Diaphragm motion and lung function predictionin patients operated for lung cancer – a pilotstudy on 27 patientsDragan R Subotic1*, Ruza Stevic2, Milan Gajic3 and Radomir Vesovic1
Abstract
Background: The influence of the diaphragm motion to the accuracy of postoperative lung function predictionafter the lung resction is still debatable.
Methods: Prospective study that included 27 patients who underwent a lung resection for cancer. Diaphragmmovements were assessed radiographically and by ultrasonography before the operation and postoperatively, withthe lung fully expanded. The relationship between the diaphragm movements and differences between ppo FEV1and measured postoperative FEV1, was analysed by expressing diaphragm movements as preoperative diaphragmamplitudes, preoperative-postoperative amplitude differences or in relation to fixed intrathoracic distances.
Results: The mean difference between preoperative and postoperative diaphragm amplitudes of the diseased sidewas 2.42 ± 1.25 cm and 2.11 ± 2.04 cm when measured radiographically and by ultra sound respectively (p > 0.05).A significant positive correlation was found for the entire group only between the patients’ height and thedifferences ppo FEV1 - actual FEV1: the prediction was more unprecise in taller patients. With the cut-off value of550 ml for differences between ppo FEV1 and actual FEV1, a significant inverse correlation was found only if thepreoperative ipsilateral diaphragm amplitude was presented as a percentage of the preoperative apex-base distancein inspiration. For right-sided tumours, the greater the difference between preoperative and postoperative ipsilateraldiaphragm amplitudes, the greater discrepancy between predicted and actual postoperative FEV1. For left-sidedtumours, inverse correlation existed if the preoperative diaphragm amplitude was presented as a percentage of thepreoperative distance apex-base.
Conclusion: Diaphragm movements influence the accuracy of the postoperative lung function prediction.
BackgroundThe postoperative lung function prediction represents aroutine in COPD patients undergoing a lung resection [1].Despite the modern technology, a certain difference mayexist between the predicted and postoperative ventilatoryparameters (in some COPD patients up to 30%), in a waythat ppoFEV1 may be either underestimated or overesti-mated [2,3].As a flow-volume loop does not recognize“ the
position and the motion of each haemidiaphragm, we
hypothesised that diaphragm movements might contrib-ute to these differences. Previous pleural infections maylead to the topography opposite to normal and to differ-ent motion of haemidiaphragms, thus contributing tothe inaccuracy of postoperative lung function prediction.We set up to determine whether diaphragm motion con-
tributes to differences between predicted and actual postop-erative ventilatory function. Also, the aim of the study wasto assess the reliability of radiographic and ultrasonographicmethods to investigate the diaphragm movements in aclinical setting.
* Correspondence: [email protected] for Thoracic Surgery, Clinical Center of Serbia, University of BelgradeSchool of Medicine, 26/20, Visegradska Street, 11000 Belgrade, SerbiaFull list of author information is available at the end of the article
MethodsProspective study on 27 patients with a lung resectionfor primary lung cancer.Inclusion criteria: complete resection, uneventful postop-
erative course, full collaboration with the patient whilemeasuring diaphragm movements.In all patients, diaphragm movements on both sides were
assessed radiographically and by ultrasonography beforethe operation and at the first outpatient control, 7-10 daysafter discharge, with the full and stable lung expansion.The baseline lung function was classified according to
GOLD criteria [4].For patients undergoing a lobectomy, the predicted
postoperative FEV1 (ppo FEV1) was calculated by using aNakahara formula [5]:
where [n] relates to the total number of subsegments inthe lobe to be removed, whilst [a] relates to the numberof subsegments obstructed by the tumor.For patients undergoing a pneumonectomy, a Juhl-
Frost equation [6] was used:
ppoFEV1 ¼ FEV1 � 1−S � 0:0526ð Þ
where S is the number of resected lung segments, andeach segment accounts for 1/19 of total lung function.Postoperative spirometry was done the same day as
the assessment of the diaphragm movements, as alreadydescribed.
Radiographic measurementBoth preoperative and postoperative chest radiographieswere done with a patient in the upright position. Postopera-tively, radiographies were done synchronously with theultrasonographic measurements, as described.On the chest radiography, the distance between the infer-
ior margin of the second rib posteriorly and horisontal linetangential to the diaphragm dome was measured in deepinspiration (distance a) and deep expiration (distance b)(Figure 1). The preoperative amplitude of the diaphragmmovements (A1) on each side was calculated by substract-ing the aforementioned distance in expiration (b1) from thesame distance measured in inspiration (a1): A1 = a1–b1.The same calculation was used to determine the post-
operative amplitude (A2), where a2 and b2 correspond topostoperative values of the same distances as in theprevious formula:
A2 ¼ a2–b2:
The difference between preoperative and postoperativeamplitudes on each side was calculated the formula:ΔA =A1–A2.For the data analysis and assessment of correlation
with the lung function prediction, the difference betweenpreoperative and postoperative amplitudes on diseasedside was expressed as a percent of the preoperative amp-litude:
ΔA %ð Þ¼ΔA � 100=A1:
For the same purpose, the preoperative ipsilateraldiaphragm amplitude was presented as a percentage
Figure 1 Radiographic measurement of diaphragm movements.
Subotic et al. Journal of Cardiothoracic Surgery 2013, 8:213 Page 2 of 7http://www.cardiothoracicsurgery.org/content/8/1/213
of the preoperative apex-base distance in inspir-ation:
A1 %ð Þ ¼ A1 � 100=a1
Ultra-sonographic measurementWith the patient in the supine, 45° semirecumbent pos-ition, a 3.75-MHz convex transducer was placed subcos-tally between the mid-clavicular and mid-axillary linesymmetrically to obtain a sagital plane of the hemidiaph-ragm during all phases of respiration. After identifyingthe dome of the right and left hemidiaphragm, two-dimensional (2D) scans were performed, by using a real-time gray scale technology in the sagital plane, thatincluded the maximal renal bipolar length. The positionof the diaphragm was measured relative to the renal pel-vis from the 2D images obtained. Craniocaudal excur-sion was measured from the renal pelvis to a point onthe diaphragm lying at the same depth from the trans-ducer on the ultrasonographic scan (Figure 2). The dis-tance between these points was measured on maximalinspiration and at the end of a forced expiration. Foreach maneuver, at least three satisfactory readings weretaken before selecting a value to be used for analysis.
Data analysisA comparison was made between diaphragm amplitudeson both sides before and after the lung resection.Differences between preoperative and postoperative
diaphragm amplitudes were analysed depending on themeasurement method.As for the relationship between the diaphragm move-
ments and differences between ppo FEV1 and measuredpostoperative FEV1, diaphragm movements were expressedboth in form of preoperative diaphragm amplitudes, orpreoperative-postoperative amplitude differences calculatedby two methods.The existence of eventual correlation between the
FEV1 prediction accuracy and tumour side, extent ofresection, patient’s age and health was also investigated.
Ethic approvalFor prospective studies using data of patients as a part ofmedical routine, the institutional policy is that such type ofstudies should be approved by the department head, whatwas the case for the present study.
StatisticsT test for equality of means, paired samples test, Pearsoncorrelation.
ResultsOf 35 operated patients who completed the protocol,after having eliminated eight patients for different rea-sons, a total of 27 patients were enrolled in the study.There were 21 males and 6 females (M/F 3.5:1), aged58.5 ± 8.5 years.Lobectomy and pneumonectomy were done in 21 and
six patients respectively.Tumour localisation was peripheral, within different
lobes in 21 patients, in whom lobectomy was done. Fourpatients with tumours in the right hilar region and twopatients with tumours in the left hilar region, underwenta pneumonectomy.According to GOLD criteria, 11(40.7%) had COPD of
different severity. Stage I COPD existed in six patients,whilst stages II and III existed in two patients each.Preoperative and postoperative values of the lung func-
tion parameters, as well as their differences, are presentedon Table 1.Of 6 patients with a pneumonectomy, difference between
predicted and postoperatively measured FEV1 was <250 mlin three patients, in one patient it was 250-300 ml, whilst intwo patients it was >300 ml. The mean predicted-measuredFEV1 difference in the pneumonectomy and lobectomygroups was 339 vs. 399.9 ml (P > 0.05).
Figure 2 Ultra-sonographic measurement of diaphragmmovements. Craniocaudal ultrasound image of the right diaphragmduring inspiration (top) and expiration (bottom). Hemidiaphragmmovements are measured as shown (arrows).
Subotic et al. Journal of Cardiothoracic Surgery 2013, 8:213 Page 3 of 7http://www.cardiothoracicsurgery.org/content/8/1/213
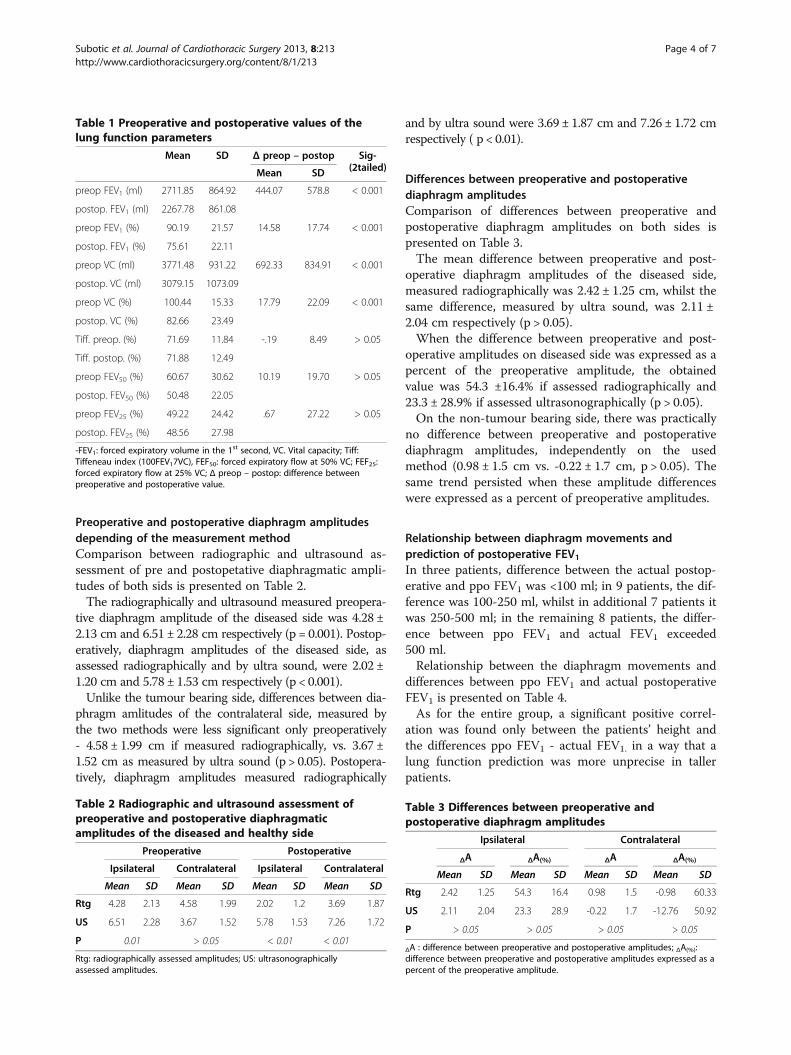
Preoperative and postoperative diaphragm amplitudesdepending of the measurement methodComparison between radiographic and ultrasound as-sessment of pre and postopetative diaphragmatic ampli-tudes of both sids is presented on Table 2.The radiographically and ultrasound measured preopera-
tive diaphragm amplitude of the diseased side was 4.28 ±2.13 cm and 6.51 ± 2.28 cm respectively (p = 0.001). Postop-eratively, diaphragm amplitudes of the diseased side, asassessed radiographically and by ultra sound, were 2.02 ±1.20 cm and 5.78 ± 1.53 cm respectively (p < 0.001).Unlike the tumour bearing side, differences between dia-
phragm amlitudes of the contralateral side, measured bythe two methods were less significant only preoperatively- 4.58 ± 1.99 cm if measured radiographically, vs. 3.67 ±1.52 cm as measured by ultra sound (p > 0.05). Postopera-tively, diaphragm amplitudes measured radiographically
and by ultra sound were 3.69 ± 1.87 cm and 7.26 ± 1.72 cmrespectively ( p < 0.01).
Differences between preoperative and postoperativediaphragm amplitudesComparison of differences between preoperative andpostoperative diaphragm amplitudes on both sides ispresented on Table 3.The mean difference between preoperative and post-
operative diaphragm amplitudes of the diseased side,measured radiographically was 2.42 ± 1.25 cm, whilst thesame difference, measured by ultra sound, was 2.11 ±2.04 cm respectively (p > 0.05).When the difference between preoperative and post-
operative amplitudes on diseased side was expressed as apercent of the preoperative amplitude, the obtainedvalue was 54.3 ±16.4% if assessed radiographically and23.3 ± 28.9% if assessed ultrasonographically (p > 0.05).On the non-tumour bearing side, there was practically
no difference between preoperative and postoperativediaphragm amplitudes, independently on the usedmethod (0.98 ± 1.5 cm vs. -0.22 ± 1.7 cm, p > 0.05). Thesame trend persisted when these amplitude differenceswere expressed as a percent of preoperative amplitudes.
Relationship between diaphragm movements andprediction of postoperative FEV1In three patients, difference between the actual postop-erative and ppo FEV1 was <100 ml; in 9 patients, the dif-ference was 100-250 ml, whilst in additional 7 patients itwas 250-500 ml; in the remaining 8 patients, the differ-ence between ppo FEV1 and actual FEV1 exceeded500 ml.Relationship between the diaphragm movements and
differences between ppo FEV1 and actual postoperativeFEV1 is presented on Table 4.As for the entire group, a significant positive correl-
ation was found only between the patients’ height andthe differences ppo FEV1 - actual FEV1. in a way that alung function prediction was more unprecise in tallerpatients.
Table 1 Preoperative and postoperative values of thelung function parameters
Table 3 Differences between preoperative andpostoperative diaphragm amplitudes
Ipsilateral Contralateral
ΔA ΔA(%) ΔA ΔA(%)
Mean SD Mean SD Mean SD Mean SD
Rtg 2.42 1.25 54.3 16.4 0.98 1.5 -0.98 60.33
US 2.11 2.04 23.3 28.9 -0.22 1.7 -12.76 50.92
P > 0.05 > 0.05 > 0.05 > 0.05
ΔA : difference between preoperative and postoperative amplitudes; ΔA(%):difference between preoperative and postoperative amplitudes expressed as apercent of the preoperative amplitude.
Subotic et al. Journal of Cardiothoracic Surgery 2013, 8:213 Page 4 of 7http://www.cardiothoracicsurgery.org/content/8/1/213
If the analysis of the influence of diaphragm move-ments to the lung function prediction was performed bysplitting the differences between ppo FEV1 and actualFEV1 to <550 ml and >550 ml, a significant inverse cor-relation was found only if the preoperative ipsilateraldiaphragm amplitude was presented as a percentage ofthe preoperative apex-base distance in inspiration – thegreater percentage, the smaller prediction discrepancy.A certain influence of the tumour side to the postoper-
ative lung function prediction was also registered. Inpatients with right-sided tumours, the greater thedifference between preoperative and postoperative ipsi-lateral diaphragm amplitudes, the greater discrepancybetween predicted and actual postoperative FEV1. Inpatients with left-sided tumours, inverse correlation wasfound if the preoperative diaphragm amplitude waspresented as a percentage of the preoperative distanceapex-base; the greater the percentage, the smallerprediction discrepancy.No significant correlation existed if diaphragm move-
ments of the entire group were expressed either in formof preoperative diaphragm amplitudes, or preoperative-postoperative amplitude differences calculated by twomethods.No significant correlation between the diaphragm
movements and lung function prediction was found ifthe analysis was done depending on whether lobectomyor pneumonectomy was done (not shown on Table).
DiscussionBefore discussing the obtained results, two points shouldbe clarified.
First, despite the reported linear relationship between dia-phragmatic excursion and inspired volumes [7], it was alsosuggested that diaphragm movements, measured by ultra-sonography, poorly reflect the pulmonary function [8]. Theexplanation that various inspiratory volumes are measuredfor the same diaphragmatic excursion, is not evidence-based.Second, the point of the radiographically determined
normal position of the right hemidiaphragm at the levelof the anterior sixth rib, appears to originate from a sin-gle study [9,10]. An obstacle for such a way of referen-cing a diaphragm position is a poor visibility of costalportions of the anterior ribs. Thoracic spine has alsobeen used as a reference point, but without validation inpopulation studies [11,12].Having in mind these limitations, our method, based
on the diaphragm apex as a determinant of the dia-phragm position, could also be put into question be-cause of use of the postero-anterior projection only,without analysis of movements in the lateral projection.However, studies that analysed both diaphragm apex andcostophrenic angle movements, showed that both move-ments were synchronous and followed a linear relation-ship [13], thus justifying our method of measurement.Finally, related to the method of the postoperative lung
function prediction, although it was demonstrated thatboth perfusion scintigraphy and Juhl-Frost formula maycorrelate well with the observed postoperative FVC andFEV1, the superiority of calculation by using a perfusionscintigraphy was clearly demonstrated [14]. We used theJuhl-Frost method because Nakahara formula is not suit-able for pneumonectomy and because the primary study
Table 4 Relationship between diaphragm movements and prediction of postoperative FEV1
Pearson correlation p t-test for equation of means
A1 ipsilateral (Rtg): preoperative amplitude of the ipsilateral diaphragm measured radiographically; A1 ipsilateral (US): the same amplitude measuredultrasonographically; ΔA ipsilateral (Rtg): difference between the preoperative and postoperative amplitudes measured radiographically; ΔA ipsilateral (US): thesame difference measured ultrasonographically; Δa ipsilateral inspirium.: difference between preoperative and postoperative value of the apex-diaphragm domedistance in deep inspiration; Δa ipsilateral insp (%):Δa ipsilateral insp expressed as a% of the apex-diaphragm dome distance in deep inspiration; A1(%): the pre-operative ipsilateral diaphragm amplitude as a percentage of the preoperative apex-diaphragm dome distance in inspiration; A2(%): the postoperative ipsilateraldiaphragm amplitude as a percentage of the preoperative apex-diaphragm dome distance in inspiration; *: right sided tumours; #: left sided tumours; §: cut-offvalue of 550 ml for the differences between ppo FEV1 and actual FEV1.
Subotic et al. Journal of Cardiothoracic Surgery 2013, 8:213 Page 5 of 7http://www.cardiothoracicsurgery.org/content/8/1/213
end point was a diaphragm motion, not the predictionmethod itself. We routinely use perfusion lung scintig-raphy in patients with moderate and severe COPD, thatwas not a case in a subset of patients with a pneumonec-tomy in the present study.In the present study, preoperative diaphragm ampli-
tudes determined by ultrasound are in the range of thosedetermined in other studies being 6 to 7 cm, 6 ± 0.7 cmor 6.8 ± 0.8 cm [15]. However, preoperative diaphragmamplitudes differed both depending on the measurementmethod and diaphragm side. Ultrasonographically mea-sured amplitudes were significantly higher vs. radio-graphically determined ones (4.28 ± 2.13 cm and 6.51 ±2.28 cm) only on the diseased side. There are no litera-ture data to compare these results. The probable explan-ation of the obtained differences is the fact that thereference points for registering diaphragm movementswere different, as described in the methods section. Infact, the current study design did not anticipate ampli-tudes to closely correspond to each other, but to assesstheir eventual influence to the lung function prediction.Similarly, it can only be speculated why these differ-
ences were smaller on the contralateral side (4.58 ±1.99 cm vs. 3.67 ± 1.52 cm).On the other hand, differences in side-to-side diaphrag-
matic motion are more analysed – ultrasonographicallymeasured values outside the range of 0.5 to 1.6 for theright-to-left ratio of maximal excursion on deap breathingshould be considered as abnormal [16]. It can explain ourultrasonographically measured amplitudes on the diseasedand contralateral side being 6.51 ± 2.28 cm vs. 3.67 ±1.52 cm. Difficulties in left hemidiaphragm visualisation areusually regarded as possible cause of these side-to-side dif-ferences. So, in one study, the diaphragmatic motion of theleft hemidiaphragm was recorded in only 45/210 (21%)subjects [17]. Another study failed to record left hemidiaph-ragm excursion in 15/23(65%) volunteers [18]. This becausethe left hemidiaphragm may be obscured by the expandinglung during deep breathing and the position of the probemay not be readily adjusted as the spleen window is small.The ultrasonographic side-to-side amplitude differences
were more pronounced compared with those measuredradiographically - 4.28 ± 2.13 cm vs. 4.58 ± 1.99 cm. Al-though the relevance of the side-to-side diaphragmatic mo-tion comparison has been noted in fluoroscopy studies[19], there are no available literature data trying to explainit.As expected, after the lung resection, both radiographic-
ally and ultrasonographically measured diaphragm ampli-tudes of the diseased side decreased. On the opposite side,the same trend existed only when amplitudes were deter-mined radiographically. When assessed by ultra sound,postoperative amplitudes on the non-tumour bearing sidewere higher compared with preoperative ones.
Concerning postoperative percent change of preopera-tive and postoperative amplitudes, in relation to pre-operative values, both methods followed the same trendof postoperative amplitude decrease on the diseased side- 54.3 ± 16.4% and 23.3 ± 28.9% decrease respectivelywhen assessed radiographically and ultrasonographically.As expected, on the non-tumour bearing side, there wasno difference between preoperative and postoperativediaphragm amplitudes, independently on the usedmethod.Concerning the primary end point of this study - influ-
ence of the diaphragm movements to discrepancy betweenthe predicted and actual postoperative lung function, it isevident that some aspects of the diaphragm motility maysignificantly contribute to the lung function prediction, butnot as independent factor.Absence of significant influence of the extent of resection
to the lung function prediction is important for practice. Alung function prediction may be more delicate if a lobec-tomy is anticipated, with several different methods of thelung function prediction being in use, as opposed to a verysimple calculation before pneumonectomy by using a per-fusion lung scintigraphy [20]. However, the small numberof patients with pneumonectomy in the analysed groupdoes not allow firm conclusions about the influence of theextent of resection.As presented, different ways of expressing diaphragm am-
plitudes were used in attempt to assess eventual correlationwith the lung function prediction. In our study, a significantcorrelation between diaphragm movements and lung func-tion prediction existed only if the diaphragm movementswere presented as 1) diaphragm amplitude as a percentageof the preoperative apex-base distance in inspiration, or 2)as a difference between preoperative and postoperative ipsi-lateral diaphragm amplitudes. These facts, together with asignificant influence of a patients’ height to the lung func-tion prediction, support the need to express the amplitudesof the diaphragm movements in relation to some fixed dis-tance or to take into consideration the loss in diaphragmamplitudes, rather than to correlate absolute values of am-plitudes. The exception are emphysema patients, in whommagnetic resonance revealed smaller mean excursions thanin control subjects and movements of the ventral portionof the diaphragm in paradox to the change in lung area[21]. Such a bias did not exist in the present study.Of practical benefit could be our finding that accurate
registering of diaphragm movements may predictwhether the difference between ppo FEV1 and actualFEV1 will exceed 550 ml.
Study limitationsBeside the limited patient number, one additional pointshould be clarified. Almost identical results were ob-tained by the two methods in relation to the mean
Subotic et al. Journal of Cardiothoracic Surgery 2013, 8:213 Page 6 of 7http://www.cardiothoracicsurgery.org/content/8/1/213
difference between preoperative and postoperative dia-phragm amplitudes of the diseased side, (2.42 ± 1.25 cmmeasured radiographically, vs 2.11 ± 2.04 cm by ultra-sound (p > 0.05). It may be confusing, having in mindsignificant differences in both preoperative and postop-erative diaphragm amplitudes, depending on the usedmethod. In our opinion, the key point is not related tothe measurement method, but to the real change in pre-operative vs. postoperative diaphragm movement. Sucha statement is supported by our results showing a cleardifference between preoperative and postoperative am-plitudes on diseased side, but only if they were expressedas a percent of the preoperative amplitudes, (54.3±16.4% measured radiographically vs 23.3 ± 28.9% mea-sured by ultrasound). Although these differences did notreach the level of statistical significance, they are evidentand it is an important achievement of a pilot study,giving a direction for further research.The identical trend of the obtained results means that
the measurement method is not essential.We are convinced that a limited patient number,
together with some methodological inconsistencies thatmay be attributed to both methods, may influence theseresults.
ConclusionThis is the first study addressing the question whetherand in which way the diaphragm motion influences thepostoperative lung function prediction. The exact way ofthis influence is still unclear. The present study was notable to suggest the cut-off values for amplitude intervalsor their ratios with some fixed intrathoracic distancethat could be reproducible and reliable for routine lungfunction prediction. We believe that it will be possibleon larger patient series.
AbbreviationsFEV1: Forced expiratory volume in the first secondppo: FEV1 predictedpostoperative FEV1COPD: Chronic obstructive pulmonarydiseaseGOLD: Global strategy for the diagnosis management and preventionof obstructive lung diseases.
Author details1Clinic for Thoracic Surgery, Clinical Center of Serbia, University of BelgradeSchool of Medicine, 26/20, Visegradska Street, 11000 Belgrade, Serbia.2Institute for Radiology, Center of Serbia, University of Belgrade School ofMedicine, 26/20, Visegradska Street, 11000 Belgrade, Serbia. 3Institute forMedical Statistics, University of Belgrade School of Medicine, 26/20,Visegradska Street, 11000 Belgrade, Serbia.
Received: 8 July 2013 Accepted: 28 October 2013Published: 18 November 2013
References1. Brunelli A, Charloux A, Bolliger C, on behalf of European Respiratory Society,
European Society of Thoracic Surgeons joint task force on fitness for radicaltherapy, et al: ERS-ESTS clinical guidelines for evaluating fitness forradical treatment (surgery and chemoradiotherapy) in patients with lungcancer. Eur Respir J 2009, 34:17–41.
2. Varela G, Brunelli A, Rocco G, et al: Predicted versus observed FEV1 in theimmediate postoperative period after pulmonary lobectomy.Eur J Cardiothorac Surg 2006, 30:644–648.
3. Ueda K, Tanaka T, Hayashi M, Li TS, Kaneoka T, Tanaka N, Hamano K:Compensation of pulmonary function after upper lobectomy versuslower lobectomy. J Thorac Cardiovasc Surg 2011, 142:762.
4. Fabbri LM, Hurd SS: Global strategy for the diagnosis, management andprevention of COPD: 2003 update. Eur Respir J 2003, 22:1–2.
5. Nakahara K, Monden Y, Ohno K, Miyoshi S, Maeda H, Kawashima Y: Amethod for predicting postoperative lung function and its relation topostoperative complications in patients with lung cancer. Ann ThoracSurg 1985, 39:260–265.
6. Juhl B, Frost N: A comparison between measured and calculated changesin the lung function after operation for pulmonary cancer.Acta Anaesthesiol Scand Suppl 1975, 57:39–45.
7. Cohen E, Mier A, Heywood P, et al: Excursion-volume relation of the righthemidiaphragm measured by ultrasonography and respiratory airflowmeasurements. Thorax 1994, 49:885–889.
8. Houston JG, Angus RM, Cowan MD, et al: Ultrasound assessment ofnormal hemidiaphragmatic movement: relation to inspiratory volume.Thorax 1994, 49:500–503.
9. Armstrong P: The normal chest. In Imaging of Diseases of the Chest. Editedby Armstrong P. London, UK: Mosby; 2000:21–62.
10. Lennon EA, Simon G: The height of the diaphragm in the chestradiograph of normal adults. Br J Radiol 1965, 38:937–943.
11. Walsh JM, Webber CL, Fahey PJ, et al: Structural change of the thorax inchronic obstructive pulmonary disease. J Appl Physiol 1992, 72:1270–1278.
12. Lando Y, Biselle PM, Shade E, et al: Effect of lung volume reductionsurgery on diaphragm length in severe chronic obstructive pulmonarydisease. Am J Respir Crit Care Med 1999, 159:796–805.
13. Kolar P, Neuwirth J, Šanda J, et al: Analysis of diaphragm movementduring tidal breathing and during its activation while breath holdingusing MRI synchronized with spirometry. Physiol Res 2009, 58:383–392.
14. Smulders SA, Smeenk FWJM, Janssen-Heijnen MLG, Postmus PE: Actual andpredicted postoperative changes in lung function after pneumonectomy.A retrospective analysis. Chest 2004, 125:1735–1741.
15. Targhetta R, Chavagneux R, Ayoub J, et al: Cinétique diaphragmatiquedroite mesurée par ultrasonographie en mode TM avec spirometrieconcomitante chez le sujet normal et asthmatique, Résultatspréliminaries. Rev Med Interne 1995, 16:819–826.
16. Houston JG, Morris AD, Howie CA, et al: Technical report: quantitativeassessment of diaphragmatic movement: a reproducible method usingultrasound. Clin Radiol 1992, 46:405–407.
17. Boussuges A: Diaphragmatic motion studied by M-mode ultrasonog-raphy. Methods, reproducibility, and normal values. Chest 2009,135:391–400.
18. Gerscovich EO, Cronan M, McGahan JP, et al: Ultrasonographic evaluationof diaphragmatic motion. J Ultrasound Med 2001, 20:597–604.
19. Alexander C: Diaphragm movements and the diagnosis of diaphragmaticparalysis. Clin Radiol 1966, 17:79–83.
20. Wernly JA, DeMeester TR, Kirchner PT, Myerowitz PD, Oxford DE, GolombHM: Clinical value of quantitative ventilation-perfusion lung scans in thesurgical management of bronchogenic carcinoma. J Thorac CardiovascSurg 1980, 80:535–543.
21. Iwasava T, Kagei S, Gotoh T, et al: Magnetic resonance analysis ofabnormal diaphragmatic motion in patients with emphysema.ERJ 2002, 19:225–231.
doi:10.1186/1749-8090-8-213Cite this article as: Subotic et al.: Diaphragm motion and lung functionprediction in patients operated for lung cancer – a pilot study on 27patients. Journal of Cardiothoracic Surgery 2013 8:213.
Subotic et al. Journal of Cardiothoracic Surgery 2013, 8:213 Page 7 of 7http://www.cardiothoracicsurgery.org/content/8/1/213