59
Desmoid Tumors Paul Chung MD August 25 th , 2016 downstatesurgery.org
Desmoid Tumors Paul Chung MD
August 25th, 2016
downstatesurgery.org

Case Presentation
• 49F who presented with epigastric abdominal pain • Pain intermittent and colicky • Associated with soft bowel movements • Denied fever/chills, nausea/vomiting
• Colonoscopy performed 1 year ago showing diverticulosis
downstatesurgery.org

Case Presentation
• PMHx: HTN, DM, ESRD (MWF), glaucoma, leiomyomatous uterus • PSHx: Debridement of Right Heel Ulcer, C-sections x 3, Tonsillectomy,
LUE AV Fistula creation, Open Cholecystectomy • FHx: unremarkable • SHx: denies T/E/D • Ax: Penicillin
downstatesurgery.org

Case Presentation
• Vitals: Stable • Gen: AAOx3, legally blind • Abd: well-healed surgical scars, no masses, non-distended, soft,
slightly TTP in epigastrium, no rebound/guarding • Ext: good bruit at LUE AVF site
• Labs: unremarkable
downstatesurgery.org

Case Presentation
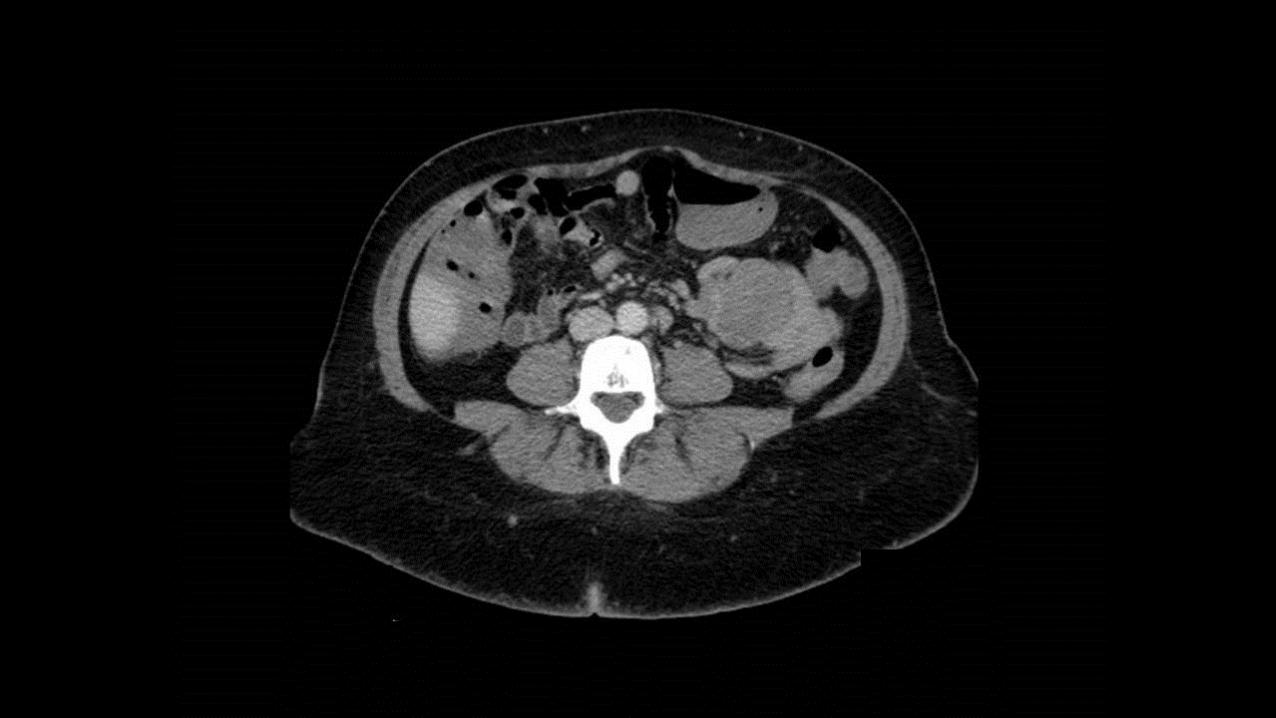
• CT Abdomen/Pelvis: well circumscribed small tissue mass measuring 4.4 x 5 cm abutting the small bowel, diverticulosis
downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org
downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

downstatesurgery.org

Intervention
• Diagnostic Laparoscopy, Exploratory Laparotomy, Small Bowel Resection, Mesenteric Mass Excision
downstatesurgery.org
Postoperative Course
• POD 0: Transferred to floor from PACU
downstatesurgery.org

Postoperative Course
• POD 0: Transferred to floor from PACU • POD 1: Tolerated regular diet
downstatesurgery.org

Postoperative Course
• POD 0: Transferred to floor from PACU • POD 1: Tolerated regular diet • POD 3: Discharged home
downstatesurgery.org

Postoperative Course
• POD 0: Transferred to floor from PACU • POD 1: Tolerated regular diet • POD 3: Discharged home • Pathology
• Well circumscribed mass lesion measuring 6.5 x 5.6 x 5 cm attached to the serosal side of bowel
• Spindle cell lesion with poorly defined interface with intestinal muscularis propria microscopically
• Strongly positive for β-Catenin, negative for CD117 • Fibromatosis, margins negative
downstatesurgery.org

Questions? downstatesurgery.org

Overview
• Definition • History • Epidemiology • Presentations • Diagnostic Tests • Treatments • Surveillance • Outcomes
downstatesurgery.org
Definition
• World Health Organization • “Clonal fibroblastic proliferations that arise in the deep soft tissues and are
characterized by infiltrative growth and tendency toward local recurrence but an inability to metastasize”
• Synonyms
• Aggressive Fibromatosis • Deep Musculoaponeurotic Fibromatosis • Well Differentiated Nonmetastasizing Fibrosarcoma • Fibrosarcoma Grade I of the Desmoid Type
Pathology and Genetics of Tumours of Soft Tissue and Bone. Fletcher CDM, Unni KK, Mertens F. World Health Organization Classification of Tumours. Lyon, France: IARC Press;2002:83-4.
downstatesurgery.org

History
• 1832: MacFarlane describes a growth in the abdominal wall of a young woman after delivery
MacFarlane J. Clinical report on the surgical practice of Glasgow Royal Infirmary. Glasgow: D. Robertson, 1832: 63
downstatesurgery.org

History
• 1832: MacFarlane describes a growth in the abdominal wall of a young woman after delivery
• 1883: “Desmoid” is coined by Müller from “Desmos”
Müller J. Ueber den feinern Bau und die Formen der krankhaften Geschwülste. Berlin: G Reimer; 1838. 80 pp.
downstatesurgery.org

History
• 1832: MacFarlane describes a growth in the abdominal wall of a young woman after delivery
• 1883: “Desmoid” is coined by Müller from “Desmos” • 1951: Gardner describes associated findings of “conspicuous surface
lumps or tumors” in all family members diagnosed with Familial Adenomatous Polyposis
Gardner EJ. A genetic and clinical study of intestinal polyposis, a predisposing factor for carcinoma of the colon and rectum. Am J Hum Genet. 1951;3(2):167-76.
downstatesurgery.org

Epidemiology
• Incidence: 2.4 – 4.3/1,000,000 cases/year • 0.03% of all neoplasms • 3% of all soft-tissue tumors • Median age 30 years • Female to Male ratio of 2:1
•Reitamo JJ, Hayry P, Nykyri E et al. The desmoid tumor. I. Incidence, sex-, ageand anatomical distribution in the Finnish population. Am J Clin Pathol 1982; 77(6): 6 •Nieuwenhuis MH, Casparie M, Mathus-vliegen LM, Dekkers OM, Hogendoorn PC, Vasen HF. A nation-wide study comparing sporadic and familial adenomatous polyposis-related desmoid-type fibromatoses. Int J Cancer. 2011;129(1):256-61. 65–673.
downstatesurgery.org

Pathophysiology
• β-catenin dysregulation implicated • CTNNB1 • Levels controlled by adenomatous polypsosis coli (APC)
• Key mediator in Wnt signaling pathway • Wnt targets include c-Myc • Wnt also implicated in development of colorectal and other GI carcinomas
• Additional mutations in the pediatric population
•Miyoshi Y, Iwao K, Nawa G, Yoshikawa H, Ochi T, Nakamura Y. Frequent mutations in the beta-catenin gene in desmoid tumors from patients without familial adenomatous polyposis. Oncol Res. 1998;10(11-12):591-4. •Ng TL, Gown AM, Barry TS, et al. Nuclear beta-catenin in mesenchymal tumors. Mod Pathol. 2005;18(1):68-74.
downstatesurgery.org

Presentations
• Sporadic • Gardner Syndrome • Pregnancy
downstatesurgery.org

Sporadic
• Most common presentation • Somatic APC mutations • Activating mutations of CTNNB1 • Most commonly associated with Desmoid tumors of the extremities
• Limb girdles • Proximal extremities
Lewis JJ, Boland PJ, Leung DH, Woodruff JM, Brennan MF. The enigma of desmoid tumors. Ann Surg. 1999;229(6):866-72.
downstatesurgery.org

Extremity Desmoids
Lewis JJ, Boland PJ, Leung DH, Woodruff JM, Brennan MF. The enigma of desmoid tumors. Ann Surg. 1999;229(6):866-72.
downstatesurgery.org

Head and Neck Desmoids
Alherabi AZ, Marglani OA, Bukhari DH, Al-khatib TA. Desmoid tumor (fibromatosis) of the head and neck. Saudi Med J. 2015;36(1):101-3.
downstatesurgery.org

Gardner Syndrome
• 5 – 15% of patients with Desmoid tumors also have a diagnosis of Familial Adenomatous Polyposis (FAP)
• 10 – 20% of FAP patients have Gardner Syndrome • Mutation in adenomatous polyposis coli (APC) gene (5q21-22) • More commonly associated with intra-abdominal Desmoid tumors • Often unresectable • Cause of death in approximately 11% of patients
Nieuwenhuis MH, Casparie M, Mathus-vliegen LM, Dekkers OM, Hogendoorn PC, Vasen HF. A nation-wide study comparing sporadic and familial adenomatous polyposis-related desmoid-type fibromatoses. Int J Cancer. 2011;129(1):256-61.
downstatesurgery.org

Intra-abdominal Desmoids: FAP
Casper M, Petek E, Henn W, et al. Multidisciplinary treatment of desmoid tumours in Gardner's syndrome due to a large interstitial deletion of chromosome 5q. QJM. 2014;107(7):521-7.
downstatesurgery.org

Mesneteric Desmoids: FAP
Ioannidis O, Paraskevas G, Chatzopoulos S, et al. Multiple desmoid tumors in a patient with familial adenomatous polyposis caused by the novel W421X mutation. Rev Esp Enferm Dig. 2012;104(3):146-50.
downstatesurgery.org

Pregnancy
• Estimated to be 8 – 18% of all Desmoid tumors • Most commonly associated with Desmoid of abdominal wall • Thought to be associated with high estrogen state • Associated with good outcomes • Not associated with increased obstetric risk
Fiore M, Coppola S, Cannell AJ, et al. Desmoid-type fibromatosis and pregnancy: a multi-institutional analysis of recurrence and obstetric risk. Ann Surg. 2014;259(5):973-8. Robinson WA, Mcmillan C, Kendall A, Pearlman N. Desmoid tumors in pregnant and postpartum women. Cancers (Basel). 2012;4(1):184-92.
downstatesurgery.org

Abdominal Wall Desmoids
Meshikhes AW, Al-zahrani H, Ewies T. Laparoscopic excision of abdominal wall desmoid tumor. Asian J Endosc Surg. 2016;9(1):79-82.
downstatesurgery.org

Intra-abdominal Desmoids: Pregnancy
De bree E, Dimitriadis E, Giannikaki E, Chryssou EG, Melissas J. A giant pregnancy-associated intra-abdominal desmoid tumour: not necessarily a contraindication for subsequent pregnancy. World J Surg Oncol. 2013;11:277.
downstatesurgery.org

Diagnosis
• CT • Preferred for intra-abdominal lesions
• MRI • Preferred for extremities, head/neck, abdominal/thoracic walls • Cannot predict clinical behavior based on imaging
• Biopsy • Confirms the diagnosis
• Endoscopy • Suspected FAP
downstatesurgery.org

Treatment
• Extra-abdominal/Abdominal Wall • Intra-abdominal
downstatesurgery.org

Extra-abdominal/Abdominal Wall Desmoids
• Initial Observation • Stable continue to observe • Progression/Symptomatic treatment
• Radiation Therapy • Primary usually given as 50 – 60 Gy over 5 – 7 weeks • Adjuvant indicated for R2 resection • Adjuvant not shown to be beneficial for R0/R1 resection • Neoadjuvant requires more studies
Church J, Simmang C. Practice parameters for the treatment of patients with dominantly inherited colorectal cancer (familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer). Dis Colon Rectum. 2003;46(8):1001-12.
downstatesurgery.org

Extra-abdominal/Abdominal Wall Desmoids
• Chemotherapy ± Radiation Therapy • Sulindac/NSAIDs • Tamoxifen ± Sulindac • Methotrexate + Vinblastine • Toremifene (SERM) • Inteferon • Doxorubicine • Imatinib/Sorafenib
Church J, Simmang C. Practice parameters for the treatment of patients with dominantly inherited colorectal cancer (familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer). Dis Colon Rectum. 2003;46(8):1001-12.
downstatesurgery.org

Extra-abdominal/Abdominal Wall Desmoids
• Surgical Resection • R1 resection acceptable if R0 resection will result in unacceptable morbidity
Crago AM, Denton B, Salas S, et al. A prognostic nomogram for prediction of recurrence in desmoid fibromatosis. Ann Surg. 2013;258(2):347-53.
downstatesurgery.org

Intra-abdominal Desmoids
• Radiation Therapy • Generally not recommended
• Chemotherapy (FAP) • Inert tumors
• No therapy • Sulindac
• Slowly Growing or Mildly Symptomatic • Tamoxifen (80 – 120 mg/day) + Sulindac • Methotrexate + Vinblastine
• Rapidly Growing • High-dose Tamoxifen (120 mg/day) • Antisarcoma-type chemotherapy
Church J, Simmang C. Practice parameters for the treatment of patients with dominantly inherited colorectal cancer (familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer). Dis Colon Rectum. 2003;46(8):1001-12.
downstatesurgery.org

Intra-abdominal Desmoids
• Surgical Resection • FAP
• Often unresectable • High rate of recurrence after resection • Resection reserved for small, well-defined tumors with clear margins • However may shorten mesentery • Prevent Ileal Pouch Anal Anastomosis for Proctectomy resulting in Ileostomy
• Sporadic • Resection offered if symptomatic/threatening function
Church J, Simmang C. Practice parameters for the treatment of patients with dominantly inherited colorectal cancer (familial adenomatous polyposis and hereditary nonpolyposis colorectal cancer). Dis Colon Rectum. 2003;46(8):1001-12.
downstatesurgery.org

Surveillance
• History and Physical with appropriate imaging • Every 3 – 6 months • For 2 – 3 years • Then annually
Soft Tissue Sarcoma: NCCN Guidelines version 2.2016
downstatesurgery.org

Recurrence
• Estimated 16 – 39% recurrence rate despite R0 resection • Up to 50% recurrence within 5 years
• Recurrence risk likely linked to underlying biology rather than margins • No difference in survival between R0 and R1 resection • Aggressive resection to achieve R0 may not be beneficial • Resection or Chemotherapy ± Radiation Therapy are options
Peng PD, Hyder O, Mavros MN, et al. Management and recurrence patterns of desmoids tumors: a multi-institutional analysis of 211 patients. Ann Surg Oncol. 2012;19(13):4036-42.
downstatesurgery.org

Outcomes: Observation
• 142 patients • 74 patients with primary tumors • 68 patients with recurrence • 83 (58.5%) received Wait & See • 59 (41.5%) received hormonal + chemotherapy • 5-year progression-free survival measured
• 49.9% vs 58.6% for the Wait & See and medical therapy groups respectively • p = 0.3196
Fiore M, Rimareix F, Mariani L, et al. Desmoid-type fibromatosis: a front-line conservative approach to select patients for surgical treatment. Ann Surg Oncol. 2009;16(9):2587-93.
downstatesurgery.org

Outcomes: Chemotherapy
• Tamoxifen • Use first described in 1983 • 15 – 20% response rate • 25 – 30% symptomatic relief rate • Data from small series and case reports
• Sulindac + Tamoxifen • 8 sporadic Desmoids
• 5 (62.5%) had stable disease, 1 (12.5%) had complete response • 17 FAP Desmoids
• 11 (64.7%) had stable disease/symptomatic improvement
Kinzbrunner B, Ritter S, Domingo J, Rosenthal CJ. Remission of rapidly growing desmoid tumors after tamoxifen therapy. Cancer. 1983;52(12):2201-4.
Hansmann A, Adolph C, Vogel T, Unger A, Moeslein G. High-dose tamoxifen and sulindac as first-line treatment for desmoid tumors. Cancer. 2004;100(3):612-20.
downstatesurgery.org

Outcomes: Surgical Resection
• 426 patients • 376 (88.3%) received surgical resection ± radiation therapy
• 63 (16.8%) had R2 resection • 42 (66.7%) had local progression
• 323 (85.9%) had R0/R1 resection • 143 (44.3%) had local recurrence
• Progression-Free Survival • Age (HR 1.97 [1.36 – 2.84], p<0.001) • Size (HR 1.67 [1.13 – 2.36], p=0.008) • Extra-abdominal tumor (HR 2.55 [1.48 – 4.40], p<0.001)
Salas S, Dufresne A, Bui B, et al. Prognostic factors influencing progression-free survival determined from a series of sporadic desmoid tumors: a wait-and-see policy according to tumor presentation. J Clin Oncol. 2011;29(26):3553-8.
downstatesurgery.org

Outcomes: Surgical Resection
• 495 patients undergoing resection (1982 – 2011) • 15 (3.0%) patients had FAP • 440 (89%) patients with R0/R1 resection
• 100 had recurrence • 92 had recurrence within 5 years
• 53 (11%) patients with R2 resection • 8 (1.6%) patients died after 5 years
• All R2 resection • 6 had intraabdominal lesions • 3 had FAP
Crago AM, Denton B, Salas S, et al. A prognostic nomogram for prediction of recurrence in desmoid fibromatosis. Ann Surg. 2013;258(2):347-53.
downstatesurgery.org

Conclusion
• Non-metastasizing, locally recurrent disease • Heterogeneous presentation
• Sporadic, Gardner Syndrome, Pregnancy-associated • Extremity, Abdominal Wall, Intra-abdominal
• R1 resection acceptable if avoiding undue morbidity • Recurrence likely related to underlying biology and less so margins • Trend toward less invasive approach such as observation
downstatesurgery.org

Thank You
downstatesurgery.org
Question
All of the following are true regarding sporadic desmoid tumors EXCEPT A. Spontaneous regression may occur B. They commonly metastasize after resection C. Surgery is the mainstay of treatment D. The site of tumor is associated with recurrence E. They occur more commonly in women
downstatesurgery.org

Question
All of the following are true regarding sporadic desmoid tumors EXCEPT A. Spontaneous regression may occur B. They commonly metastasize after resection C. Surgery is the mainstay of treatment D. The site of tumor is associated with recurrence E. They occur more commonly in women
downstatesurgery.org









![Intra-Abdominal and Abdominal Wall Desmoid Fibromatosis · intra-abdominal and involving the small bowel mesentery [2]. TREATMENT Surgery Margin-negative resection has historically](https://static.documents.pub/doc/80x56/5e5a290071d21b380f5b7e74/intra-abdominal-and-abdominal-wall-desmoid-fibromatosis-intra-abdominal-and-involving.jpg)







