Diagnosis and Treatment of Painful Neuropathies and Nerve Entrapment Syndromes Michel Kliot MD, Professor Northwestern University Feinberg School of Medicine Director, Peripheral Nerve Center
Transcript
Diagnosis and Treatment of Painful Neuropathies and Nerve Entrapment Syndromes
Michel Kliot MD, ProfessorNorthwestern University Feinberg School of Medicine Director, Peripheral Nerve Center
Neuropathic Pain Treatment
Daniela Maria Menichella MD/PhDDepartment of NeurologyNorthwestern University Feinberg School of MedicineChicago, IL
Pain is the most common symptom
• Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage (external or internal to the body stimulus)
• Acute Pain: Associated with a stimulus (eg pinprick, flame) and subsides after stimulus removed
• Chronic Pain: Outlasts the stimulus and healing process
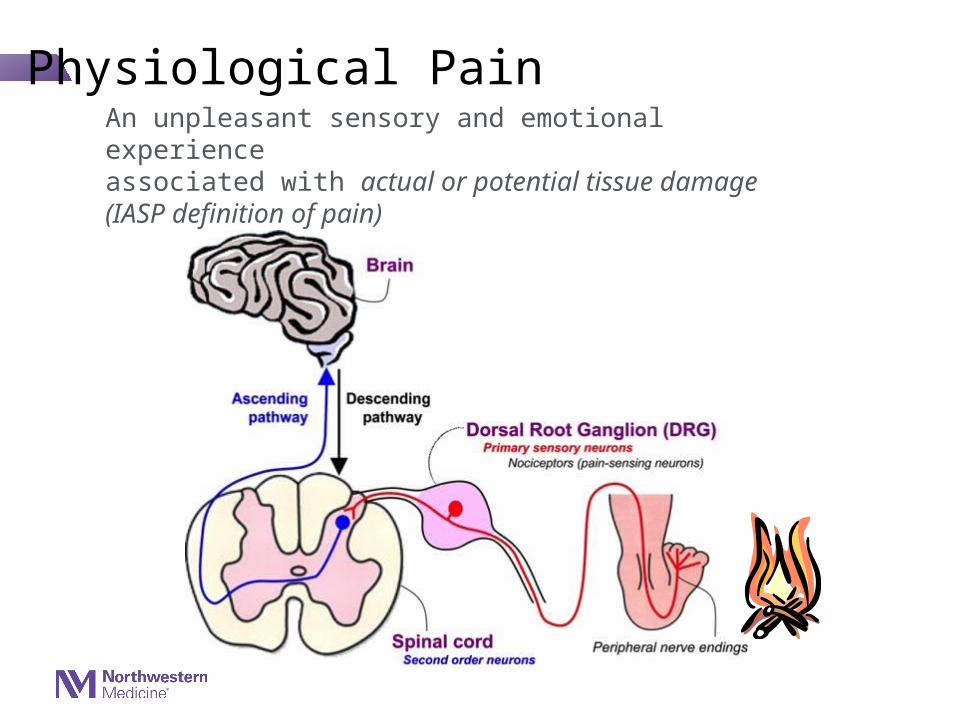
Physiological PainAn unpleasant sensory and emotional experience associated with actual or potential tissue damage(IASP definition of pain)
• Nociceptive Pain
• Inflammatory Pain
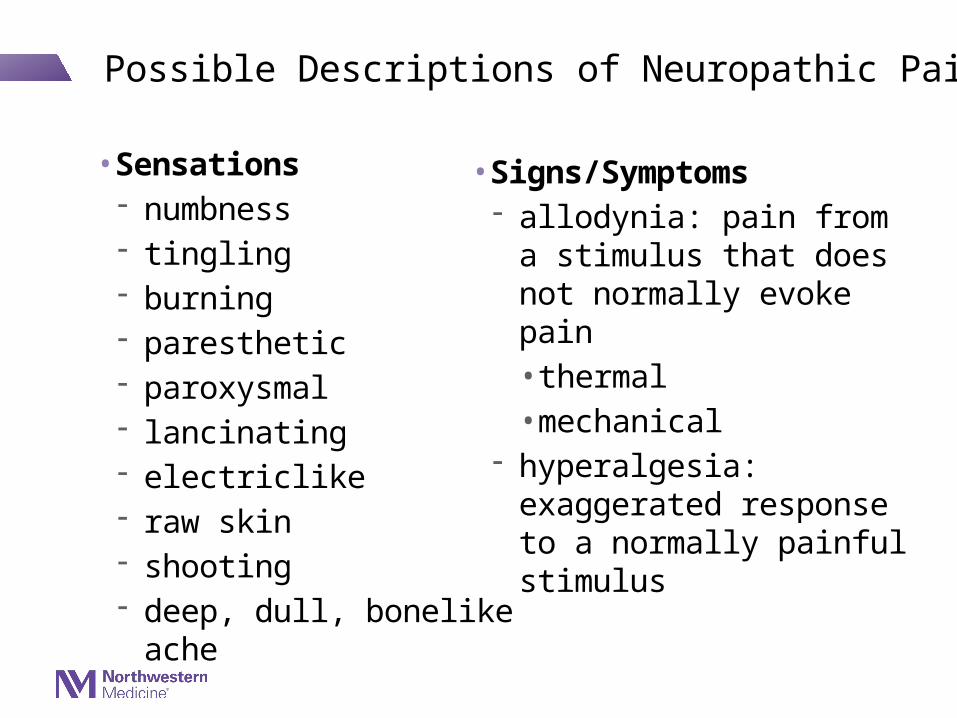
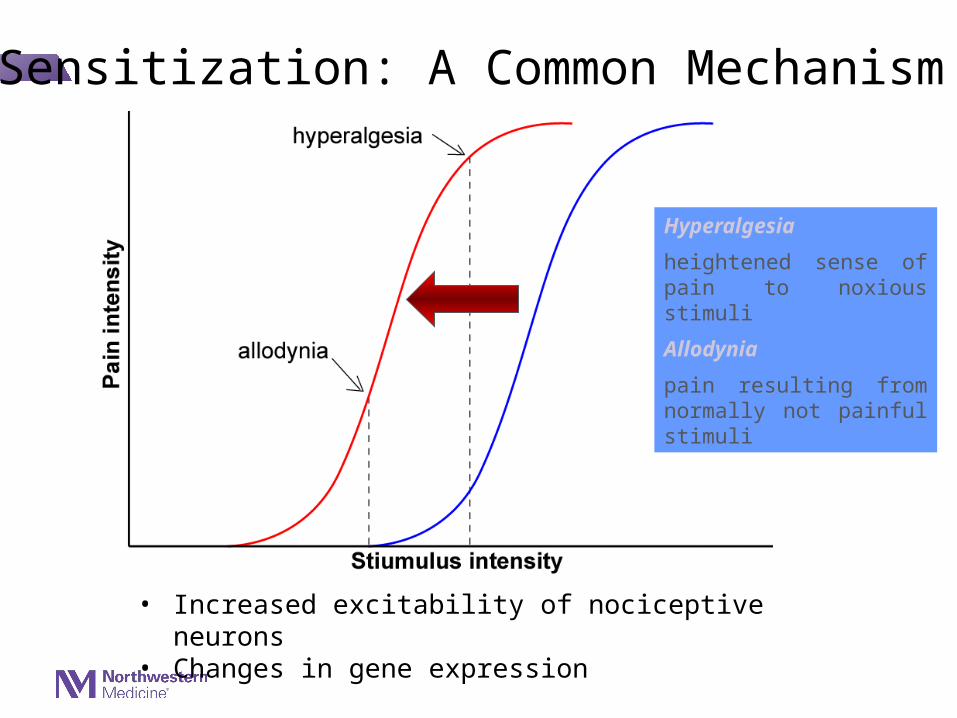
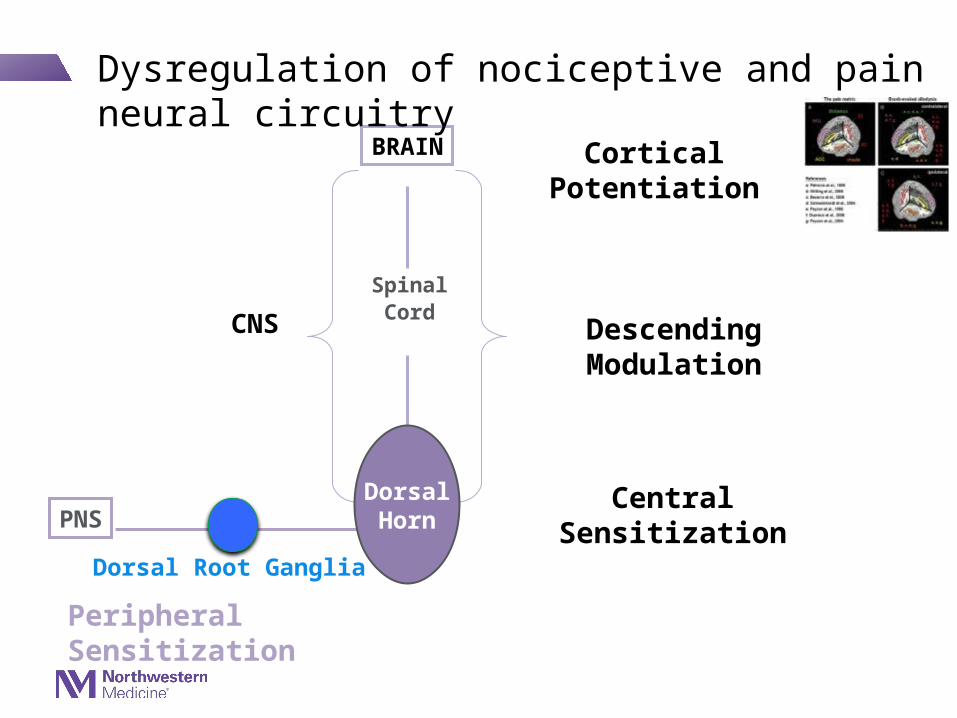
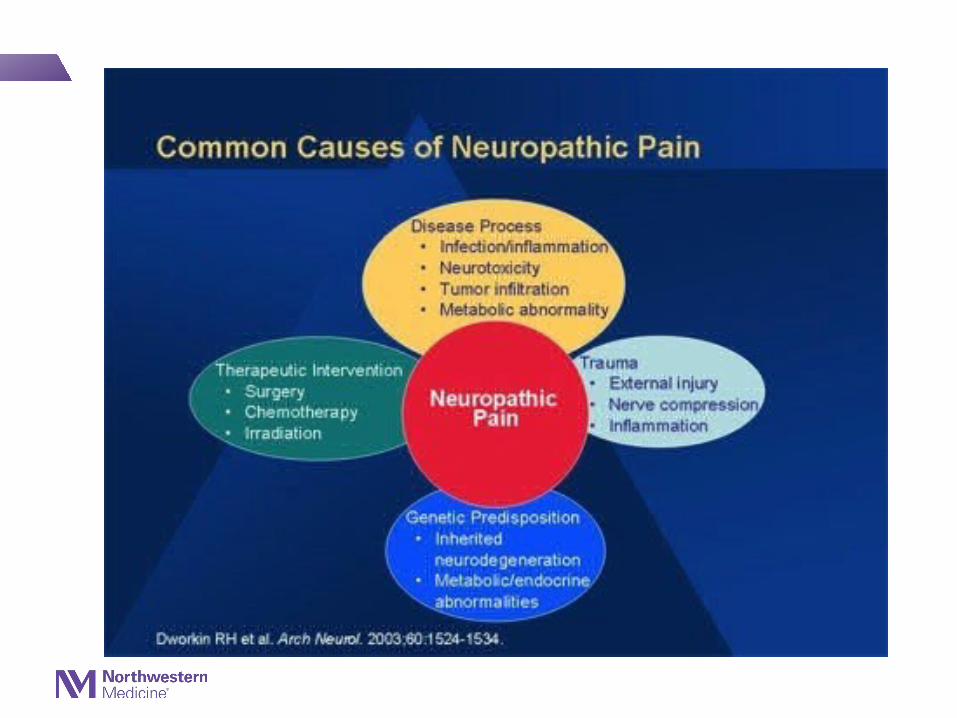
• Neuropathic pain arises from lesions to or dysfunction of the nervous system.
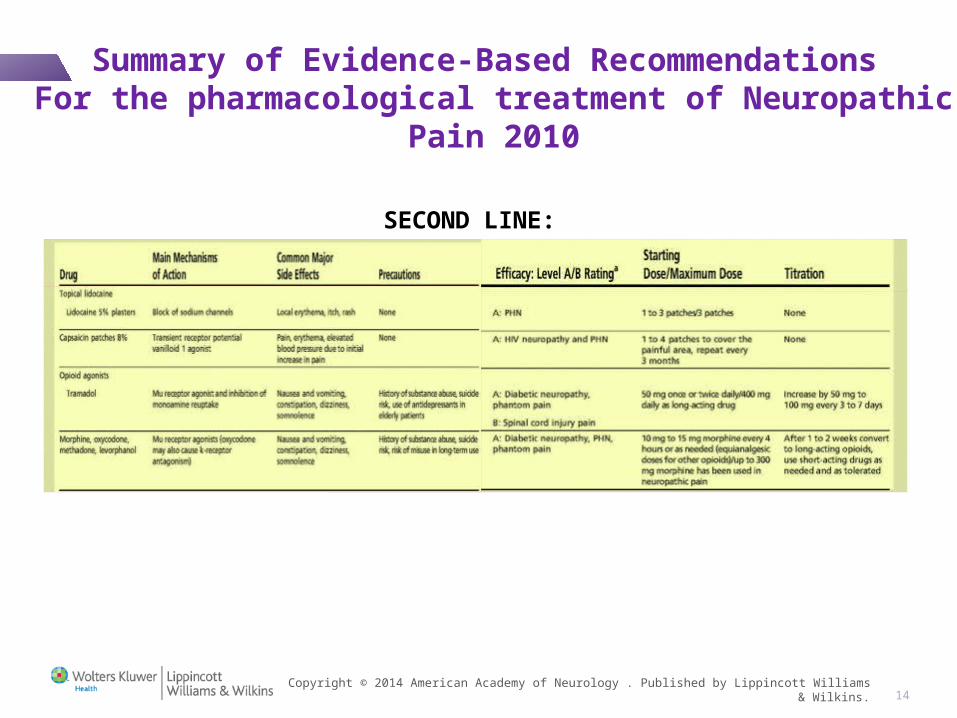
• Second-line treatment: combination of first-line drugs plus topical agents (Lidocaine or capsaicin).
• Third-line treatment: Opiod (Tramadol) and in particular cases of peripheral neuropathic pain Botulin Toxin A.
• Overall, the group found not much evidence for the effect of cannabinoids.
• Compared to earlier recommendations the new guideline downgrade the use opioid. Botulin Toxin A is new in the list.
• The complete data set has been submitted for publication.
New Guidelines for the treatment of Neuropathic Pain: IASP-Neuropathic Pain Special Interest Group (NeuPSIG).
Conclusion• The management of patients with neuropathic pain is challenging because
of the multiplicity of mechanisms underlying this debilitating condition. • Evidence-based recommendations for the pharmacological treatment of
neuropathic pain have been recently proposed.• Because of the multiplicity of mechanisms underlying neuropathic pain it is
possible that each of the painful symptoms may correspond to distinct mechanisms and therefore respond to specific treatments.
• Classification of patient according sensory phenotypes will direct rational therapies based on underlying mechanisms of pain and hopefully lead to a more effective and personalized management of patient with neuropathic pain.
• Molecular mechanisms underlying neuropathic pain and novel therapeutic targets can be investigated using animal models.
• Chemokine signaling is a new candidate responsible for hyper-excitability in a distinct subpopulation of DRG neurons in diabetes and a possible novel therapeutic target for PDN.
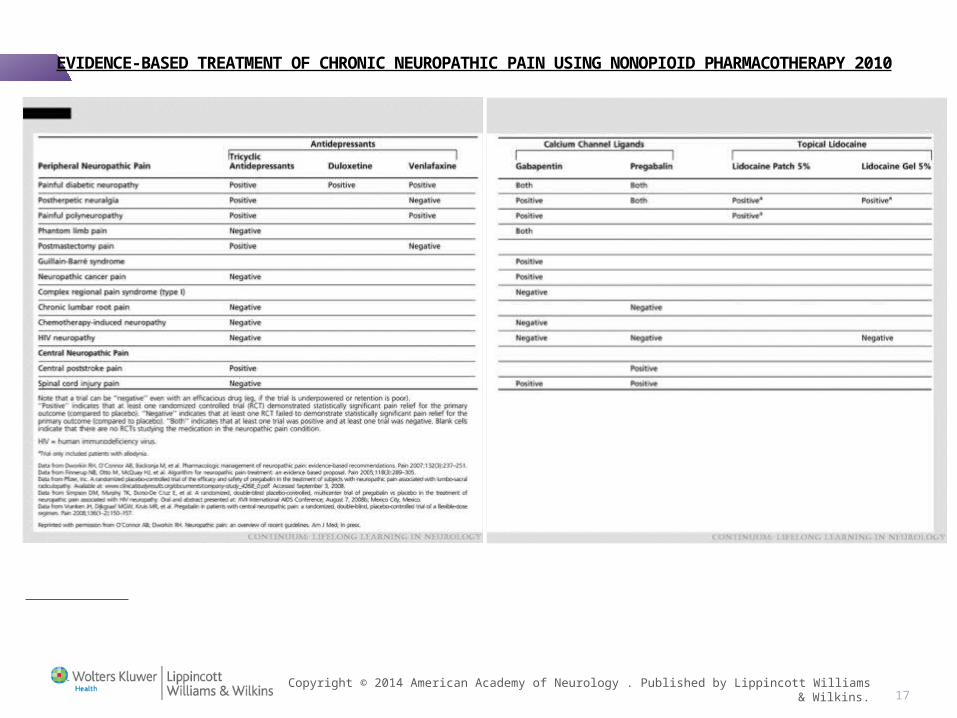
EVIDENCE-BASED TREATMENT OF CHRONIC NEUROPATHIC PAIN USING NONOPIOID PHARMACOTHERAPY 2010
TABLE 4-1 Summary of the Results of Published and Available Unpublished Randomized Controlled Trials Involving First-Line Nonopioid Medications for Patients With Neuropathic Pain
17
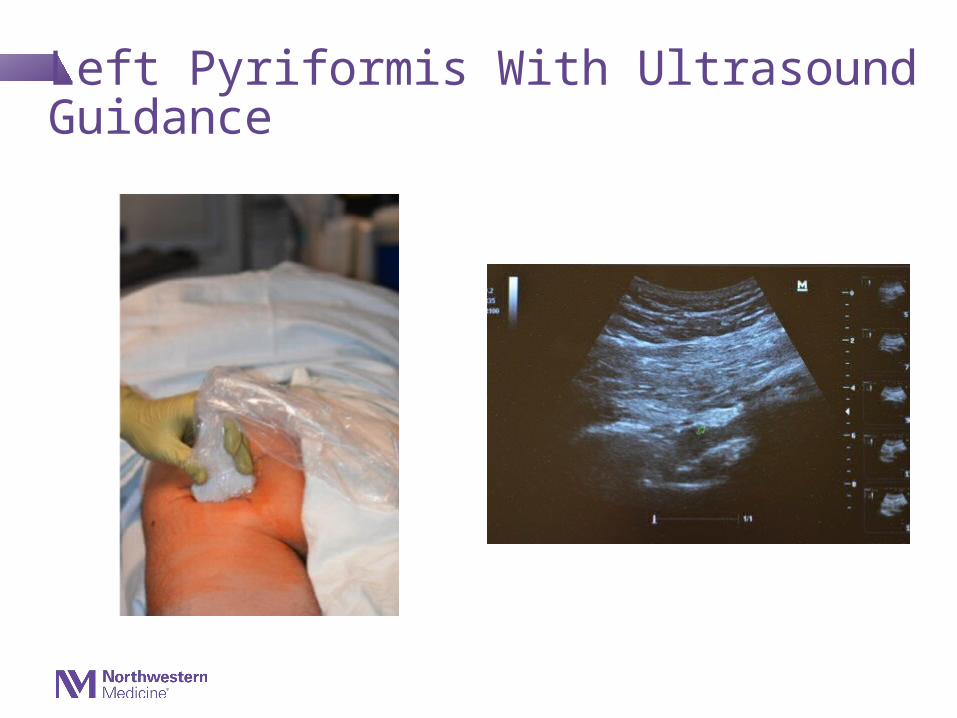
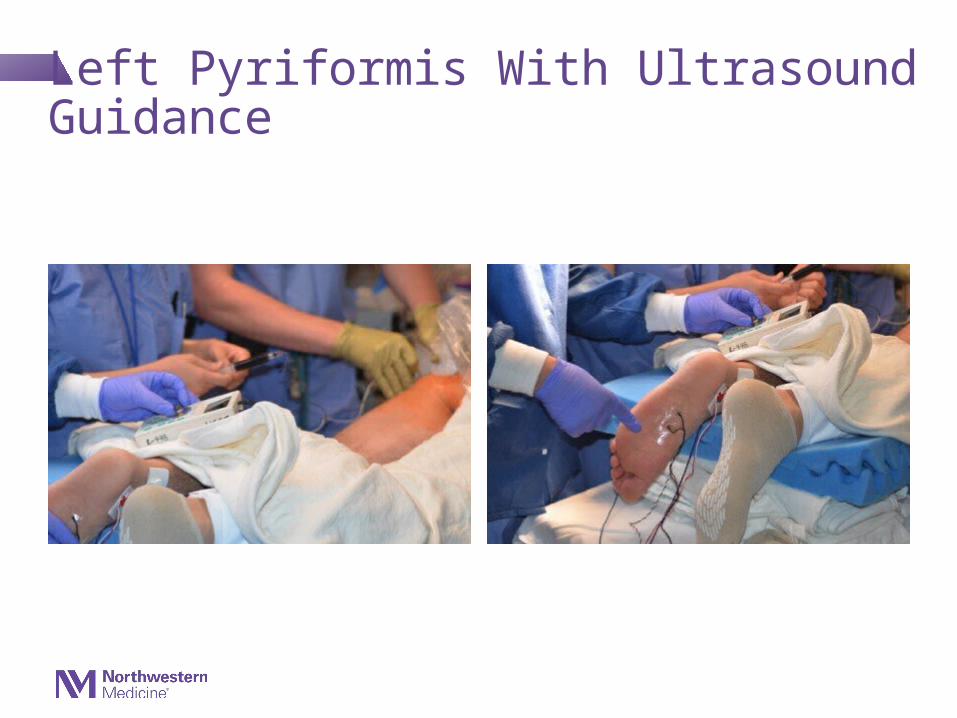
Other More Invasive Treatments- Local Injections (local anesthetic, steroid…) with image guidance
- Spinal Cord or Peripheral Nerve Stimulators
- Spinal Cord Pumps
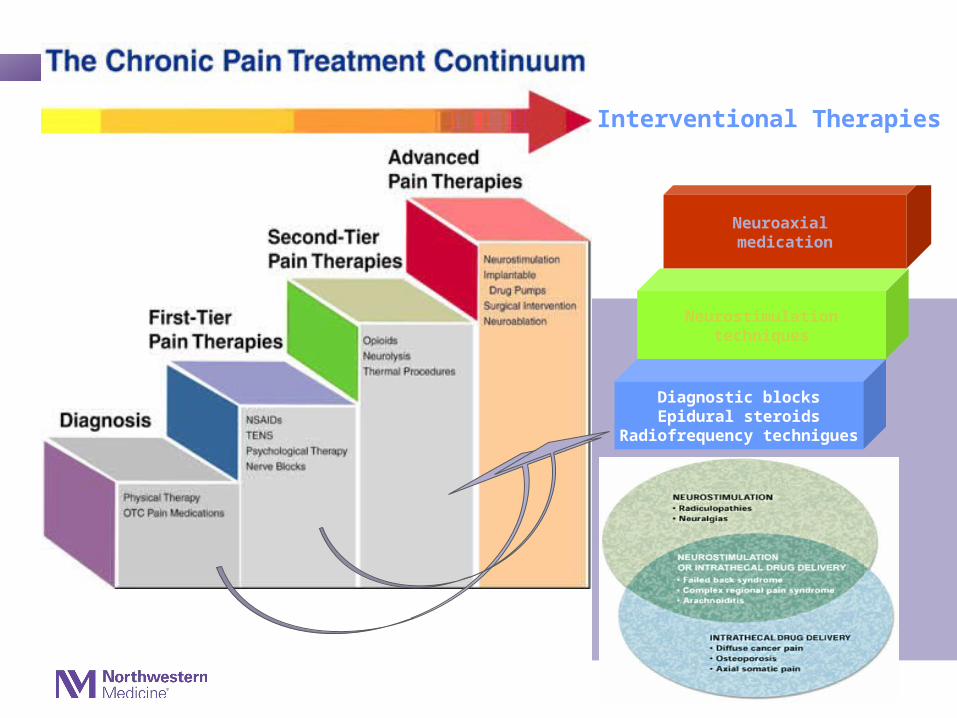
Diagnostic blocksEpidural steroids
Radiofrequency technigues
Neurostimulationtechniques
Neuroaxial medication
Interventional Therapies
Focal Peripheral Nerve Pathology Entrapments, Masses, And Traumatic Injuries
Michel Kliot MDProfessor of NeurosurgeryDirector of Peripheral Nerve CenterNorthwestern University Feinberg School of MedicineChicago, IL
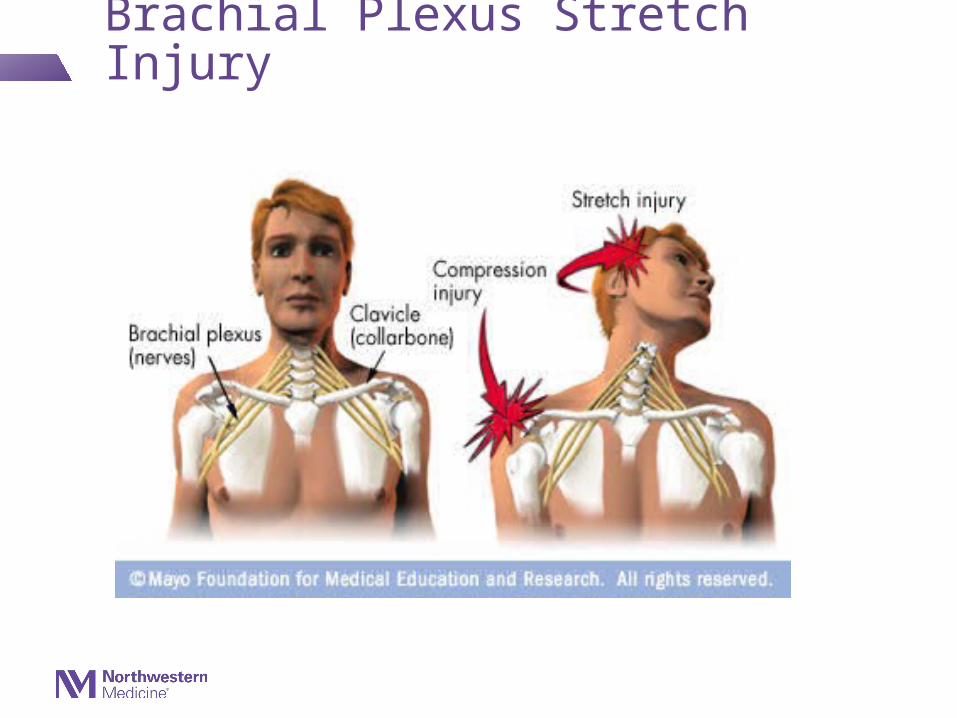
Nerve Pain, Numbness, And/Or Weakness Caused By
•Compression and/or stretching of nerves from entrapment syndromes, trauma, or masses
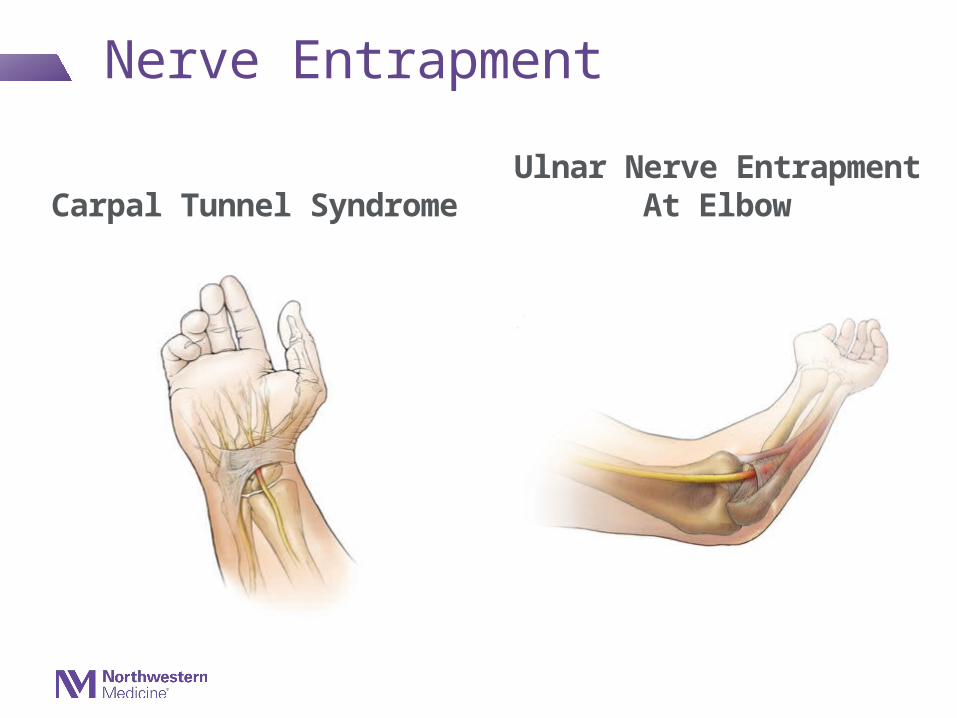
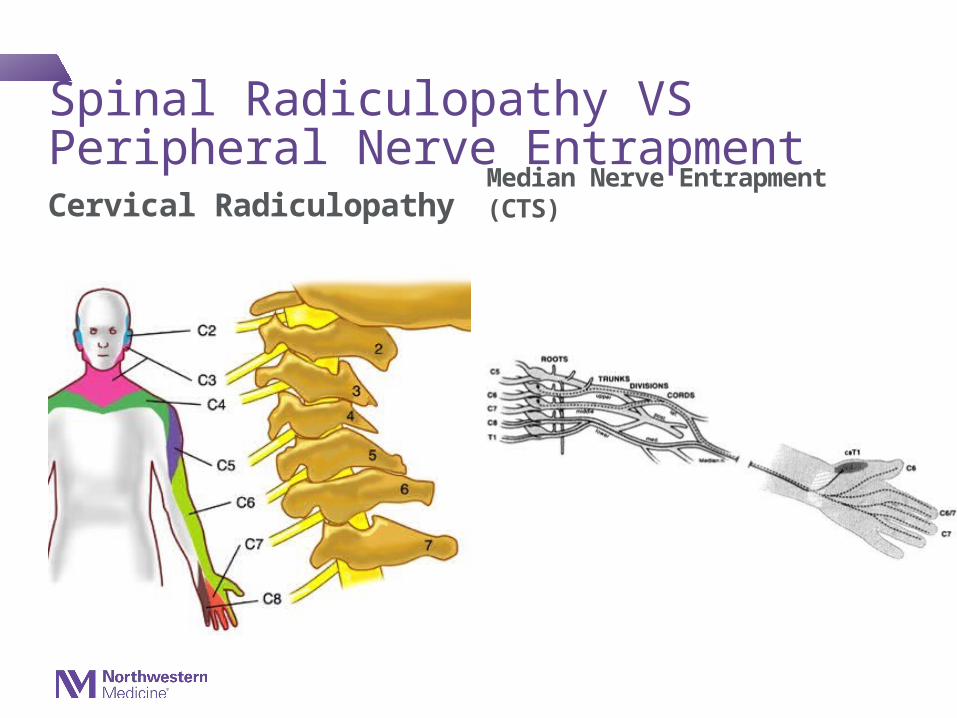
Nerve Entrapment
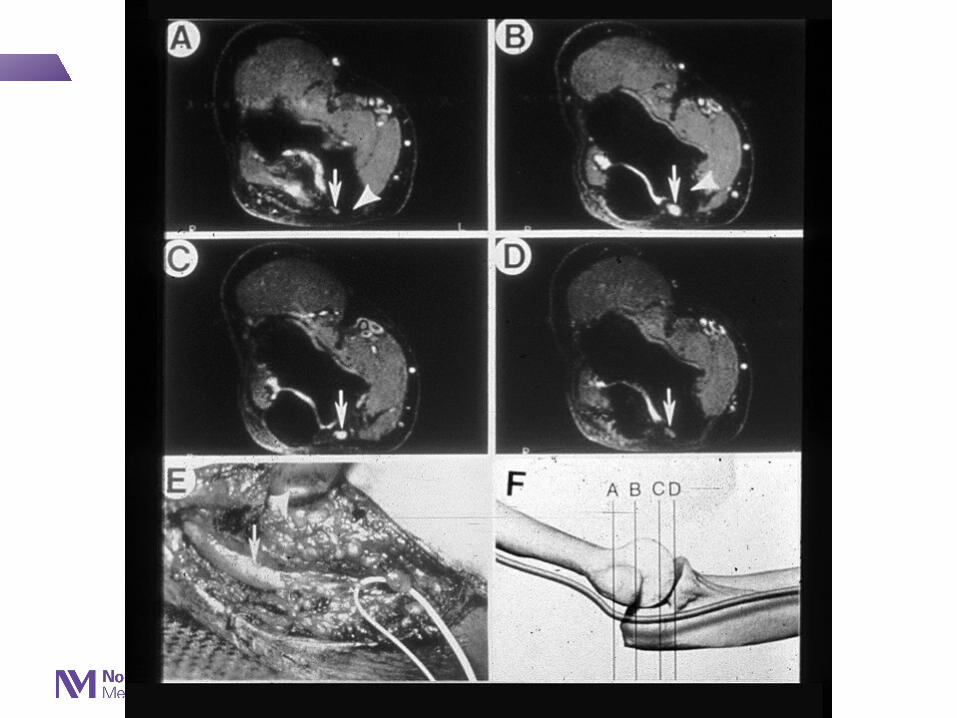
Carpal Tunnel Syndrome Ulnar Nerve Entrapment At Elbow
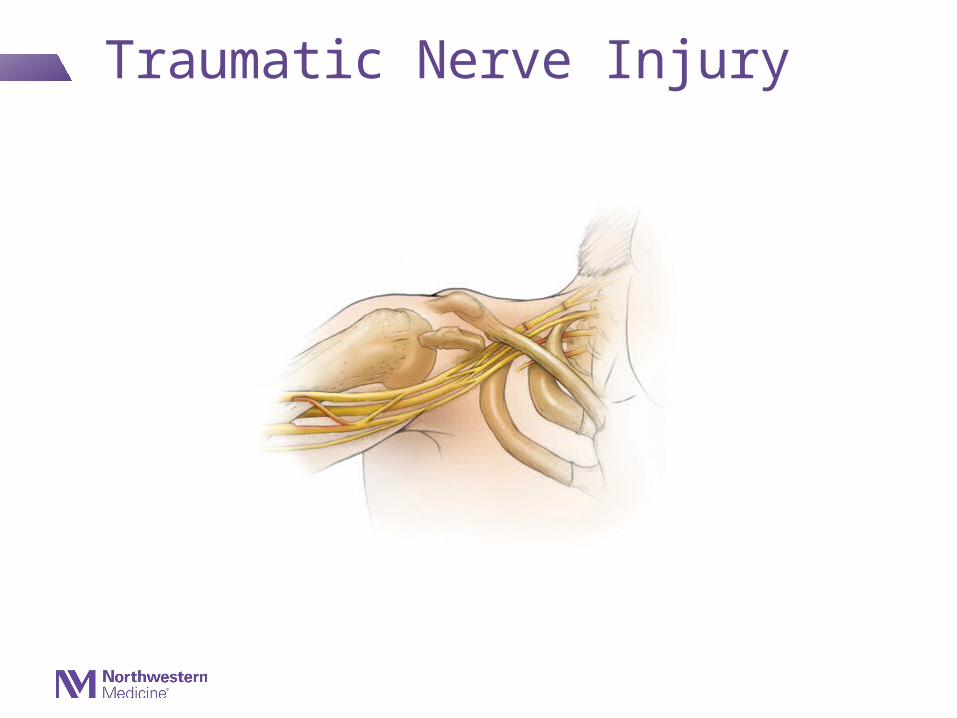
Traumatic Nerve Injury
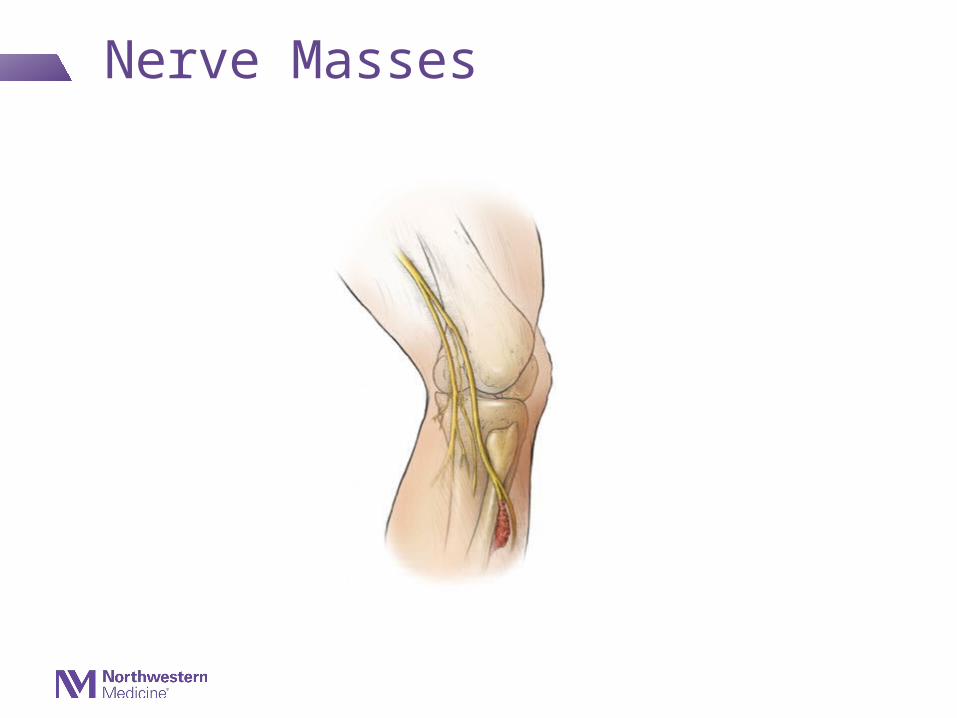
Nerve Masses
Entrapment Syndromes• Common
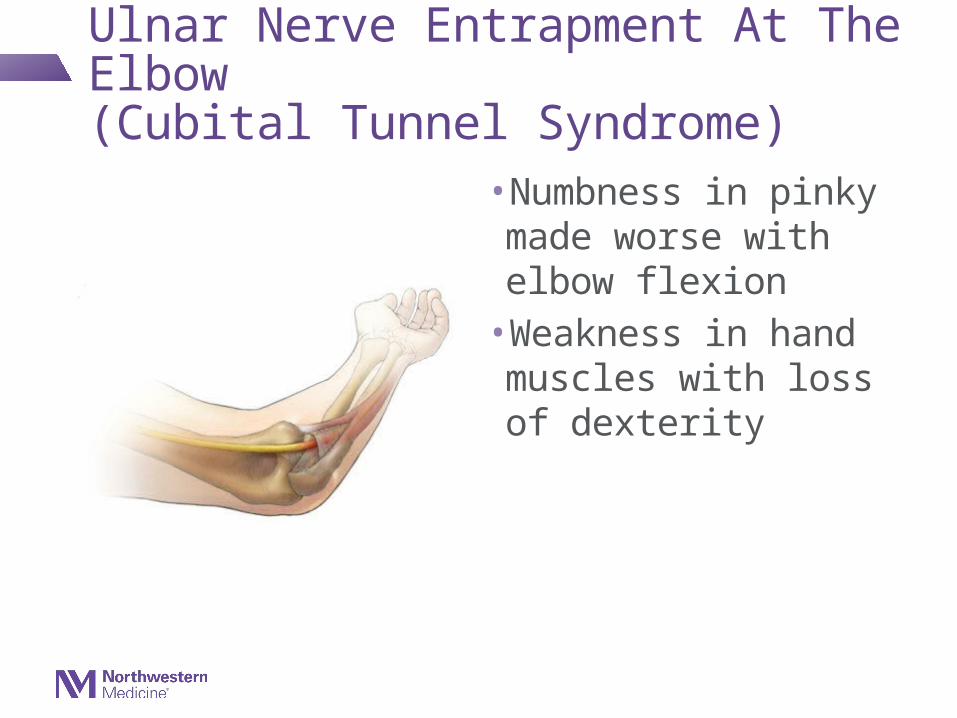
– Carpal Tunnel Syndrome– Ulnar Nerve Entrapment At The Elbow or
distribution of a single peripheral nerve involved
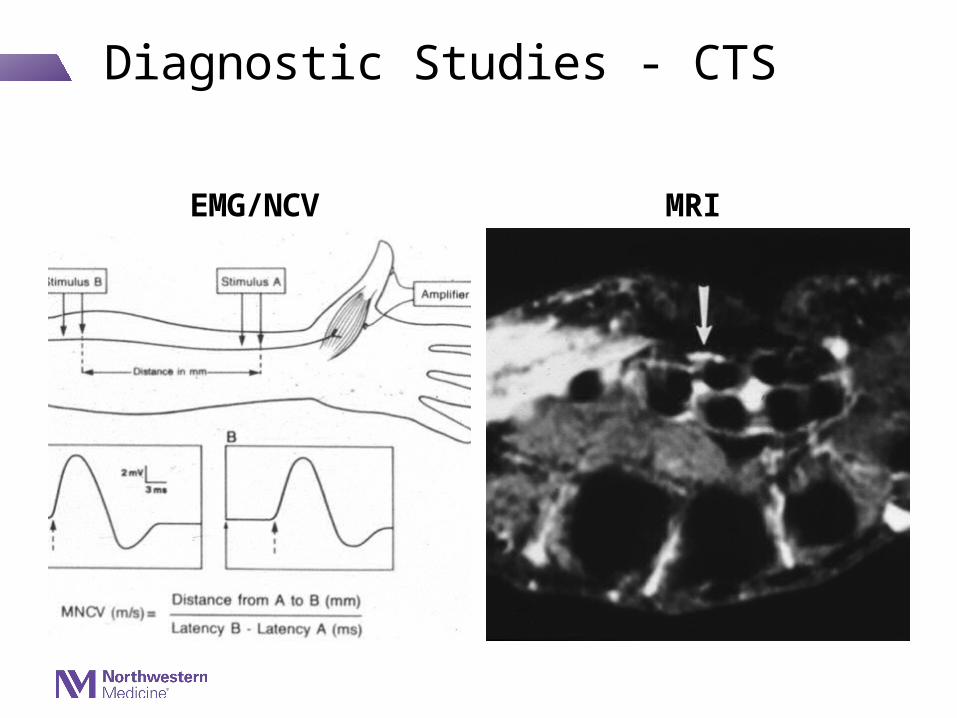
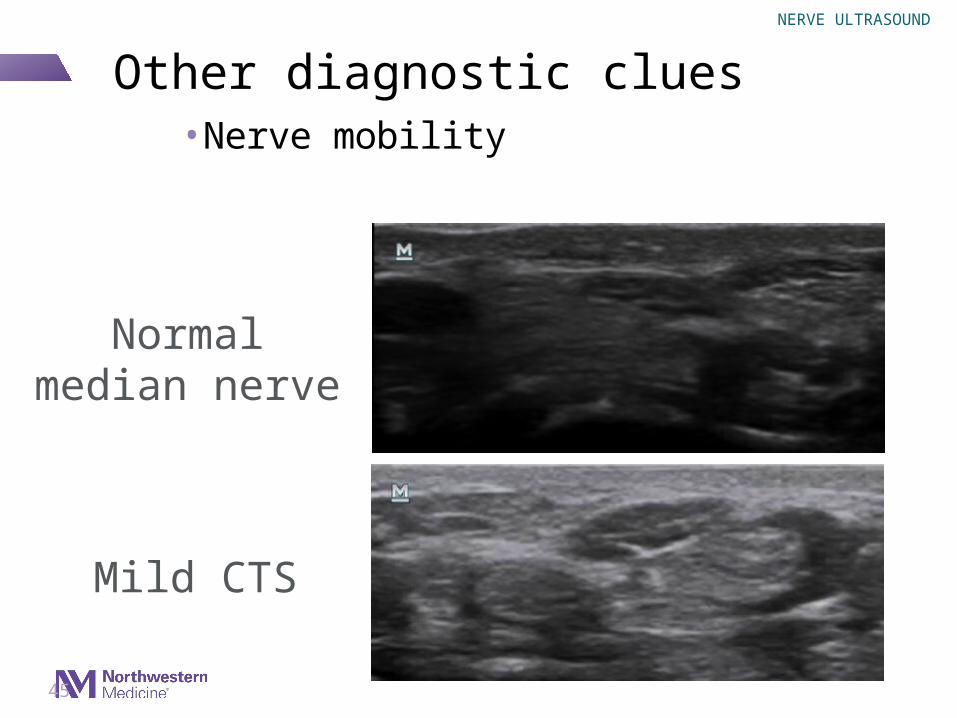
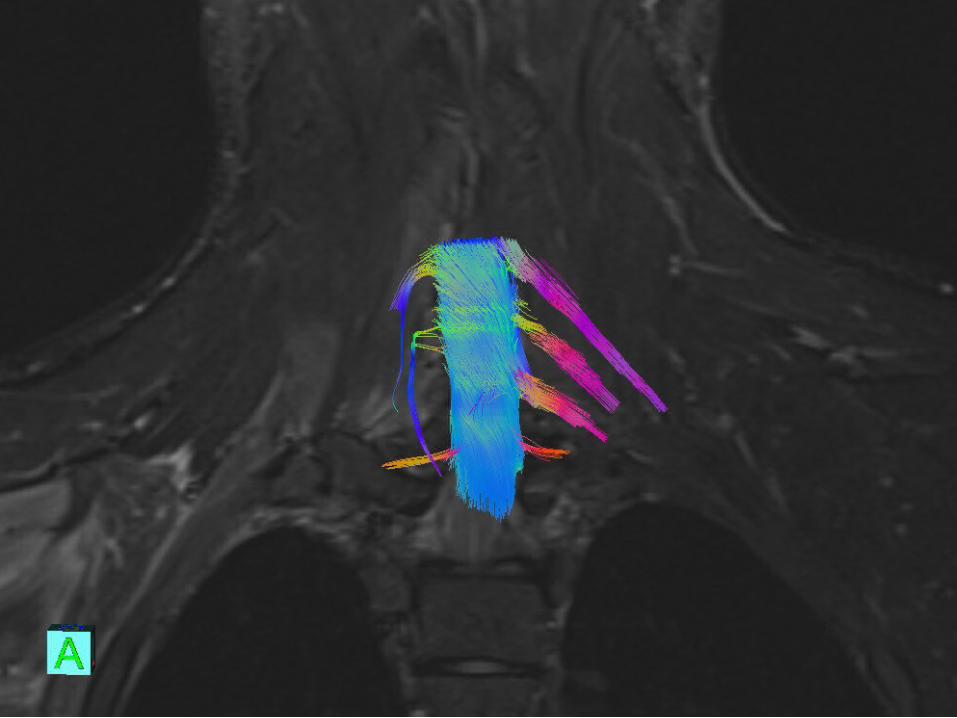
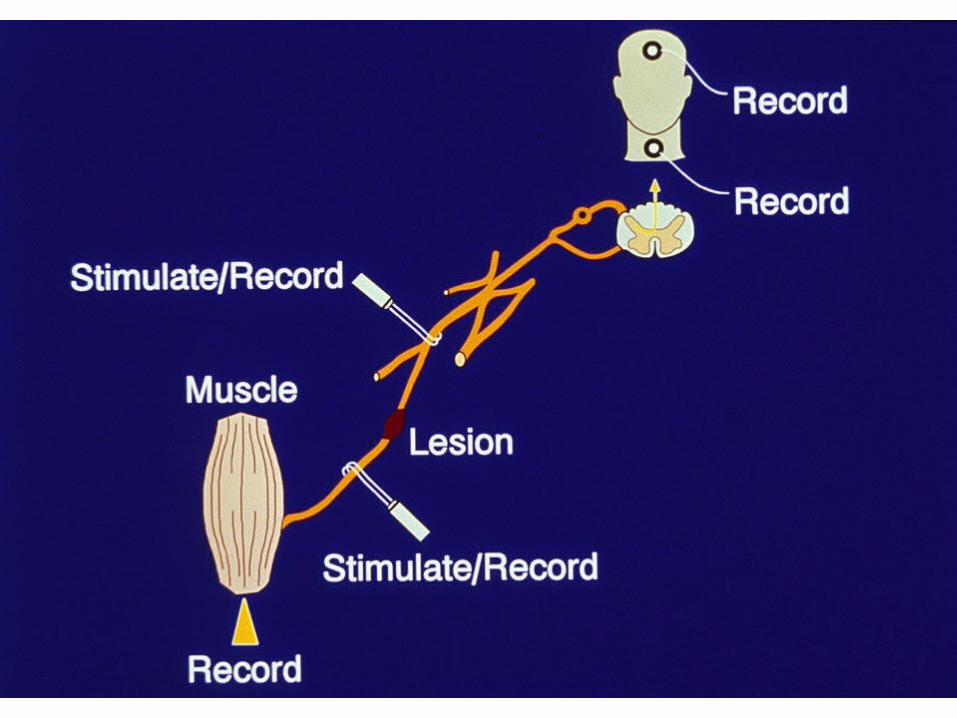
• Diagnosis confirmed with EMG/NCV usually and/or imaging (ultrasound/MRI) studies
When a patient meets a doctor there are at least 3 distinctly different possible outcomes:
1. Improves
2. Stays the Same
3. Deteriorates
First do no harm Wanting
to help
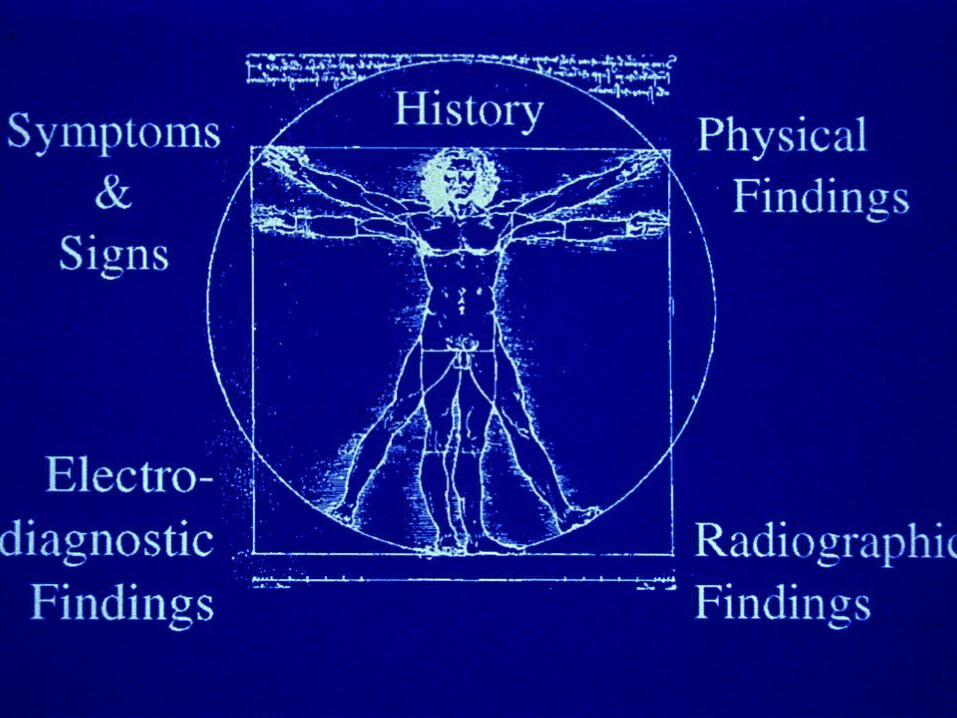
Diagnostic/TreatmentApproach/Philosophy
A clinical diagnosis – made on the basis of a history, symptoms and findings – is strengthened when supported by one or more diagnostic studies or interventions.
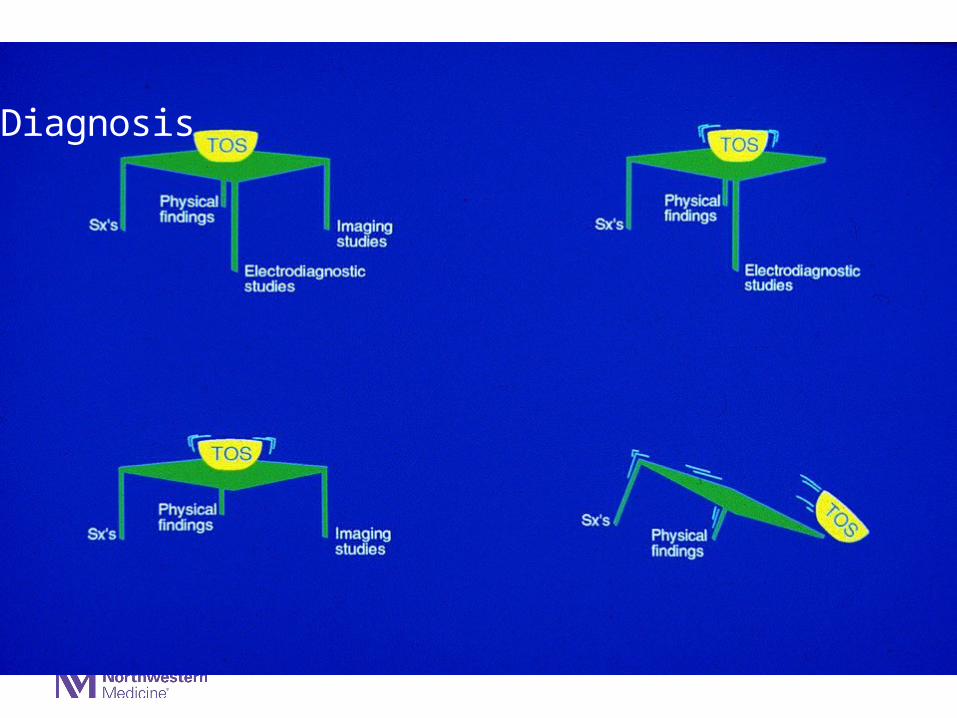
Diagnosis
Giving Clinical Advice
Although one’s clinical approach changes over time with experience
It is always useful to ask what one would do for a family member or if
you were in the patient’s shoes
Peripheral Nerve Surgeon’s Grading Schema
•Injuries that might improve with medical treatment
•Injuries that might benefit from a surgical repair
Clinical Grading of a Chronic Peripheral Nerve Problem (e.g Entrapment neuropathy)
Medical Treatment• Mild: Intermittent tolerable symptoms without axonal loss / stable or
improving
• Moderate: Constant tolerable symptoms without axonal loss / stable or improving
Surgical Treatment• Moderate: Constant intolerable symptoms without axonal loss / stable or
deteriorating
• Severe: Clinical and electrodiagnostic evidence of axonal loss
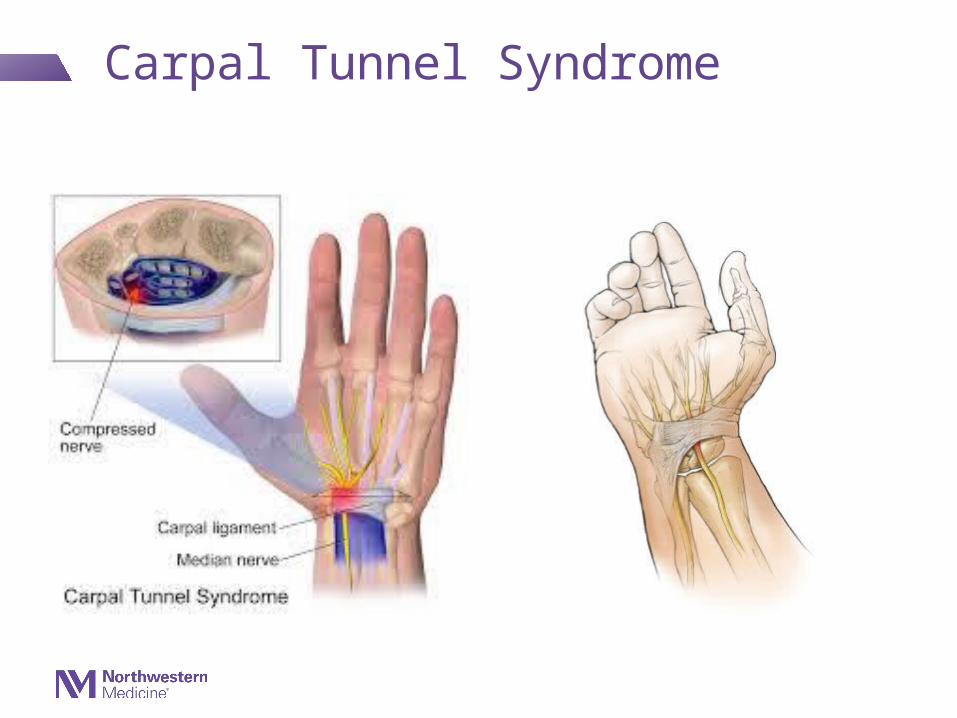
Carpal Tunnel Syndrome
Carpal Tunnel Syndrome:Symptoms
• Numbness and/or dysesthesias in 1st through 3rd fingers
• Wrist and/or hand pain (can radiate as proximal as shoulder)