical analysisThe maximum tensile strength of POSS-PCUS polymer was
higher than that of POSS-PCUC (7.48 ± 0.43 MPa versus0.88 ± 0.22 MPa: P b 0.001), but not significantly differentfrom that of Medpor® (6.16 ± 0.20 MPa). Human auricularcartilage was significantly less than all three test scaffolds(2.02 ± 0.25 MPa) (P b 0.001; Table 2). The percentage elon-gations at breaking points of both polymers were significantlyhigher compared to human auricular cartilage (40.62% ± 28%)and Medpor® (4.40% ± 11%). However, POSS-PCUS exhibiteda tensile strain of 417.08% ± 26%, which was significantly(P b 0.01) higher than POSS-PCUc (273.74% ± 27%). Med-por® had a significantly greater Young's modulus compared to
Figure 2. Auricular scaffold microstructure. Scanning electron microscopy (SEM) images of the cross-sectional and surface of POSS-PCU nanocomposites andMedpor®. Note that in POSS-PCUc a surface film forms with much reduced porosity (white arrows).
Table 1Physicochemical properties of POSS-PCU auricular nanocomposites compared to Medpor®.
Rq indicates mean root square roughness; values are mean ± SD, (n = 4).a Data obtained from the manufacturer.
6 L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
POSS-PCUS, POSS-PCUC and native auricular cartilage(140.9 ± 0.04 versus 5.73 ± 0.17, 0.58 ± 0.12, and 5.02 ±0.04 MPa) respectively; P b 0.001: Table 2). On univariateanalysis, POSS-PCUC Young's modulus was significantly lowerthan the others, while there was no significant difference betweenPOSS-PCUS and native auricular cartilage (Table 2).
Contact angle measurementsThe surfaces of POSS-PCUS, POSS-PCUC and Medpor®
scaffolds had significantly different average captive bubble
contact angle of 53.24° ± 0.13°, 48.73° ± 0.06° and 45.67° ±0.26°, respectively (Table 1, P b 0.05).
Atomic force microscopy (AFM)POSS-incorporated PCU polymer induced a relatively high
density of nanoscale structural features compared to Medpor®surfaces that had a relatively smooth microscale (Figure 3).POSS-PCUs showed an average roughness of 82.2 ± 11.8 nmover a 225-μm2 area, while POSS-PCUc was significantlyrougher (Rq = 214.3 ± 12.2 nm, P b 0.001). However,
Table 2Mechanical properties of POSS-PCU auricular nanocomposites compared to Medpor® and human auricular cartilage.
Values are mean ± SD, (n = 6).a Elastic modulus has been reported to vary between 227 and 307 MPa.43
7L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
Medpor® displayed an average microscale roughness of119.0 ± 13.8 nm, which was significantly (P b 0.001) higherthan POSS-PCUs and less than POSS-PCUc (Table 1).
Fibroblast proliferationProliferation and metabolic activity of fibroblasts seeded on
both POSS-PCU polymers, Medpor® and TCP increased withincreasing cell culture period (Figure 4, A). Compared withTCP, all scaffold samples showed a significant reduction(P b 0.001) in metabolic activity of seeded cells at all timepoints. No significant differences in metabolic activity wereobserved between nanocomposite scaffolds.
Extracellular collagen releaseCollagen staining quantification demonstrated that the
fibroblasts seeded on all samples produced a significantlyincreased level of soluble collagen over the course of 6 days,followed by a small and non-significant increase after day 10(Figure 4, B). TCP had a significant reduction (P b 0.001) incollagen production after 6 days of culture, compared to allscaffolds. No significant differences in collagen production wereobserved between the two forms of POSS-PCU. Howevercompared to Medpor®, cells seeded on POSS-PCUS produced asignificantly increased (P b 0.05) amount of collagen at 6 and10 days. The amount of collagen production per metabolic activeunit was also significantly higher for POSS-PCUs compared toPOSS-PCUc (Figure 4, C). SEM images also showed whatappeared to be an increase in extracellular matrix (ECM)production on POSS-PCUS scaffold (Figure 5).
Fibroblast morphologyFibroblasts adhered to both POSS-PCU scaffolds as well as to
Medpor® (Figure 5). However, a higher number of cellaggregates with rounded morphologies were observed forPOSS-PCUc when compared to POSS-PCUs and Medpor®(Figure 5). The ECM secreted by the cells on both POSS-PCUnanocomposites and Medpor® seemed to occlude the pores,especially on the former. On Medpor®, pseudopodia spanned thepores (1-2 μm).
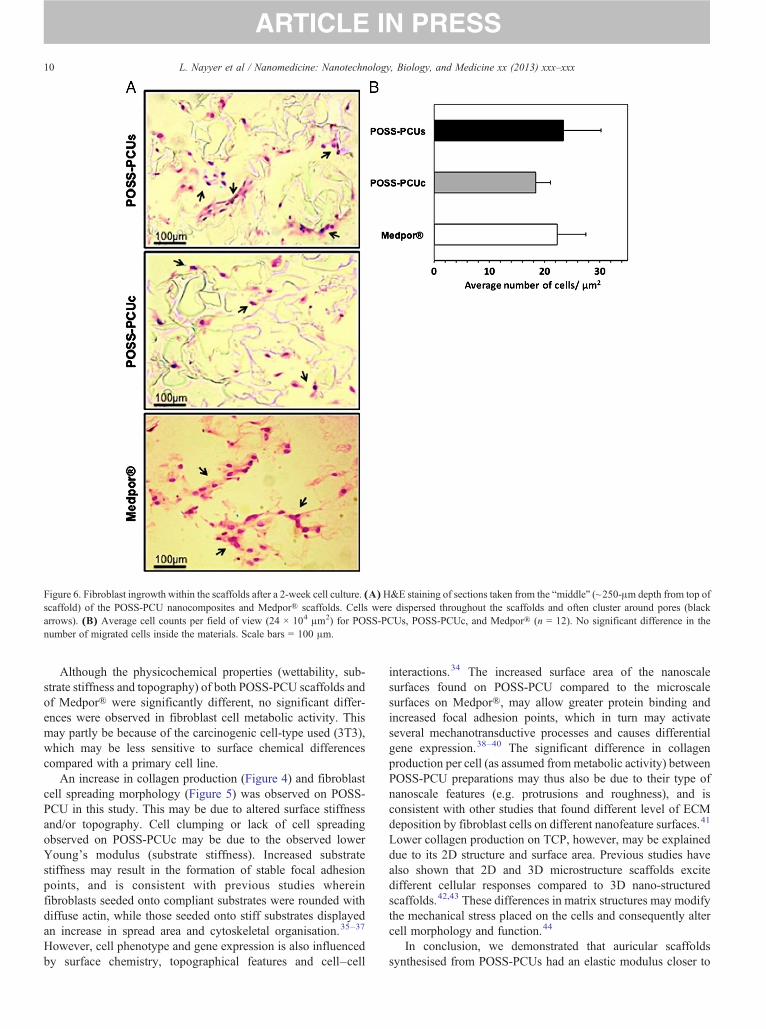
Fibroblast ingrowthHistological analysis of the “middle” sections of the scaffolds
after a 2-week cell culture revealed that fibroblasts migrated tothe center of all the scaffolds, secreting a thin extracellularnetwork into and surrounds the interpore spaces. Cells wereelongated and spindle shaped (Figure 6, A). No significantdifferences in number of fibroblasts migration were observedbetween scaffold cross-sectional surfaces (Figure 6, B).
Discussion
Nanocomposite (POSS-PCU, UCL-Nano™) scaffolds forauricular reconstruction, were successfully created using twodifferent fabrication methods: solvent evaporation/porogenleaching and phase-separation (coagulation)/porogen leaching.The physicochemical and in vitro interactions of these novelconstructs were compared with those of Medpor®, the current“gold standard” synthetic material for auricular reconstruction.
POSS-PCU fabrication methods produced two types ofauricle-shaped construct with similar average pore sizes butdifferent porosities. POSS-PCUS produced a denser foamscaffold, with a reduced total porosity and more open-macroporestructure on the material surface compared to POSS-PCUC
(Figure 2). These differences may be due to the mechanism ofDimethylacetamide (DMAC) removal from the scaffold, namelyevaporation compared with water dissolution/dispersion inPOSS-PCUc synthesis. DMAC removal by evaporation doesnot cause pore formation and porosity is solely determined byporogen leaching in water, while in phase separation, DMACdissolution and porogen leaching both contribute to poreformation. Therefore, there is less control of porosity in thephase-separation (“coagulation,” “c”) method. Coagulation mayalso be responsible for the less porous “skin” that forms on thetopmost surface of the material due to the increased rate ofDMAC–water demixing,22 Ways to reduce “skin” formation arebeing explored by our group, including the dispersion or“sprinkling” of porogen particles on the surface of the polymer.
Scaffold porosity is important for angiogenesis and fibroustissue ingrowth, which may both play a vital role in implantstabilisation, as previously shown in a comparison of Medpor®with a non-porous silicone implants.23,24 It has been suggestedthat an interconnective pore size of greater than 100 μm isrequired to accommodate a hierarchical vascular network withina biomaterial (taking into the diameter of a capillary and thesurrounding perivascular associated cells).25–27 Conversely,high porosity will decrease biomechanical strength and soachieving the right balance is critical in the development of newimplant materials. Under a given molecular weight (MW) ofpolymer and content of porogen, the strength and modules ofPOSS-PCUs scaffolds fabricated with solvent evaporation werehigher than those of the POSS-PCUc scaffolds fabricated withthe phase-separation approach. Owing to solvent dissolution andporogen leaching in POSS-PCUc, more microvoids in the matrixof macropores act as material defects and contribute unfavorablyto the mechanical properties. As expected the modulus of the
Figure 4. Fibroblast interaction with auricular scaffold materials. Metabolicactivity (A), total collagen content (B), and concentration of collagen productionper metabolic active unit (C) after 2, 6 and 10 days of fibroblasts culture onPOSS-PCUs (white; n = 4) and POSS-PCUc (gray; n = 4), Medpor® (darkgray, n = 4) and tissue culture plastic (TCP, black; n = 4) surfaces. (A) Nosignificant difference in the rate of cell metabolism was observed between thematerials. (B,C)A significant increase in total collagen production and collagenproduction permetabolic unit was observed on fibroblasts grown on POSS-PCUscompared with Medpor® on day 6 and 10. (C) POSS-PCUs also presentedsignificantly a higher level of collagen production per metabolic active unit whencompared to the POSS-PCUcNC after 6 and 10 days. (A,B)Themeasurementsare relative to day 2 TCP (%). *P b 0.001 and **P b 0.05, errors bar = SD.
Figure 3. Atomic force microscopy images of auricular scaffold materials.Incorporating POSS nanoparticles into polymer matrix (PCU) resulted insurface with nanotopography features on both nanocomposite materialscompared with the microscale features of Medpor®. The root mean squareaverage surface roughness (Rq) values are presented in Table 1.
8 L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
POSS-PCU scaffold decreased with increasing porosity and withdecreasing relative density, which agrees with power-low theorybetween mechanical parameters and relative density.28,29
POSS-PCU fabricated using solvent evaporation had anincreased tensile strength compared to coagulation synthesis,due to the greater density and reduced porosity of POSS-PCUs.The POSS-PCUS scaffold had an elastic modulus of 5.73 MPa,similar to that of human elastic cartilage (5.02 ± 0.17 MPa),
Figure 5. SEM micrograph images of fibroblast morphology after a 10-day culture on polymer scaffolds. Increased fibroblast spreading and confluency wasobserved on the POSS-PCUs NC compared to POSS-PCUc (had a rounder morphology) and Medpor®, where an increased number of cell aggregations (whitearrow) were observed.
9L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
and was considerably more flexible compared with Medpor®.Matching the mechanical properties of native tissue is importantconsideration of biomaterial design and failure to do so maycontribute to increased infection and extrusion rates in vivo.Elastic modulus mismatch of Medpor® with native tissue hasbeen previously suggested as the cause of seroma formationand partial or total extrusion of implanted frameworks within arabbit model, despite significant fibrovascular invasion.30 Localstress concentrations at the skin–implant interface (due to thedifferential loading tissue environment) may result in micro-movement, the detachment of biomaterial–cell/protein bindingsites and in turn increase the opportunity for infection andconsequently implant extrusion.31 Therefore, the close elasticmodulus match of POSS-PCUs to the native ear may enable themechanical load to be shared across the tissue interface in abiologically relevant manner, and thus prevent tension, micro-movement and extrusion. This theory will of course need to betested in vivo. Biomaterial designs for auricular reconstructionneed to support cell adhesion and proliferation to allow tissueingrowth, and thereby biomaterial integration. Previous studieshave shown that both Medpor® and POSS-PCU can sustain cell
attachment and proliferation.27,32 Surface properties such aschemistry, surface energy and topography are important indetermining the interaction between cells and material. BothPOSS-PCU preparations exhibited a significantly reducedhydrophobicity and had significantly different surface topogra-phies compared with Medpor®. Considering that both nano-composites were of the same chemical composition and variedonly in the manufacturing processing, the differences in thesurface roughness may account for the differences in hydro-phobicity (according to the Wenzel equation).33 POSS-PCUchad the highest surface roughness. We hypothesize that theobserved significant differences in roughness between POSS-PCUc and POSS-PCUs are related to the differences in themethod of DMAC removal (water or air interface) duringpolymer solidification rather than representing differences inthe polymer structure. Changes in material surface chemistryand topography determine protein adsorption, protein confor-mation and consequently cell behavior.34 Altering themanufacturing process of POSS-PCU is thus a simple andpotentially useful means of controlling the surface chemistryand topography.
Figure 6. Fibroblast ingrowth within the scaffolds after a 2-week cell culture. (A)H&E staining of sections taken from the “middle” (~250-μm depth from top ofscaffold) of the POSS-PCU nanocomposites and Medpor® scaffolds. Cells were dispersed throughout the scaffolds and often cluster around pores (blackarrows). (B) Average cell counts per field of view (24 × 104 μm2) for POSS-PCUs, POSS-PCUc, and Medpor® (n = 12). No significant difference in thenumber of migrated cells inside the materials. Scale bars = 100 μm.
10 L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
Although the physicochemical properties (wettability, sub-strate stiffness and topography) of both POSS-PCU scaffolds andof Medpor® were significantly different, no significant differ-ences were observed in fibroblast cell metabolic activity. Thismay partly be because of the carcinogenic cell-type used (3T3),which may be less sensitive to surface chemical differencescompared with a primary cell line.
An increase in collagen production (Figure 4) and fibroblastcell spreading morphology (Figure 5) was observed on POSS-PCU in this study. This may be due to altered surface stiffnessand/or topography. Cell clumping or lack of cell spreadingobserved on POSS-PCUc may be due to the observed lowerYoung's modulus (substrate stiffness). Increased substratestiffness may result in the formation of stable focal adhesionpoints, and is consistent with previous studies whereinfibroblasts seeded onto compliant substrates were rounded withdiffuse actin, while those seeded onto stiff substrates displayedan increase in spread area and cytoskeletal organisation.35–37
However, cell phenotype and gene expression is also influencedby surface chemistry, topographical features and cell–cell
interactions.34 The increased surface area of the nanoscalesurfaces found on POSS-PCU compared to the microscalesurfaces on Medpor®, may allow greater protein binding andincreased focal adhesion points, which in turn may activateseveral mechanotransductive processes and causes differentialgene expression.38–40 The significant difference in collagenproduction per cell (as assumed frommetabolic activity) betweenPOSS-PCU preparations may thus also be due to their type ofnanoscale features (e.g. protrusions and roughness), and isconsistent with other studies that found different level of ECMdeposition by fibroblast cells on different nanofeature surfaces.41
Lower collagen production on TCP, however, may be explaineddue to its 2D structure and surface area. Previous studies havealso shown that 2D and 3D microstructure scaffolds excitedifferent cellular responses compared to 3D nano-structuredscaffolds.42,43 These differences in matrix structures may modifythe mechanical stress placed on the cells and consequently altercell morphology and function.44
In conclusion, we demonstrated that auricular scaffoldssynthesised from POSS-PCUs had an elastic modulus closer to
11L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
that of native ear cartilage. They also maintained cell growth andincreased collagen production, compared to scaffolds made fromPOSS-PCUc and Medpor®. Therefore, POSS-PCUs can be apromising alternative biomaterial for auricular reconstruction,but further in vitro and vivo studies are required to fullycharacterize the biological suitability.
References
1. Osguthorpe JD. Head and neck burns. Evaluation and currentmanagement. Arch Otolaryngol Head Neck Surg 1991;117:969-74.
2. Cox NH, Jones SK, MacKie RM. Malignant melanoma of the head andneck in Scotland: an eight-year analysis of trends in prevalence,distribution and prognosis. Q J Med 1987;64:661-70.
3. Harris J, Kallen B, Robert E. The epidemiology of anotia and microtia.J Med Genet 1996;33:809-13.
4. Luquetti DV, Leoncini E, Mastroiacovo P. Microtia-anotia: a globalreview of prevalence rates. Birth Defects Res A Clin Mol Teratol2011;91:813-22.
5. Brent B. Technical advances in ear reconstruction with autogenous ribcartilage grafts: personal experience with 1200 cases. Plast ReconstrSurg 1999;104:319-34.
6. Kawanabe Y, Nagata S. A new method of costal cartilage harvest fortotal auricular reconstruction: part I. Avoidance and prevention ofintraoperative and postoperative complications and problems. PlastReconstr Surg 2006;117:2011-8.
7. Walton RL, Beahm EK. Auricular reconstruction for microtia: part II.Surgical techniques. Plast Reconstr Surg 2002;110:234-49.
8. Zhang Q, Zhang R, Xu F, Jin P, Cao Y. Auricular reconstruction formicrotia: personal 6-year experience based on 350 microtia earreconstructions in China. Plast Reconstr Surg 2009;123:849-58.
9. Cenzi R, Farina A, Zuccarino L, Carinci F. Clinical outcome of 285Medpor grafts used for craniofacial reconstruction. J Craniofac Surg2005;16:526-30.
11. Lavenus S, Ricquier JC, Louarn G, Layrolle P. Cell interaction withnanopatterned surface of implants.Nanomedicine (Lond) 2010;5:937-47.
12. Feng B, Jinkang Z, Zhen W, Jianxi L, Jiang C, Jian L, et al. The effectof pore size on tissue ingrowth and neovascularization in porousbioceramics of controlled architecture in vivo. Biomed Mater 2011;6:015007.
13. Discher DE, Janmey P, Wang YL. Tissue cells feel and respond to thestiffness of their substrate. Science 2005;310:1139-43.
14. Kannan RY, Salacinski HJ, Butler PE, Seifalian AM. Polyhedraloligomeric silsesquioxane nanocomposites: the next generation materialfor biomedical applications. Acc Chem Res 2005;38:879-84.
15. Kannan RY, Salacinski HJ, Odlyha M, Butler PE, Seifalian AM. Thedegradative resistance of polyhedral oligomeric silsesquioxane nanocoreintegrated polyurethanes: an in vitro study. Biomaterials 2006;27:1971-9.
16. Chaloupka K, Motwani M, Seifalian AM. Development of a newlacrimal drainage conduit using POSS nanocomposite. Biotechnol ApplBiochem 2011;58:363-70.
17. Desai M, Ahmed M, de Mel A, Tsui J, Seifalian AM, Hamilton G.Performance of a nanocomposite polymer small diameter bypass graft ina long-term sheep model. J Vasc Surg 2012;55:77-8.
18. Jungebluth P, Alici E, Baiguera S, Blanc KL, Blomberg P, Bozoky B, et al.Tracheobronchial transplantation with a stem-cell-seeded bioartificialnanocomposite: a proof-of-concept study. Lancet 2011;378:1997-2004.
19. He W, Ma Z, Yong T, Teo WE, Ramakrishna S. Fabrication of collagen-coated biodegradable polymer nanofiber mesh and its potential forendothelial cells growth. Biomaterials 2005;26:7606-15.
20. Gentleman E, Fredholm YC, Jell G, Lotfibakhshaiesh N, O'DonnellMD, Hill RG, et al. The effects of strontium-substituted bioactiveglasses on osteoblasts and osteoclasts in vitro. Biomaterials 2010;31:3949-56.
22. Ahmed M, Ghanbari H, Cousins BG, Hamilton G, Seifalian AM. Smallcalibre polyhedral oligomeric silsesquioxane nanocomposite cardiovas-cular grafts: influence of porosity on the structure, haemocompatibilityand mechanical properties. Acta Biomater 2011;7:3857-67.
23. Shanbhag A, Friedman HI, Augustine J, von Recum AF. Evaluation ofporous polyethylene for external ear reconstruction. Ann Plast Surg1990;24:32-9.
24. Sclafani AP, Romo III T, Silver L. Clinical and histologic behavior ofexposed porous high-density polyethylene implants. Plast Reconstr Surg1997;99:41-50.
25. Bigham WJ, Stanley P, Cahill Jr JM, Curran RW, Perry AC.Fibrovascular ingrowth in porous ocular implants: the effect of materialcomposition, porosity, growth factors, and coatings. Ophthal PlastReconstr Surg 1999;15:317-25.
26. Cheung HY, Lau KT, Lu TP, Hui D. A critical review on polymer-basedbio-engineered materials for scaffold development. Composites Part B-Engineering 2007;38:291-300.
27. Klawitter JJ, Bagwell JG, Weinstein AM, Sauer BW. An evaluation ofbone growth into porous high density polyethylene. J Biomed Mater Res1976;10:311-23.
28. Hou QP, Grijpma DW, Feijen J. Porous polymeric structures for tissueengineering prepared by a coagulation, compression moulding and saltleaching technique. Biomaterials 2003;24:1937-47.
30. Neel HB. Implants of Gore-Tex: comparison with Teflon-coatedpolytetrafluoroethylene carbon and porous polyethylene implants. ArchOtolaryngol 1983;109:427-33.
31. Murphy EF. History and philosophy of attachment of prostheses to themusculo-skeletal system and of passage through the skin with inertmaterials. J Biomed Mater Res 1973;7:275-95.
32. Punshon G, Vara DS, Sales KM, Kidane AG, Salacinski HJ,Seifalian AM. Interactions between endothelial cells and a poly(carbonate-silsesquioxane-bridge-urea) urethane. Biomaterials 2005;26:6271-9.
34. Jell G, Minelli C, Stevens M. Biomaterial-related approaches: surfacestructuring. In: Meyer U, Meyer T, Handschel J, Wiesmann HP, editors.Fundamental of tissue engineering and regenerative medicine. Leipzig:Springer; 2009. p. 469-84.
35. Georges PC, Janmey PA. Cell type-specific response to growth on softmaterials. J Appl Physiol 2005;98:1547-53.
36. Wang YL. Traction forces and rigidity sensing of adherent cells. ConfProc IEEE Eng Med Biol Soc 2009;2009:3339-40.
37. Yeung T, Georges PC, Flanagan LA, Marg B, Ortiz M, Funaki M, et al.Effects of substrate stiffness on cell morphology, cytoskeletal structure,and adhesion. Cell Motil Cytoskeleton 2005;60:24-34.
38. Biggs MJ, Richards RG, Dalby MJ. Nanotopographical modification: aregulator of cellular function through focal adhesions. Nanomedicine2010;6:619-33.
39. Dalby MJ, Yarwood SJ, Johnstone HJ, Affrossman S, Riehle MO.Fibroblast signaling events in response to nanotopography: a gene arraystudy. IEEE Trans Nanobioscience 2002;1:12-7.
40. Pattison MA, Wurster S, Webster TJ, Haberstroh KM. Three-dimensional, nano-structured PLGA scaffolds for bladder tissuereplacement applications. Biomaterials 2005;26:2491-500.
41. Schenke-Layland K, Rofail F, Heydarkhan S, Gluck JM, Ingle NP,Angelis E, et al. The use of three-dimensional nanostructures to instruct
12 L. Nayyer et al / Nanomedicine: Nanotechnology, Biology, and Medicine xx (2013) xxx–xxx
cells to produce extracellular matrix for regenerative medicine strategies.Biomaterials 2009;30:4665-75.
42. Abbott A. Cell culture: biology's new dimension.Nature 2003;424:870-2.43. Wang F, Weaver VM, Petersen OW, Larabell CA, Dedhar S, Briand P,
et al. Reciprocal interactions between beta1-integrin and epidermalgrowth factor receptor in three-dimensional basement membrane breast
cultures: a different perspective in epithelial biology. Proc Natl AcadSci U S A 1998;95:14821-6.
44. Hansen JC, Lim JY, Xu LC, Siedlecki CA, Mauger DT, Donahue HJ.Effect of surface nanoscale topography on elastic modulus of individualosteoblastic cells as determined by atomic force microscopy. J Biomech2007;40:2865-71.





















![Nanocomposite [5]](https://static.documents.pub/doc/80x56/577c7ecf1a28abe054a26499/nanocomposite-5.jpg)






