Page 1
4/9/2017
1
Idaho Academy of Nutrition & Dietetics Annual Meeting – Boise, Idaho
Nutrition Focused Physical Assessment(NFPE)
Ainsley Malone, MS, RD, CNSC, FAND,FASPEN
Disclosure• I have nothing to disclose
Objectives
• Outline the importance of a nutrition focused physical examination in the overall nutrition assessment process.
• Explain nutrition-focused physical assessment techniques for identifying and grading malnutrition of subcutaneous fat loss and muscle loss
• Describe edematous conditions and demonstrate how to assess for the presence of edema
What is NFPE?Exam which uses physical assessment and physical function findings to help determine nutritional status and diagnose
malnutrition
A comprehensive nutrition assessment must include a NFPE.
MacronutrientMacronutrientFat (orbital, triceps, ribcage)
Muscle (temples, shoulders, clavicles, scapula, thigh, calves)Fluid (extremities)
MicronutrientSkin, Nails, Hair, Head/neck, Oral cavity, Eyes, Nose/Face
Page 2
4/9/2017
2
Why Should Dietitians Use NFPE?• Reveals and confirms problem areas that indicate malnutrition
and micronutrient deficiencies
• A unique contribution to patient assessment
• An important component of Subjective Global Assessment (SGA) – Looks similar to newest adult malnutrition criteria – SGA has been validated in multiple patient populations as a tool to
assess malnutrition– ASPEN-Academy criteria was created to be a more objective
framework for assessing malnutrition
Baker JP, et al. Nutritional assessment: a comparison of clinical judgment and objective measurements. NEJM, 1982.Detsky AS, McLaughlin JR, et al. What is subjective global assessment? JPEN, 1987.
How…?Prepare Yourself
• Review the medical record, social history, labs, medications
• Discuss with medical team to assess appropriateness of performing the examination
• Gather necessary equipment– Wash hands– Wear gloves/personal protective equipment when appropriate
• Prioritize the areas you wish to examine
• Obtain patient’s nutrition history
Prepare the Patient• Introduce yourself and explain the process
• Respect patient privacy and ask permission– Draw curtains, close doors – Expose areas of body only as needed
• Before the examination, ask the patient or family p ymember nutrition related questions
• Explain the process as you perform the exam
Inspection– Most frequently used– Broad observation followed by closer
lookCritical evaluation
How…?Techniques of the physical exam
– Critical evaluation
PalpationPalpation– Examining body structures,
pulsations by touch
Page 3
4/9/2017
3
Auscultation– Listening to body sounds– Heart, lungs, intestines– Broad observation followed by closer
look
How…?Techniques of the physical exam
Percussion– Produces sounds to locate organ
borders– Identifies if organ is solid or filled
with fluid or gas
Muscular System OverviewPerforming a physical exam is best done using a “head to toe” approach
Exam Area: Temples -Temporalis MuscleView patient when standing directly in front of them, ask patient to
turn head side to sideSevere Mild - Moderate Normal
Hollowing, scooping, depression
Slight depressionCan see/feel well-
defined muscle
Exam Area: Orbital Area - Fat Pad Around EyeView patient when standing directly in front of them,
touch above cheekboneSevere Mild - Moderate Normal
Hollow look, depressions, dark circles, loose skin
Slightly dark circles, somewhat hollow
look
Slightly bulged fat pads. Fluid retention
may mask loss
Page 4
4/9/2017
4
Exam Area: Clavicle & Acromion Bone - Deltoid MusclePatient arms at side; observe shape
Severe Mild - Moderate NormalShoulder to arm joint looks square. Bones
prominent. Acromion protrusion very
prominent
Acromion process may slightly protrude
Rounded, curves at arm/shoulder/neck
Exam Area: Scapular Bone Region Trapezius, Supraspinatus, Infraspinatus Muscles
Ask patient to extend hands straight out, push against solid object. Severe Mild - Moderate Normal
Prominent, visible bones, depressions
between ribs/scapula or shoulder/spine
Mild depression or bone may show
slightly
Bones not prominent, no significant depressions
Exam Area: Thoracic & Lumbar Region –Ribs, Lower Back, Midaxillary Line
Have patient press hands hard against a solid objectSevere Mild -Moderate Normal
Depression between the ribs very apparent;
iliac crest very prominent
Ribs apparent, but depressions less
pronounced; iliac crest somewhat prominent
Chest is full, ribs do not show. Slight to no protrusion of the iliac
crest.
Upper Arm Assessment Technique
Mild -Moderate
Normal
Severe
Page 5
4/9/2017
5
Exam Area: Upper Arm Region -Triceps/BicepsArm bent, roll skin between fingers, do not include muscle in pinch
Severe Mild - Moderate NormalVery little space
between folds, fingers touch
Some depth pinch, but not ample
Ample fat tissue obvious between folds
of skin
BeforeAfter
Keys A. JAMA. 1948;138:500-511
Exam Area: Dorsal Hand - Interosseous MuscleLook at thumb side of hand; look at pads of thumb when tip of
forefinger touching tip of thumbSevere Mild - Moderate Normal
Depressed area between thumb-
forefingerSlightly depressed
Muscle bulges, could be flat in some well nourished people
Exam Area: Anterior Thighs – Quadriceps& Patellar Region
Ask patient to sit, leg propped up, knee bent Grasp quads to differentiate muscle vs. fat tissue
Severe Mild -Moderate NormalDepression/line on thigh,
obviously thinBones prominent, little sign of muscle around
knee
Mild depression on inner thigh
Knee cap less prominent, more rounded
Well rounded, well developed
Muscles protrude, bones not prominent
kneep
Exam Area: Posterior Calf Region -Gastrocnemius Muscle
Grasp the calf muscle to determine amount of tissueSevere Mild -Moderate Normal
Thin, minimal to no muscle definition
Not well developed Well-developed bulb
of muscle
Page 6
4/9/2017
6
Things to Consider: Etiology of Muscle Wasting Causes of Muscle Atrophy
• Amyotrophic lateral sclerosis (ALS or Lou Gehrig's disease)
• Polio• Guillain-Barre syndrome
M t th ( h
• Muscular dystrophy • Osteoarthritis • Dermatomyositis and
polymyositis• Rheumatoid arthritis
• Motor neuropathy (such as diabetic neuropathy)
• Injury • Burns • Long-term corticosteroid
therapy
• Spinal cord injury • Stroke• Lengthy ICU stay
Malnutritionhttp://www.nlm.nih.gov/medlineplus/ency/article/003188.htmGarmin, Anderson, et al 1997 Metab
Summary: Fat Loss
3 areas – Orbital Region– Upper Arm Area
• Triceps
• Biceps• Biceps– Thoracic & Lumbar Regions
• Rib cage
• Lower back
• Mid-axillary line
Summary: Muscle Loss
Upper Body• Temporalis
• Clavical Bone Region– Pectoralis Major, Deltoid,
Trapezius
Lower Body• Patellar Area
• Anterior Thigh (Quadriceps)
• Posterior Calf • Acromion Bone Region
– Deltoids
• Scapula Bone Area– Trapezius, Supraspinatus,
Infraspinatus
• Hands (Interosseous Muscles)
(Gastrocnemius)
Page 7
4/9/2017
7
What is fluid retention?
• Edema is the abnormal retention of fluid in interstitial
spaces and cavities (e.g., peritoneal/abdominal cavity)
• Systemic fluid retention may not clinically manifest until it
accounts for at least 10% of body weight or when accounts for at least 10% of body weight or when
interstitial fluid volume is increased by 2.5-3 liters.
• Fluid accumulation around the heart, fluid in the lungs,
small pockets of ascites, or hematomas can be seen on
imaging studies.
Causes of Fluid Retention• Conditions
associated with fluid accumulation– Heart failure– Renal & liver
di
Increased capillary hydrostatic pressure
Hypervolemia; kidney disease, pregnancy, CHF
Loss of plasma proteins Kidney disease, liver disease,
burn victims, malabsorption, , malnutrition disease
– Lymphatic obstruction
– Critical illness
malnutrition Obstruction of lymphatic
circulation Obstructing tumor, infection,
damages to the lymph nodes or lymph node removal (cancers)
Increased capillary permeability
Usually from inflammatoryresponse or response to infections
Fluid Accumulation – Academy/ASPEN Clinical Characteristics Of Malnutrition
– Is an essential part of our physical exam– Is SUPPORTIVE evidence, RARELY ever directly
related to malnutrition– Weight loss is frequently masked by fluid retention
and weight gain may be presentg g y p– Interferes with ability assess muscle wasting and fat
loss
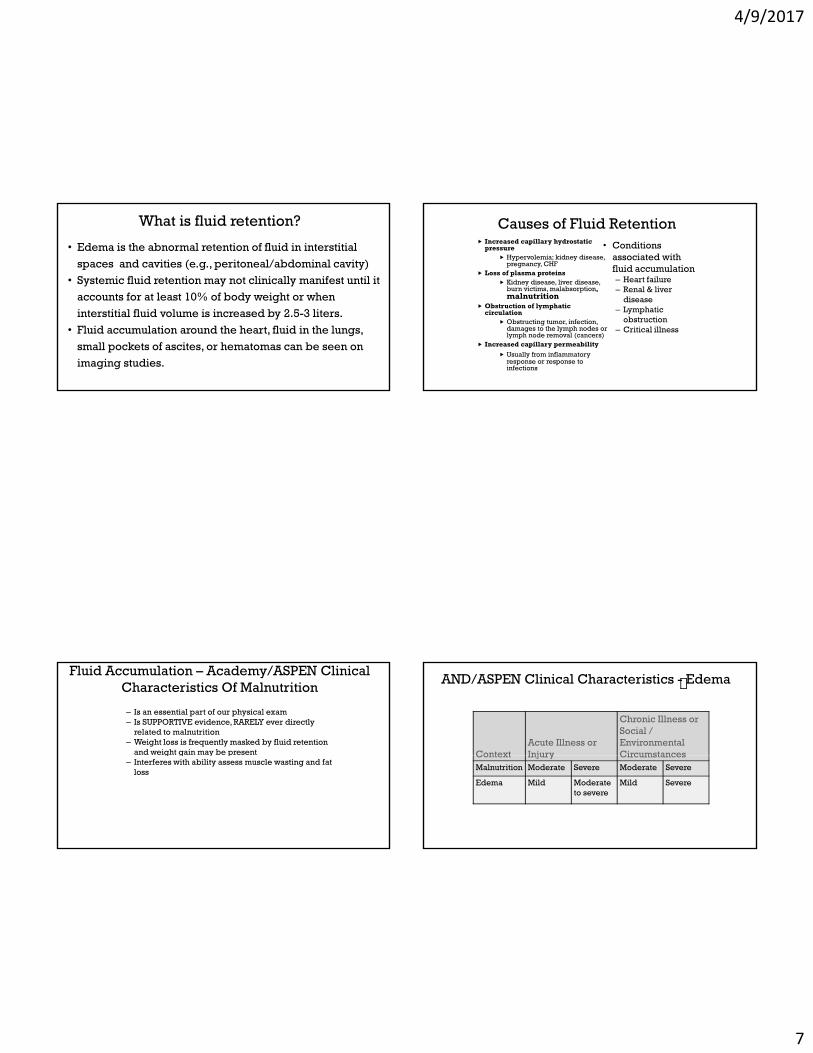
AND/ASPEN Clinical Characteristics - Edema
ContextAcute Illness or Injury
Chronic Illness or Social / Environmental CircumstancesContext Injury Circumstances
Malnutrition Moderate Severe Moderate Severe
Edema Mild Moderate to severe
Mild Severe
Page 8
4/9/2017
8
Feasibility of accessing data in hospitalized patients… Nicolo et al. JPEN 2013
• Cross-sectional survey at 4 different hospitals: 2 tertiary teaching,1 urban, 1 rural; included 262 adults
• Determined availability of data to support the proposed AND/ASPEN malnutrition characteristics/ S o c c e c
• Data on edema available at time of nutrition assessment– All patients – 84.4%, Non-ICU – 85.9%, ICU – 82.7%
• Edema used as one of the characteristics to define malnutrition– All patients – 26.6%, Non-ICU – 16.2%, ICU – 39.1%
Assessment Strategy
• Perform general survey, then head-to-toe
• Use inspection and palpation
• Determine if onset is acute vs chronic– Acute: < 72 hours– Chronic: better? worse? same?Chronic: better? worse? same?
• Correlate physical findings of fluid accumulation with other evidence – vital signs, input/output records, labs, weight, etc.
Assessing Fluid Retention• Primarily found in dependent areas such as the sacrum,
ankles, feet, scrotum, vulva• The clinician may evaluate generalized or localized fluid
accumulation during a physical exam• Localized:oc e
–extremities, abdomen (ascites), and/or vulva/scrotal area
• Generalized:– if severe, is referred to as anasarca
• Vital signs, intake and output, weight, history, imaging studies
Dependent Edema – Ambulatory Patients Legs, Ankles, Feet
Page 9
4/9/2017
9
Dependent Edema – Bed Bound Patients Scrotum, Vulva, Sacrum
Additional fluid
Other AreasEdema And
Ascites
Assessing Edema
• Press firmly but gently with your thumb for at least 5 seconds over
– The dorsum of the foot
– Behind each malleolus
– Over the shins
S it f d i t d l f 1 t 4• Severity of edema is rated on a scale from +1 to +4
Grade DepthDescription
0none
No impression or distortion observed, bone structure
easily identified
1+ 2 mm or less
Slight pitting without distortion, rapidly
disappears
Somewhat deeper pit,
2+2 – 4 mm
distortion not easily apparent, disappears 10-25
seconds later
3+4 – 6 mm
Noticeably deep pitting, entire extremity looks full,
swollen; indentation can last longer than 1 minute
4+ 6 – 8 mmVery deep pitting, extremity
is grossly misshapen, indentation lasts 2-5 minutes
Page 10
4/9/2017
10
Translating Edema To Degree Of MalnutritionExamine for edema
Tips Severe malnutrition
Moderate malnutrition
Well-nourished
Consider patient’s history, causes for fluidaccumulation
Patients who are bedridden are more likely to have
Deep to very deep pitting (+3 to +4 edema)
Mild to moderate pitting (+1 to +2 edema)
No signs of fluid accumulation
accumulation likely to have edema in the genital area and sacrum
Mobile patients will more likely have peripheral edema
To Summarize
• Performing a nutrition focused physical exam is a unique contribution from the RD
• Is a component of a complete nutrition assessment
• NFPE is important to identify key malnutrition characteristics
• Is performed using a “head to toe” approach• Is performed using a “head to toe” approach
• Doesn’t require much time to perform
• Assessment of muscle and fat mass utlize techniques of observation and palpation
• Exam confidence and competence easily obtained
Many Thanks!