74
Disorders of Small Disorders of Small and Large Bowel and Large Bowel Jay Green Jay Green October 26, 2006 October 26, 2006
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | eustace-robbins |
| View: | 214 times |
| Download: | 1 times |

Disorders of Small Disorders of Small and Large Boweland Large BowelJay GreenJay Green
October 26, 2006October 26, 2006

Case 1Case 1
54 y.o. F, abdominal pain54 y.o. F, abdominal pain Started 2 days ago, shortly after Big MacStarted 2 days ago, shortly after Big Mac Hurts all over, comes and goes, crampyHurts all over, comes and goes, crampy +D yesterday, bloated, +N today, +D yesterday, bloated, +N today, ø Vø V PMH: DMII, HTN, TAH/BSO (’04)PMH: DMII, HTN, TAH/BSO (’04) Ideas?Ideas?
DDx - ApproachDDx - Approach
Think anatomyThink anatomyIntraperitonaeal, retroperitoneal, otherIntraperitonaeal, retroperitoneal, other
Think VITAMIN D, VINDICATED, whatever…Think VITAMIN D, VINDICATED, whatever… VascularVascular
Ischemic gut, MI, AAAIschemic gut, MI, AAA InfectionInfection
Gastro, PUD, psoas abscessGastro, PUD, psoas abscess NeoplasticNeoplastic
IntussusceptionIntussusception InflammatoryInflammatory
Diverticulitis, Cholecystitis, Pancreatitis, AppendicitisDiverticulitis, Cholecystitis, Pancreatitis, Appendicitis TraumaticTraumatic
ObstructionObstruction PregnancyPregnancy

Small Bowel ObstructionSmall Bowel Obstruction
Top 3 causes?Top 3 causes? HerniaHernia AdhesionsAdhesions CACA
Most likely to cause strangulation?Most likely to cause strangulation? Hernia – often closed loopHernia – often closed loop
Others to think about?Others to think about? Gallstone ileus, volvulus, intussusception, Gallstone ileus, volvulus, intussusception,
abscess, hematoma, foreign bodyabscess, hematoma, foreign body

More than half of SBO recurrMore than half of SBO recurr TrueTrue FalseFalse
Bathing in tomato juice removes the Bathing in tomato juice removes the smell of a skunksmell of a skunk
TrueTrue FalseFalse

SBO – Quick factsSBO – Quick facts
20% of acute abdo admissions20% of acute abdo admissions Mortality <5% (30% with strangulation, Mortality <5% (30% with strangulation,
60% in 1900)60% in 1900) >50% recur>50% recur

H&PH&P
Recurrent abdo pain, crampy, <>Recurrent abdo pain, crampy, <> Worry if pain becomes constant severeWorry if pain becomes constant severe Vomiting, distension, constipationVomiting, distension, constipation Prev surgeryPrev surgery Vitals: normal, tachy, hypoTN, feverVitals: normal, tachy, hypoTN, fever Distention, Distention, ∆∆BS (BS (↑ pitch), tympany↑ pitch), tympany ±scars/hernia, ±tender mass±scars/hernia, ±tender massBohner H, et al: Simple data from history and physical examination help to exclude bowel obstruction and to avoid radiographic studies in patients with acute abdominal pain. Eur J Surg 1998; 164:777
Vomiting, distension, constipationVomiting, distension, constipation Prev surgeryPrev surgery
∆ ∆BSBS
Review of the basicsReview of the basics
Types?Types? Mechanical & functionalMechanical & functional Simple & closed loop (Simple & closed loop (±strangulation)±strangulation)
Common causes of ileus?Common causes of ileus? Trauma, infection, sx, meds, metabolic, Trauma, infection, sx, meds, metabolic,
renal colicrenal colic

Physicians reliably can distinguish bowel Physicians reliably can distinguish bowel strangulation from simple obstructionstrangulation from simple obstruction
TrueTrue FalseFalse
Cracking knuckles leads to arthritisCracking knuckles leads to arthritis TrueTrue FalseFalse

Simple vs Strangulated - Simple vs Strangulated - How good are we?How good are we?
Confident diagnosis of “non-strangulating Confident diagnosis of “non-strangulating obstruction” wrong 31% of the time.obstruction” wrong 31% of the time.
No parameter is sensitive, specific, or No parameter is sensitive, specific, or predictive for strangulationpredictive for strangulation
Not very good!Not very good!
Sarr et al. Preoperative recognition of intestinal strangulation obstruction: Prospective evaluation of diagnostic capability. Am J Surg 145:176-182, 1983.

PathophysiologyPathophysiology
Mechanical SBO Mechanical SBO
→ → prox dilationprox dilation
→ ↑ → ↑ local peristalsis local peristalsis
→ ↑ → ↑ secretory activitysecretory activity
→ ↓ → ↓ reabsorption fluid/lytesreabsorption fluid/lytes
→ → capillary/lymphatic obstruction capillary/lymphatic obstruction
→ → edema edema
→ → perforation or strangulationperforation or strangulation

InvestigationsInvestigations
Labs:Labs: ↑↑WBC, WBC, ±±↑CPK, ↑CPK, ±±↑lactate↑lactate
Imaging:Imaging: 3 views (60% +SBO, 25% suggestive)3 views (60% +SBO, 25% suggestive)
Five places to look for air?Five places to look for air? How many A/F levels?How many A/F levels? Dilated?Dilated?




CT Scan?CT Scan?
Not required for diagnosisNot required for diagnosis Can help define site/causeCan help define site/cause
Other imaging?Other imaging? Small bowel series, U/SSmall bowel series, U/S
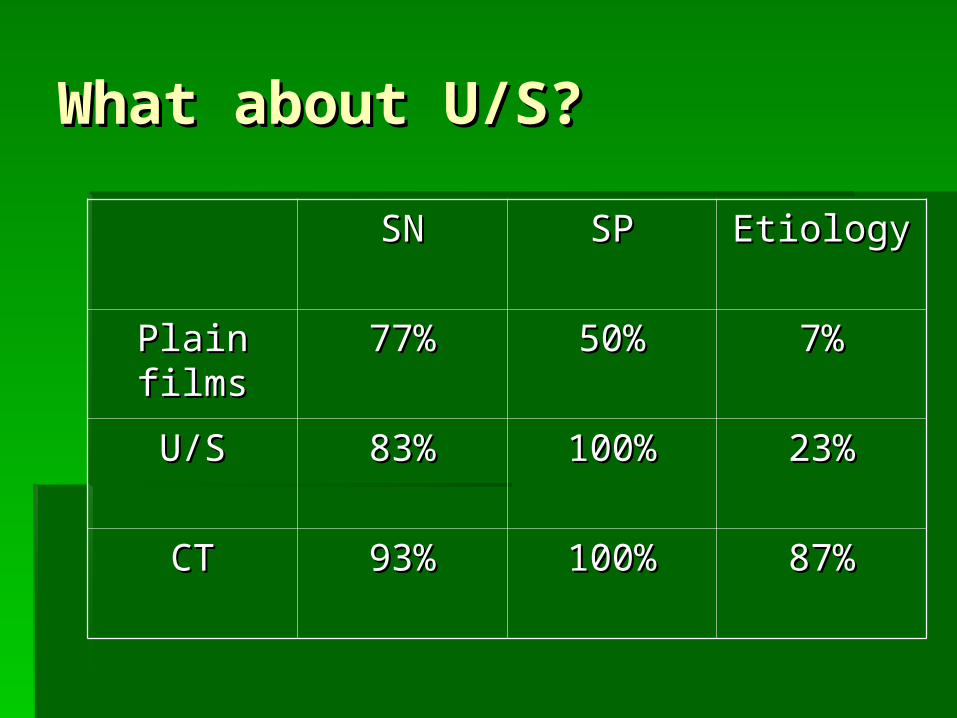
What about U/S?What about U/S?
SNSN SPSP EtiologyEtiology
Plain filmsPlain films 77%77% 50%50% 7%7%
U/SU/S 83%83% 100%100% 23%23%
CTCT 93%93% 100%100% 87%87%

½ of complete SBO resolve ½ of complete SBO resolve spontaneouslyspontaneously
TrueTrue FalseFalse
Eating 3 poppy seed bagels may result in Eating 3 poppy seed bagels may result in positive urine drug screen for opiatespositive urine drug screen for opiates
TrueTrue FalseFalse
ManagementManagement
Fluid resuscitationFluid resuscitation DecompressionDecompression
NG tubeNG tube
?Antibiotics?Antibiotics Observation vs. surgeryObservation vs. surgery
““never let the sun rise or set on an SBO”never let the sun rise or set on an SBO”
75% of partial/30-50% complete resolve75% of partial/30-50% complete resolve

Take home pointsTake home points
You are not good at dx strangulationYou are not good at dx strangulation
AXR - >2 A/F levels, >2.5cm, air x 5AXR - >2 A/F levels, >2.5cm, air x 5
½ of SBO resolve spontaneously½ of SBO resolve spontaneously
Case 2Case 2
28M central/RLQ crampy abdominal 28M central/RLQ crampy abdominal pain, Npain, N
Last BM this am, no fever/chills/VLast BM this am, no fever/chills/V Best guess?Best guess? 28F same hx?28F same hx?
25% signs initially suggestive of appe = gyne25% signs initially suggestive of appe = gyne 84F type II DM same hx?84F type II DM same hx? 4M same hx? 4M same hx?

Case 2Case 2
Vitals – 37.3, 85, 126/85, 18Vitals – 37.3, 85, 126/85, 18 RLQ tenderness, +guardingRLQ tenderness, +guarding
Investigations?Investigations?

Appendicitis – Quick factsAppendicitis – Quick facts
7% lifetime incidence7% lifetime incidence 250 000 cases/yr in the USA 250 000 cases/yr in the USA First appendectomy – 1735First appendectomy – 1735

What the heck is this?What the heck is this?
The AppendixThe Appendix
"Its major importance would appear to be "Its major importance would appear to be financial support of the surgical financial support of the surgical profession." - Alfred Sherwood Romerprofession." - Alfred Sherwood Romer
Leonardo da Vinci (1492)
PathophysiologyPathophysiology
ObstructionObstruction ↑ ↑ pressurepressure distensiondistension ischemia + bacteria/PMN invasionischemia + bacteria/PMN invasion swells, irritatesswells, irritates necrosis and rupturenecrosis and rupture

HistoryHistory
Three most common symptoms?Three most common symptoms? abdo pain, anorexia, nauseaabdo pain, anorexia, nausea
Rule out based on pain location?Rule out based on pain location? no, can even have LUQ painno, can even have LUQ pain
Physical examPhysical exam
Vitals – 37.3, 85, 126/85, 18Vitals – 37.3, 85, 126/85, 18 Do normal vitals r/o appendicitis?Do normal vitals r/o appendicitis? What if T = 38.1?What if T = 38.1?
Low grade fever in 15% (40% if ruptured)Low grade fever in 15% (40% if ruptured)
EponymsEponyms McBurney’sMcBurney’s, Rovsing’s, Obturator, Psoas, , Rovsing’s, Obturator, Psoas,
DunphyDunphy

H&PH&P
Three important signs/symptoms?Three important signs/symptoms? RLQ pain, rigidity, migration of painRLQ pain, rigidity, migration of pain
Four to help rule out appendicitis?Four to help rule out appendicitis? Pain > 48h, similar pain, lack of migration, Pain > 48h, similar pain, lack of migration,
lack of lack of ↑↑ pain with movement/cough pain with movement/cough
CMT is uncommon in women with acute CMT is uncommon in women with acute appendicitisappendicitis
TrueTrue FalseFalse
The air expelled in a sneeze can travel The air expelled in a sneeze can travel up to 100mphup to 100mph
TrueTrue FalseFalse
Classic AppendicitisClassic Appendicitis
Peri-umbilical pain Peri-umbilical pain RLQ migration RLQ migration N, anorexia, VN, anorexia, V No history of similar pain in pastNo history of similar pain in past Pain < 48hrs at presentationPain < 48hrs at presentation Pain Pain ↑ with movement/cough↑ with movement/cough Low grade feverLow grade fever Rigidity & guardingRigidity & guarding Local RLQ tendernessLocal RLQ tenderness
Serial examsSerial exams
Review of 30 years of publicationsReview of 30 years of publications ““active observation” = reassess pt q2-3hactive observation” = reassess pt q2-3h Pain resolved in 1/3 of patients Pain resolved in 1/3 of patients No change in perforation rateNo change in perforation rate Negative appendectomy rate 6%Negative appendectomy rate 6%
vs 20-30% (?lower with CT or U/S)vs 20-30% (?lower with CT or U/S)
Jones PF. Suspected acute appendicitis: Trends in management over 30 years. Jones PF. Suspected acute appendicitis: Trends in management over 30 years. Br J SurgBr J Surg 2001; 88:1570-77. 2001; 88:1570-77.
What labs?What labs?
Commonly orderedCommonly ordered CBC, CBC, ββ-hcg, U/A-hcg, U/A ±LFT’s/lipase, ±CRP±LFT’s/lipase, ±CRP
FindingsFindings ↑ ↑ WBC, U/A – pyuria, microscopic hematuriaWBC, U/A – pyuria, microscopic hematuria
Necessary?Necessary?
ββ-hcg!-hcg!

U/S vs CTU/S vs CT
CTCT SN 94%, SP 95%, LR+ 13.3, LR- 0.09SN 94%, SP 95%, LR+ 13.3, LR- 0.09 + usually visualize appendix, not operator + usually visualize appendix, not operator
dependent, ID other pathologydependent, ID other pathology - radiation- radiation
Contrast?Contrast? Rectal – best but not practicalRectal – best but not practical Oral – delay, ?tolerated, esp. helpful in thin/kidsOral – delay, ?tolerated, esp. helpful in thin/kids IV – not recommendedIV – not recommended

U/S vs CTU/S vs CT
U/SU/S SN 86%, SP 81%, LR+ 5.8, LR- 0.19SN 86%, SP 81%, LR+ 5.8, LR- 0.19 + pregnant, kids, female, thin pts+ pregnant, kids, female, thin pts - obese, strictures, retrocecal, normal- obese, strictures, retrocecal, normal
MRI?MRI? Very sensitive but not availableVery sensitive but not available
?Change Management??Change Management?
2 studies of CT in pts w/ suspected 2 studies of CT in pts w/ suspected appendicitis comparing Tx plan before & after appendicitis comparing Tx plan before & after access to results of scansaccess to results of scans CT changed disposition in 27 – 59% of ptsCT changed disposition in 27 – 59% of pts Prevented d/c of ~3% pts w/ appendicitisPrevented d/c of ~3% pts w/ appendicitis Prevented negative laparotomy in 3-13%Prevented negative laparotomy in 3-13% Alternate Dx in 11-20%Alternate Dx in 11-20%
Frank et al. Unenhanced helical CT scanning of the abdomen and pelvis Frank et al. Unenhanced helical CT scanning of the abdomen and pelvis changes disposition of patients presenting to the emergency department changes disposition of patients presenting to the emergency department with possible acute appendicitis. J Emerg Med 2002; 23: 1-7with possible acute appendicitis. J Emerg Med 2002; 23: 1-7
Rao et al. Effect of computed tomography of the appendix on treatment Rao et al. Effect of computed tomography of the appendix on treatment of patients and use of hospital resources. N Eng J Med. 1998; 338: 141-of patients and use of hospital resources. N Eng J Med. 1998; 338: 141-66
Thanks Moritz!

To image or not?To image or not?
Imaging based on risk-stratificationImaging based on risk-stratification Don’t image:Don’t image:
Low risk – Low risk – minimal physical findings, hungry, alternative dx, minimal physical findings, hungry, alternative dx, hx similar pain, sympt > 3 dayshx similar pain, sympt > 3 days
First few hours of painFirst few hours of pain
Image Image Intermediate risk – lack classic appendicitis findingIntermediate risk – lack classic appendicitis finding
?Image?Image High risk – classic presentationHigh risk – classic presentation Will go to OR anywayWill go to OR anyway

Wake the surgeon?Wake the surgeon?
Time from onset of symptoms to rupture?Time from onset of symptoms to rupture? 24-36 hours24-36 hours
Average time to seek medical careAverage time to seek medical care 17 hours17 hours
Complication rate Complication rate 3% vs 12% with rupture3% vs 12% with rupture
MortalityMortality <0.1% vs 3-4% with rupture<0.1% vs 3-4% with rupture

Take home pointsTake home points
Normal vitals do not rule out appendicitisNormal vitals do not rule out appendicitis
Think about U/S over CT in skinny/kidsThink about U/S over CT in skinny/kids
Image pts with equivocal presentationImage pts with equivocal presentation
Single most important lab test Single most important lab test ββ-hcg-hcg

Mesenteric adenitis?Mesenteric adenitis?
Most common associated conditionMost common associated condition 5-10% admissions for appendicitis5-10% admissions for appendicitis
?More common than appendicitis?More common than appendicitis Mostly childrenMostly children Non-specific infl. of mesenteric LNNon-specific infl. of mesenteric LN
Can follow viral illnessCan follow viral illness Yersinia species (Y. enterocolitica)Yersinia species (Y. enterocolitica)
Mesenteric adenitis?Mesenteric adenitis?
O/E:O/E: ±±Mild feverMild fever Diffuse tenderness, RLQ, no peritonitisDiffuse tenderness, RLQ, no peritonitis 20% other lymphadenopathy20% other lymphadenopathy
Ix: Ix: ±↑WBC ±↑WBC U/S or CT may be helpfulU/S or CT may be helpful
Tx: Tx: none, self-limitednone, self-limited
Case 3Case 3
65M65M Suprapubic and LLQ pain x days, similar bouts Suprapubic and LLQ pain x days, similar bouts
of pain in pastof pain in past Anorexia, nauseaAnorexia, nausea O/E: Vitals normal, LLQ tender, no peritoneal O/E: Vitals normal, LLQ tender, no peritoneal
signs, ?distendedsigns, ?distended
#1 in DDx?#1 in DDx? Initial investigations?Initial investigations?
Diverticular disease factsDiverticular disease facts
10% > 45yrs, 80% > 80yrs10% > 45yrs, 80% > 80yrs ?Dietary deficiency in fibre?Dietary deficiency in fibre 85% L-sided (opposite in Japan)85% L-sided (opposite in Japan)
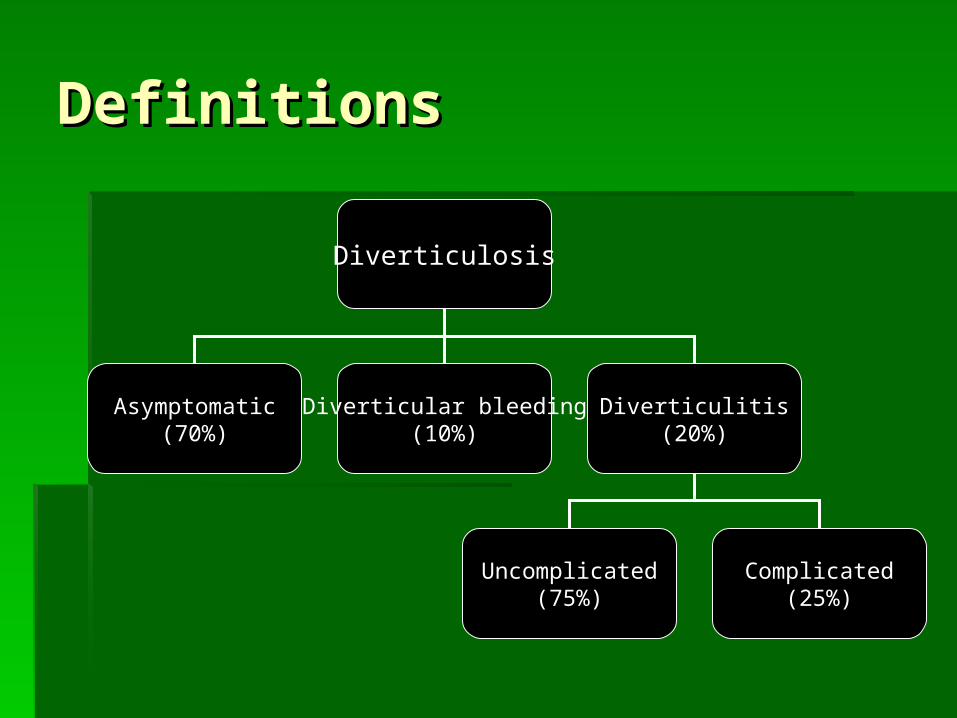
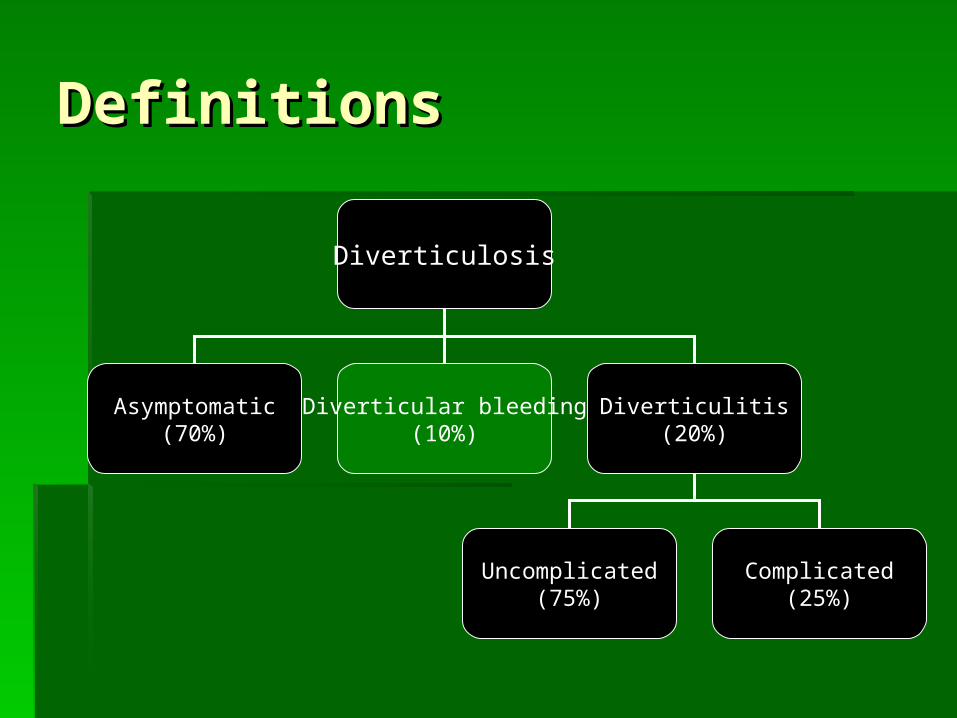
DefinitionsDefinitions
Diverticulosis
Asymptomatic(70%)
Diverticular bleeding(10%)
Diverticulitis(20%)
Uncomplicated(75%)
Complicated(25%)

DefinitionsDefinitions
Diverticulosis
Asymptomatic(70%)
Diverticular bleeding(10%)
Diverticulitis(20%)
Uncomplicated(75%)
Complicated(25%)

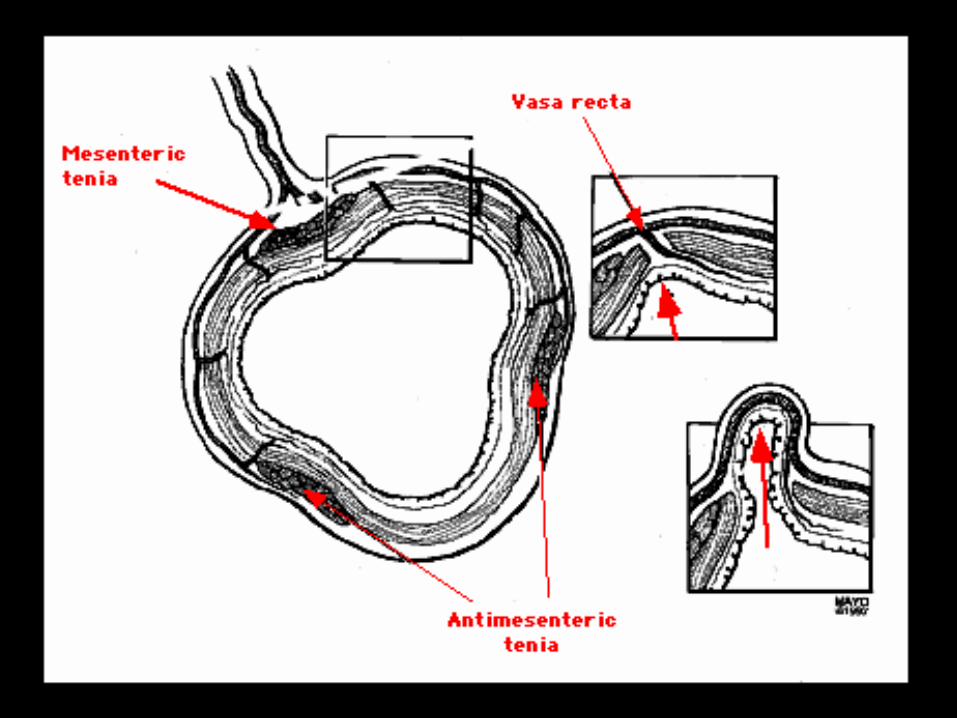
Anatomy/PathogenesisAnatomy/Pathogenesis
Vasa recta penetrate colonic wallVasa recta penetrate colonic wall Forms weak pointsForms weak points
Small (low fibre) stool Small (low fibre) stool ↑ pressure ↑ pressure herniation of mucosa at vasa rectaherniation of mucosa at vasa recta

DiverticulosisDiverticulosis

Clinical featuresClinical features
Usually nilUsually nil Can present like IBSCan present like IBS
Abdo pain/crampingAbdo pain/cramping BloatingBloating Constipation/diarrheaConstipation/diarrhea
ManagementManagement
If necessaryIf necessary AnalgesiaAnalgesia Anti-spasmodicsAnti-spasmodics
Modify natural history of diseaseModify natural history of disease High-fibre dietHigh-fibre diet ±stool softeners±stool softeners
Case 3bCase 3b
65M65M HematocheziaHematochezia No painNo pain O/E: Vitals normal, abdo benign, FOB+O/E: Vitals normal, abdo benign, FOB+
Top 3 in DDx?Top 3 in DDx?
DefinitionsDefinitions
Diverticulosis
Asymptomatic(70%)
Diverticular bleeding(10%)
Diverticulitis(20%)
Uncomplicated(75%)
Complicated(25%)

Diverticular bleedingDiverticular bleeding
40% of all LGIB 40% of all LGIB 5% severe bleed5% severe bleed Typically Typically painless painless hematocheziahematochezia
ManagementManagement
ResuscitationResuscitation Localization of bleeding siteLocalization of bleeding site
r/o UGIB, colonoscopyr/o UGIB, colonoscopy ± angiography or radionuclide scan± angiography or radionuclide scan
TreatmentTreatment SurgerySurgery

DefinitionsDefinitions
Diverticulosis
Asymptomatic(70%)
Diverticular bleeding(10%)
Diverticulitis(20%)
Uncomplicated(75%)
Complicated(25%)
DiverticulitisDiverticulitis
Diverticulum obstructed Diverticulum obstructed
inflammation inflammation microperforation microperforation
pericolic inflammationpericolic inflammation
painpain

Diagnosis – H&P, LabsDiagnosis – H&P, Labs
HistoryHistory LLQ pain, several days, prev. painLLQ pain, several days, prev. pain
O/EO/E Fever, LLQ tenderness, Fever, LLQ tenderness, ±distension, ±mass±distension, ±mass
LabsLabs ↑↑WBCWBC

Diagnosis - ImagingDiagnosis - Imaging
OptionsOptions Plain filmsPlain films Barium enemaBarium enema Water-soluble contrast enemaWater-soluble contrast enema ColonoscopyColonoscopy CT scanCT scan
Barium enema is an appropriate Barium enema is an appropriate investigation in acute diverticulitisinvestigation in acute diverticulitis
TrueTrue FalseFalse
Spicy food can cause ulcersSpicy food can cause ulcers TrueTrue FalseFalse
Plain filmsPlain films
Not useful in diagnosis of diverticulitisNot useful in diagnosis of diverticulitis Utility lies in ruling out obstruction/ Utility lies in ruling out obstruction/
perforationperforation
Barium enemaBarium enema
Useful to diagnose asymptomatic Useful to diagnose asymptomatic diverticulosisdiverticulosis
CONTRAINDICATED in acute CONTRAINDICATED in acute diverticulitisdiverticulitis Potential for barium peritonitisPotential for barium peritonitis


Water-soluble contrast Water-soluble contrast enemaenema
Less detail than bariumLess detail than barium Can see contrast collect in abscess Can see contrast collect in abscess
cavity, peritoneum, along fistulaecavity, peritoneum, along fistulae Less info than CT about disease extentLess info than CT about disease extent

ColonoscopyColonoscopy
Not for acute settingNot for acute setting
CT scanCT scan
Investigation of choiceInvestigation of choice SN 69-95%, SP 75-100%SN 69-95%, SP 75-100% Evaluate extent of diseaseEvaluate extent of disease Exclude other pathologyExclude other pathology If known uncomplicated diverticulitis – not If known uncomplicated diverticulitis – not
necessarynecessary
ManagementManagement
UncomplicatedUncomplicated OutpatientOutpatient AnalgesiaAnalgesia Oral AbxOral Abx
Septra/Flagyl, Cipro/Flagyl, ClavulinSeptra/Flagyl, Cipro/Flagyl, Clavulin
FibreFibre F/UF/U
ManagementManagement
ComplicatedComplicated InpatientInpatient AnalgesiaAnalgesia IV AbxIV Abx Surgery vs. medical managementSurgery vs. medical management
Surgery or not?Surgery or not?
First episodeFirst episode Usually medical managementUsually medical management 3-30% recurr3-30% recurr
Subsequent episodes, Subsequent episodes, immunocompromisedimmunocompromised More likely to require surgery or More likely to require surgery or
precutaneous abscess drainageprecutaneous abscess drainage

Take home pointsTake home points
Diverticulosis Diverticulosis asympt vs. IBS-like asympt vs. IBS-like
bleeding bleeding
inflammationinflammation
Imaging of choice in diverticulitis is CTImaging of choice in diverticulitis is CT
Most uncomplicated pts can go homeMost uncomplicated pts can go home
Questions?Questions?
ReferencesReferences
Ferri: Ferri's Clinical Advisor: Ferri: Ferri's Clinical Advisor: Instant Diagnosis Instant Diagnosis and Treatmentand Treatment, 8th ed., 2006 Mosby, 8th ed., 2006 Mosby
Leyner, Goldberg. Leyner, Goldberg. Why Do Men Have Nipples?Why Do Men Have Nipples? 2005 Three Rivers Press2005 Three Rivers Press
Mandell, Bennett, & Dolin: Mandell, Bennett, & Dolin: Principles and Principles and Practice of Infectious DiseasesPractice of Infectious Diseases, 6th ed., 2005 , 6th ed., 2005 Churchill LivingstoneChurchill Livingstone
Marx, Hockberger & Walls. Marx, Hockberger & Walls. Rosen’s Rosen’s Emergency MedicineEmergency Medicine, 6, 6thth ed., 2006 Mosby ed., 2006 Mosby
UpToDateUpToDate

![Lymphoproliferative disorders in inflammatory bowel ... · transplantation lymphoproliferative disorders (PTLD), which can develop due to both primary and secondary immunosuppression[6].](https://static.documents.pub/doc/80x56/5f0addb37e708231d42db993/lymphoproliferative-disorders-in-inflammatory-bowel-transplantation-lymphoproliferative.jpg)





![RESEARCH ARTICLE Open Access Bacteroides ......disorders, such as inflammatory bowel diseases [22-25], irritable bowel syndrome [26], colorectal cancer [27,28] and obesity [29] have](https://static.documents.pub/doc/80x56/601c289ed6c5db6c731ba9e0/research-article-open-access-bacteroides-disorders-such-as-inflammatory.jpg)









