60
Diagnosis and Treatment of Invasive Candida Infections in Neonates and Children AHD October 11, 2012 Rupesh Chawla MD MSc FRCPC Clinical Assistant Professor Alberta Children’s Hospital
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | quentin-oscar-jefferson |
| View: | 215 times |
| Download: | 1 times |

Diagnosis and Treatment of Invasive Candida Infections in Neonates and
Children
AHD October 11, 2012Rupesh Chawla MD MSc FRCPC
Clinical Assistant ProfessorAlberta Children’s Hospital

Questions
• 1. Which Candida species is found more commonly in neonates and children compared to adults?
• A. Candida albicans• B. Candida glabrata• C. Candida krusei• D. Candida parapsilosis• E. Candida tropicalis

Questions
• 2. What is the sensitivity of blood culture to detect candidemia?
• A. > 90%• B. 80-90%• C. 70-80%• D. 60-70%• E. 50-60%• F. < 50%

Questions
• 3. Which antifungal should not be used in neonates if there is urinary tract involvement?
• A. Conventional Amphotericin B• B. Fluconazole• C. Liposomal Amphotericin B• D. Flucytosine

Outline
• 1. To describe the epidemiology of Invasive Candida Infections (ICI) in neonates and pediatric patients
• 2. To describe existing and possible future diagnostic techniques for Candida infections
• 3. To outline the current recommended treatment strategies in neonates and pediatric patients for ICI

Epidemiology

Epidemiology• Candida infections are the leading cause of
invasive fungal infections (IFI) in hospitalized patients
• Candida are the third most common isolate recovered from pediatric (and neonatal) cases of nosocomial bloodstream infection in the United States
• Fungal infections possess the second highest case fatality rate among all causes of sepsis in children
• C. albicans has been associated with high rates of mortality (47% adults vs. 29% children vs. 20-50% neonates) Wisplinghoff H et al. Pediatr Infect Dis J. 2003:686-91
Watson S et al. Am J Respir Crit Care Med. 2003:695-701Kaufman D Semin Perinatol. 2003:414-24 Pappas PG et al. Clin Infect Dis. 2003:634-43

Epidemiology
• Candidemia is frequently associated with signs and symptoms of a sepsis syndrome
• A study on the epidemiology of sepsis revealed that in the cases of sepsis caused by fungal organisms has increased by 207% between 1979 and 2000– Likely related to an increase in prevalence of
susceptible hosts (intensive care, immunosuppressive therapy, broad spectrum antibiotics)
Pappas PG et al. Clin Infect Dis 2009:503-35Martin GS et al. N Engl J Med 2003:1546-54

Epidemiology
• A study looking at pediatric patients in the United States in 2000 revealed Candidemia:– Occurred at a frequency of 43 cases/100,000
admissions (95% CI, 35-52 cases)– Was associated with a 10.0% increase in mortality
(95% CI, 6.2%-13.8%), 15% in neonates– A mean 21.1 day increase in length of stay (95%
CI, 14.4-27.8 days)– A mean increase in total per-pt hospital charge of
$92,266 (95% CI, $65,058-$119,474)Zaoutis T et al. Clin Infect Dis 2005:1232-9Morgan J et al. Infect Control Hosp Epidemiol 2005:540-7

Epidemiology
Candida species– There has a been a recent shift from Candida
albicans to non-albicans species of Candida as the dominant causative agent
Rangel-Frausto MS et al. Clin Infect Dis. 1999:253-8Yamamura DL et al. Canadian Med Assoc J. 1999:493-9Viscoli C et al. Clin Infect Dis 1999:1071-9Nguyen MH et sl. Am J Med. 1996:613-7Macdonald L et al. Clin Infect Dis. 1998:642-5Zaoutis TE et al. Pediatr Infect Dis J. 2004:635-41Pfaller MA et al. Clin Microbiol Rev. 2007:133-63Singhi S et al. Indian J Pediatr. 2009:1033-44 Horn DL et al. Clin Infect Dis. 2009:1695-703

Invasive Candidiasis (IC) PATH ALLIANCE: 2019 adult and pediatric pts from
23 North American centers• Patient Categories*:
– General Medicine 66.3%– Surgical (Non-Transplant) 32.8%– Solid Tumor 17.4%– Hematologic Malignancy 9.8%– Solid Organ Transplant 8.2%– Stem Cell Transplant 2.9%– HIV/AIDS 2.0%– Neonatal ICU 1.3%
* Categories were not mutually exclusiveHorn DL et al. Clin Infect Dis. 2009:1695-703Pathnet 2004-8 data

Distribution of Candida species
• C. albicans: 45.6%• C. glabrata: 26.0%• C. parapsilosis: 15.7%• C. tropicalis: 8.1%• C. krusei: 2.5%• C. lusitaniae: 0.8%• C. guillermondii: 0.2%• C. dubliniensis: 0.3%• Other/unknown: 0.7%
Pathnet 2004-8 dataN= 2019 episodes of Candidemia

Candida species• Pt population effects species distribution• C. parapsilosis had lowest mortality (23.7%) and were less
likely to be:– Neutropenic (5.1%)– Receive corticosteroids (33.5%)– Receive other immunosuppressants (7.9%)
• C. krusei had highest mortality (52.9%) and more commonly:– Prior use of antifungal (70.6%)– Hematologic malignancy (52.9%)– Stem cell transplantation (17.7%)– Neutropenic (45.1%)– Corticosteroid treatment (60.8%)
Horn DL et al. Clin Infect Dis. 2009:1695-703

Epidemiology
Candida species • Age group changes distribution in species of
Candida– C. albicans most common in all: 48% cases– C. parapsilosis more common in neonates (42%) and
children (38%) compared to adults (15%)– C. glabrata infrequent in neonates (9%) and children
(3%) compared to adults (17%)• Candidemia was attributed to vascular devices in
58% neonates, 70% children, and 44% adultsBlyth CC et al. Pediatrics. 2009:1360-8

Frequency of Isolation of Candida sp. Causing Candidemia Sepsis
Candida sp. All Patients Neonates
C. albicans 50 63
C. glabrata 24 6
C. tropicalis 12 <1
C. krusei 7 <1
C. parapsilosis 4 29
C. dubliniensis 1 <1
Other species 2 <2
% of Blood Culture Isolates
CID 29:253-8, 1999 & Crit Care Med 27:882-92, 1999
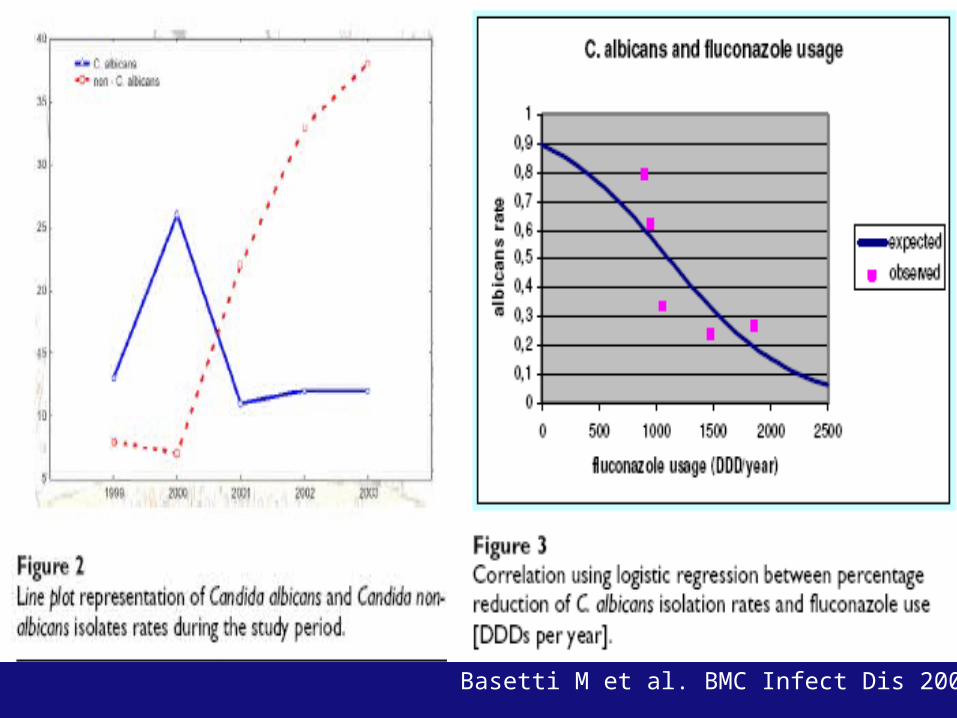
Basetti M et al. BMC Infect Dis 2006
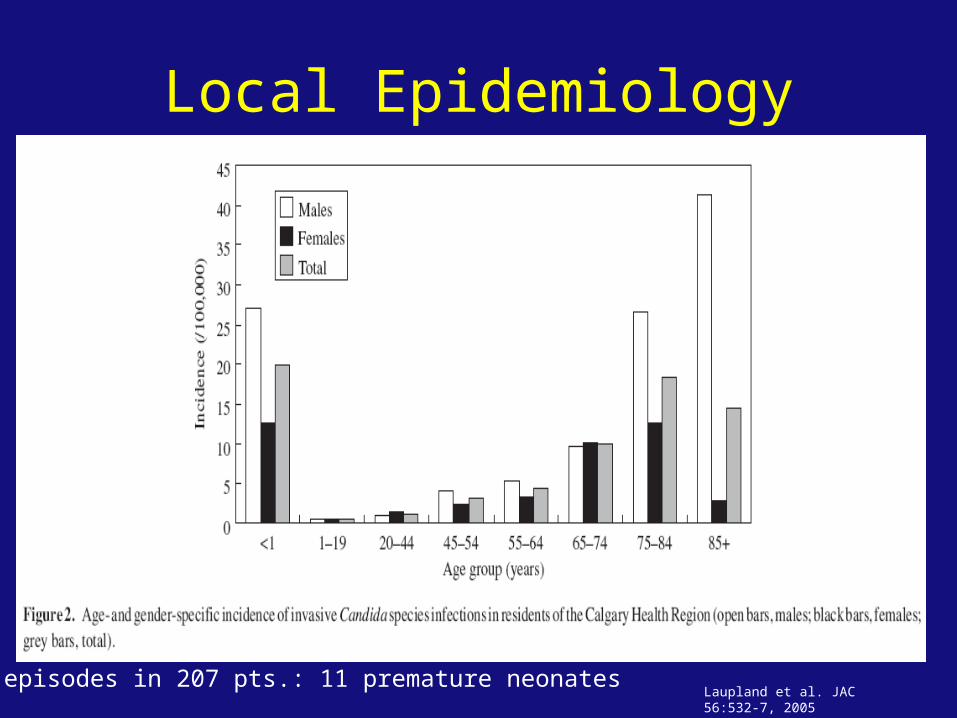
Local Epidemiology
Laupland et al. JAC 56:532-7, 2005209 episodes in 207 pts.: 11 premature neonates

Local Epidemiology
Laupland et al. JAC 56:532-7, 2005
Epidemiology
Candida species• Candida parapsilosis is a common pathogen in
neonates and children • Associated with catheter infection and parenteral
nutrition– Has affinity for foreign material and growth advantage
in TPN solutions• GI colonization occurs in higher rate in neonates• Transmission from HCW also suggested as
contributor as is commonly carried on hands of HCW
Pappas PG et al. Clin Infect Dis. 2003:634-43 Blyth CC et al. Pediatrics. 2009:1360-8
EpidemiologyRisk Factors Pediatric Patient• Use of broad spectrum antibiotics• Use of central venous catheters (CVC)• Total parenteral nutrition (TPN) use• Use of renal replacement therapy in ICU• Cardiac disease • Short Gut Syndrome• Neutropenia• Use of implantable prosthetic devices• Receipt of immunosuppresive agents (glucocorticoids,
chemotherapy agents, and immunomodulators)Pappas PG et al. Clin Infect Dis. 2009:503-35Macdonald L et al. Clin Infect Dis. 1998:642-5Stamos JK et al. Clin Infect Dis. 1995:571-5

EpidemiologyRisk Factors Neonates• Prematurity (especially Gestational Age <28 weeks)• VLBW (<1500 grams)• High burden of colonization with Candida sp• Shock, DIC• Hyperglycemia• Necrotizing Enterocolitis (NEC), abdominal surgery, spontaneous intestinal
perforation• Cardiac surgery• Prior use of intralipid, TPN• Central Venous catheter• Prolonged broad spectrum antibiotic Rx• Neutropenia or use of immunosuppresive agents (steroid Rx)• H2 blockers• Intubation and or tracheostomy• Length of stay > 7 days before candidemia
Weese-Mayer DE et al. Pediatr infect Dis J. 1987:190-6Saiman L et al. Pediatr Infect Dis J. 2000:319-24


Diagnosis

Diagnosis
• Early diagnosis is difficult– Non-specific clinical signs and symptoms– Invasive diagnostic procedures are risky– There is a lack of sensitive, minimally invasive
assays

Diagnosis
• Antifungal therapy is initiated when Candida is recovered from:– Blood cultures– Usually sterile body fluids– Abscesses or wounds (burns, GI surgery)
• This may be too late

Time to Therapy: Mortality
Delay in treatment is an independent determinant of hospital mortality
All pt (N=157) Delay, 33.1% No Delay 11.1%
Morrell et al. Antimicrob Agents Chemother. 2005:3640-5

Relationship between hospital mortality and the number of days to initiation of fluconazole therapy.
Garey K W et al. Clin Infect Dis. 2006;43:25-31
© 2006 by the Infectious Diseases Society of America

Diagnosis
• Lab Aids in the Diagnosis of ICI– Microscopy– Culture– PCR– Serology

Patterns of Diagnostic Test Usage: PATH Alliance, 2008
Method of Diagnosis
Candida(N=4,623)
Aspergillus(N=745)
Zygomycetes(N=85)
GM assay 35.6%
CXR 1.0% 16.6% 15.4%
BG test 0.5% 0.7%
CT scan 6.3% 52.6% 40.0%
Culture 99.7% 74.9% 85.9%
Histopathology 3.5% 25.5% 67.4%
PCR <0.1% 6.0%
Horn DL et al. Clin Infect Dis. 2009:1695-703Pathnet 2004-8 data
Diagnostic Strategies• Cultures
– Blood, urine, other body fluids• Candida blood cultures
– < 10% + in pts with hepatosplenic candidiasis– ~60% + with 2 or more organs involved at autopsy
• Serology • Imaging
– CT, MRI (for hepatosplenic candidiasis)• Dilated eye exam
– 4-5% with candidemia have eye involvement

Diagnosis
• Candida blood cultures: sensitivity likely in the range of 50-60% from autopsy studies
• Time to positivity is also an issue• Early empiric therapy is key• Rapid diagnostic tests may help but not quite
ready for prime time

Diagnosis:Commercially Available Non-Culture
Methods
• Serologic Techniques– Beta-D-glucan– Mannan plus antimannan
• PCR– SeptiFast

(13) -D-Glucan as a Marker for Invasive Mycosis
• Cell wall component of yeast and filamentous fungi
• Amebocyte lysate assay• Does detect:
– Aspergillus,Candida, Fusarium,Trichosporon, Saccharomyces, and Acremonium
• Does not detect:– Cryptococcus, Zygomycetes

(13) -D-Glucan as a Marker for Invasive Mycosis
• Sensitivity for IFI 63-100%• Specificity for IFI 76-100%
• In a 6 yr autopsy based study it detected 10/12=83.3% Candida
• In another study in known serum/plasma samples it was + in 87% of pts with Candidemia Ostrosky-Zeichner J Inv Fungal Infect. 2008:42-5
Obayashi et al. Clin Infect Dis. 2008:1864-70Pickering et al. J Clin Microb. 2005:5957-62

Combined Mannan/ Anti-Mannan for Diagnosis of IC
• Platelia anti-mannan and mannan EIA– Anti-mannan EIA detects Ab to both alpha and
beta epitopes– Mannan EIA detects alpha mannan
• Simultaneous detection of Ag and AB result in sensitivity of 80-95% and specificity of 53-95%
• At least twice weekly monitoring is required for optimal performance
Mycosis 2002;45:455-60JCM 2002;51:433-42

PCR for the Diagnosis of Invasive Candidiasis
• Potential target: conserved area of 18S ribosomal RNA gene
• Potential pan-fungus screening tool• Potential for use in serial screening (early
diagnosis)• Sensitivity and specificity vary by assay and
sample type NOT READY for PRIMETIME
PCR for the Diagnosis of Invasive Candidiasis
• SeptiFast (Roche)• Real time multiplex PCR using LightCycler• Whole blood• Detects and IDs 20 most common clinically
relevant pathogens (14 bacteria and 6 fungi)• Fungi detected: C. albicans, C. glabrata, C.
tropicalis, C. parapsilosis, C. krusei, A. fumigatus

PCR for the Diagnosis of Invasive Candidiasis
• Sensitivity for Candidemia 31-75%: marginal at best
• Multicenter blinded challenge studies essential
• Better clinical studies needed• What does DNAemia mean?

Pediatric Data on Non-Culture Methods
• (13) -D-Glucan – Data in Pediatric pts suggests cut off value could be higher than
in adults :• 120 non-immunocompromised pts (mean age 9.2 yrs)• Neonates excluded• Mean value 68 pg/ml (adults 48 pg/ml)
– Study of pediatric cancer patients with mucosal colonization with Candida species
• Did not give rise to diagnostically significant levels of Candida mannan or Candida DNA in serum specimens.
• -D-Glucan values may be higher than the cut-off value in some pediatric patients without clinical evidence of ICI (higher than currently recommended cut-off value of ≥80 pg/ml)
• Suggests the utility of Candida mannan or Candida DNA in the diagnosis of ICI, however, the -D-Glucan levels in pediatric cancer subjects should be interpreted with caution.
Smith PB et al. Clin Vaccine Immunol 2007:924-5Mokaddas E et al. BMC Infect Dis 2010:292

Pediatric Data on Non-Culture Methods
• Mannan/Antimannan assay– Platelia Candida antigen kit in 70 of 184 pre-term
infants admitted to a NICU between March 2004 and March 2006
• Frequency of confirmed candidemia was 6.5% • Assay sensitivity 94.4%, specificity 94.2%, PPV 85% and NPV
98%– However in another study:
• 6 pediatric pts with prolonged ICU stay and a birth weight of 400-1320 g
• 5/6 positive results with Platelia ELISA. All positive results in this group of patients are considered as false positive (83.3%).
Oliveri S et al. Clin Microbiol Infect.2008:391-3Siemann M et al. Mycoses. 1998:373-7

Treatment

Treatment
• Clinical Practice Guidelines for the Management of Candidiasis: 2009 Update by the Infectious Disease Society of America
• Excellent Resource
Pappas PG et al. Clin Infect Dis 2009:503-35

IDSA Grading System for ranking recommendations in clinical guidelinesCategory, grade Definition
Strength of recommendationA Good evidence to support
recommendation for/against use
B Moderate evidence to support recommendation for/against use
C Poor evidence to support recommendation
Quality of evidenceI Evidence from 1 proper RCTII Evidence from 1 well designed clinical trial
(without randomization)III Evidence from opinion of respected
authorities (clinical experience, descriptive studies, or reports of expert committees)

Treatment: Neonates
• Ampho B (1 mg/kg daily) for disseminated candidasis (A-II)
• If urinary tract involvement is excluded Liposomal Ampho B (3-5 mg/kg daily) can be used (B-II)
• Fluconazole is a reasonable alternative (12 mg/kg daily) (B-II)
• Recommended length of therapy 3 weeks
Pappas PG et al. Clin Infect Dis 2009:503-35

Treatment: Neonates• Lumbar puncture and dilated retinal exam recommended
with neonates with positive sterile body fluid and/or urine cultures (B-III)– CNS involvement usually manifests as meningoencephalitis and
should be assumed with high incidence of this complication– Role of flucytosine with Candida meningitis not routinely
recommended• Imaging of GU tract, liver, and spleen should be performed
if sterile body fluid culture persistently positive (B-III)• Intravascular catheter removal strongly recommended (A-
II)• Echinocandins used with caution (only with resistance or
toxicity issues) (B-III)• Consider prophylaxis with fluconazole in nurseries with
high rates of ICI in high risk neonates (A-I)Pappas PG et al. Clin Infect Dis 2009:503-35
Treatment: PediatricNonNeutropenic Patient
• Fluconazole or an echinocandin as initial therapy (A-I)– Echinocandin: moderately severe to severe illness or
recent azole exposure (A-III)– Fluconazole: mild to moderate illness and no recent
azole exposure• Transition to Fluconazole for pt with isolate likely
to be susceptible (A-II)• C. glabrata echinocandin preferred (B-III)• C. parapsilosis fluconazole recommended (B-III)
Pappas PG et al. Clin Infect Dis 2009:503-35

Treatment: PediatricNonNeutropenic Patient
• Ampho B or Liposomal Ampho B if intolerance or limited availability of other agents (A-I)
• Recommended duration without metastatic complications is 2 weeks after documented clearance of Candida from bloodstream (A-III)
• CVC removal strongly recommended (A-II)• Dilated fundoscopy within 1st week of therapy
Pappas PG et al. Clin Infect Dis 2009:503-35

Treatment: PediatricNonNeutropenic Patient
• Empirical therapy for suspected ICI– Same as treatment (B-III)– Should be considered in critically ill pts with risk
factors of ICI and no other cause of fever, based on clinical assessment of risk factors, serologic markers for ICI, and/or culture data from nonsterile sites (B-III)
Pappas PG et al. Clin Infect Dis 2009:503-35

Treatment: PediatricNeutropenic Patient
• Echinocandin or Liposomal Ampho B (A-II) recommended for most pts
• Fluconazole for less critically ill and no recent azole exposure reasonable (B-III)
• Voriconazole if additional mold coverage desired (B-III)
• C. glabrata echinocandin preferred (B-III), Liposomal Ampho B (more cost and toxicity)(B-III)
• C. parapsilosis fluconazole or Liposomal Ampho B recommended (B-III)
Pappas PG et al. Clin Infect Dis 2009:503-35

Treatment: PediatricNeutropenic Patient
• C. krusei echinocandin, Liposomal Ampho B or Voriconazole (B-III)
• Duration without persistent fungemia or metastatic focus 2 weeks after clearance from bloodstream, resolution of symptoms of candidemia, and resolution of neutropenia (A-III)
• CVC removal should be considered (B-III)
Pappas PG et al. Clin Infect Dis 2009:503-35

Treatment: PediatricNeutropenic Patient
Empiric for suspected ICI• Liposomal Ampho B (A-I), Caspofungin (A-I), or
Voriconazole (B-I) recommended• Fluconazole and Itraconazole alternative (B-I)• Ampho B alternative but higher toxicity (A-I)• Azoles should not be used for empirical Rx if
azole received for prophylaxis (B-II)
Pappas PG et al. Clin Infect Dis 2009:503-35

Summary
• 1. Candida sp. are a significant cause of bloodstream infections in neonates and pediatric patients
• 2. Early diagnosis of infections with Candida is crucial to reduce mortality but is currently limited and therefore it is important to maintain a high index of suspicion and consider empirical therapy
• 3. Treatment of Candida infections depends on age, severity of illness and previous exposure to previous antifungals (prophylaxis)

Questions and Comments??

Questions
• 1. Which Candida species is found more commonly in neonates and children compared to adults?
• A. Candida albicans• B. Candida glabrata• C. Candida krusei• D. Candida parapsilosis• E. Candida tropicalis

Questions
• 2. What is the sensitivity of blood culture to detect candidemia?
• A. > 90%• B. 80-90%• C. 70-80%• D. 60-70%• E. 50-60%• F. < 50%

Questions
• 3. Which antifungal should not be used in neonates if there is urinary tract involvement?
• A. Conventional Amphotericin B• B. Fluconazole• C. Liposomal Amphotericin B• D. Flucytosine

Extra Slides

Epidemiology
Risk Factors in PICU Patients• Presence of CVC: OR 30.4 (95% CI, 7.7-119.5)• Malignancy: OR 4.0 (95% CI, 1.23-13.1)• Vancomycin use > 3 days in prior 2 weeks: OR
6.2 (95% CI, 2.4-16)• Anaerobic antimicrobial use > 3 days in prior 2
weeks: OR 3.5 (95% CI, 1.5-8.4)
Zaoutis TE et al. Clin Infect Dis. 2010:e38-45

Combination Therapy for Candida
• No difference in primary endpoints
• Secondary endpoints– faster clearance
• Secondary analysis:– Difference in
intermediate APACHE range

Combination Therapy for Candida
• International, open-label, noncomparative, clinical trial of micafungin alone and in combination for treatment of newly diagnosed and refractory candidemia.Ostrosky-Zeichner L, Kontoyiannis D, Raffalli J, Mullane KM, Vazquez J, Anaissie EJ, Lipton J, Jacobs P, van Rensburg JH, Rex JH, Lau W, Facklam D, Buell DN.Eur J Clin Microbiol Infect Dis. 2005 Oct;24(10):654-61.
• No difference

















