1 Practical course: Basic biochemical methods and ischemic heart models Determination of infarct size in isolated perfused rat hearts subjected to ischemia/reperfusion A practical manual Prepared by Csaba Csonka MD PhD Tamas Csont MD PhD 2011 Supported by: HURO/0901/069/2.3.1 HU-RO-DOCS
Transcript
1
Practical course: Basic biochemical methods and ischemic heart models
Determination of infarct size in isolated perfused
rat hearts subjected to ischemia/reperfusion
A practical manual
Prepared by Csaba Csonka MD PhD Tamas Csont MD PhD
2011
Supported by: HURO/0901/069/2.3.1 HU-RO-DOCS
2
Content: Ex vivo organ perfusion 3
Langendorff rat heart 3
Species 6
The perfusion system 7
The perfusion fluid 8
Oxygenization 10
Thermostation 10
Getting started 11
Anesthesia and anticoagulation 12
Cutting out the heart 14
Cannulation 14
Induction of ischemia followed by reperfusion 16
End points 18
Detection of infarct size 19
Slicing the hearts and TTC incubation 19
Evaluation of the scanned pictures 20
Cleaning 21
References 22
3
Ex vivo organ perfusion In science, the term ex vivo (Latin: "out of the living") refers to experimentations or measurements done in or on tissue/organ in an artificial environment outside the organism. Ex vivo conditions allow experimentation under more controlled conditions than is possible in in vivo experiments (in the intact organism), at the expense of altering the "natural" environment. The term ex vivo is not synonymous to the term in vitro ("within the glass").
Langendorff rat heart Coronary artery disease and its most severe manifestation, ischemia-reperfusion-induced myocardial infarction, continue to be the leading cause of mortality in the “western” type societies. Therefore, attenuation of ischemia/reperfusion injury is of great importance. There is a conflict between the quantity and quality of data that can be acquired from an experimental model versus its clinical relevance. However, a primary advantage of using ex vivo tissues is the ability to perform tests or measurements that would otherwise not be possible or ethical in living subjects. At a practical level, the isolated heart, especially from small mammals, provides a highly reproducible preparation which can be studied quickly and in large numbers at relatively low cost. The isolated perfused mammalian heart preparation was established by the German physiologist Oskar Langendorff in 1895 as a tool for studying heart biology. Since then it has been one of the most widely accepted technique in modern cardiovascular and pharmacological research to study physiological, pharmacological, biochemical, molecular biological aspects of basic and pre-clinical research using animals in spite of a few shortcomings. These measurements can be made in the absence of the confounding effects of other organs, the systemic circulation, and a host of peripheral complications such as circulating neural and hormonal factors.
4
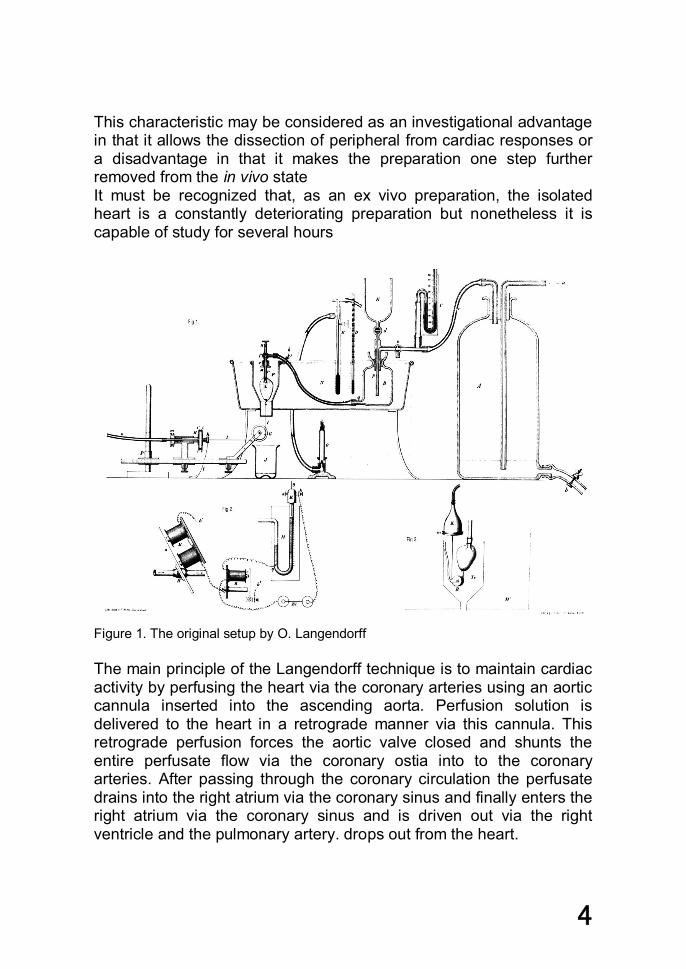
This characteristic may be considered as an investigational advantage in that it allows the dissection of peripheral from cardiac responses or a disadvantage in that it makes the preparation one step further removed from the in vivo state It must be recognized that, as an ex vivo preparation, the isolated heart is a constantly deteriorating preparation but nonetheless it is capable of study for several hours
Figure 1. The original setup by O. Langendorff The main principle of the Langendorff technique is to maintain cardiac activity by perfusing the heart via the coronary arteries using an aortic cannula inserted into the ascending aorta. Perfusion solution is delivered to the heart in a retrograde manner via this cannula. This retrograde perfusion forces the aortic valve closed and shunts the entire perfusate flow via the coronary ostia into to the coronary arteries. After passing through the coronary circulation the perfusate drains into the right atrium via the coronary sinus and finally enters the right atrium via the coronary sinus and is driven out via the right ventricle and the pulmonary artery. drops out from the heart.
5
The Langendorff technique is well suited to many different models of cardiac disease and dysfunction. Some of the more widely used models include:
anoxia or hypoxia at various degrees of oxygen deprivation ischemia (blockade of circulation; total or low flow) ischemia (global or regional) ischemia followed by reperfusion ischemic pre- and ischemic postconditioning drug response toxicology (e.g., screening for novel test compounds) donor-heart transplantation storage techniques stem-cell therapy for myocardial diseases
Types of the Langendorff perfusion: (i) Constant Flow Mode - perfusate is pushed through the heart at a constant rate and the perfusion pressure is measured to give a representation of the coronary resistance (ii) Constant Pressure Mode - the desired pressure is maintained and the resulting fluctuations in the rate of coronary flow are measured. Both type of Langendorff perfusion can be performed in recirculating (recycling of perfusate) and non-recirculating modes.
Another method where the perfusion of the coronary arteries is maintained by the own work of the heart: the working heart preparation.
As shown in Figure 3, this is a more complex preparation where both the left atrium and ventricle are cannulated. The perfusion fluid enters to the left atrium from the left atrial reservoir through the left atrial cannula. From the left atrium, and than from the left ventricle the own work of the heart ejects the perfusion fluid through the aorta against a certain resistance ultimately into the artificial lung. This resistance (called afterload) renders coronary circulation possible. Coronary flow is collected after dropping out from the heart and pumped to the lung. After oxygenation and filtration all the perfusion fluid arrived back to the left atrial reservoir and the cycle starts again.
6
Species
Hearts from any mammalian species including also humans (together with non-mammalian hearts such as those from reptiles or birds) may be ex vivo perfused. Isolated perfusions of large animal hearts such as pigs, or dogs are less frequently used. This is probably due to the high cost, greater variability, large volumes of perfusion fluids and large equipment that is required.
Without doubt the most frequently studied and the best characterized heart is the rat heart. There are numerous reports of studies with other rodents. The advent of transgenic technology will undoubtedly result in increasing numbers of studies using mice.
Animal limitations
Rabbit difficulties with anesthesia Rat very short action potential duration (not perfect for
are much more difficult), very high heart rate Guinea pig totally collateralized, non-similarly to human
Figure 2. Main species used in our lab
7
The perfusion system
O2
filter
pump heartchamber
aorticflowmeter
3-way taplung
left atrialreservoire
O2
elasticchamber
Langendorffchamber
perfu
sion
pres
sure
KH
KH
Figure 3. Outline of our Langendorff and Neely perfusion systems
Units: Storage Connectors Neely chamber rigid connectors Langendorff chamber elastic connectors Elastic chamber and bubble trap cannulae Left atrial reservoir Heart suspending chamber Basic requirements against components Fix volume, fix shape Heat-, acid-, lye-resistant; do not absorb drugs Transparent Easy to clean, cheap, replaceable
8
The perfusion fluid As a perfusion fluid, crystalloid-based perfusion buffers (eg Ringer-lactate, Krebs-Henseleit buffer, Tyrode’s solution, etc.) are preferred, rather than blood. Its main functions:
nutrients for energy production (eg glucose, pyruvate, free fatty acids, lactate, proteins)
insure Ca2+ for contractions maintain pH 7.4±0.05 as buffer system (eg CO2/HCO3
-, PO43-)
sustain extracellular necessary ionmilieu (K+, Na+, Mg2+, Cl-) maintain osmolarity (290-300 mOsm) oxygen supply (see later) washout of metabolites
Krebs Henseleit solution: In our system the Krebs-Henseleit solution content in mmol/L: NaCl 118.6, KCl 4.3, NaHCO3 25, KH2PO4 1.2, MgSO4 1.2, glucose 11.1 and CaCl2 1.5, pH 7.3–7.5, gassed with carbogen [95% O2, 5% CO2]) at a constant perfusion pressure of 100 H2Ocm at 37 °C. Components for 5L Krebs-Henseleit solution: Weight (g) MW final cc (mmol/L) NaCl 34.66 58.44 118.6 NaHCO3 10.5 84.01 25.0 KCl 1.6 74.56 4.3 MgSO4×7H2O 0.72 120.37 1.2 KH2PO4 0.817 136.09 1.2 Glucose×1H2O 11.0 198.17 11.1 CaCl2×2H2O 1.1 147.02 1.5 Procedure
1. Measure out 4L of distilled water. Water temperature should be room temperature.
2. While gently stirring the water, add the powdered components except for CaCl2. Stir until dissolved. Do not heat.
3. Rinse original package with a small amount of water to remove all traces of powder. Add to solution in step 2.
9
4. Solution should be gassed for 5 min with 95% O2 and 5% CO2 carbogen.
5. Separately, measure out 1L of distilled water. While gently stirring the water, add CaCl2×2H2O. Stir until dissolved.
6. Mix solutions in a 5-L dish. 7. While stirring, adjust the pH of the medium to 7.4 using of 1N
HCl 8. Filter immediately using vacuum pump and membrane with a
porosity of 5 microns. Storage and Stability Store Krebs-Henseleit solution 2-8 °C, use it before 3 days. Deterioration of the liquid medium may be recognized by any or all of the following: (i) pH change, (ii) precipitate or particulates, (iii) cloudy appearance (iv) color change.
10
Oxygenization Carbogen (mixture of 95% O2 and 5% CO2) is used to oxygenize Krebs-Henseleit solution via a sintered glass gas distributor connected to the high-pressure gas cylinder using a gas reductor. Gassing with CO2 is necessary to maintain pH, therefore, use of pure O2 deteriorate quickly cardiac function. O2 solubility in Krebs-Henseleit solution is approximately 17 mL/L using carbogen at 37 °C. In case of heart of a 300-g rat, CF is approximately 15-20 mL/min Oxygen consumption in different tissues: Cardiac State MVO2(ml O2 min-1 100g-1) Arrested heart 2 Resting heart rate 8 Heavy exercise 70 Brain 3 Kidney 5 Skin 0.2 Resting muscle 1 Contracting muscle 50
Thermostation In order to maintain experimental environment closest to the physiological milieu, maintenance of an accurate temperature setup is one of the most critical factor during the experiments. Therefore, all containers of the perfusion system has a water-jacket connected to a large capacity thermostat pump. Procedure:
1. Open carbogen gas flow by adjusting the gas redactor to get approximately 200 mL/min gas flow
2. Switch on the thermostat and check temperature before onset of experiments
11
Getting started 1. Pay attention to the good fit of all connections and close taps well. 2. Open carbogen, adjust gas flow to ~200 mL/min. Check pressure on the manometer of the gas cylinder. Do not forget to open the tap connected to Langendorff system. 3. Fill up the perfusion system with Krebs-Henseleit solution using a syringe of 50 ml in a reverse manner (from the bottom) to prevent accumulation of air below the glass frit filter. Open the 3-way tap so that it remains closed to the direction of the cannula. Then fit the syringe into the tap and squish the Krebs-Henseleit solution as quickly as you can do it. Level of Krebs-Henseleit solution should be over the level of glass frit in the Langendorff reservoir. Air bubbles are not allowed to remain under the glass frit because they jeopardize the function of isolated hearts due to the possibility of aeroembolism. If perfusion fluid has flown out for any reason dropping should be stopped as soon as possible. 4. Then fill up the Langendorff reservoir from the top with Krebs-Henseleit solution. The pressure of fluid column (perfusion pressure) should be 100 H2Ocm. It means that the vertical distance between the end of the cannula and the liquid level of the perfusion fluid in the Langendorff reservoir should be exactly 100 cm. Check distance with tape measure. 5. Prepare the tools:
2 pcs scissors 3 pcs forceps (one pair are anatomic) 1 pc bulldog clamp 1 pc glass baker for the isolated heart (fill the baker with Krebs-
Henseleit solution and store it on 4 ˚C or on ice) aluminium foil permanent marker for writing the animal code, date, and study
name on the aluminium foil.
12
Anesthesia and anticoagulation
Isolation of the heart requires the donor animal to be rendered unconscious prior to excision. Anesthesia can be induced by inhalation of agents such as isoflurane or injection (intravenously or intraperitoneally) with agents such as pentobarbitone. For intravenous injection, femoral vein is the preferred route the vein is accessed by a small skin incision. An alternative to anesthesia is cervical dislocation, however it is allowed only for newborn rats. Ether is hazardous as it is irritant to the animal. Therefore, it is not allowed to use according to the latest regulations.
Whatever the choice of procedure (and this may be influenced by local animal welfare regulations), every effort should be made to minimize stress prior to and during anesthesia. Therefore, keep the animal in a quiet environment and minimize handling.
In order to prevent the formation of thrombi in the excised heart, it is strongly recommended to administer anticoagulant, namely heparin before isolation. Heparin is given parenterally because it is not absorbed from the gut, due to its high negative charge and large size. Heparin is preferably injected intravenously to femoral vein which is accessed by a small skin incision.
Heparin activates lipases, therefore, in studies studying lipid or fatty acid metabolism it is advisable to choose another anticoagulant. Coagulation tests are much shorter in rats than in humans, therefore without heparin the ex vivo model should be prepared extremely fast. The conventional dose for heparine is 500 IU/kg.
Coagulation tests:
Rat Human Blood clotting time (s) 125±4 508±5 Bleeding time (s) 88±4 270±3
13
Procedure
1. Measure animal weight 2. Calculate necessary amount of pentobarbital (Euthasol) 3. Inject requested volume intraperitoneally 4. During time when anesthetic takes effect, prepare heparine
(final concentration is 500 U/mL) 5. When animal is unconscious, Inject requested volume
intravenously to femoral vein (500 U/kg) accessed by a small skin incision
6. Wait 1 min 7. Go to next step
14
Cutting out the heart
Once the animal is anesthetized the heart can be excised. Generally, the diaphragm is accessed by a transabdominal incision and cut carefully to expose the thoracic cavity. The thorax is opened by a bilateral incision along the lower margin of the last to first ribs, the thoracic cage is then reflected over the animals head, exposing the heart. We then cradle the heart between their fingers (it is essential to do this gently to avoid contusion injury) and then lift the heart slightly before incising the aorta, vena cava and pulmonary vessels. Immediately after excision, hearts are immersed in cold perfusion solution (4 °C to limit any ischemic injury during the period between excision and the restoration of vascular perfusion).
Cannulation
For adequate perfusion of the heart a suitably sized cannula is required for insertion into the aorta.
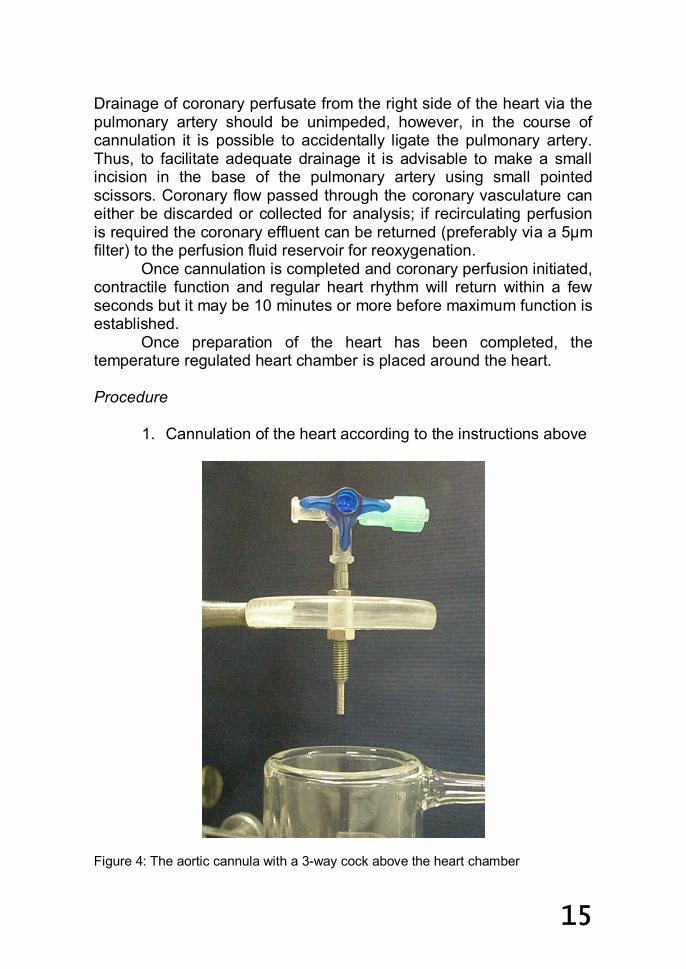
The external diameter is typically similar to, or slightly larger than, that of the aorta (about 3mm for a heart from a 250g rat). Several small circumferential grooves is usually machined into the distal end of the cannula to prevent the aorta from slipping off (fig 4).
It is advisable to have the perfusion fluid gently dripping from the aortic cannula prior to cannulation since this helps minimize the chance of air emboli at the time the heart is attached to the cannula.
Before cannulation cut the aorta transversally just before the origin of the innominate artery to form a intact regular aortic ostia for cannulation.
Hearts should be held gently between the tips of blunt-ended fine curved forceps, taking care to avoid stretching or ripping of the aortic wall. The aorta is then gently eased over the end of the cannula, taking care not to insert the cannula too far (5-7 mm) into the aorta since this would occlude the coronary ostia or damage the aortic valve. The aorta is then clamped to the cannula with a small blunt artery clip (bulldog clamp), whilst a ligature is rapidly tied around the aorta, locking into the grooves; the artery clip can then be removed. Full flow of perfusate should be initiated as soon as the heart is mounted on the cannula.
Once the heart is securely attached to the cannula any surplus tissue (such as bits of thymus, fat or lungs) can be trimmed away.
15
Drainage of coronary perfusate from the right side of the heart via the pulmonary artery should be unimpeded, however, in the course of cannulation it is possible to accidentally ligate the pulmonary artery. Thus, to facilitate adequate drainage it is advisable to make a small incision in the base of the pulmonary artery using small pointed scissors. Coronary flow passed through the coronary vasculature can either be discarded or collected for analysis; if recirculating perfusion is required the coronary effluent can be returned (preferably via a 5µm filter) to the perfusion fluid reservoir for reoxygenation.
Once cannulation is completed and coronary perfusion initiated, contractile function and regular heart rhythm will return within a few seconds but it may be 10 minutes or more before maximum function is established.
Once preparation of the heart has been completed, the temperature regulated heart chamber is placed around the heart. Procedure
1. Cannulation of the heart according to the instructions above
Figure 4: The aortic cannula with a 3-way cock above the heart chamber
16
Induction of ischemia followed by reperfusion
The induction of regional ischemia is performed by the ligation of the left anterior descending coronary artery usually after a 10-15 min long normoxic (equilibration) perfusion period. To stabilize the heart, hold it gently with your finger and place a small suture (3-0 non-absorbable suture silk, Mersilk®) from the mid level of the left atrium to the mid level of the pulmonary tract. The suture must be deep enough, which you could carry out easily with a “half moon”-shaped suture. The ligature ends are passed through a short plastic tube to form a snare.
Figure 5. The place of the ligature to induce regional ischemia
The major coronary arteries min rats, in contrast to larger
mammalian species do not lie on the surface of the heart, rather are covered with a layer of myocardium throughout their course.
17
Figure 6. Coronary arteries in rats (panle A: arrow, panel B: “L”) are not in the surface of the heart
For coronary artery occlusion and reperfusion, the plastic tube is pressed onto the surface of the heart directly above the coronary artery and released to induce coronary occlusion and released to induce reperfusion. There are no exact definitions in the literature about the pressure to induce coronary occlusion. Extra forces to certainly occlude coronary occlusion can result in tissue damage. Therefore, in isolated heart perfusions models the same forces are provided by a 100 g weight flung over a small pulley.
The occlusion is performed with the help of a plastic bead, and a plastic tube. The silk must be attached to a 100 g heavy weight without any retraction to maintain the same occlusion force during experiments for all og the hearts. After a successful occlusion, a 30-40% decrease is detectable in coronary flow. Induction of ischemic preconditioning
Ischemic preconditioning is usually achieved by 3 intermittent 5 min long coronary occlusion and reperfusion. In contrast with postconditioning it is performed in regional ischemia. Do not forget to adjust the length of preischemic perfusion in your ischemia/reperfusion control group (usually 40 min).
18
End points
Once the heart is cannulated and successfully beating, there are several parameters that can be measured and recorded from the Langendorff preparation including:
infarct size histology/morphology myocardial contractile function ventricular pressure and its derivatives ventricular volume and its derivatives flows (aortic, coronary, cardiac output) pressure-volume work electrophysiology including arrhythmias tissue and perfusate samples for various biochemical
measurements Note:
In the Langendorff system, because the cardiovascular system is no longer a closed loop, the ventricles do not fill with the perfusate and therefore do not perform pressure-volume work. Left ventricular pressure can however still be measured with the use of a fluid-filled balloon-tipped catheter connected to a pressure transducer. Once inserted, the ventricle can contract isovolumetrically against the balloon. Although this parameter can not be accreted as real left ventricular pressure, it is used to describe cardiac performance.
19
Detection of infarct size
Using popular Langendorff perfusion, 2,3,5-triphenyltetrazolium chloride (TTC, CAS 298-96-4) staining became the gold standard of infarct size determination. Among the advantages of the TTC staining the relatively low cost, high throughput, easy performance, reliability and reproducibility can be mentioned. TTC staining is a well described method used by uncountable researchers; however, it contained several non-objective parameters. Therefore, a kind of standardization of this method is necessary in order to minimize errors of measurements and thus comparison of different working groups all over to world is more possible.
TTC is a redox indicator commonly used in biochemical experiments to differentiate between metabolically active and inactive tissues. This white crystalline powder forms colorless solution with water is enzymatically reduced to brick-red precipitations of formazan dye (TPF, 1,3,5-triphenylformazan, CAS 531-52-2) in living tissues with intact mitochondrial respiration due to the activity of various dehydrogenases (i.e. succinate dehydrogenase) in the presence of electron donor NADH. After TTC staining, necrotic zone remains as pale areas of the heart.
There is a consensus in the literature that in ex vivo isolated rat heart experiments after ischemia usually a 120 min of reperfusion is used to measure infarct size.
To delineate from area at risk at the end of reperfusion coronary arteries are re-occluded and hearts are perfused with 5 mL 0.1% Evans blue dissolved in Krebs-Henseleit solution followed by a short rinsing (2 sec) with Krebs-Henseleit.
Slicing the hearts and TTC incubation Hearts are preferred to stain after slicing rather than perfusing
the heart with TTC. After delineation remove atria from the ventricles and slice the heart manually to 5-6 uniform slices (with equal thickness) perpendicular to the long axis of the left ventricle (LV) by eye. Use a 24-well microplate to incubate slices at 37°C for 10 min. Fill wells with 2 mL of 1% weight/volume TTC prepared in 0.1 M phosphate buffer (dissolve 7.12g Na2HPO4×2H2O (MW 178) in 400 mL and 1.56g NaH2PO4×2H2O (MW 120) in 100 mL distilled water, mix and set pH from 7.2 to 7.4 with Na2HPO4). Prior to slicing and TTC staining, hearts are stored overnight at -20°C because myocardial
20
tissue can be cut more easily when it is in a semi-frozen state and yesterdays’ hearts can be incubated all together using completely the same incubating conditions. After TTC staining slices are fixed with 10% formalin solution for 12 min, rinsed with PBS, and then scanned between glass plates. Glass plates preferred than plexiglas because glass can not be easily scratched which can worsen the quality of the scanned image.
Evaluation of the scanned pictures Cumulative planimetry appears to be superior and to more
accurately reflect the degree of tissue damage than manual dissection of stained from unstained tissue. Moreover, documentation and later control of the evaluation is also missed without computer based planimetry. There are several useful softwares.
InfarctSize 2.4™ software is a standard computer program with the usual picture editing functions specially developed to evaluate 2D scanned images of heart slices by Pharmahungary Group. Procedure:
2. Prepare Evans blue dye 3. Perfusate the heart with Evans blue to delineate area at risk 4. Incubate the heart in TTC to detect infarct size 5. Measure area at risk and infarct size with manual dissection 6. Express area at risk in % of the total heart mass 7. Express infarct size in % of the area at risk
21
Cleaning
After the experiment has been completed, the equipment should be thoroughly cleaned. It is important to remember that the solutions used to provide isolated organ or tissue preparations with nutrients will also provide an ideal environment for bacteria and fungal growth. Regular procedure of glassware maintenance and post experimental cleanup:
The apparatus is manufactured of heat-resistant borosilicate glass and can be easily cleaned. When the experiment is finished, remove heart and let the Krebs-Henseleit fluid run away the system. Then flush out carefully and accurately all of the components of the perfusion system (glasswares: reservoirs and chambers, stopcocks, aerators, cannulae, flowmeters, transducers, connectors and other associated parts) using 1 liter of deionized water. Repeat this step 4 times. The last cycle should be done with boiling distilled water. After the final water rinse, disassemble the perfusion system and let all the cleaning water run away. Aerators should be carefully blown dry using gas or air. Regularly clean the top and fixing bolts using distilled water to avoid the formation of saline deposits.
Covering equipment to reduce air borne contamination from microbes and spores is useful. Last steps:
Switch off thermostat Close carbogen flow Wash up hand tools Take care (hazardous) waste material
22
References
Csonka C, Kupai K, Kocsis GF, Novák G, Fekete V, Bencsik P, Csont T, Ferdinandy P. Measurement of myocardial infarct size in preclinical studies. J Pharmacol Toxicol Methods. 61:163-70. (2010) Review.
DIRECTIVE 2010/63/EU OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL on the protection of animals used for scientific purposes
Hearse DJ, Sutherland FJ. Experimental models for the study of cardiovascular function and disease. Pharmacol Res. 41:597-603. (2000)Review.
García-Manzano A, González-Llaven J, Lemini C, Rubio-Póo C. Standardization of rat blood clotting tests with reagents used for humans. Proc West Pharmacol Soc. 44:153-5. (2001)
Krebs, H. A. and Henseleit, K. Untersuchungen über die Harnstoffbildung im Tierkörper. Hoppe-Seyler's Zeitschrift für Physiol. Chemie. 210, 33-66. (1932)
Langendorff O. Untersuchungen am uberlebenden Saugethierherzen. Pflugers Archives fur die Gesamte Physiologie des Menschen and der Tiere 61:291-332. (1895)
Neely JR, Liebermeister H, Battersby EJ and Morgan HE. Effect of pressure development on oxygen consumption by isolated rat heart. American Journal of Physiology 212:H804-H814. (1967)
Sutherland FJ, Hearse DJ. The isolated blood and perfusion fluid perfused heart. Pharmacol Res. 41:613-27. (2000) Review.
Zimmer HG. The Isolated Perfused Heart and Its Pioneers. News Physiol Sci. 13:203-210. (1998)