Page 1
1
Caring for the Patient with Acute Pancreatitis Bruce D. Askey, MS, ANP-BC
Associate Lecturer
Fitzgerald Health Education Associates, Inc.
North Andover, MA
Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology
Guthrie Clinic Sayre, PA/Ithaca, NY
Disclosure
• No real or potential conflict of interest to disclose
• No off-label, experimental or investigational use of drugs or devices will be presented.
© Fitzgerald Health Education Associates, Inc.
2
Objectives
• Upon completion of the learning activity the participant will be able to:
– Describe the pathophysiology of acute pancreatitis.
– Discuss the potential complications of acute pancreatitis.
– Discuss the management of acute pancreatitis.
© Fitzgerald Health Education Associates, Inc.
3
Page 2
2
American College of Gastroenterology
• The information for this presentation was taken from the guidelines set forth by the American College of Gastroenterology.1
– www.amjgastro.com – Source: 1. Tenner, et al. American college of gastroenterology guideline:
Management of acute pancreatitis. The American Journal of Gastroenterology advance online publication, 30 July 2013; doi: 10.1038/ajg.2013.218
© Fitzgerald Health Education Associates, Inc.
4
Acute Pancreatitis by the Numbers
• >200,000 annual hospitalizations
– >$2.5 billion annual cost
– 75−85% will have a mild clinical course which resolves in 5−7 days
• Mild attack
– Only 1% mortality
• Severe attack
– Results in mortality rate approaching 20%
© Fitzgerald Health Education Associates, Inc.
5
Definition
• Autodigestion of pancreatic and peripancreatic tissues by naturally occurring pancreatic digestive enzymes
– Trypsin: Digests proteins
– Amylase: Digests carbohydrates
– Lipase: Digests fats
© Fitzgerald Health Education Associates, Inc.
6
Page 3
3
Pathophysiology
• Enzymes
– Generally stored in an inactive form within the pancreas
– Activated in the small intestine
• Pancreatitis occurs when the enzymes are activated within the pancreas itself.
© Fitzgerald Health Education Associates, Inc.
7
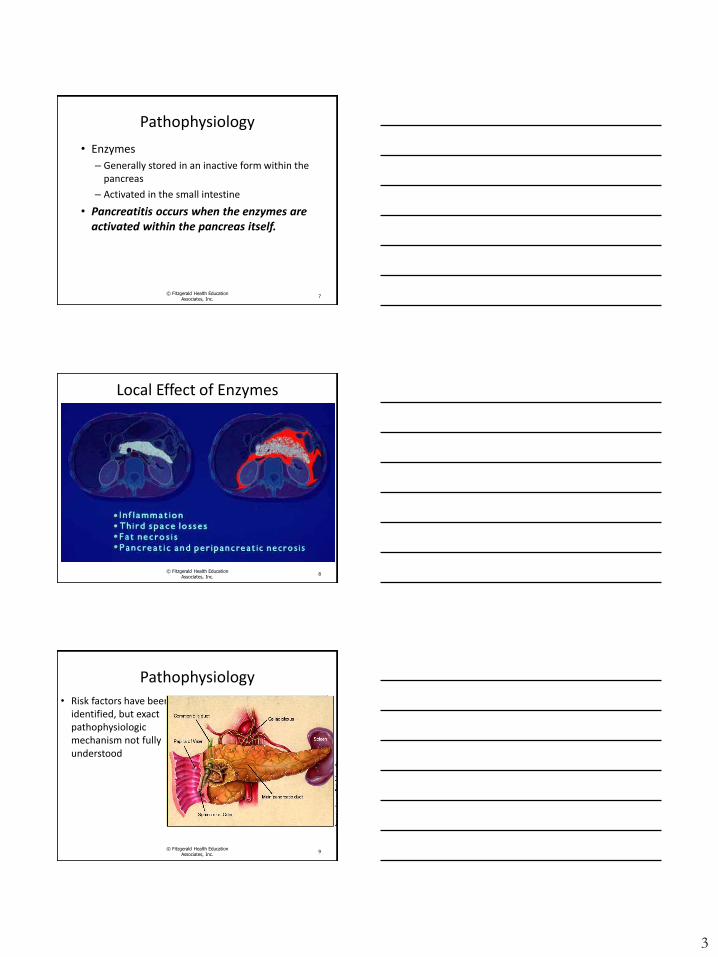
Local Effect of Enzymes
© Fitzgerald Health Education Associates, Inc.
8
Pathophysiology
• Risk factors have been identified, but exact pathophysiologic mechanism not fully understood
© Fitzgerald Health Education Associates, Inc.
9
Page 4
4
Symptoms
• Epigastric pain
– Bandlike pattern that often bores straight through to the back
– “Chemical burn”
• Nausea, vomiting, anorexia
• Fever, diaphoresis, dehydration
© Fitzgerald Health Education Associates, Inc.
10
Physical Exam
• Looks mildly uncomfortable to toxic
• Epigastric pain with palpation
• Abdominal distension, possibly hypoactive bowel sounds
• Dehydration, orthostatic
– Tachycardia
– Hypotension
© Fitzgerald Health Education
Associates, Inc. 11
Physical Exam (continued)
• Grey-Turner’s sign: Flank ecchymosis=High mortality
© Fitzgerald Health Education Associates, Inc.
12
Page 5
5
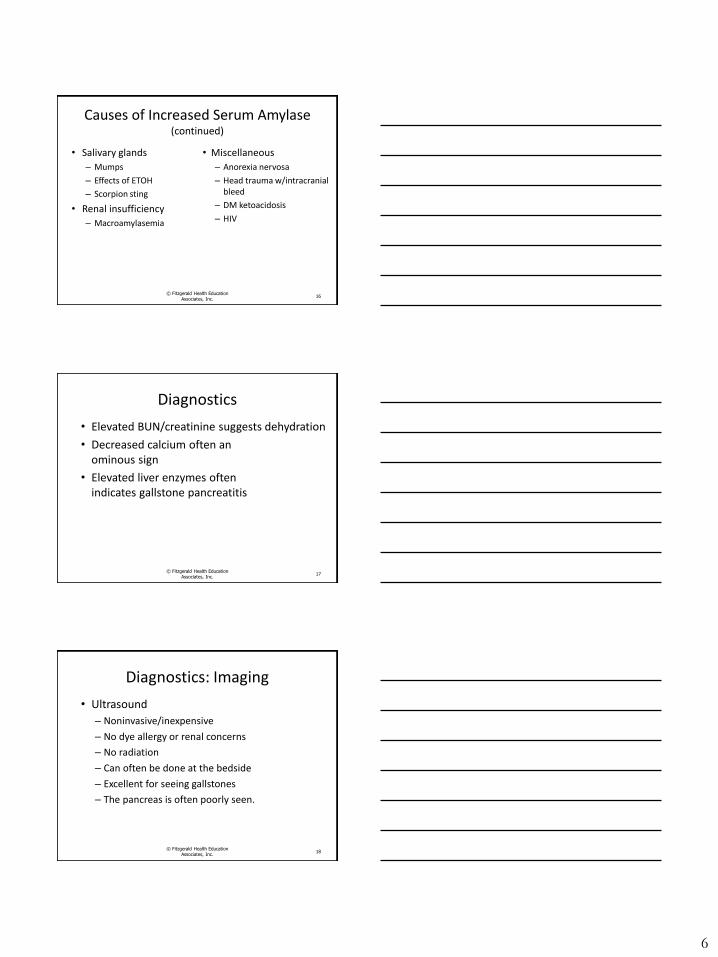
Physical Exam
• Cullen’s sign: Periumbilical ecchymosis=High mortality
© Fitzgerald Health Education Associates, Inc.
13
Diagnostics
• Increased pancreatic enzymes
– Degree of elevation parallels degree of inflammation
– Lipase: More specific than amylase
– Amylase
• WBC often elevated
© Fitzgerald Health Education Associates, Inc.
14
Causes of Increased Serum Amylase
• Pancreatic – Pancreatitis, CA
• Intra-abdominal – Acute cholecystitis
– CBD obstruction
– Perforated hollow viscus
– Ischemia, infarction
– Acute appendicitis
– Salpingitis
– Ruptured ectopic pregnancy
• Tumors – Ovarian cysts
– Papillary cystadenoma of ovary
– Lung carcinoma
• Miscellaneous – Morphine
– Endoscopy
– Sphincter of Oddi spasm
© Fitzgerald Health Education Associates, Inc.
15
Page 6
6
Causes of Increased Serum Amylase (continued)
• Salivary glands
– Mumps
– Effects of ETOH
– Scorpion sting
• Renal insufficiency
– Macroamylasemia
• Miscellaneous
– Anorexia nervosa
– Head trauma w/intracranial bleed
– DM ketoacidosis
– HIV
© Fitzgerald Health Education Associates, Inc.
16
Diagnostics
• Elevated BUN/creatinine suggests dehydration
• Decreased calcium often an ominous sign
• Elevated liver enzymes often indicates gallstone pancreatitis
© Fitzgerald Health Education Associates, Inc.
17
Diagnostics: Imaging
• Ultrasound
– Noninvasive/inexpensive
– No dye allergy or renal concerns
– No radiation
– Can often be done at the bedside
– Excellent for seeing gallstones
– The pancreas is often poorly seen.
© Fitzgerald Health Education
Associates, Inc. 18
Page 7
7
Diagnostics: Imaging (continued)
• CT scan
– Excellent modality to view the pancreas
– Can see pancreatic tumors that may not be seen with ultrasound
– Can use specific pancreatic protocol
– Dye allergy and renal failure limits its use
© Fitzgerald Health Education
Associates, Inc. 19
Diagnostics: Imaging (continued)
• MRI
– Excellent modality to view the pancreas
– Can see pancreatic tumors that may not be seen with ultrasound
– Can use specific pancreatic protocol
– The presence of a pacemaker limits its use
© Fitzgerald Health Education
Associates, Inc. 20
Differential Diagnosis
• Choledocholithiasis
• Perforated ulcer
• Mesenteric ischemia
• Intestinal obstruction
• Salpingitis
• Ectopic pregnancy
© Fitzgerald Health Education Associates, Inc.
21
Page 8
8
Predisposing Conditions
• Gallstones
• Alcohol
• Hyperlipidemia
• Hereditary
• Hyperparathyroidism/ hypercalcemia
• ERCP
• Postoperative
• Pancreatic trauma
• Cystic fibrosis
• Pregnancy
• Vascular diseases
• Infectious agents
© Fitzgerald Health Education Associates, Inc.
22
Predisposing Conditions (continued)
• Structural abnormalities
–Ampullary
–Biliary
– Sphincter of Oddi
–Main PD
–Accessory PD
• Medications
© Fitzgerald Health Education Associates, Inc.
23
Gallstones
• Responsible for 35−70% of all cases
• Treatment with cholecystectomy, sphincterotomy
• Shown to decrease recurrence of pancreatitis
© Fitzgerald Health Education Associates, Inc.
24
Page 9
9
Impacted Gallstones
Endoscopic Retrograde Cholangiopancreaography (ERCP)
• Useful in gallstone pancreatitis when CBD stone impaction is suspected
• With +US, should be performed prior to discharge
© Fitzgerald Health Education Associates, Inc.
26
Alcohol
• Responsible for 30% of pancreatitis
– Pathogenesis remains unclear.
• Toxic metabolite hypothesis
– Direct toxicity to acinar cells
• Reflux of duodenal contents by sphincter of Oddi relaxation
– Eventual necrosis, fibrosis and chronic pancreatitis
© Fitzgerald Health Education Associates, Inc.
27
Page 10
10
Hypertriglyceridemia
• Most with hx of DM or hypertriglyceridemia
• Some cases are induced by drugs (e.g., estrogens).
• Most cases are in excess of 1000 mg/dL (11.3 mmol/L).
• Possible for 500−1000 mg/dL (5.65−11.3 mmol/L) to cause
28 © Fitzgerald Health Education
Associates, Inc.
Medications • Azathioprine
• Sulfonamides – Bactrim®
• Oral 5-ASA
• Antibiotics – Metronidazole
– Tetracycline
– Nitrofurantoin
• Valproic acid
• Corticosteroids
• Furosemide
• Estrogens
• Methyldopa
– Aldomet®
• Pentamidine
• Didanosine
• Octreotide
• DPP-4 inhibitor
• GLP-agonist
• Others
© Fitzgerald Health Education Associates, Inc.
29
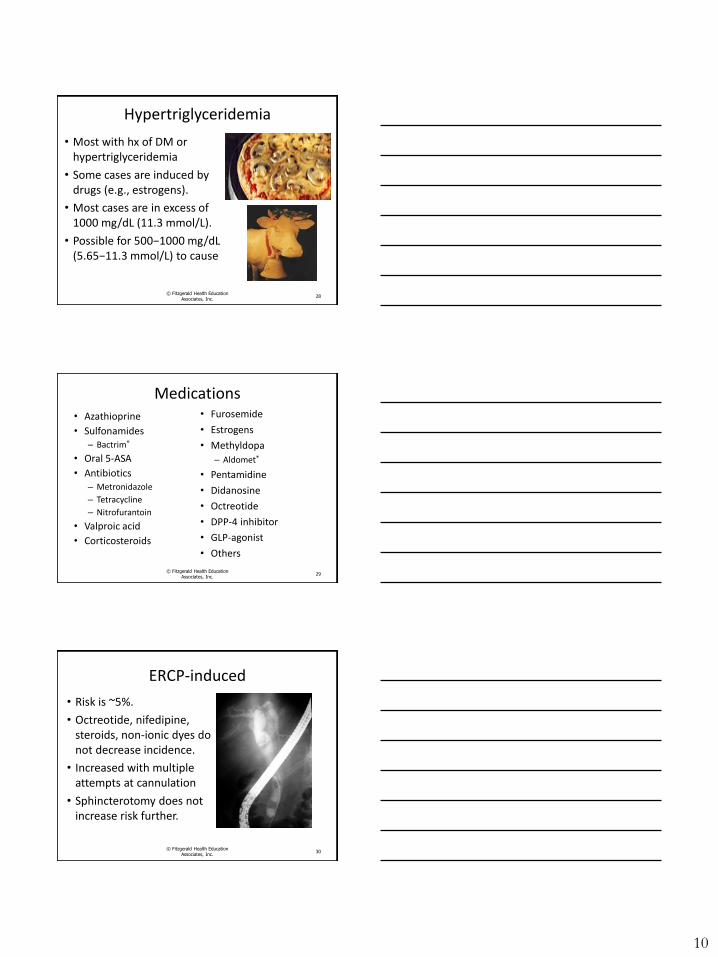
ERCP-induced
• Risk is ~5%.
• Octreotide, nifedipine, steroids, non-ionic dyes do not decrease incidence.
• Increased with multiple attempts at cannulation
• Sphincterotomy does not increase risk further.
© Fitzgerald Health Education Associates, Inc.
30
Page 11
11
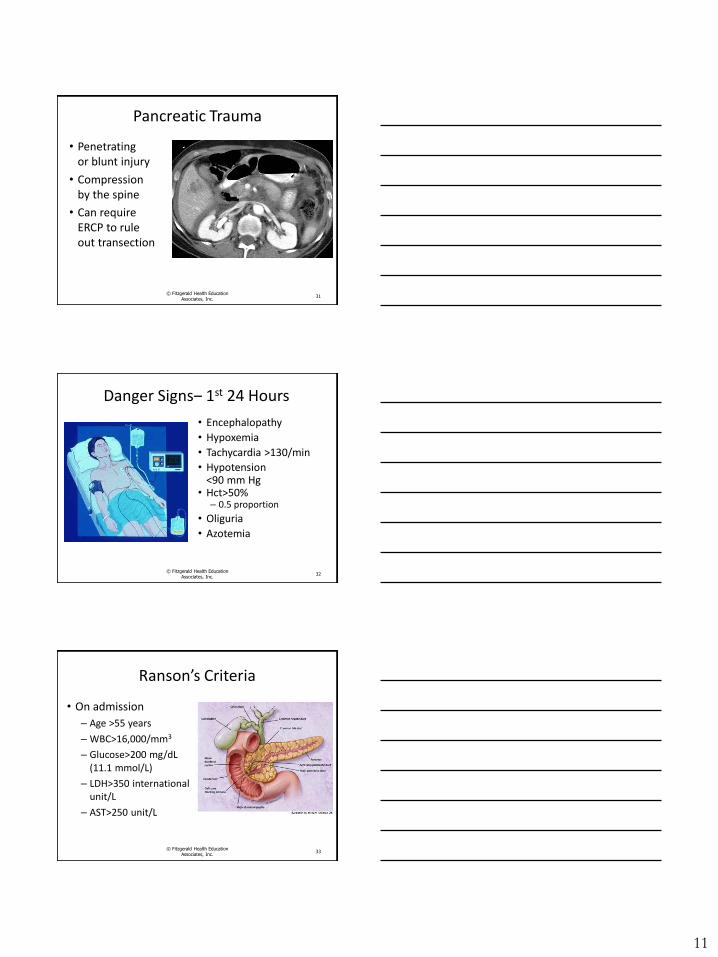
Pancreatic Trauma
• Penetrating or blunt injury
• Compression by the spine
• Can require ERCP to rule out transection
© Fitzgerald Health Education Associates, Inc.
31
Danger Signs‒ 1st 24 Hours
• Encephalopathy
• Hypoxemia
• Tachycardia >130/min
• Hypotension <90 mm Hg
• Hct>50% – 0.5 proportion
• Oliguria
• Azotemia
32 © Fitzgerald Health Education
Associates, Inc.
Ranson’s Criteria
• On admission
– Age >55 years
– WBC>16,000/mm3
– Glucose>200 mg/dL (11.1 mmol/L)
– LDH>350 international unit/L
– AST>250 unit/L
© Fitzgerald Health Education Associates, Inc.
33
Page 12
12
Ranson’s Criteria (continued)
• During 1st 48 hours
–Hct decrease>10% (0.1 proportion)
–BUN increase>5 mg/dL (1.8 mmol/L)
–Calcium<8 mg/dL (2 mmol/L)
–PaO2<60 mm Hg
–Base deficit>4 mEq/L
– Fluid sequestration>6L
© Fitzgerald Health Education Associates, Inc.
34
Ranson’s Criteria (continued)
• <3 signs=Excellent prognosis
• 3−5 signs=10−20% mortality
• ≥6 signs ≥50% mortality
• General rule – ≥3 signs=Severe pancreatitis
© Fitzgerald Health Education Associates, Inc.
35
Atlanta Criteria 2013
• Mild acute pancreatitis – Absence of organ failure
– Absence of local complications
• Moderately severe acute pancreatitis – Local complications and/or
– Transient organ failure (<48 hours)
• Severe acute pancreatitis – Persistent organ failure (>48 hours)
© Fitzgerald Health Education Associates, Inc.
36
Page 13
13
Complications
• Hypovolemia
• Adult Respiratory Distress Syndrome (ARDS)
• Disseminated Intravascular Coagulation (DIC)
• Infection/pancreatic necrosis
© Fitzgerald Health Education Associates, Inc.
37
Complications (continued)
• Hypovolemia
– 250−500 mL/hour of crystalloid
• Can require more fluid based on clinical status
– Lactated Ringer’s solution can be more effective than normal saline
– Goal: Decrease the BUN
– Reassess within 6 hours of admission
© Fitzgerald Health Education Associates, Inc.
38
Complications (continued)
• Hypovolemia (cont.)
– Assess breath sounds for rales
– Monitor electrolytes
– Monitor heart rate and blood pressure
– Monitor central venous pressure, cardiac output and pulmonary artery pressures if central line is in place
– Assess for heart failure
© Fitzgerald Health Education
Associates, Inc. 39
Page 14
14
Complications (continued)
• Adult respiratory distress syndrome (ARDS)
– Occurs between days 2−7 of acute pancreatitis
– Monitor respiratory rate and status
– Monitor oxygen saturations
© Fitzgerald Health Education Associates, Inc.
40
Complications (continued)
• Disseminated intravascular coagulation (DIC)
– Trypsin activates prothrombin resulting in coagulation and depletion of clotting factors
– Assess for signs of bleeding
– Monitor complete blood count (CBC)
– Monitor PT/INR/PTT
© Fitzgerald Health Education Associates, Inc.
41
Complications (continued)
• Infection/pancreatic necrosis
– Monitor temperature
– CT
– Aspiration with C/S and appropriate antibiotics
© Fitzgerald Health Education Associates, Inc.
42
Page 15
15
Supportive Care
• Essential – Close clinical surveillance
– NPO
– IV fluid replacement
– Nutritional support
– Relief of pain
© Fitzgerald Health Education Associates, Inc.
43
Supportive Care (continued)
• No proven benefit – Antibiotics (unless infection is identified)
– Reduction of pancreatic secretion • H-2 blocker, NG suction, glucagon, anticholinergic,
somatostatin
© Fitzgerald Health Education Associates, Inc.
44
Case Study
• GK is a 47-year-old male with no past medical history who presents to the emergency room complaining of a 10-h history of severe continuous epigastric pain, which bores through to his back. He reports associated nausea and vomiting.
© Fitzgerald Health Education Associates, Inc.
45
Page 16
16
Case Study (continued)
• He routinely drinks 20 cans of beer daily and has done so for the past 25 years.
– 1 drink=12 oz (0.35 L) of beer, 5 oz (0.15 L) of wine, 1.5 oz (0.04 L) of 80-proof liquor
• He is on no medications and has no allergies but admits that he has never had a physical and goes to the ER when he “needs something from the doctors.”
© Fitzgerald Health Education
Associates, Inc. 46
Case Study (continued)
• His blood pressure is 94/52 mm Hg and his heart rate is regular at 128 beats per minute.
• In light of the fact that this presentation is about acute pancreatitis, you suspect that he has the condition.
• What tests will confirm acute pancreatitis?
• What is the likely etiology in this case?
© Fitzgerald Health Education Associates, Inc.
47
Case Study: Additional Information • White blood cell count=14,500 mm3
– N: 4.5‒11.1,000 mm3
• Blood glucose=350 mg/dL (19.4 mmol/L)
– N: 80‒100 mg/dL (4.4‒5.6 mmol/L)
• LDH=290 international units/L
– N: 140‒280 international units/L
• AST=410 units/L
– N: 8‒48 units/L
© Fitzgerald Health Education Associates,
Inc. 48
Page 17
17
What is his Ranson’s score? Based on his Ranson’s score, what is
his prognosis?
© Fitzgerald Health Education Associates, Inc.
49
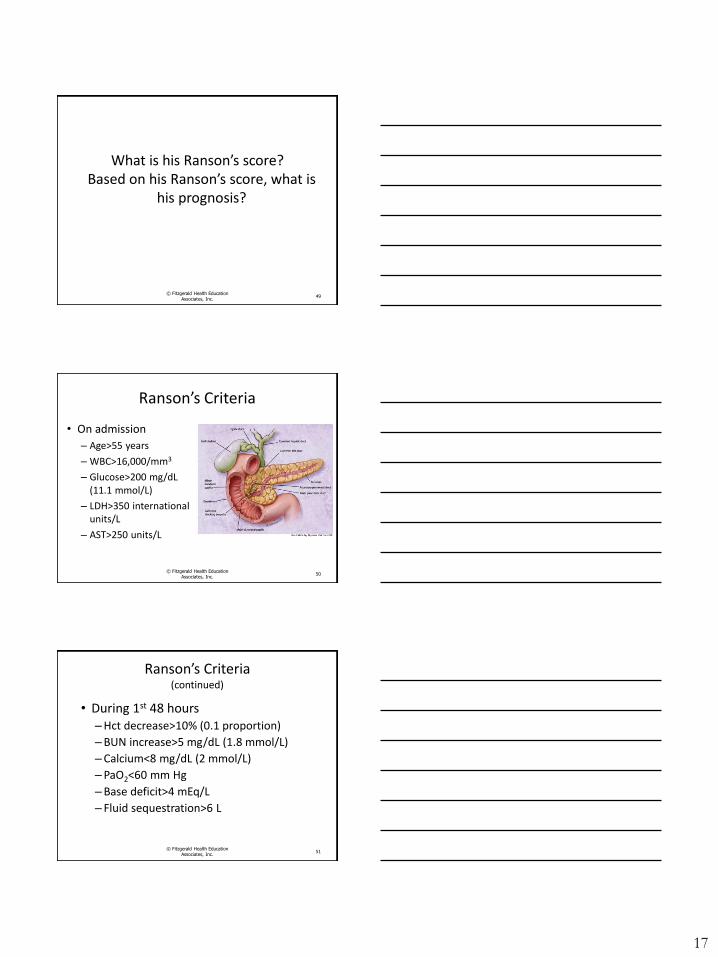
Ranson’s Criteria
• On admission
– Age>55 years
– WBC>16,000/mm3
– Glucose>200 mg/dL (11.1 mmol/L)
– LDH>350 international units/L
– AST>250 units/L
© Fitzgerald Health Education Associates, Inc.
50
Ranson’s Criteria (continued)
• During 1st 48 hours –Hct decrease>10% (0.1 proportion)
–BUN increase>5 mg/dL (1.8 mmol/L)
–Calcium<8 mg/dL (2 mmol/L)
–PaO2<60 mm Hg
–Base deficit>4 mEq/L
– Fluid sequestration>6 L
© Fitzgerald Health Education Associates, Inc.
51
Page 18
18
Ranson’s Criteria (continued)
• <3 signs=Excellent prognosis
• 3−5 signs=10−20% mortality
• ≥6 signs ≥50% mortality
• General rule
– ≥3 signs=Severe pancreatitis
© Fitzgerald Health Education Associates, Inc.
52
Case Study
• How should this patient be managed?
• What lab parameters should be monitored?
• What clinical parameters should be assessed?
• What do you get when you cross an elephant with a rhino?
© Fitzgerald Health Education Associates, Inc.
53
Questions?
© Fitzgerald Health Education Associates, Inc.
54
Page 19
19
© Fitzgerald Health Education Associates, Inc.
55
Thank you for your time and attention.
Bruce D. Askey, MS, ANP-BC
www.fhea.com [email protected]
End of Presentation
• Images/Illustrations: Unless otherwise noted, all images/ illustrations are from open sources, such as the CDC or Wikipedia or property of FHEA or author.
• All websites listed active at the time of publication.
© Fitzgerald Health Education Associates, Inc.
56
Copyright Notice
Copyright by Fitzgerald Health Education Associates, Inc. All rights reserved. No part of this publication may be reproduced or transmitted in
any form or by any means, electronic or mechanical, including photocopy, recording or any information storage and retrieval system, without permission from Fitzgerald
Health Education Associates, Inc.
Requests for permission to make copies of any part of the work should be mailed to:
Fitzgerald Health Education Associates, Inc.
85 Flagship Drive
North Andover, MA 01845-6184
© Fitzgerald Health Education Associates, Inc.
57
Page 20
20
Statement of Liability
• The information in this program has been thoroughly researched and checked for accuracy. However, clinical practice and techniques are a dynamic process and new information becomes available daily. Prudent practice dictates that the clinician consult further sources prior to applying information obtained from this program, whether in printed, visual or verbal form.
• Fitzgerald Health Education Associates, Inc. disclaims any liability, loss, injury or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents of this presentation.
© Fitzgerald Health Education Associates, Inc.
58
Fitzgerald Health Education Associates, Inc.
85 Flagship Drive
North Andover, MA 01845-6154 978.794.8366 Fax-978.794.2455
Website: fhea.com
Learning & Testing Center: fhea.com/npexpert
www.facebook.com/fitzgeraldhealth
@npcert
© Fitzgerald Health Education Associates, Inc.
59