Hospital-Based Health Technology Assessment Difficult Decision Difficult Decision - - Making at User Interface: Making at User Interface: Why The Traditional Approach Doesn’t Work Janet Martin, PharmD, MSc(HTA&M) Director, High Impact Technology Evaluation Centre Co-Director, Evidence-Based Perioperative Clinical Outcomes Research Unit Assistant Professor, Departments of Medicine, Anesthesia & Perioperative Medicine, London Health Sciences Centre, University of Western Ontario, London, Canada
Transcript
Hospital-Based Health Technology Assessment
Difficult DecisionDifficult Decision --Making at User Interface:Making at User Interface:
Why The Traditional Approach Doesn’t Work
Janet Martin, PharmD, MSc(HTA&M)
Director, High Impact Technology Evaluation Centre
Co-Director, Evidence-Based Perioperative Clinical Outcomes Research Unit
Assistant Professor, Departments of Medicine, Anesthesia & Perioperative Medicine,
London Health Sciences Centre, University of Western Ontario, London, Canada
Hospital-Based Health Technology Assessment
Difficult DecisionDifficult Decision --Making at User Interface:Making at User Interface:
Why The Traditional Approach Doesn’t Work
“Truly, Madly, Deeply”
Janet Martin, PharmD, MSc(HTA&M)
Director, High Impact Technology Evaluation Centre
Co-Director, Evidence-Based Perioperative Clinical Outcomes Research Unit
Assistant Professor, Departments of Medicine, Anesthesia & Perioperative Medicine,
London Health Sciences Centre, University of Western Ontario, London, Canada
Many thanks . . .
LHSC
CIHR
CADTH
…our team
LHSC_CSTAR_POS_2C_RGB
Davy Cheng, John Parker, Kirsten Krull-Naraj, Glen Kearns, Richard Jones
Hospital HTA Decision-Making
I. Importance of HTA in HospitalsII. Traditional Decision MakingIII. Key ChallengesIV. ‘Know4Go’ as a SolutionV. Future Directions
Why Hospital HTA?
� Technological innovations are restructuring health care in profoundly beneficial and unsettling ways
� Demand for innovative technologies has outpaced our capacity to provide them
� Technological innovations are especially concentrated in the hospital setting
� Innovations relevant to hospitals often not assessed by national, provincial, or academic HTA units. Even when they are, they are rarely ready for decision-making.
Shortcomings in External HTA
� HTA reports produced by external agencies are useful, but (necessarily) insufficient
� External HTA agencies cannot informatively advise whether our hospital needs another CT scanner, a surgical robot, bifurcated stents, or another fluoroquinolone
� These decisions need to be taken with local considerations of infrastructure, existing technologies, patient population, health professional skills, learning curves, competing priorities
…though, there is room for more collaboration acros s hospitals.
Hospital HTA is Unique
� Fast-paced, real-time, at the point of decision-making
� In collaboration with decision-makers (“end-users”)
� Contextualized to local setting (not hypothetical)
� Accountable to “predictions”� Decision impact is “felt” very quickly
“HTA in a box”Truly, madly, deeply.
Decisions become moral dilemmas.
Hospitals are Costly
30%
Hospitals account for >30% of health care expenditures in Canada (CIHI, 2004)
Then Now
ThenGet the evidence straightGet the evidence straight
“Evidence is biased”
“HTA is biased”
“Numbers are Tortured & Statistics Lie”
Evidence schmevidence…let’s just get on with it
“It works. And, I want it. No time for assessments here.”
“That’s not the way I see it”
New is inherently better.
If it is “better”, it must be “worth it”.
Symptoms ofCompromised Decision-Making
“The evidence doesn’t apply to my patient”� Aprotinin versus Tranexamic Acid”� Antipsychotics for dementia in elderly� Spinal fusion for low back pain� Arthroscopic knee surgery
Obviously the evidence is wrong, because everyone i s still doing it.� Beta-blocker for immediate treatment of AMI� Beta-blocker for patients undergoing non-CV surgery
This place is archaic…only about the cost!� COX-II selective inhibitors not admitted to formula ry� Insulin glargine and detemir not admitted to formular y� Nandrolone not admitted to formulary
Key Challenges: Too Fast or Too Slow Adoption?
� Gizmo Idolatry. Technology is fun� New is better, and certainly more fun� “on the market” means “done deal”� sufficient burden of proof is presumed
� Sooner is better than later� For new technologies (and drugs), there is constant
pressure to take them up� Just let us “try it out”, and then we can decide� May save money
� We have responsibility to be leading edge� Innovation is our job� Teaching is our mandate� Discovery is up to us
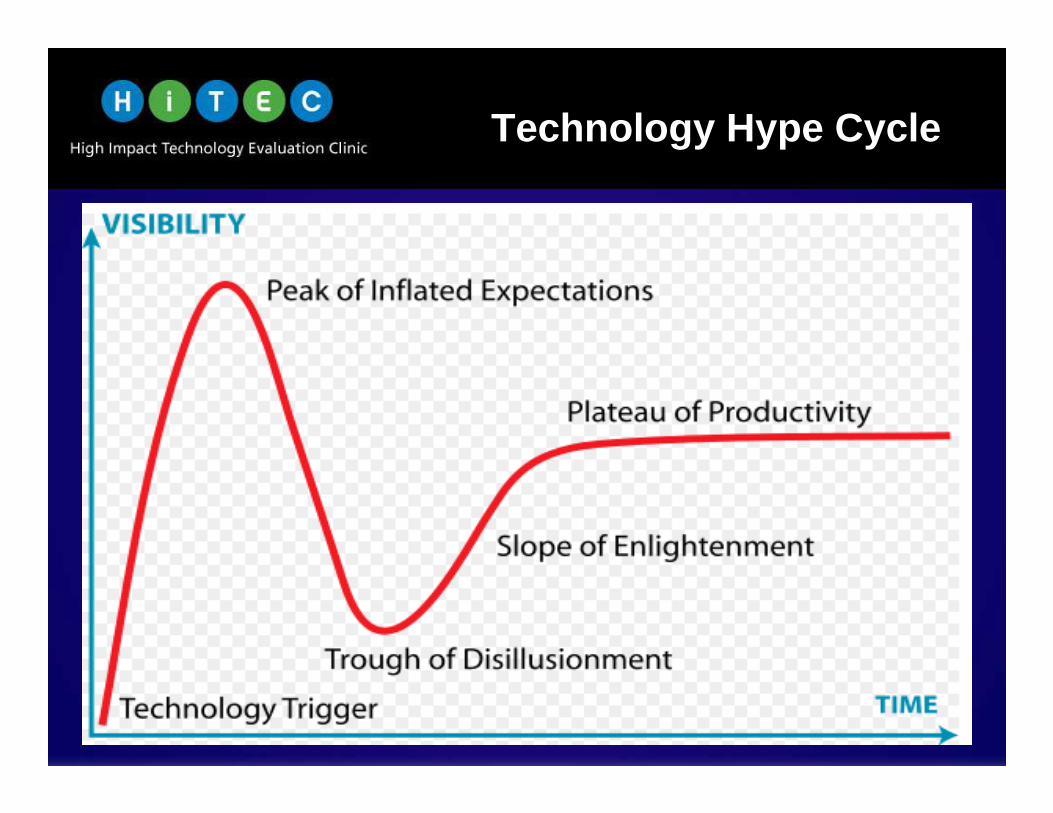
Technology Hype Cycle
Multiple Opposing Pressures
ThenThen
B:R
Comprehensive Meta Analysis V2.exe.lnk
Systematic Review ≠ Decision
Economic Analysis ≠ Decision
Evidence is one consideration, but not the only consideration.
Yes No
Then NowEvidence is essentialEvidence is essential Evidence is essential, Evidence is essential,
but insufficientbut insufficient
Application of Evidence to Decisions:� Too technical � Too linear� Too blunt
Evidence from expanded domains of influence� social, legal, ethical, environmental, etc� opportunity costsneed to be made explicit before decisions can
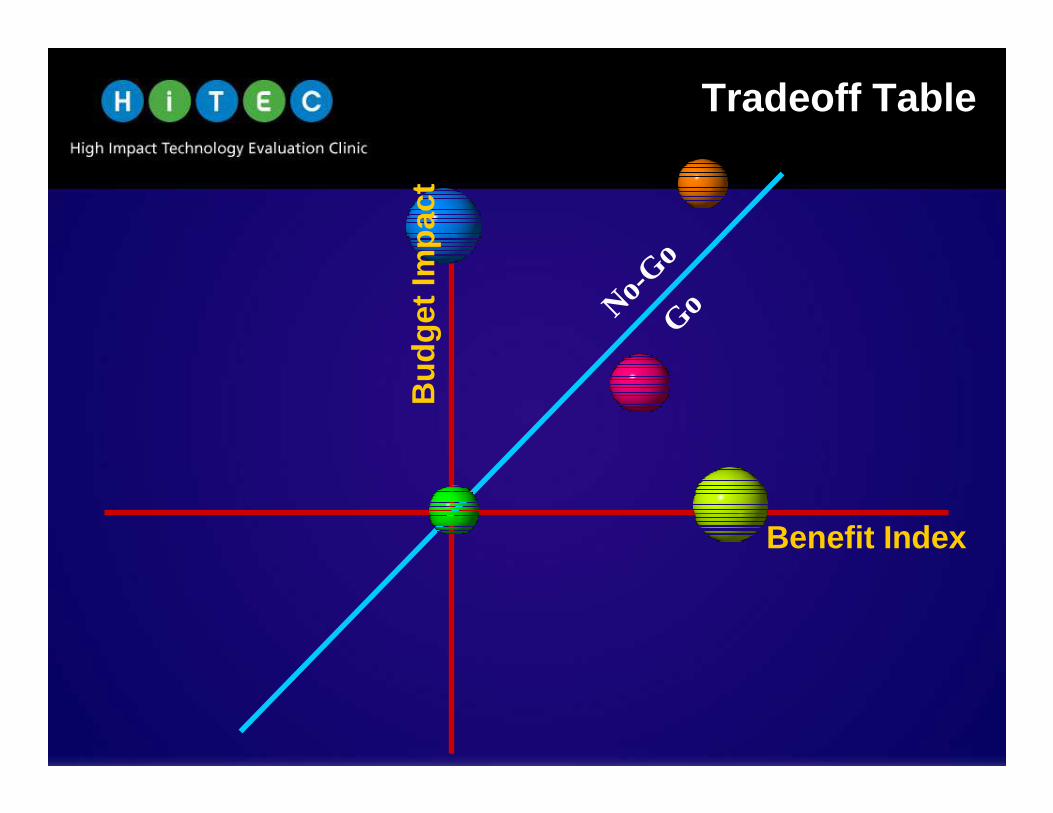
A new approach to increase decisionA new approach to increase decision --maker uptake of best maker uptake of best available evidence:available evidence:
�� Embeds the decision in context of past, present, fu tureEmbeds the decision in context of past, present, fu ture
The average man’s judgment is so poor, he runs a risk
every time he uses it.
- Edgar W. Howe
ThenFocused on “Go”
“just given me the gizmo, and no one gets hurt”
“I don’t see the evidence, do you?”
“it works, and I want it”
“evidence, schmevidence. Just get on with it”
NowFocused on “4Go”“Now I understand”
“Makes sense. I can live with that”
“Finally! You’ve shown me explicitly what I’ve tried to understand for yrs”
“We need to more of this”
“How can we put the whole capital planning through Know4go?”
Summary
� Hospital HTA juxtaposes evidence, decision-makers, and opportunity costs within a fixed set of resources and circumstances (a perfect petri dish)
� Traditional evidence-based decision-making forces a linear approach to what should be nuanced and multifactorialdecision-making
� If we are to engage rather than alienate the end-user, we need to make HTA relevant, explicit and tangible
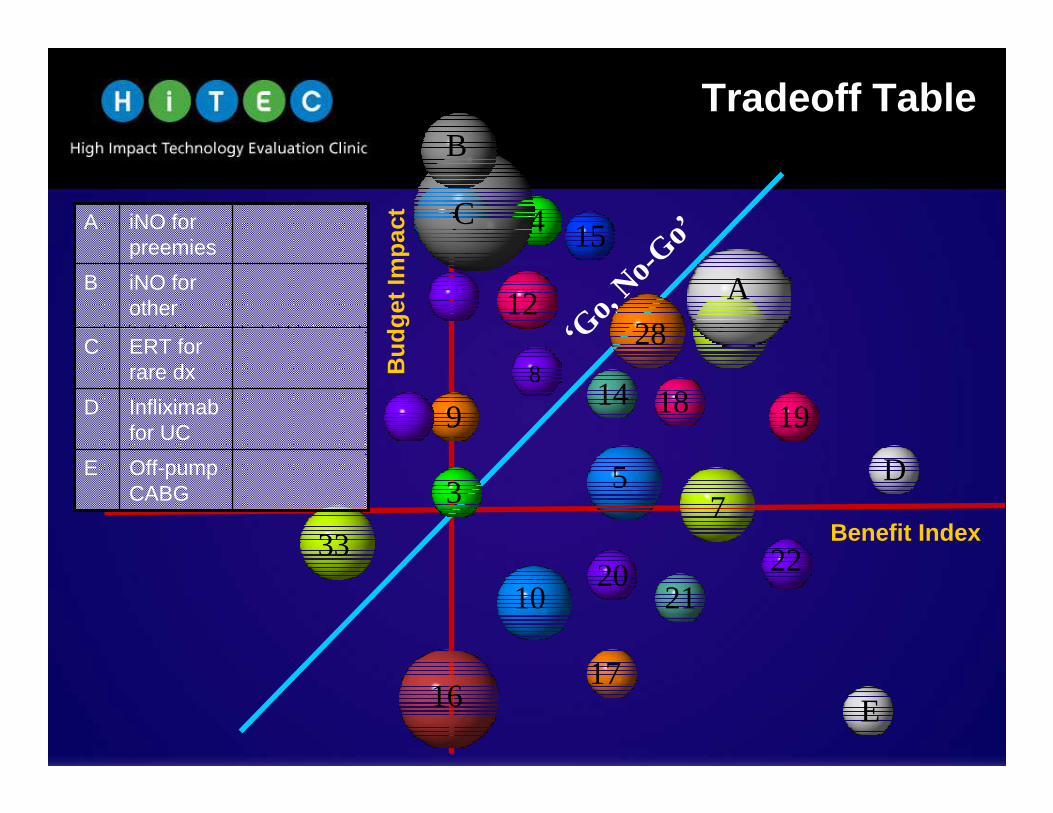
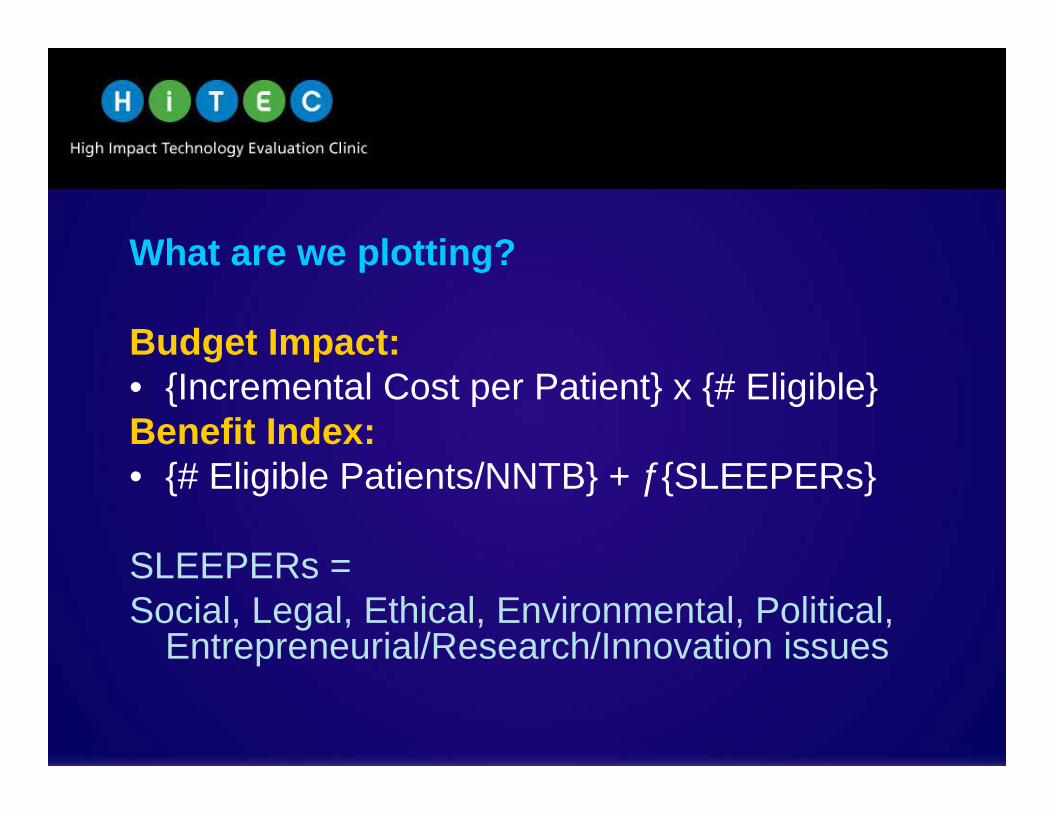
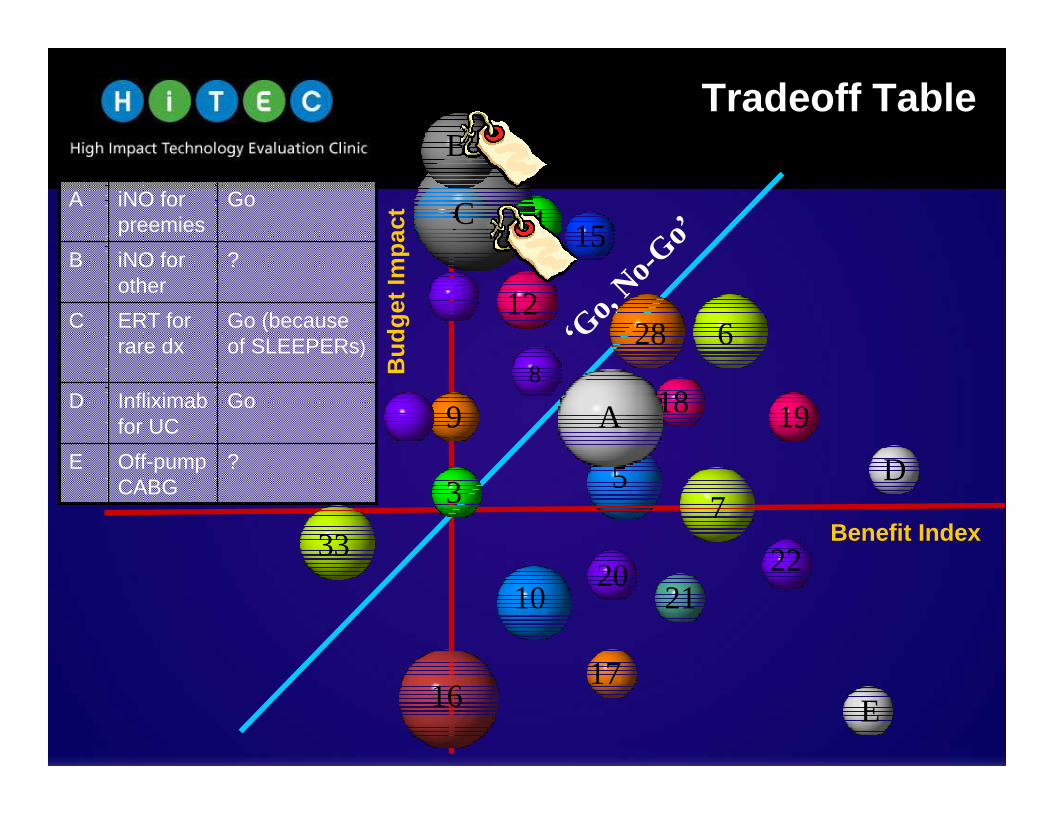
� Know4Go provides framework to explicate the evidence, and its uncertainty, while acknowledging the SLEEPERs, and enumerating what is 4Gone.
� Without explicit acknowledgment of SLEEPERs and the 4Go, decisions prematurely trumped by factors other than evidence, and decisions to 4Go anything are unbearable
Future Efforts
“Only in Research” as an alternative to Yes/No decisions� One study commissioned so far: Venofer vs IV Iron Dextran
Decommissioning/Reinvestment� Knee and back surgeries, beta-blockers, cerclage, iNO
Know4Go useful for other settings, other perspectives?� Other hospitals, MOH, regions
Canadian Surgical Technologies & Advanced Robotics (CSTAR)
� A living laboratory for testing surgical devices and procedures, and training for Ontario (John Parker, Director; Kirsten Krull-Naraj, VP)
� SLEEPERs need refining for surgery and devices
� Devices are only inherently as good as the skilled hands that it is within, and the effectiveness of the team around it
Technology Hype Cycle
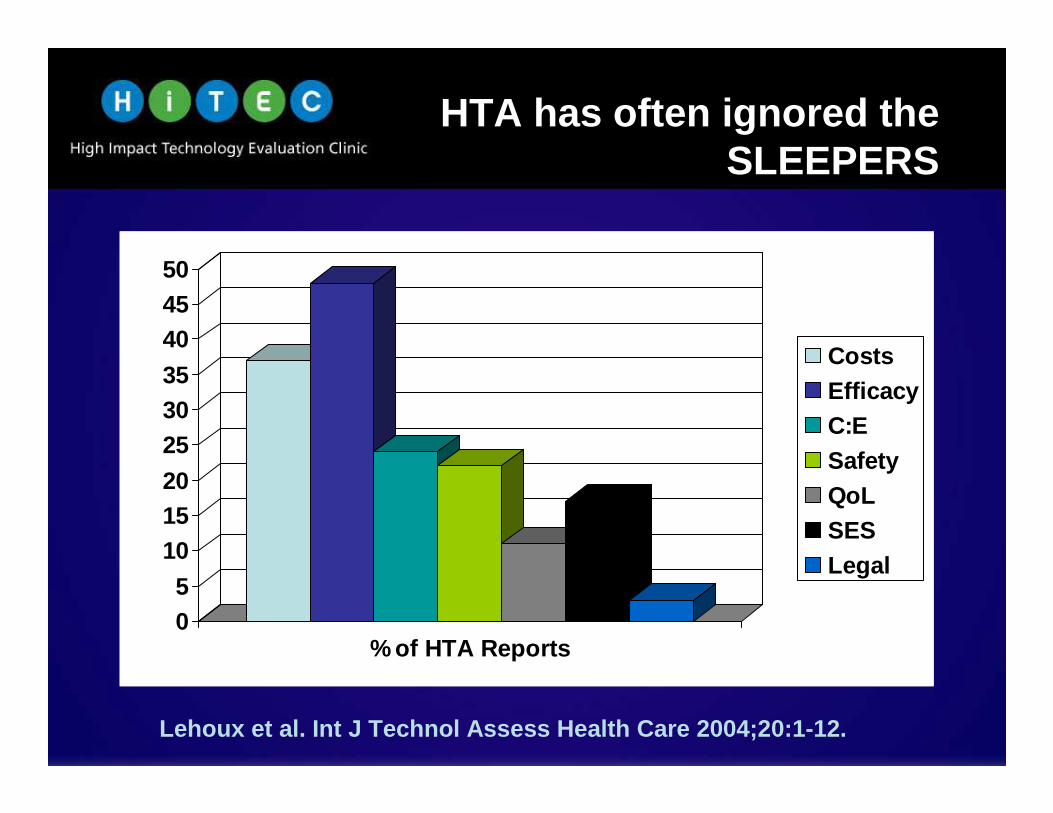
HTA has often ignored the SLEEPERS
05
101520
253035
404550
% of HTA Reports
CostsEfficacyC:ESafetyQoLSESLegal
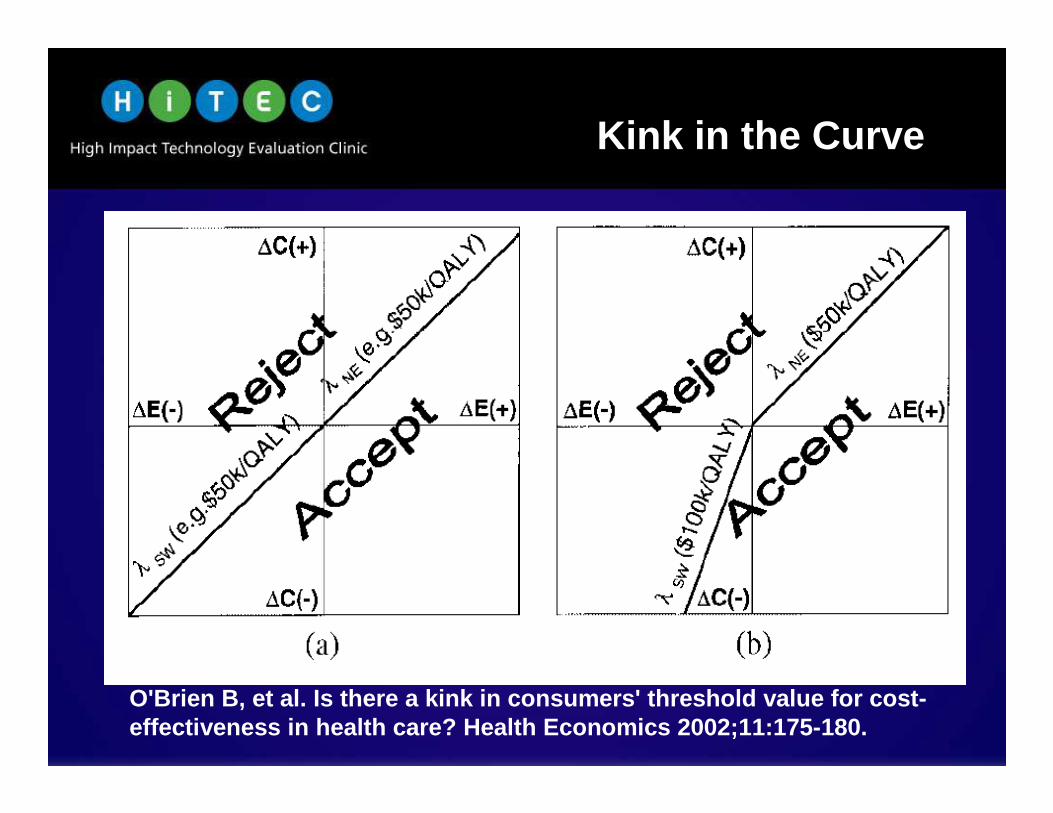
Lehoux et al. Int J Technol Assess Health Care 2004;20 :1-12.
The application of what we know will have a bigger impact on health and disease than any single drug or technology likely to be introduced in the next decade.
Sir Muir Gray
NHS Knowledge Service
We are drowning in informationwhile starving for wisdom.
E.O. Wilson
What we do
LHSC_CSTAR_POS_2C_RGB
HTA Reports
What does it look like?
� Receive Requests during Annual RFP – Administration or Clinicians (formal application process)
� Prioritize Requests– High impact clinically, economically, politically
� Systematically Review Evidence, Resources– Collaborate with requestor and end-users to ensure relevance
– Define benefits, risks, costs, other resource issues
� Stakeholder Meeting (users, non-users) to Elicit SL EEPERS– Elicit the SLEEPERs, Rate their Importance