52
Diabetes Mellitus and metabolic syndrome
Diabetes Mellitus and metabolic syndrome

Metabolic syndrome
Insulin Resistance Syndrome
Glucose Intolerance
Dyslipidemia Hypertension
Endothelial dysfunction Macrovascular disease
Dysfibrinolysis
Metabolic syndrome• Identified insulin resistance subjects• Identified high risk for develop T2 DM• Identified high risk for CVD
IDF(2005) criteria• Abdominal obesity (Ethnic specific)– Waist >102 cm (men), >88 cm (women)– Waist >90 cm (m), >80 cm (w) Asian
• Hypertriglyceridemia > 150 mg/dl• HDL <40 mg/dl (men); < 50 mg/dl (women)• Hypertension 130/85 mmHg≥• Fasting hyperglycemia (serum) 100 mg/dl≥
“Plus 2 of the following”
Pre-diabetic stages• Impaired glucose tolerance
– 2 hrs OGTT: 140<IGT<200• Impaired fasting glucose
– Fasting plasma: 100<IFG<126
Diabetes Mellitus
Symtoms• Asymtomatic(~50%)• Polyurea• Acute complication ex DKA, Focal
seizure, Coma.• Chronic complication

Diagnosis• Symptoms + Plasma glucose>=200 mg%• Fasting plasma glucose>=126 mg%• 75 gm OGTT
– 2 hr plasma glucose > =200 mg%
Diagnosis• Repeat 1 time after abnormal of the first
test.• Except, in case of hyperglycemia with
acute diabetic complication

Diabetes classification• Primary diabetes
– Type 1 diabetes– Type 2 diabetes
• Secondary diabetes

Diabetes classification• Secondary diabetes
– Pancreatic Diabetes– Endocrine disorder ex Hyperthyroidism
,Cushing’s syndrom, Primary hyperaldosteronism, Acromegary, Pheochromocytoma, Glucagonnoma.

Diabetes classification• Secondary diabetes
– Drug ex Glucocorticoid, B-adrenergic blocked, thiazide diuretic
– Other ex genetic syndrome, Insulin antibody

Type 1 diabetes• Acute onset• Ketoacidosis pone• Thin• Young age• Need insulin treatment

Type 2 diabetes• Slow onset• Ketoacidosis resistance• Norma weight or obese• Middle to old age• Response to oral hypoglycemic agent

Pathogenesis• Type 1 diabetes• Type 2 diabetes

Pathogenesis of type 1 DM
Pathogenesis of type 1 DM
Islet cell auto antibody
Pathogenesis of type 1 DM
Islet cell auto antibody
Destruction of Islet cell

Pathogenesis of type 1 DM
Islet cell auto antibody
Destruction of Islet cell
Insulin deficiency
Pathogenesis of type 1 DM
Islet cell auto antibody
Destruction of Islet cell
Insulin deficiency
Host Factor

Pathogenesis of type 1 DM
Islet cell auto antibody
Destruction of Islet cell
Insulin deficiency
Host Factor Precipitating Factor
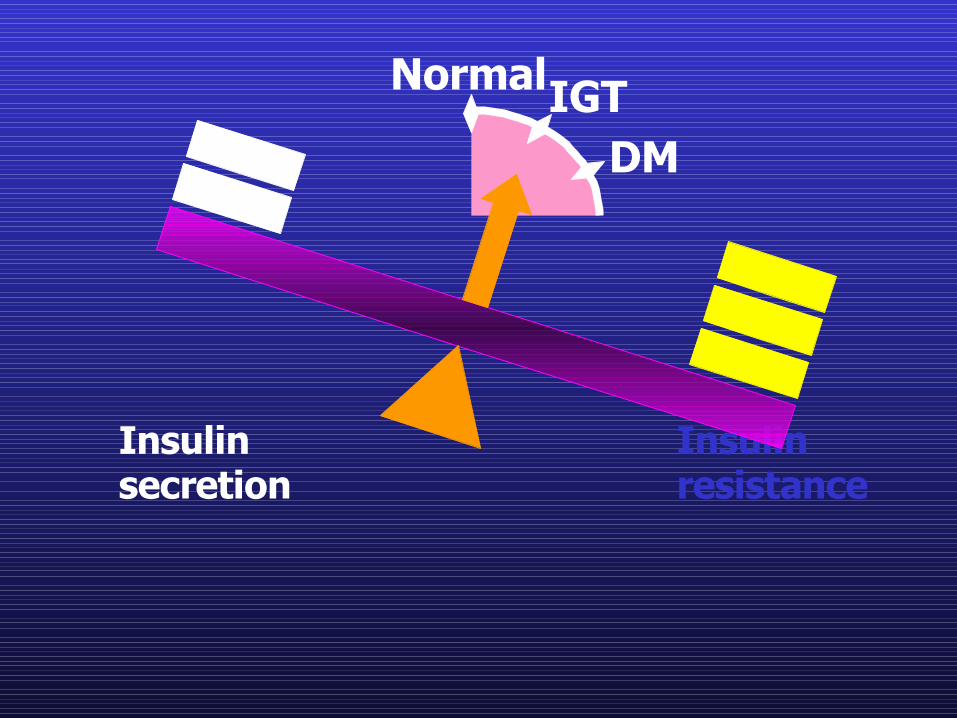
Pathogenesis of type 2 DM
Insulin resistance is an etiology of type 2 DM

Insulin Resistance• A core defect in type 2 diabetes – 92% of
patients with type 2 diabetes have insulin resistance
• Definition: Impaired response to the physiological effects of insulin, including those on glucose, lipid, protein metabolism and vascular endothelial functionHaffner SM, et al. Diabetes Care, 1999
Consensus Development Conference of the American Diabetes Association, Diabetes Care, 1997
Emerging Strategies Emerging Strategies
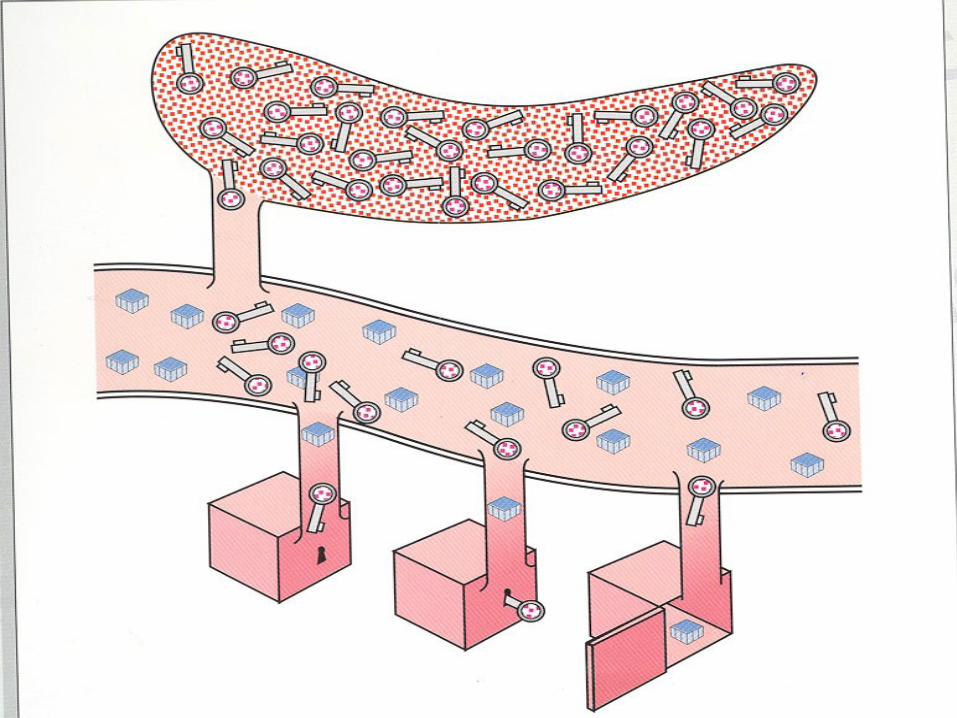

• Insulin acts like a key
• Sugar get into cell
• Lower blood sugar to normal

NormalIGTDM
Insulin secretion
Insulin resistance

NormalIGTDM
Insulin secretion
Insulin resistance
Insulin secretion
Insulin resistance
NormalIGTDM
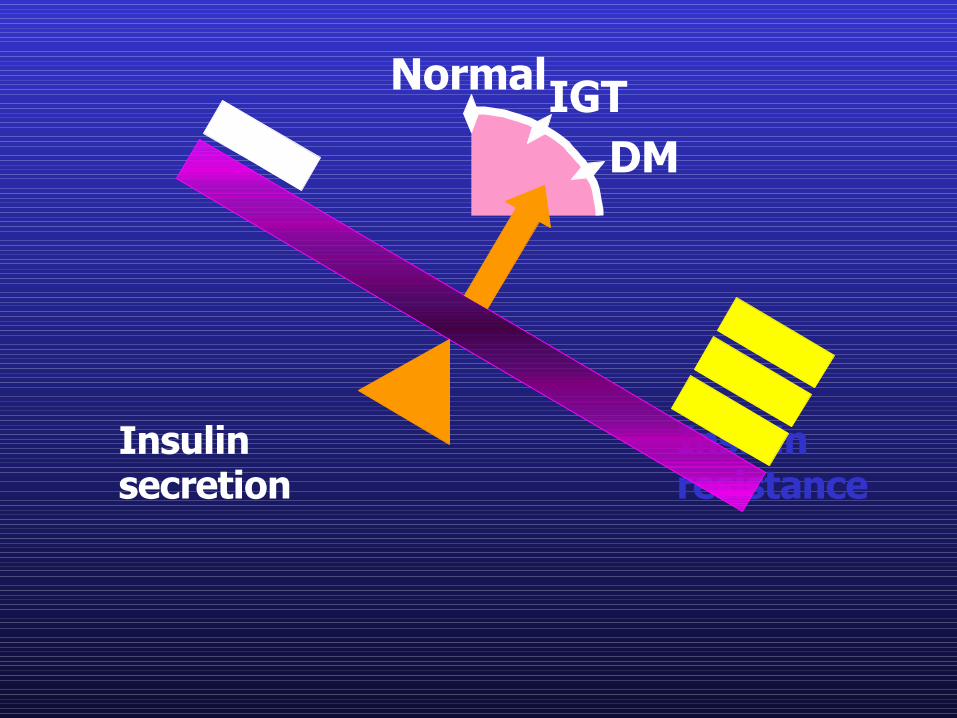
Insulin secretion
Insulin resistance
NormalIGTDM

Diabetic complication• Acute diabetic complication• Chronic diabetic complication

Acute complication• Diabetic Ketoacidosis (DKA)• Hyperosmolar non-ketotic coma (HNKC)• Focal hyperglycemic seizure

Diabetic Ketoacidosis• Severe hyperglycemia (plasma glucose
>300 mg%)• Ketoacidosis
– Wide anion gap metabolic acidosis– Positive serum ketone
Hyperosmolar non-ketotic coma• Very severe hyperglycemia( plasma
glucose> 600 mg%)• Neurological change• Severe hyperosmolarity (serum
osmole>320mOsm/l)• No ketoacidosis

Focal hyperglycemic seizure• Severe hyperglycemia( plasma glucose>
300 mg%)• Seizure mostly focal seizure• Mild Hyperosmolarity (serum osmole
290-310mOsm/l)• No ketoacidosis

Chronic complication• Macrovascular complication• Microvascular complication
– Diabetic retinopathy– Diabetic nephropathy
• Diabetic neuropathy

National Diabetes Data Group. Diabetes in America. 2nd ed. NIH;1995.
Atherosclerosis in Diabetes
• ~80% of all diabetic mortality– 75% from coronary atherosclerosis– 25% from cerebral or peripheral
vascular disease• >75% of all hospitalizations for diabetic
complications

0
2
4
6
8
10
12
14
16
18
Annual
CH
D D
eath
s per
1000 P
erso
ns
Kannel WB, McGee DL. JAMA 1979;241:2035-2038.
Framingham Study: DM and CHD Mortality
20-Year Follow-up1717
88
1717
44
MenMen WomenWomen
DMDM
Non-DMNon-DM
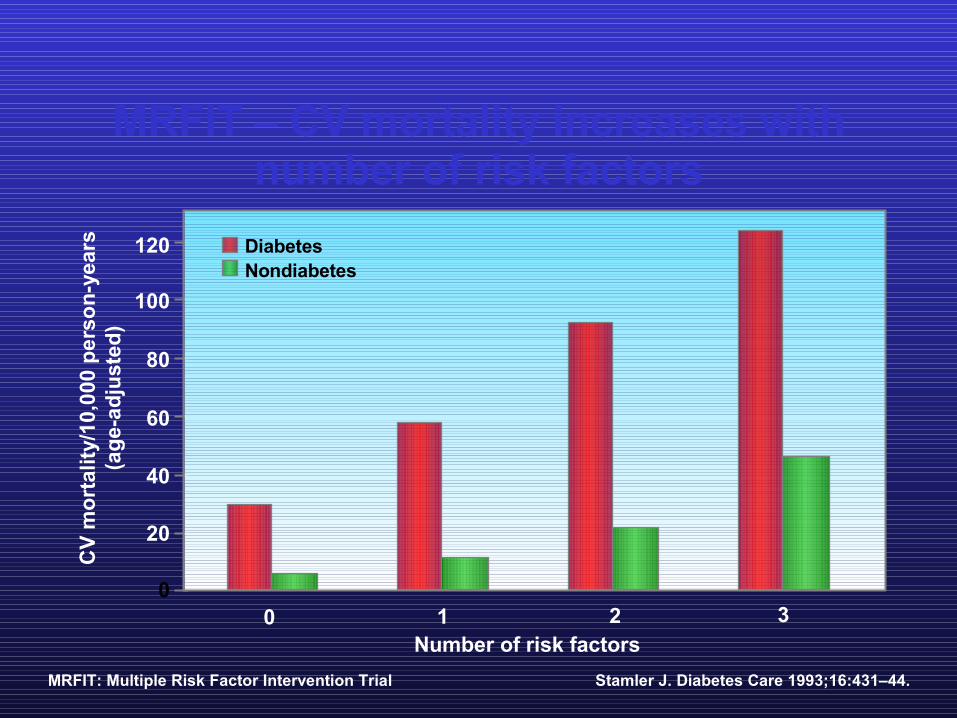
MRFIT – CV mortality increases withnumber of risk factors
120
100
80
60
40
20
0
Stamler J. Diabetes Care 1993;16:431–44.
Number of risk factors
CV
mor
talit
y/10
,000
per
son-
year
s(a
ge-a
djus
ted)
0 1 2 3
DiabetesNondiabetes
MRFIT: Multiple Risk Factor Intervention Trial

Thrombosis
PAI-1
Fibrinogen
C-reactiveprotein
FFADyslipidaemiaVLDL ( triglycerides)
HDL
Obesity
TNF-α
Lipaemia
Advanced glycation
end products
Geneticpredisposition
Hypertension
Hyper-insulinaemia
Pancreas
Liver
Adipo-cytes
Skeletal muscles
Glycatedprotein
Hyperglycaemia
Insulin resistance FFA
Libby P, et al. Circulation 2002;106:2760–63.FFA: free fatty acid; HDL: high-density lipoprotein, PAI: plasminogen activator inhibitor, TNF: tumour necrosis factor, VLDL: very low-density lipoprotein
Multiple mechanisms of vascular damage associated with dysglycaemia

Diabetic retinopathy• Most common cause of blindness in
developed country• Recommended to screen by fundoscopic
exam every year.• Improve glycemic and hypertensive control
are the best method to prevent DR

Diabetic retinopathy• Classification
– Non-proliferative DR– Proliferative DR– Proliferative DR with vitreous
Hemorrage or retinal detachment

Screening• Annual test for
– Type 1: duration more than 5 years– Type 2: ALL– Plan for or during pregnancy
Diabetic nephropathy• Most common cause of ESRD in developed
country• Recommended to screen urine for
microalbumin every year• Improve glycemic and hypertension
control are the best method to prevent DN

Diabetic nephropathy• Classification
– Microalbuminuria (30-300mg/day)– Macroalbuminuria( > 300 mg/day)– Renal insufficiency (serum Cr >2 mg/dl)– ESRD
Screening• Annual test for
– Type 1: duration more than 5 years– Type 2: ALL– Plan for or during pregnancy

Diabetic neuropathy• Discomfort and lead to serious
compliaction such as amputation.• Recommended to screening by test pinpick
and vibration sensation very year. However, those tests are not early diagnostic test.

Diabetic neuropathy• Distal Symmetrical Polyneuropathy• Autonomic neuropathy: postural
hypotension, neurogenic bladder, gastroparesis, diarrhea, impotent.
• Focal and multifocal neuropathy

Management• Diet control• Diabetic education• Drug
– Oral hypoglycemic agents– Insulin

Follow up• Glycemic control
– FPG– Glycosylated protein
• Fructosamine: 2-3 weeks• Hb a1c:2-3 months
Follow up• Chronic complication screening
– Urine microalbuminemia– Fundoscope– Sensation test– Lipid– EKG

















