25
DIFFUSE MALIGNANT MESOTHELIOMA GENERAL THORACIC SURGERY CHAPTER 65
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | belinda-austin |
| View: | 222 times |
| Download: | 5 times |

DIFFUSE MALIGNANT MESOTHELIOMA
GENERAL THORACIC SURGERY
CHAPTER 65
Diffuse malignant pleural mesothelioma
• Uncommon and lethal cancer.
• Currently no standard treatment.
• Asbestos exposure is major risk factors.
• Important for thoracic surgeons to be knowledgeable about mesothilioma – Because they are often called on to make the diagnosis and to recommend treatment.

Epidemiology — Asbestos
• Asbestos belongs to the family of silicate fiber.
• Include two mineralogical groups:
Amphibole and Serpentine.

Amphibole fibers
• Narrow and straight fibers.
• Migrate through the lymphatics of pulmonary parenchyma and accumulate in interstitial space and subpleural region.
• Crocidolite asbestos ( blue asbestos ) -- The most associate with malignant mesothelioma.

Serpentine fibers
• Large, curly shaped fiber.
• do Not travel beyond the major airways.
• Chrysotile ( white asbestos, the only member of Serpentin ) -- More associate with lung cancer.
Diffuse malignant pleural mesothelioma
• Peak age—6th decade.
• Men.
• Long latency period ( at least 20 years ) .
• Incidence—men 15/million, women 3/million.
• Histology—Table 65-2.

Clinical presentation
• Nonspecific,
Chest pain, dyspnea, pleural effusion, pericardial effusion, weight loss, cough, anorexia, weakness, fever, hemoptysis.
• Horner’s syndrome.
• Spontaneous pneumothorax.

Clinical presentation
• Abnormal ECG– Sinus tachycardia (42%).
• Echocardiographic findings.
• No specific tumor marker.
• Rise serum hyaluronan.
• CA-125 (20%).
Radiographic appearance
• Chest-x ray— Variable and related to stage of tumor. • Large pleural effusion, pleural thickening, pleural-
based mass. • Encasement of lung and obliteration of pleural space. • Involve pericardium and pericardial effusion. • Chest wall invasion, invasion through diaphragm. • CT— Most accurate noninvasive way to stage. • PET scan.

Diagnosis
• Thoracentesis, cytology ( positive rate 30-50% ) . • Percutaneous pleural biopsy. • Thoracoscopy. • Open pleural biopsy. • AVOID Exploratory thoracotomy.• Bronchoscopy. • Meidastinoscopy. • Bone scans.
Staging
• Not an accurate, universally accepted staging system.
• Butchart (1976). Table 65-3.
• TNM system. Table 65-4.
• Liver is the most common site of distal metastasis, the contralateral lung is second.


Treatment
• Patient with malignant mesothelioma face a dual problem— Control of the locoregional tumor throughout the course of their disease, prevention of distant metastases as late manifestation of their cancer.
• Choice of treatment – Location and extent of he tumor, the general medical condition of patient.
• Surgery, radiation, chemotherapy, immunotherapy, supportive care.
Radiation therapy
• Difficult to evaluate the success of radiation therapy as the only treatment.
• Usually given in conjunction with surgical resection or chemotherapy.
• Limited by the volume of primary tumor that invole entire hemithorax, proximity of the tumor to many vital structures that intolerant high doses of radiation.
• 4500 cGy. • Adjuvant treatment after surgical resection of gross
tumor.
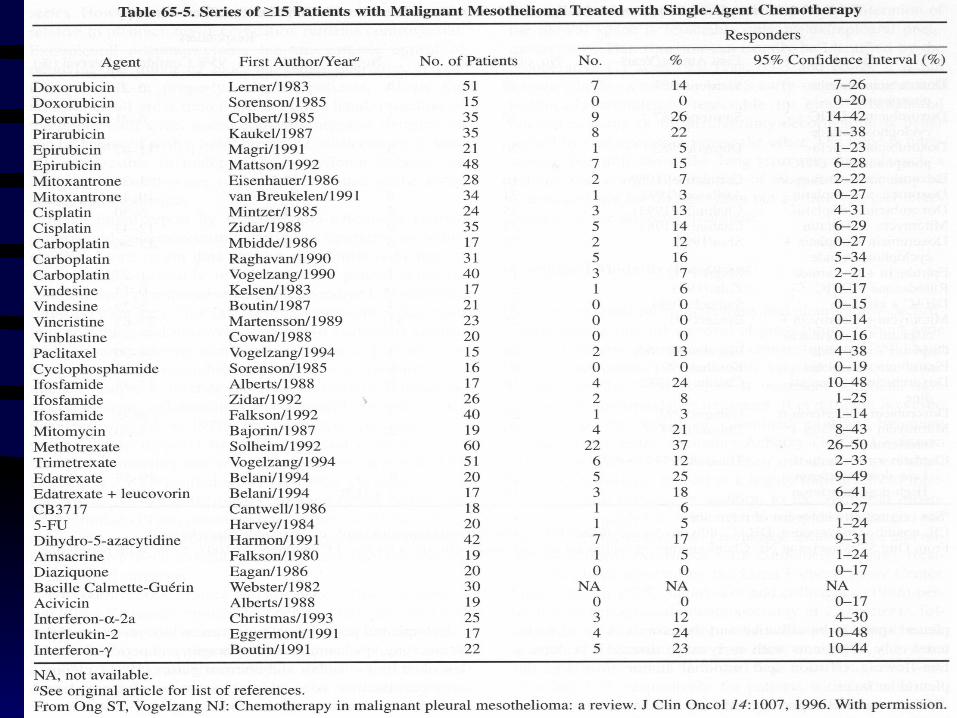
Chemotherapy
• Table 65-5.
• Combination treatment. Table 65-6.
• Response rate 30-40%


Immunotherapy
• Interferon– As antiproliferative effect on mesothelioma cell line.
• Human interferon-α-2a combined with mitomycin C.
• Interferon-γ – As an intrapleural treatment in early-stage diaseas ( 40x106U infused into pleural space twice weekly for 2 months ) , 56% response.
• Intrapleural interleukin 2.

Intrapleural gene therapy
• Herpessimplex virus thymidine kinase ( HSVtk ) gene– Transfer to tumor via adenovirus.
• Administration of antiviral drug– Ganciclovir– Led the tumor death.
Surgery
• Still the mainstay of treatment.
• Three operation–
(1). Extrapleural pneumonectomy.
( pleuropneumonectomy ) (2). Pleurectomy-decortication.
(3). Palliative limited pleurectomy.

Extrapleural pneumonectomy
• En bloc resection of pleura, lung, ipsilateral hemidiaphragm, pericardium,
• Value– Controversial.
• Operative mortality 6- 30%.
• Preoperative CT, lung function, ventilation-perfusion scan, cardiac function evaluate.

Pleurectomy-decortication
• Remove all gross pleural disease, without removing underlying lung.
• Also remove hemidiaphragm and pericardium.
Palliative limited pleurectomy
• Resection parietal pleura to control pleural effusion.
• Thoracoscopy and talc poudrage — High effective in controlling effusion.






![Diffuse malignant peritoneal mesothelioma · 2016. 12. 12. · Diffuse malignant peritoneal mesotheliomadan update on treatment. Cancer Treat Rev 2012;38:605e12. [8] Yu GH, Soma L,](https://static.documents.pub/doc/80x56/60f842b284d46037843a85de/diffuse-malignant-peritoneal-mesothelioma-2016-12-12-diffuse-malignant-peritoneal.jpg)










