35
Diltiazem overdose in a 14-year-old Labrador Lisa Fiorenza Clinical Advisor: Dr. Bruce Kornreich Pre-clinical Advisor: Dr. Wayne Schwark Special thanks: Dr. Josh Smith, Dr. Freddie Brewer
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | lydia-erica-collins |
| View: | 215 times |
| Download: | 0 times |

Diltiazem overdose in a 14-year-old Labrador
Lisa Fiorenza
Clinical Advisor: Dr. Bruce Kornreich
Pre-clinical Advisor: Dr. Wayne Schwark
Special thanks: Dr. Josh Smith,
Dr. Freddie Brewer

Signalment/Chief Complaint
• 14 year old • Spayed female• Yellow Labrador• Collapse episodes• Arrhythmia at rDVM

History
• 3 episodes of collapse over 2.5 wks– Vocalizes prior– Relatively normal before and after episodes
• Lethargic since

History
• At rDVM– Arrhythmia ausculted– Chem: BUN= 37 [10-32], ALT= 253 [20-98], Alk Phos=
454 [17-111]
– Baseline T4= 0.9 ug/dL [1.5-3]
– Chest rads: suspect cardiomegaly– ECG: ventricular tachycardia – Sotalol 1.5 mg/kg PO q12 hrs initiated

Initial Exam
• QAR, transported into ER on gurney
• Irregularly irregular rhythm– HR varied from 60 bpm to 240 bpm
• Poor pulses w/ deficits
• Abdominal fluid wave

Diagnostics
• Gaslyte, QATS, blood smear– Mild respiratory alkalosis
• 4DX– Anaplasma positive
• Mild peritoneal fluid on FAST scan– Modified transudate
• MAP 110 mmHg on Cardell• Troponin
– 0.77 ng/dL [0-0.1]

Dr. Brewer’s last emergency call!
• ECG– HR 115-250 bpm– Sinus rhythm w/ frequent paroxysms of SVT– Short P-R interval, wide QRS complexes, +/- delta
waves– Right axis shift
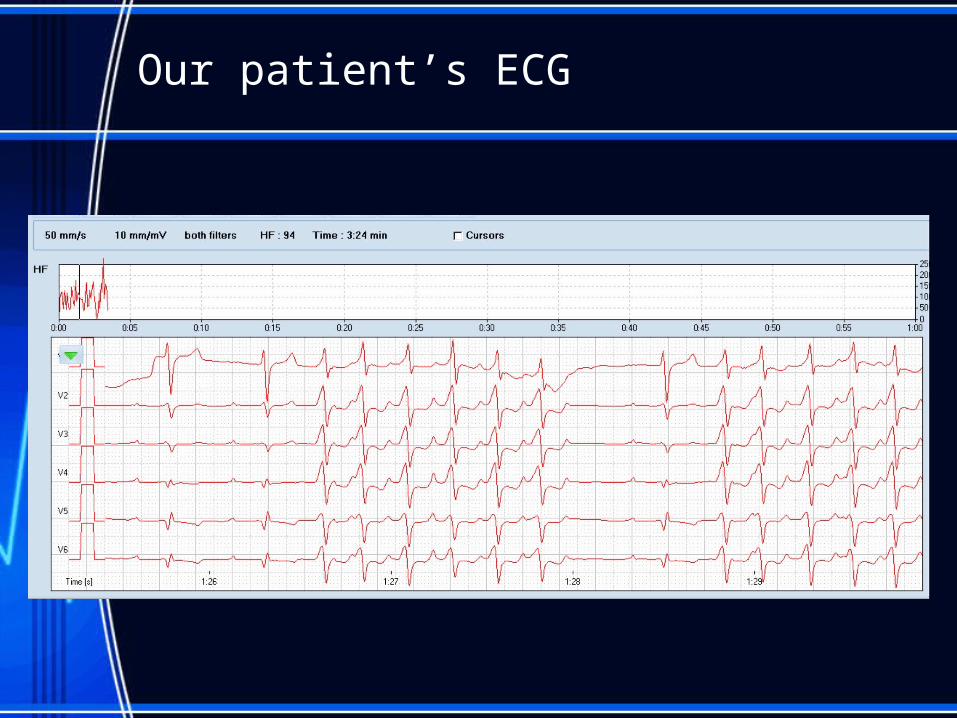
Our patient’s ECG

Dr. Brewer’s last emergency call!
• Echo– Dilated LV, normal LA– Mild systolic dysfunction
• Near-normal when in sinus rhythm
– Dilated pulmonary veins– Mild MVD with mild regurgitation– Normal right heart, pericardium, outflow velocities

Decreased systolic function
QuickTime™ and aMicrosoft Video 1 decompressorare needed to see this picture.

Problems
1. Collapse x32. Tachyarrhythmia
– Supraventricular vs ventricular
3. Poor pulses w/ deficits4. Mild myocarditis
– Tachycardiomyopathy suspected
5. Mildly decreased systolic function
• Lethargy• Hypothyroid• Mild liver enzyme elevations• Anaplasma positive

Diagnosis
• Wide complex tachycardia with suspected secondary tachycardiomyopathy
• Rule outs: – Wolff-Parkinson White syndrome (SVT)– Ventricular tachycardia (VT)
Treatment
• Sotalol 1.5 mg/kg– Class III: Potassium channel blocker
• Prolongs repolarization time
– Also a non-selective Beta-blocker• Decreases HR
• Diltiazem ~2 mg/kg– Class IV: Calcium channel blocker (CCB)
• Decreases SA node discharge• Decreases AV node conduction• For suspected Wolff-Parkinson White syndrome

Diltiazem
• Four 60 mg pellets per capsule

Diltiazem overdose
• Received 4x dose (~9 mg/kg) of Diltiazem extended release capsule

Diltiazem overdose
• Four hours later, patient obtunded in ICU kennel
• HR= 30 bpm• Techs unable to get blood pressure• Cardiology & E/CC called
– Flash echo• Bradycardia, decreased contractility
– ECG…

Diltiazem Overdose
HR ~ 45 bpm
Gave atropine dose

Uh oh…
HR ~ 15 bpm

And then…

Compressions & RoSC
HR ~ 110 bpm
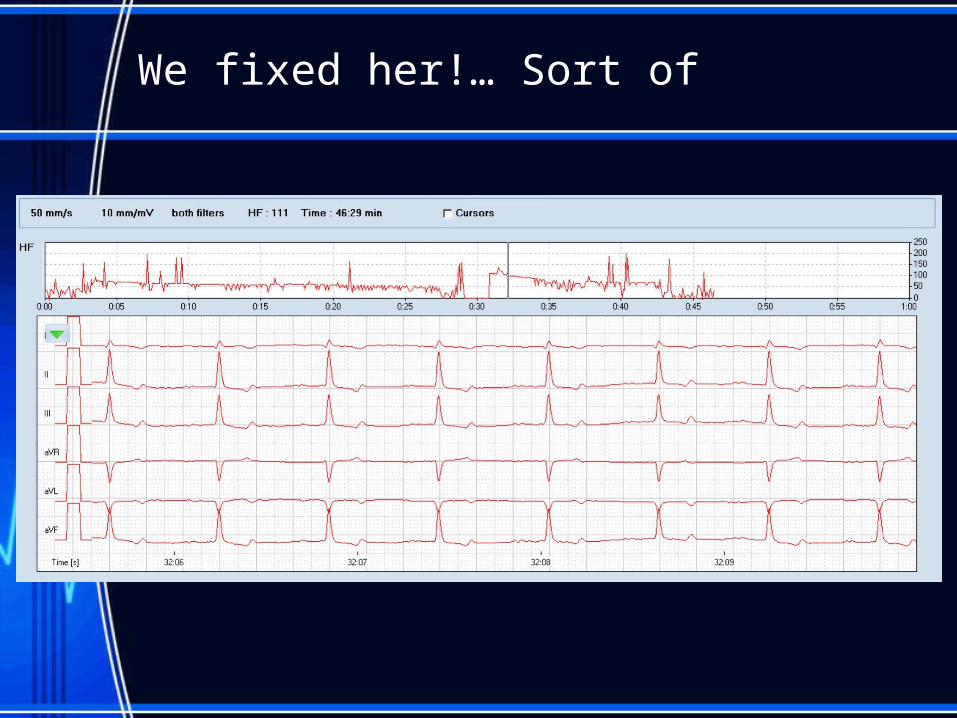
We fixed her!… Sort of

Calcium channel action
• SA and AV node!
• Ca channel opens
• Ca influx stimulates SR release of lots more Ca
• Muscle contraction occurs
Courtesy of ABPI

Calcium Channel Blocker Uses
• Benzothiazepines (diltiazem)– Supraventricular tachycardias– Acute renal failure
• Dihydropyridines (amlodipine)– Hypertension
• Vascular-selective

Diltiazem MOA
• Blocks influx of Ca through L-type (long-lasting) Ca channels of pacemaker cells especially– Slows SA node activity
– Decreases AV node conduction– Minimal vasodilation (intermediate selectivity)
• Ultimately, decreases HR and prolongs refractory period– Good if you’re tachycardic, bad in excess…

CCB overdose signs
Bradycardia & decreased contractility
Decr Cardiac output
Hypotension
Shock
Death
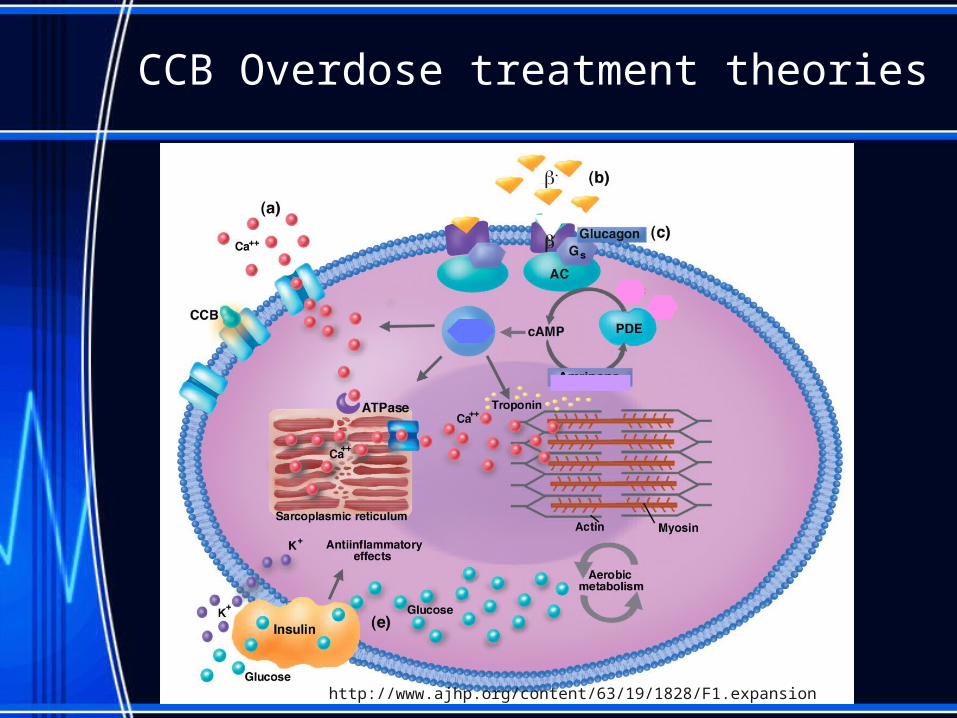
CCB Overdose treatment theories
http://www.ajhp.org/content/63/19/1828/F1.expansion
CCB Overdose treatments
• Decontamination (asymptomatic)– Emesis– Charcoal + cathartic
• 2-4 times in 24 hrs for extended-release capsules
• Supportive– IVF, colloids
CCB Overdose treatments
• What works– Pressor (sympathomimetics) CRIs
• Epi, dobutamine, dopamine, norepi, isoproterenol
– High-dose insulin CRI (+ dextrose)– Lipid emulsion
• What doesn't– Atropine – Glucagon– Ca gluconate?

DoBUTamine MOA
• Sympathomimetic– Direct stimulation of 1 receptors
• Positive inotrope ( cardiac contractility)• Positive chronotrope ( HR)
• Titrate up to effect, then wean off while monitoring

Back to our patient
• Epinephrine during code brought her back
• Marked bradycardia & hypotension– Dobutamine CRI: started at 5 mcg/kg/min, titrated
up to effect (15 mcg/kg/min)– Successfully weaned off after ~ 20 hrs– Monitored HR, BP, continuous ECG, electrolytes

3 days later…
QuickTime™ and aH.264 decompressor
are needed to see this picture.
There’s our girl!

Cost
• ER Visit: $350• ER Cardio exam & echo: $490• Diagnostics/treatment*: $700• Holter monitor: $250 • Costs assoc w/ overdose: $1600
• TOTAL: $3,390 - $1,600= $1,790
*1st night in ICU + anything not affected by overdose

Moral of the story?
• ALWAYS read the Rx labels AND tx sheet
• Nobody’s perfect!– Honesty saved her life

References
• Malouin, A. and King, L. (2009). Ca Channel and Beta Blocker Drug Overdose. In D. Silverstein and K. Hopper, Small Animal Critical Care Medicine (357-62). St. Louis, MO: Saunders.
• Hayes, C. and Knight, M. (2012). Calcium Channel Blocker Toxicity in Dogs and Cats. Vet Clin Small Anim, 42(2), 263-277.
• Cooke, K.L. and Snyder, P.S. (1998). Calcium Channel Blockers in Veterinary Medicine. J Vet Intern Med 12, 123-131.
• American College of Emergency Physicians. (1995). Clinical policy for the initial approach to patients presenting with acute toxic ingestion or dermal or inhalation exposure. Ann Emerg Med. 25, 570-85.
• Kornreich, B. (2012, November). Mechanisms of Arrhythmia. Block 5. Lecture conducted from Ithaca, NY.
Questions?
Thank you!!Bruce Kornreich
Wayne Schwark
Josh Smith
Freddie Brewer
Thank you!!
Family
Friends
c/o 2014

















