DISCUSSION PAPER: PERSONAL EXPERIENCE * Benjamin Alexander New York Blood Center New York. New York 10021 I am grateful to several of the authors preceding me, who provided manu- scripts covering their presentations. Although allusion will be made to some points in their material, most of my discussion derives from our personal and published experience.', 2 I should like to describe-no, redescribe-some stud- ies we made many years ago on four severely afflicted subjects who, except for rare lapses, received, as a prophylactic measure, normal fresh-frozen ci- trated plasma three to four times weekly for 10-20 months. From several aspects, not much has changed since our report, Limited time precludes de- tailed description. FIGURE 1 depicts the effects of repeated plasma infusions on the clotting times of three subjects. A similar program had been reported earlier,3 wherein management was purported to be successful in one patient by plasma administration weekly for three months. T.K. (FIGURE 1) was a subject aged 24 who had had numerous hemorrhages into joints, muscles, and genitourinary tract, and from the gums, frequently incapacitating and requiring innumerable hospitalizations. His original clotting time (modified Lee-White) was 65-90 minutes. He had been studied for years at another hospital, where weekly plasma therapy for two years was ineffective in preventing hemorrhages, which precluded steady employment. During our study, the patient received 206 plasma infusions of 150 ml each three times weekly for 18 months. For another one and one-half months he received 100-150 ml daily or twice daily, because of a bleeding episode. Thereafter, he received plasma therapy three times weekly, except for several lapses of four days to one month, when he left town on holidays. The regimen covered a period of 20 months, and the total plasma given was approximately 38 liters. I.G., aged 28, had a clotting time of 120 minutes. Since the age of six he had experienced bleeding episodes into joints and muscles, from mucous mem- branes, and into the genitourinary tract, becoming severely crippled and in- capacitated. During the study he received 270 infusions over 19 months, totaling about 41 liters, as follows: 150 ml three times weekly for nine months, four times weekly for one and one-half months, daily for one and one-half months, four times weekly for 5% months, and three times weekly thereafter. There were occasional short lapses (four or five days) for experimental pur- poses, and one for ten days because of an episode of jaundice (?serum hepa- titis), which prevented his return for scheduled treatment. R.R., 17 years old, with a clotting time of 180 minutes, had had hemorrhages since early infancy, mostly into joints and from deciduous teeth, requiring 90 hospital admissions, resulting in considerable crippling, and precluding school attendance. During this study he received 173 plasma infusions, each 180 ml, three times weekly for 13 months, totaling about 31 liters. There was one four- * Supported by PHS Grant HL 09011; 0901 1-OS1. 181
Transcript
DISCUSSION PAPER: PERSONAL EXPERIENCE *
Benjamin Alexander
New York Blood Center New York. New York 10021
I am grateful to several of the authors preceding me, who provided manu- scripts covering their presentations. Although allusion will be made to some points in their material, most of my discussion derives from our personal and published experience.', 2 I should like to describe-no, redescribe-some stud- ies we made many years ago on four severely afflicted subjects who, except for rare lapses, received, as a prophylactic measure, normal fresh-frozen ci- trated plasma three to four times weekly for 10-20 months. From several aspects, not much has changed since our report, Limited time precludes de- tailed description. FIGURE 1 depicts the effects of repeated plasma infusions on the clotting times of three subjects. A similar program had been reported earlier,3 wherein management was purported to be successful in one patient by plasma administration weekly for three months.
T.K. (FIGURE 1) was a subject aged 24 who had had numerous hemorrhages into joints, muscles, and genitourinary tract, and from the gums, frequently incapacitating and requiring innumerable hospitalizations. His original clotting time (modified Lee-White) was 65-90 minutes. He had been studied for years at another hospital, where weekly plasma therapy for two years was ineffective in preventing hemorrhages, which precluded steady employment. During our study, the patient received 206 plasma infusions of 150 ml each three times weekly for 18 months. For another one and one-half months he received 100-150 ml daily or twice daily, because of a bleeding episode. Thereafter, he received plasma therapy three times weekly, except for several lapses of four days to one month, when he left town on holidays. The regimen covered a period of 20 months, and the total plasma given was approximately 38 liters.
I.G., aged 28, had a clotting time of 120 minutes. Since the age of six he had experienced bleeding episodes into joints and muscles, from mucous mem- branes, and into the genitourinary tract, becoming severely crippled and in- capacitated. During the study he received 270 infusions over 19 months, totaling about 41 liters, as follows: 150 ml three times weekly for nine months, four times weekly for one and one-half months, daily for one and one-half months, four times weekly for 5% months, and three times weekly thereafter. There were occasional short lapses (four or five days) for experimental pur- poses, and one for ten days because of an episode of jaundice (?serum hepa- titis), which prevented his return for scheduled treatment.
R.R., 17 years old, with a clotting time of 180 minutes, had had hemorrhages since early infancy, mostly into joints and from deciduous teeth, requiring 90 hospital admissions, resulting in considerable crippling, and precluding school attendance. During this study he received 173 plasma infusions, each 180 ml, three times weekly for 13 months, totaling about 31 liters. There was one four-
* Supported by PHS Grant HL 09011; 0901 1-OS1.
181
182 Annals New York Academy of Sciences
day lapse, when icy road conditions prevented his coming to the laboratory for scheduled treatment.
Another subject, eight years old (not shown in FIGURE l ) , had had muscle and joint hemorrhages since early childhood, interfering seriously with school work and restricting physical activity. For prophylaxis he received 11 1 plasma infusions, 100 ml each three times weekly for ten months, with one lapse of two and one-half weeks because of chickenpox.
No attempt was made to give plasma of only one blood group, although for the first six months all donors were typed. Since no reactions (only ten were observed throughout the study; incidence 1.2-1 % severe, 3% moderate)
3 o s 4 o a m = ~ ~ ~ HOURS AFTER PLASMA ADMINISTRATION
FIGURE 1. Effect of repeated infusions of normal human plasma on clotting time of hemophilic blood. The numeral in parentheses represents the number of determi- nations of the clotting time at the designated interval. The points on the curves rep- resent the averages of these determinations.
could be attributed to incompatibility, typing was discontinued thereafter. Certain points evident in FIGURE 1 . are noteworthy: (a) the clot-promoting effects of normal plasma on the retarded clotting never changed over the long interval of treatment; (b) no refractoriness developed, a fact of utmost im- portance in view of the contrary report of Monroes and Jones,4 (c) the respon- siveness was uniform, and characteristic for each individual.
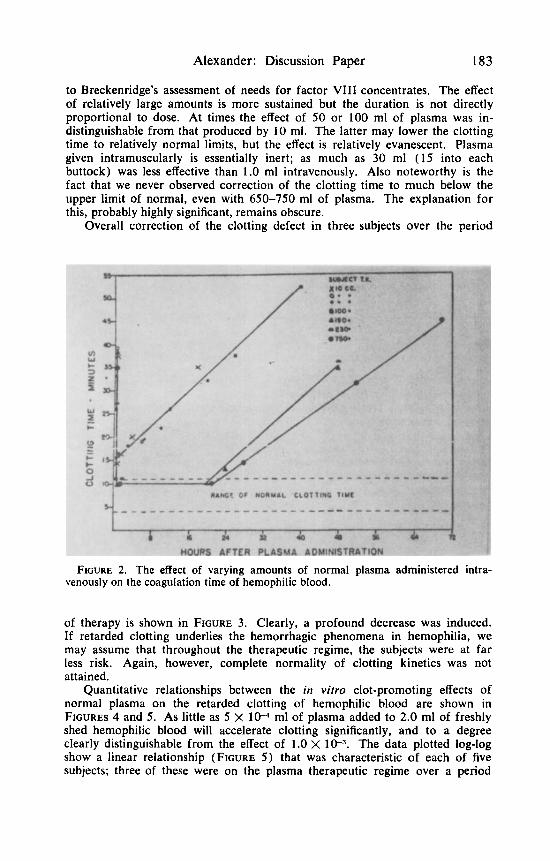
FIGURE 2 shows the effect of varying doses of normal plasma infused into a single patient. Note the striking difference between 100 and 190 ml in the duration of the effect and little difference between 230 and 750 ml. These data provide a quantitative basis for estimating plasma needs, predicated upon correction of the clotting defect inherent in a given patient. This is pertinent
Alexander: Discussion Paper 183
to Breckenridge’s assessment of needs for factor VIII concentrates. The effect of relatively large amounts is more sustained but the duration is not directly proportional to dose. At times the effect of 50 or 100 ml of plasma was in- distinguishable from that produced by 10 ml. The latter may lower the clotting time to relatively normal limits, but the effect is relatively evanescent. Plasma given intramuscularly is essentially inert; as much as 30 ml (15 into each buttock) was less effective than 1.0 ml intravenously. Also noteworthy is the fact that we never observed correction of the clotting time to much below the upper limit of normal, even with 650-750 ml of plasma. The explanation for this, probably highly significant, remains obscure.
Overall correction of the clotting defect in three subjects over the period
FIGURE 2. The effect of varying amounts of normal plasma administered intra- venously on the coagulation time of hemophilic blood.
of therapy is shown in FIGURE 3. Clearly, a profound decrease was induced. If retarded clotting underlies the hemorrhagic phenomena in hemophilia, we may assume that throughout the therapeutic regime, the subjects were at far less risk. Again, however, complete normality of clotting kinetics was not attained.
Quantitative relationships between the in vitro clot-promoting effects of normal plasma on the retarded clotting of hemophilic blood are shown in FIGURES 4 and 5. As little as 5 x 1W ml of plasma added to 2.0 ml of freshly shed hemophilic blood will accelerate clotting significantly, and to a degree clearly distinguishable from the effect of 1 .O x 1 W$. The data plotted log-log show a linear relationship (FIGURE 5 ) that was characteristic of each of five subjects: three of these were on the plasma therapeutic regime over a period
184 Annals New York Academy of Sciences
FIGURE 3. The overall reduction in coagulation time induced by regularly admin- istered normal plasma to persons with hemophilia. The areas enclosed by the rec- tangles represent the clotting time over the study period, integrated from the curves in FIGURE 1.
of 10-23 months. The linear relationship remained relatively constant through- out and seemed to correlate with the clinical severity of the disease. Thus, T.K., with the slope of -0.35, had the mildest; I.G., slope -0.75, had the worst; R.R. and J.G., with slopes of -0.62 and -0.59, respectively, had mod- erate disease, as judged by the degree of crippling and incapacitation.
That our therapeutic regime, admittedly laborious and cumbersome, pro- duced substantial, sustained reduction in overall clotting impairment is indis-
FIGURE 4. Correction of retarded clotting of freshly drawn hemophilic blood by addition of normal citrated human plasma in vitro. For details see text.
Alexander: Discussion Paper 185
putable. The cardinal question is whether this approach was effective in preventing, or reducing the number of, hemorrhagic episodes, or “nipping them in the bud.” It is practically impossible to establish or record all the minor hemorrhages and ecchymoses that a hemophiliac ordinarily experiences, gen- erally dismissed lightly. During the course of prophylactic plasma therapy, our subjects were unanimous in their opinion that hemorrhagic phenomena were more minor and less frequent, despite a pronounced increase in activity. With every lapse in therapy, the lesser hemorrhagic phenomena reappeared.
We felt that our prophylactic regimen was valid, clinically effective, safe, and promising. This seems to have been borne out by more recent experience of others with factor VIII concentrates. T.K. is one case in point. It will be
FIGURE 5 . Logarithmic plot of relationship presented in FIGURE 4.
recalled that a similar prophylactic regimen of plasma given once weekly at another hospital was ineffective. In contrast, when he received plasma regularly three times weekly, he had no major hemorrhages despite greatly increased activity (swimming, bowling, baseball, basketball, gymnastics, squash, running, horseback riding). In no instance was there more than localized ecchymosis even following types of trauma that had hitherto resulted in moderate to severe hemorrhages. Hemostatis following gum scraping for dental care was good, and simplified for the hygienist. For the first time, the patient could do sus- tained remunerative work for one and one-half years. During the therapeutic interval, however, he experienced four significant hemorrhagic episodes. The first occurred five days after a plasma infusion, when, while on a five-day holiday the patient fell down some steps, incurring severe trauma to arm and
186 Annals New York Academy of Sciences
leg. The second hemorrhage, hematuria, developed after four days without plasma, again while the patient was traveling. This subsided within one week after therapy was resumed.
A third episode, oozing from an extensive pyogenic ulceration of the buccal mucosa, which persisted despite plasma therapy, ceased dramatically after the first of several penicillin injections administered in doses of 200 000 units with each plasma infusion for one week. The ulcer cleared promptly. The fourth episode occurred spontaneously when the subject was again on a month’s holiday; incapacitating hemarthroses developed five days after the last plasma, followed later by hematuria. This persisted for six weeks despite several whole- blood transfusions and plasma infusions daily or twice daily, each of which reduced the clotting time to normal range. The addition of penicillin to some of the plasmas was also ineffective in instituting hemostasis.
The clinical experience with I.G. also warrants brief emphasis: he had suffered extensive crippling as a result of repeated hemarthroses and hemor- rhages into the gastrocnemii. This patient, likewise, was rehabilitated. For the first time in his life, he was able to do some remunerative work in his profession (commercial artist). Despite incapacitation as a consequence of past hemor- rhages, he was able to travel 80 miles for each treatment. During the study he had four hemorrhagic episodes. Two, into elbow and knee, occurred after plasma had been withheld for four days for experimental purposes; the third, an ileofemoral bleed, began during a weekend about 60 hours after a plasma infusion and required hospitalization. Therapy was changed from three to four infusions weekly. The fourth episode occurred when plasma was omitted for ten days when, because of jaundice, he was advised to remain at home. Except for the ileofemoral episode, the others were mild to moderate, each lasting about one week while therapy was continued.
Because it was felt, after one year’s observation, that this patient’s hem- orrhagic tendency could be readily controlled by repeated plasma infusions, a bilateral open tenoplasty of the Achilles tendons was performed to overcome abnormal plantar flexion consequent to old hemorrhages into the gastrocnemii. It was felt that this handicap compromised gait, resulting in undue strain on the knees and thus predisposing them to trauma. Seven days after an uneventful operation, the wounds began to ooze despite daily plasma infusions which re- duced the clotting time to relatively normal levels. At this time, the patient was slightly febrile and the wounds had partially separated. Because infection was suspected, the patient was given full doses of oral sulfadiazine and 200 000 units of intravenous penicillin with a daily plasma infusion for one week. Following the first dose of penicillin, bleeding ceased and recovery was un- eventful, the wounds healing by secondary intention. One hundred and fifty cubic centimeters of plasma was given daily for 42 days and every other day thereafter. The operative result was good: the patient’s gait was greatly im- proved.
These clinical observations are noteworthy since they highlight certain important aspects inherent in a prophylactic program. Regular and frequent administration of plasma, and presumably also of concentrates, is essential, as we have found lapses in therapy are apt to result in recurrence of bleeding episodes. Secondly, “tailoring” therapy to the needs of the individual is im- portant. Thirdly, the experience with I.G. indicated very early that recon- structive elective surgery was feasible.
In closing I should like to bring out one final point relevant to the hazard
Alexander : Discussion Paper 187
of hepatitis. Clearly, the use of plasma or concentrates that derive from a minimal number of donors minimizes the risk.5 I.W. became jaundiced during the therapeutic regime. Assuming that this was an episode of serum hepatitis (although we cannot be sure), our figures, calculated from our records of his having received plasma from about 540 individual donors u p to four months (presumptive incubation period) before he showed clinical jaundice, suggest that the incidence of S.H. infectiousness in the Boston population at large was (in 1945-1947) about 0.20% t if we consider that the other three hemophiliacs on the regimen were still susceptible to the disease, or 0.8% if they were ex- cluded. The latter figure would seem more valid, since it is well known that hemophiliacs or others who have received blood frequently for other diseases are more likely to have acquired some immunity.
It would be of interest to know how our approximate figures compare with more recent data predicated on newer epidemiology studies with more sophisti- cated diagnostic techniques. It should be emphasized that in our study only a few individuals were challenged with a large number of samples of potentially infectious material, whereas in most other similar studies a large number of subjects were challenged with known infectious material or with blood and/ or its derivatives obtained from a large number of random, or now screened, donors.
REFERENCES
1. ALEXANDER, B. & G. LANDWEHR. 1948. Studies of hemophilia. I. The control of hemophilia by repeated infusions of normal human plasma. J.A.M.A. 138:
1. ALEXANDER, B. & G. LANDWEHR. 1948. The assay of the antihemophilic clot- promoting principle in normal human plasma with some observations on the re- lative potency of certain plasma fractions. J. Clin. Invest. 27: 98-105.
3. JOHNSON, J. B. 1943. Management of hemophilia with lyophile human plasma intravenously injected. J.A.M.A. 118: 799.
4. MONROE, F. L. & H. W. JONES. 1943. The detrimental effect of frequent trans- fusions in the treatment of a patient with hemophilia. Amer. J. Med. Sci. 206: 710.
5. GROSSMAN, C. M. & E. W. SAWARD. 1946. Homologous serum jaundice following the administration of commercial pooled plasma. New Eng. J. Med. 234: 181.
6. NEEFE, J. R., S. S. GELLIS & J. STOKES. JR. 1946. Homologous serum hepatitis and infectious (epidemic) hepatitis. Amer. J. Med. 1: 3.
1 74- 179.
T Susceptibility to serum hepatitis is far from loo%.'' 1. K. received plasmas from 540 individual donors by record, totalling 121 liters.