Idiopathic dilated cardiomyopathy (DCM) is a seriousdisorder and is the most common cause of heart failure inyoung patients. Its prevalence in the U.S.A. is 36 cases per1 million, being responsible for 25% of the more than750,000 cases of heart failure reported and forapproximately 250,000 deaths. The long-term outcome ofapproximately 50% of patients is terminal heart failurerequiring cardiac transplantation[1,2]. A genetic origin forDCM has been reported in up to 25% of cases but themajority are sporadic, and a viral or immune pathogenesisis suspected in approximately 20–30% of idiopathicDCM[3–6]. Virus-induced myocarditis may progress to anautoimmune phase after resolution or amelioration of the
initial infection, and than finally to progressive dilatationafter resolution or amelioration of the immune injury[7].Chronic viral infection of the myocardium has beendetected in patients clinically presenting with myocarditisand DCM. Thus, although viruses are classically regardedas agents of self-limiting infections, a considerable body ofevidence implicates them in the aetiology of chronicdiseases, including DCM[8–10].
The diagnosis or exclusion of virus-induced inflam-matory cardiomyopathy depends on accurate analysis ofendomyocardial biopsies, and confusion in diagnosis andsubsequent errors in therapy are particularly likely ifinadequate diagnostic tools are employed. Even with the useof adequate diagnostic methods, it is difficult to makedecisions regarding specific therapeutic strategies becauseof overlapping phases of the disease. Nevertheless, and inspite of some as yet unresolved shortcomings of thediagnostic procedures (e.g. sampling error), a rationaldecision regarding specific therapy requires the use of allcurrently available diagnostic tools.
European Heart Journal Supplements (2002) 4 (Supplement I), I73–I80
Diagnosis and treatment of patients with virusinduced inflammatory cardiomyopathy
U. Kühl1, M. Pauschinger1, M. Noutsias1, J.-F. Kapp2 and H.-P. Schultheiss1
1Department of Cardiology and Pneumonology, Medical Clinic II, Department of Cardiology, University HospitalBenjamin Franklin, Free University of Berlin, and 2Schering AG, Spezial Therapeutika, Berlin, Germany
Chronic viral induced inflammatory cardiomyopathy causesprogression of left ventricular dysfunction and is an importantcause of dilated cardiomyopathy. Despite of the progress madein heart failure therapy, mortality of dilated cardiomyopathy isstill 10% per year. Current heart failure therapy is symptomaticand does not impact on the specific underlying pathogenicmechanisms. Thus, specific treatment strategies that aredirected against the underlying pathogenetic causes arerequired if myocarditis and its sequela, namely inflammatorycardiomyopathy, are to be successfully treated. Becausehistological and, especially, clinical diagnosis is fraught withnumerous problems, an aetiological classification based onhistology, immunohistochemistry and molecular biology isfavourable, particularly in view of the improvements inmethods made in recent years. The combination of thesediagnostic techni-ques allows a new classification of dilated
Correspondence: Uwe Kühl, PhD, University Hospital BenjaminFranklin, Department of Cardiology and Pneumonology, FreeUniversity of Berlin, Hindenburgdamm 30, D-12200 Berlin,Germany.
Dow
nloaded from https://academ
ic.oup.com/eurheartjsupp/article-abstract/4/suppl_I/I73/442320 by guest on 03 April 2019
Current heart failure therapy is symptomatic and does notimpact on the specific underlying pathogenic mechanisms.Progression of left ventricular dysfunction therefore cannotbe halted by conventional heart failure therapies. Thus,specific treatment strategies that are directed against theunderlying pathogenetic causes are required if myocarditisand its sequela, namely inflammatory cardiomyopathy, areto be successfully treated.
Myocardial damage may occur during several stages ofvirus-induced cardiomyopathy (Fig. 1). The acute phasebegins with myocardial cell infection and viral replication,culminating in cell lysis caused by virus. Early defencemechanisms include a cellular immune response thatprevents further virus spreading and results in virusclearance. This is achieved by production of antiviralcytokines and elimination of virus-infected myocardial cellsthrough cytokine-activated macrophages and natural killercells, perforin mediated cell cytolysis (cytotoxic T lympho-cytes) and induction of apoptosis[11,12]. Thus, both the viralpathogen itself and the protective antiviral immune responsemay produce irreversible loss of infected myocardial cells,thereby contributing to irreversible damage of themyocardium, long-term remodelling and progression ofheart failure. Successful virus clearance and resolution ofthe inflammatory process therefore results in persistentsequelae.
If there is no history of virus-induced disease, then theobserved clinical outcome is referred to as DCM. PersistentT-cell activation, induced by intrinsic myocardial antigensthat cross-react with viral peptides (molecular mimicry),may induce an inflammatory process that is not terminatedand escapes regular control mechanisms[12] (see the reviewby Afanasyeva and Rose, in the present supplement).Resulting immune-mediated injury may further increaseventricular dysfunction. The pathogenetic mechanisms thatare involved are poorly understood, but the first encounterwith antigens may set the stage for later harmfulautoimmune processes, when antigen-specific and antigennon-specific signals are presented to the immune system.For example, these signalling molecules includecostimulatory cell surface markers such as CD28 or CD40,their ligands (i.e. B7 or CD154), and soluble mediators suchas interleukin (IL)-1, tumour necrosis factor-alpha, IL-12,interferon (IFN)-gamma, IL-4 and IL-13, all of which mayplay important roles in orchestrating the later adaptiveimmune response.
Diagnosis of inflammatorycardiomyopathy
Histological analysis
Myocardial inflammation is defined by the presence ofinfiltrating lymphocytes, either with (active myocarditis) orwithout (borderline myocarditis) myocyte necrosis.
I74 U. Kühl et al.
Eur Heart J Supplements, Vol. 4 (Suppl I) December 2002
Figure 1 Pathogenesis of virus-induced inflammatory cardiomyopathy.
Direct viral infection
Myocardial cell death
(Auto-) Immune response
Inflammation and cell dysfunction
Immunoadsorption
Cellularimmunity
T-lymphocytesMacrophages
NK-cells
Humoralimmunity
Heart reactiveantibodies
Immunomodulatory therapy
Immunemodulation
CytokinesTNF-α, IFN,Il-1, Il-2, Il-6
Viralpersistence
Coxsackie virusAdenovirus
Viral replication
Anti-viral treatmentImmunosuppression
Dow
nloaded from https://academ
ic.oup.com/eurheartjsupp/article-abstract/4/suppl_I/I73/442320 by guest on 03 April 2019
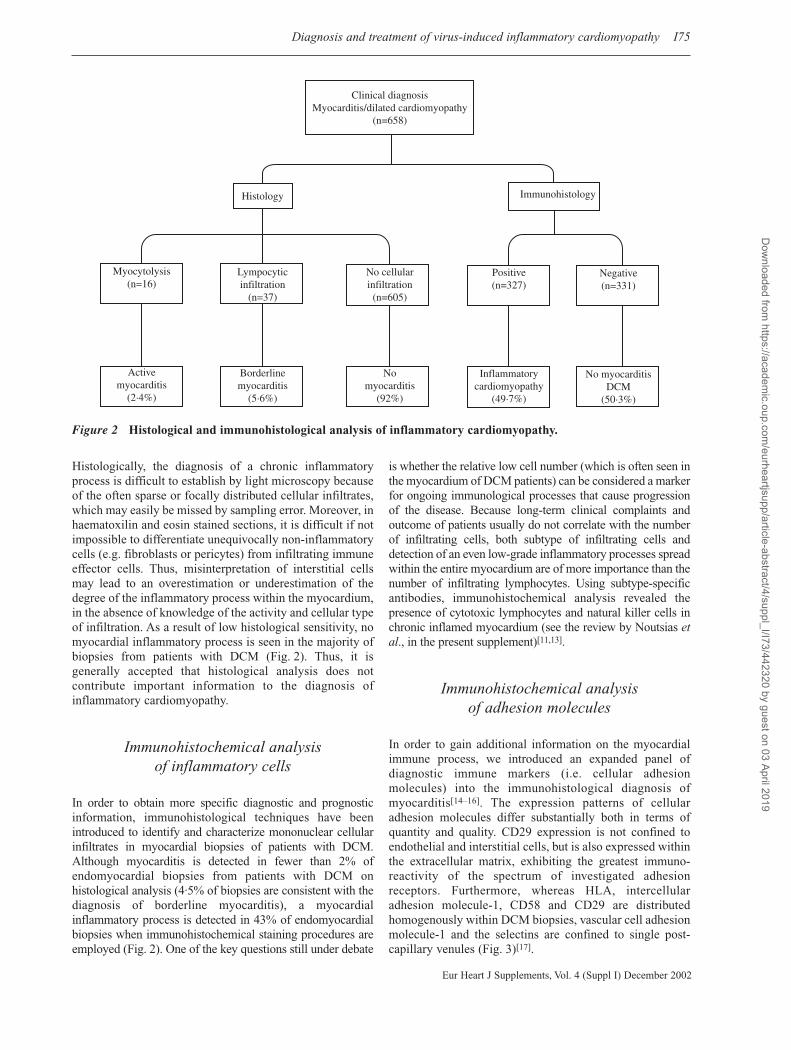
Histologically, the diagnosis of a chronic inflammatoryprocess is difficult to establish by light microscopy becauseof the often sparse or focally distributed cellular infiltrates,which may easily be missed by sampling error. Moreover, inhaematoxilin and eosin stained sections, it is difficult if notimpossible to differentiate unequivocally non-inflammatorycells (e.g. fibroblasts or pericytes) from infiltrating immuneeffector cells. Thus, misinterpretation of interstitial cellsmay lead to an overestimation or underestimation of thedegree of the inflammatory process within the myocardium,in the absence of knowledge of the activity and cellular typeof infiltration. As a result of low histological sensitivity, nomyocardial inflammatory process is seen in the majority ofbiopsies from patients with DCM (Fig. 2). Thus, it isgenerally accepted that histological analysis does notcontribute important information to the diagnosis ofinflammatory cardiomyopathy.
Immunohistochemical analysis of inflammatory cells
In order to obtain more specific diagnostic and prognosticinformation, immunohistological techniques have beenintroduced to identify and characterize mononuclear cellularinfiltrates in myocardial biopsies of patients with DCM.Although myocarditis is detected in fewer than 2% ofendomyocardial biopsies from patients with DCM onhistological analysis (4·5% of biopsies are consistent with thediagnosis of borderline myocarditis), a myocardialinflammatory process is detected in 43% of endomyocardialbiopsies when immunohistochemical staining procedures areemployed (Fig. 2). One of the key questions still under debate
is whether the relative low cell number (which is often seen inthe myocardium of DCM patients) can be considered a markerfor ongoing immunological processes that cause progressionof the disease. Because long-term clinical complaints andoutcome of patients usually do not correlate with the numberof infiltrating cells, both subtype of infiltrating cells anddetection of an even low-grade inflammatory processes spreadwithin the entire myocardium are of more importance than thenumber of infiltrating lymphocytes. Using subtype-specificantibodies, immunohistochemical analysis revealed thepresence of cytotoxic lymphocytes and natural killer cells inchronic inflamed myocardium (see the review by Noutsias etal., in the present supplement)[11,13].
Immunohistochemical analysis of adhesion molecules
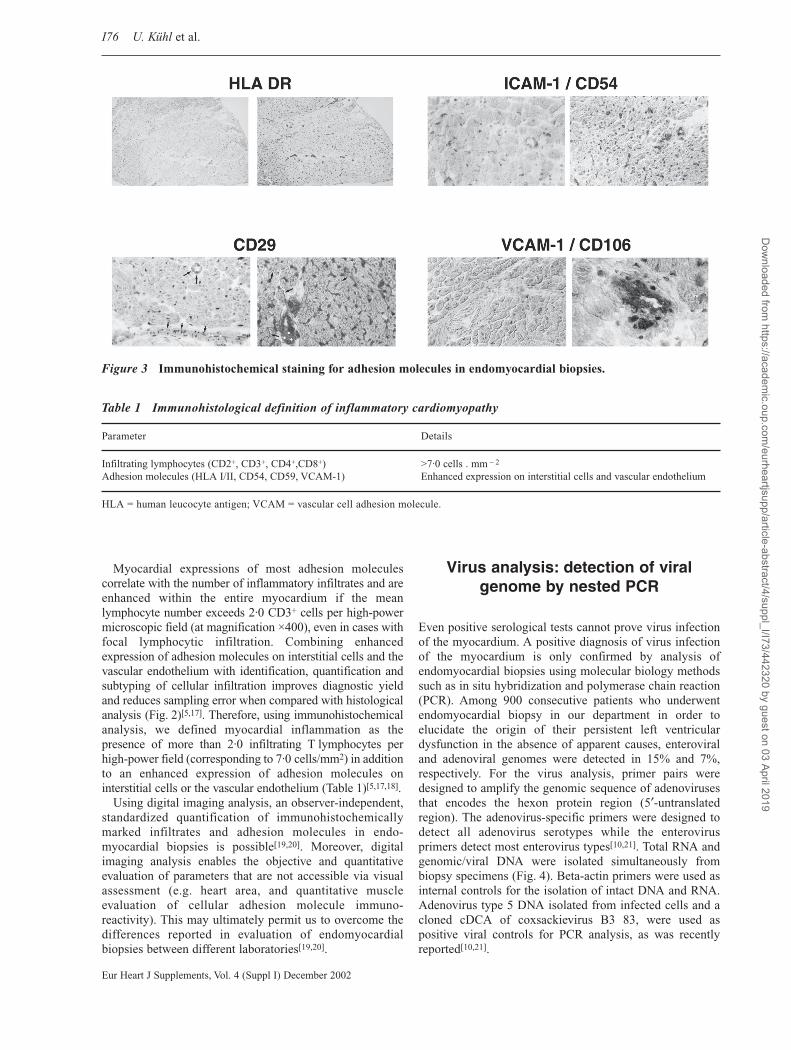
In order to gain additional information on the myocardialimmune process, we introduced an expanded panel ofdiagnostic immune markers (i.e. cellular adhesionmolecules) into the immunohistological diagnosis ofmyocarditis[14–16]. The expression patterns of cellularadhesion molecules differ substantially both in terms ofquantity and quality. CD29 expression is not confined toendothelial and interstitial cells, but is also expressed withinthe extracellular matrix, exhibiting the greatest immuno-reactivity of the spectrum of investigated adhesionreceptors. Furthermore, whereas HLA, intercellularadhesion molecule-1, CD58 and CD29 are distributedhomogenously within DCM biopsies, vascular cell adhesionmolecule-1 and the selectins are confined to single post-capillary venules (Fig. 3)[17].
Diagnosis and treatment of virus-induced inflammatory cardiomyopathy I75
Eur Heart J Supplements, Vol. 4 (Suppl I) December 2002
Figure 2 Histological and immunohistological analysis of inflammatory cardiomyopathy.
ic.oup.com/eurheartjsupp/article-abstract/4/suppl_I/I73/442320 by guest on 03 April 2019
Myocardial expressions of most adhesion moleculescorrelate with the number of inflammatory infiltrates and areenhanced within the entire myocardium if the meanlymphocyte number exceeds 2·0 CD3+ cells per high-powermicroscopic field (at magnification ×400), even in cases withfocal lymphocytic infiltration. Combining enhancedexpression of adhesion molecules on interstitial cells and thevascular endothelium with identification, quantification andsubtyping of cellular infiltration improves diagnostic yieldand reduces sampling error when compared with histologicalanalysis (Fig. 2)[5,17]. Therefore, using immunohistochemicalanalysis, we defined myocardial inflammation as thepresence of more than 2·0 infiltrating T lymphocytes perhigh-power field (corresponding to 7·0 cells/mm2) in additionto an enhanced expression of adhesion molecules oninterstitial cells or the vascular endothelium (Table 1)[5,17,18].
Using digital imaging analysis, an observer-independent,standardized quantification of immunohistochemicallymarked infiltrates and adhesion molecules in endo-myocardial biopsies is possible[19,20]. Moreover, digitalimaging analysis enables the objective and quantitativeevaluation of parameters that are not accessible via visualassessment (e.g. heart area, and quantitative muscleevaluation of cellular adhesion molecule immuno-reactivity). This may ultimately permit us to overcome thedifferences reported in evaluation of endomyocardialbiopsies between different laboratories[19,20].
Virus analysis: detection of viralgenome by nested PCR
Even positive serological tests cannot prove virus infectionof the myocardium. A positive diagnosis of virus infectionof the myocardium is only confirmed by analysis ofendomyocardial biopsies using molecular biology methodssuch as in situ hybridization and polymerase chain reaction(PCR). Among 900 consecutive patients who underwentendomyocardial biopsy in our department in order toelucidate the origin of their persistent left ventriculardysfunction in the absence of apparent causes, enteroviraland adenoviral genomes were detected in 15% and 7%,respectively. For the virus analysis, primer pairs weredesigned to amplify the genomic sequence of adenovirusesthat encodes the hexon protein region (5′-untranslatedregion). The adenovirus-specific primers were designed todetect all adenovirus serotypes while the enterovirusprimers detect most enterovirus types[10,21]. Total RNA andgenomic/viral DNA were isolated simultaneously frombiopsy specimens (Fig. 4). Beta-actin primers were used asinternal controls for the isolation of intact DNA and RNA.Adenovirus type 5 DNA isolated from infected cells and acloned cDCA of coxsackievirus B3 83, were used aspositive viral controls for PCR analysis, as was recentlyreported[10,21].
I76 U. Kühl et al.
Eur Heart J Supplements, Vol. 4 (Suppl I) December 2002
Figure 3 Immunohistochemical staining for adhesion molecules in endomyocardial biopsies.
Table 1 Immunohistological definition of inflammatory cardiomyopathy
ic.oup.com/eurheartjsupp/article-abstract/4/suppl_I/I73/442320 by guest on 03 April 2019
Biopsy derived diagnosis andclassification of viral heart disease
Because pathological/anatomical and, especially, clinicaldiagnosis is fraught with numerous problems, an aetiologicalclassification based on histology, immunohistochemistryand molecular biology is favourable, particularly in view ofthe improvements in methods made in recent years. Such aclassification may not only contribute toward improving ourunderstanding of underlying pathological mechanisms, butultimately may also assist in developing specificimmunomodulatory treatments.
Current standards for diagnostic procedures requireroutine histological staining, which allows analysis ofhistomorphological changes and may depict myocytolysis(active myocarditis). For analysis of chronic inflammatoryprocesses, however, immunohistological methods arerecommended. Detection of viral genome and replicationrequires molecular biological techniques such aspolymerase chain reaction (PCR) and in situ hybridization.According to the data obtained using these methods,clinically suspected DCM can be subclassified to differentdisease entities (Fig. 2)[22,23]. Further information is derivedfrom cytokine analysis of patients. Preliminary data suggestthat dysregulation of the host defence mechanisms againstviral infections, associated with an inappropriate T-helper-2-like immune response that lacks antiviral IFN-gamma,favours enteroviral RNA persistence and subsequentprogression of left ventricular dysfunction (Kühl et al.,unpublished data). A rise in pro-inflammatory antiviralT-helper-1 cytokines such as IFN-gamma appears to benecessary to control and eliminate viral RNA, therebylimiting progression of the disease.
Treatment of patients with virus-induced inflammatory cardiomyopathy
In spite of progress made in heart failure therapy since theintroduction of angiotensin-converting enzyme inhibitors,beta-blockers, spironolactone and amiodarone/implantablecardiovertor–defibrillator treatment, mortality associatedwith DCM is still 10%/year[24–26]. Current heart failuretherapy is symptomatic and does not impact on specificunderlying pathogenic mechanisms. Progression of leftventricular dysfunction therefore cannot be halted bytherapy with digitalis, diuretics, angiotensin-convertingenzyme inhibitors and beta-blocking agents. Thus, specifictreatment strategies that are directed against the underlyingpathogenetic causes are required if myocarditis and itssequela, namely inflammatory cardiomyopathy, are to besuccessfully treated.
Immunosuppressive and immunomodulatory therapy
Potential therapeutic efficacy of immunosuppressivetherapy was suggested by previous uncontrolledstudies[27–32]. However, it has not proved efficacious inprevious randomized trials in patients with recent-onsetcardiomyopathy because spontaneous recovery occurredboth in patients treated with conventional therapy and inthose treated with anti-inflammatory (methylprednisolone,cyclosporine A, intravenous immune globulin)therapy[33–35]. Selection of patients on histological ratherthan immunohistological and molecular biologicaldiagnostic criteria, and failure to account for the highspontaneous healing rate of recent-onset myocarditis maytherefore account for those findings[36–38]. Moreover,Frustaci et al. reported that most patients who did notrespond to immunosuppressive therapy were enterovirus-positive in a retrospective PCR analysis, demonstratingvirus-induced myocyte damage during immunosuppressivetreatment (see the review by Frustaci et al., in the presentsupplement). In order to avoid such diagnosticshortcomings future trials must focus on reliable diagnosticcriteria, which should include histological andimmunohistological evaluation of myocardial inflammatoryprocesses, as well as molecular biological analysis ofmyocardial virus infection (Fig. 5).
Immunosuppressive treatment regimens includecorticosteroids, azathioprine or cyclosporin A. Alpha-methylprednisolone is generally initially given at a rate of1 mg . kg – 1 body weight (for children 1–2 mg . kg – 1) for4 weeks, after which the dosage is tapered biweekly inincrements of 8–12 mg until a maintenance dose of 12 mgis reached. The treatment should last for 6 months. In casesof persistent inflammation (35–40% of patients are affectedby this), azathioprine may be administered in addition tolow-dose corticosteroid. However, this appears to beeffective only if a sufficient level of immunosuppression isachieved, which is signalled by a reduction in peripheral
Diagnosis and treatment of virus-induced inflammatory cardiomyopathy I77
Eur Heart J Supplements, Vol. 4 (Suppl I) December 2002
Figure 4 Molecular biological analysis (polymerasechain reaction [PCR]) of enteroviral RNA inendomyocardial biopsies. Lanes 1 and 7, molecularweight markers; lane 2, positive control; lanes 3 and 4,negative biopsy; lanes 5 and 6, enterovirus RNA-positivebiopsies.
Dow
nloaded from https://academ
ic.oup.com/eurheartjsupp/article-abstract/4/suppl_I/I73/442320 by guest on 03 April 2019
lymphocytes levels to around 1000/µl. Provided thatadequate molecular biology and immunohistochemicalcharacterization of patients is conducted, both clinical andhaemodynamic improvement can be achieved in 65% ofcases with immunosuppressive treatment (Fig. 6).
Antiviral therapy with interferon-beta
Three types of IFNs have been identified, which differ bothin structure and in antigenic properties; IFN-alpha isderived from leucocytes, IFN-beta from fibroblasts andIFN-gamma from lymphocytes. The important role playedby the IFNs as a natural defence mechanism against virusesis documented by three lines of experimental and clinicalevidence: in many viral infections a strong correlation hasbeen established between IFN production and naturalrecovery; inhibition of production or action of IFNenhances the severity of infection; and treatment with IFNprotects against viral infection. The antiviral effect isindependent of virus type and results in an intracellularblock of the viral replication cycle. IFNs increase resistancetoward viral replication, even in cells that neighbourinfected cells but have not yet been infected. Becauseeffective concentrations of IFN-beta can be attained in vivo,IFN-beta may become useful in the treatment of patientswith viral cardiomyopathy.
Analyzing virus positive patients in a phase II pilot study,we demonstrated that patients with persistence of viralgenomes and left ventricular dysfunction benefit fromantiviral treatment with IFN-beta (manuscript submitted).Before IFN-beta treatment, clinical complaints andhaemodynamic course did not improve and left ventriculardiameters slowly increased, in spite of constant heart failuremedication before IFN-beta treatment and during therapy.After 6 months of IFN-beta treatment, viral genomes were
no longer detectable in the biopsies of all treated patients,indicating that this treatment had led to a completeelimination of both adenoviral and enteroviral genomes.Virus clearance was accompanied by a reduction in clinicalcomplaints such as angina pectoris, dyspnoea, palpitationsand fatigue, resulting in improvement in New York HeartAssociation functional class. This clinical improvement wasassociated with a significant increase in left ventricularejection fraction and a decrease in left ventricular diameters.Because viral genomes were no longer detectable in anypatient after completion of IFN-beta treatment, our datasuggest that the beneficial clinical effect of IFN-beta isbased on elimination of cardiotropic viral genomes, whichoccurred even in DCM patients with a long history ofdisease.
Conclusion
Myocarditis is caused by a wide variety of pathologicalconditions, in particular viral infections, and often precedesthe development of DCM. The infecting virus initiates thedisease process and then may persist as an insidiousmolecular pathogen, causing ongoing cardiac damage (viralheart disease). If the host immune system can effectivelyclear the viral infection, then cardiac inflammation oftenresolves. Dysregulation of the immune response, however,may result in a persisting pathological (auto)immuneprocess (chronic myocarditis/inflammatory cardio-myopathy), causing progression of left ventricular dys-function. Cytokines play a critical role in the developmentof viral persistence and chronic inflammation. Becausepathological/anatomical and, especially, clinical diagnosisis fraught with numerous problems, the current standard ofbiopsy-based diagnostic procedures means that routinehistological staining, which allows analysis of histo-
I78 U. Kühl et al.
Eur Heart J Supplements, Vol. 4 (Suppl I) December 2002
Figure 5 Biopsy-derived diagnosis and classification of inflammatory cardiomyopathy.
Acute viral myocarditis
Cardiomyopathy
Antiviral therapy
Non-inflammatorycardiomyopathy
Inflammatorycardiomyopathy
No viral persistence
Symptomatic therapy
No viral persistence
Immunosuppression
Viral persistence
Dow
nloaded from https://academ
ic.oup.com/eurheartjsupp/article-abstract/4/suppl_I/I73/442320 by guest on 03 April 2019
morphologic changes and may demonstrate myocytolysis(active myocarditis), is quite appropriate. For the analysis ofchronic inflammatory processes, immunohistologicalmethods are recommended. Detection of viral genome andreplication requires molecular biology techniques such asPCR and in situ hybridization. The aetiological classifi-cation thus obtained may not only contribute towardimproving our understanding of underlying pathologicalmechanisms, but ultimately may also assist in developingspecific immunomodulatory treatments.
Preliminary results from ongoing treatment trials suggestthat specific antiviral or anti-inflammatory treatmentstrategies are successful in patients who have been carefullyselected and characterized according to biopsy-baseddiagnostic criteria. At present, the optimal timeframe forstarting antiviral or immunosuppressive therapy isspeculative because of lack of data. However, treatmentshould certainly begin as early as possible and before theemergence of serious ventricular dysfunction, becausecomplete normalization of ventricular function is unlikelyto be achieved once serious myocardial damage hasoccurred.
References[1] Hosenpud JD, Bennett LE, Keck BM, et al. The Registry of the
International Society for Heart and Lung Transplantation: six-teenth official report: 1999. J Heart Lung Transplant 1999; 18:611–26.
[2] Elliot P. Diagnosis and management of dilated cardiomyopathy.Eur Heart J 2000; 84: 106–112.
[3] Michels V, Moll, P, Miller, et al. The frequency of familial dilatedcardiomyopathy in a series of patients with idiopathic dilatedcardiomyopathy. N Engl J Med 1992; 326: 77–82.
[4] Richardson P, McKenna W, Bristow M, et al. Report of the 1995World Health Organization/International Society and Federationof Cardiology Task Force on the Definition and Classification ofcardiomyopathies [news]. Circulation 1996; 93: 841–2.
[5] Kuhl U, Noutsias M, Seeberg B, et al. Immunohistologicalevidence for a chronic intramyocardial inflammatory process indilated cardiomyopathy. Heart 1996; 75: 295–300.
[6] Feldmann AM, McNamara D. Myocarditis. N Engl J Med 2000;343: 1388–98.
[7] Liu PP, Mason JW. Advances in the understanding of myocarditis.Circulation 2001; 104: 1076–82.
[8] Baboonian C, Treasure T. Meta-analysis of the association ofenteroviruses with human heart disease. Heart 1997; 78: 539–43.
[9] Kawai C. From myocarditis to cardiomyopathy: mechanisms ofinflammation and cell death: learning from the past for the future.Circulation 1999; 99: 1091–100.
Diagnosis and treatment of virus-induced inflammatory cardiomyopathy I79
Eur Heart J Supplements, Vol. 4 (Suppl I) December 2002
90
80
70
60
Before After Before After Before AfterTreatment Treatment Treatment
P < 0·05
EF(%) EF(%) EF(%)EF>55% 30%>EF<55%
70
60
50
40
P < 0·001 P < 0·05
60
50
40
30
20
10
0
EF<30%
(a)
n=2
n=13
n=16
n=10
11
14
15
1
Before AfterTreatment
NYHA
I
II
III
IV
(b)
Figure 6 (a) Haemodynamic improve-ment in patients with mild (leftventricular ejection fraction [EF] >55%),moderate (EF 30–55%) and severe (EF<30%) left ventricular dysfunction duringimmunosuppressive treatment (n = 41).(b) Clinical improvement (in terms ofNew York Heart Association [NYHA]classification) of patients during immuno-suppressive treatment (n = 41).
Dow
nloaded from https://academ
ic.oup.com/eurheartjsupp/article-abstract/4/suppl_I/I73/442320 by guest on 03 April 2019
[10] Pauschinger M, Bowles NE, Fuentes-Garcia FJ, et al. Detectionof adenoviral genome in the myocardium of adult patients withidiopathic left ventricular dysfunction. Circulation 1999; 99:1348–54.
[11] Badorff C, Noutsias M, Kuhl U, et al. Cell-mediated cytotoxicityin hearts with dilated cardiomyopathy: correlation with interstitialfibrosis and foci of activated T lymphocytes. J Am Coll Cardiol1997; 29: 429–34.
[12] Fairweather D, Kaya Z, Shellam GR, et al. From infection toautoimmunity. J Autoimmun 2001; 16: 175–86.
[13] Noutsias M, Pauschinger M, Schultheiss H, et al. Phenotypiccharacterization of infiltrates in dilated cardiomyopathy: diagnos-tic significance of T-lymphocytes and macrophages in inflamma-tory cardiomyopathy. Med Sci Monit 2002; 8: CR478–87.
[14] Kuhl U, Toussaint H, Ulrich G, Wagner D, Wolff P, SchultheissHP. Evaluation of immunohistological data for the diagnosis ofmyocarditis. In: Schultheiss HP, ed. New concepts of viral heartdisease. Berlin, Heidelberg, New York, Springer-Verlag, 1988:325–36.
[15] Kuhl U, Noutsias M, Seeberg B, et al. Immunohistologicalevaluation of myocardial biopsies from patients with dilatedcardiomyopathy. J Heart Fail 1994; 9: 231–45.
[16] Kuhl U, Noutsias M, Seeberg B, et al. Chronic inflammation inthe myocardium of patients with clinically suspected dilatedcardiomyopathy. J Card Fail 1994; 1: 13–25.
[17] Noutsias M, Seeberg B, Schultheiss HP, et al. Expression of celladhesion molecules in dilated cardiomyopathy: evidence forendothelial activation in inflammatory cardiomyopathy.Circulation 1999; 99: 2124–31.
[18] Kuhl U, Seeberg B, Schultheiss HP, et al. Immunohistologicalcharacterization of infiltrating lymphocytes in biopsies of patientswith clinically suspected dilated cardiomyopathy. Eur Heart J1994; 15: 62–7.
[19] Noutsias M, Pauschinger M, Ostermann K, et al. Digital imageanalysis system for the quantification of infiltrates and cell adhe-sion molecules in inflammatory cardiomyopathy. Med Sci Monit2002; 8: MT59–71.
[20] Noutsias M, Fechner H, de Jonge H, et al. Human coxsackie-adenovirus receptor is colocalized with integrins alpha(v)beta(3)and alpha(v)beta(5) on the cardiomyocyte sarcolemma and upreg-ulated in dilated cardiomyopathy: implications for cardiotropicviral infections. Circulation 2001; 104: 275–80.
[21] Pauschinger M, Doerner A, Kuehl U, et al. Enteroviral RNA repli-cation in the myocardium of patients with left ventricular dys-function and clinically suspected myocarditis. Circulation 1999;99: 889–95.
[22] Schultheiss HP, Kühl U. Cardiomyopathies and specific heartmuscle diseases. In: Poole-Wilson PA, Coluci C, Massie BN,Chatterje K, eds. Heart failure: scientific principles and clinicalpractice. New York, Chruchill Livingstone; 1997: 423–38.
[23] Schultheiss HP, Pauschinger M, Dörner A, et al. Inflammatory
[24] Dec GW Jr, Palacios IF, Fallon JT, et al. Active myocarditis in thespectrum of acute dilated cardiomyopathies. Clinical features,histologic correlates, and clinical outcome. N Engl J Med 1985;312: 885–90.
[25] Grogan M, Redfield MM, Bailey KR, et al. Long-term outcomeof patients with biopsy-proved myocarditis: comparison withidiopathic dilated cardiomyopathy. J Am Coll Cardiol 1995; 26:80–4.
[26] McCarthy RE, Boehmer JP, Hruban RH, et al. Long-termeoutcome of fulminant myocarditis as compared with acute (non-fulminant) myocarditis. N Engl J Med 2000; 342: 734–5.
[27] Kuhl U, Strauer BE, Schultheiss HP. Methylprednisolone inchronic myocarditis. Postgrad Med J 1994; 70: S35–42.
[28] McNamara DM, Rosenblum WD, Janosko KM, et al. Intravenousimmune globulin in the therapy of myocarditis and acutecardiomyopathy. Circulation 1997; 95: 2476–8.
[30] Gullestad L, Aass H, Fjeld JG, et al. Immunomodulating therapywith intravenous immunoglobulin in patients with chronic heartfailure. Circulation 2001; 103: 220–5.
[31] Staudt A, Schaper F, Stangl V, et al. Immunohistological changesin dilated cardiomyopathy induced by immunoadsorption therapyand subsequent immunoglobulin substitution. Circulation 2001;103: 2681–6.
[32] Wojnicz R, Nowalany-Kozielska E, Wojciechowska C, et al.Randomized, placebo-controlled study for immunosuppressivetreatment of inflammatory dilated cardiomyopathy: two-yearfollow-up results. Circulation 2001; 104: 39–45.
[33] Parrillo JE, Cunnion RE, Epstein SE. A prospective, randomized,controlled trial of prednisolon for dilated cardiomyopathy. N EnglJ Med 1989; 321: 1061–8.
[34] Mason JW, O’Connell JB, Herskowitz A, et al. A clinical trial ofimmunosuppressive therapy for myocarditis. The MyocarditisTreatment Trial Investigators. N Engl J Med 1995; 333: 269–75.