BSc (Hons) Osteopathy - Module: U49599 Effectiveness of a Postural Awareness Software (PAS) for increasing the postural awareness on computer users An exploratory study into PAS user’s perception of changes to their posture for a better understanding of the potential of this tool to the Osteopathic profession By Rui Santiago Supervisor: Philip von Hauenschild Keywords: Posture Awareness, Reminder Software, Computer User. Word Count: 4275 27-03-2011
Transcript
BSc (Hons) Osteopathy - Module: U49599
Effectiveness of a Postural Awareness Software (PAS) for increasing the postural awareness on
computer users
An exploratory study into PAS user’s perception of changes to their posture for a better understanding of the potential of this tool to the
Osteopathic profession
By Rui Santiago Supervisor: Philip von Hauenschild
4. Results ......................................... ................................................................14 4.1. General Demographics ......................................................................................14 4.2. Posture Awareness Data ...................................................................................15 4.3. Exploratory Data ................................................................................................16
5. Discussion ...................................... .............................................................19 5.1. Relationship between awareness and symptoms ..............................................19 5.2. Exploratory Questions........................................................................................19 5.3. Study Limitations ...............................................................................................21 5.4. Clinical Implications ...........................................................................................23 5.5. Suggestions for future research.........................................................................24
6. Conclusion...................................... .............................................................25 7. Acknowledgement................................. ......................................................26 8. References ...................................... .............................................................27 Appendix A – Participant Information Sheet......... ........................................32 Appendix B – Exercises Handout ..................... .............................................35 Appendix C – PAS installation instructions......... .........................................37 Appendix D – Initial Questionnaire ................. ...............................................39 Appendix E – Final Questionnaire ................... ..............................................43 Appendix F – Consent Form.......................... .................................................47 Appendix G – GANTT Project Plan .................... ............................................49
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
3/49
1. Abstract Background: The number of work days lost due to musculoskeletal disorders (MSD) makes the
search for strategies to prevent them a priority. This study looked at the effectiveness of PAS on
a potential precursor for MSD’s: posture awareness.
Participants: Data was examined from 41 participants (26 female, 15 male) out of an initial 50,
drop out rate of 18%. 68% of patients were aged between 20 and 40. 14 were osteopathy
patients.
Methods: Participants installed PAS in their computer and used it for 2 weeks. It prompted the
participant to perform previously shown exercises during the use of computer.
5-point Likert scales were used in 2 questionnaires to auto-assess posture awareness before and
after the use of PAS. The patients’ compliance with the exercises prescribed was also auto-
assessed and compared with this result to understand its influence. Exploratory qualitative data
was obtained through the use of a comment box to retrieve participants’ opinions or remarks in
their own words.
Results: Significant improvement in postural awareness could be demonstrated. The Wilcoxon
signed-rank test showed ρ < 0.05. The progression of postural awareness found no correlation
with the compliance of the participants or with any of the other variables used.
Conclusion: Using PAS may be an option for the Osteopathic profession to obtain better
treatment outcomes for computer users. Its role on patients’ posture awareness and compliance
with prescribed exercises were identified as areas for future research.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
4/49
2. Introduction
2.1. Aim
The aim of this study was to assess the effectiveness of a software tool (PAS) on the computer
user’s perception of posture.
PAS reminds computer users about their posture by providing regular on-screen prompts and
displays stretching exercises that they can follow.
The lack of osteopathic literature targeted at understanding new strategies to intervene in the
management and treatment of computer users led to an increasing interest in this area.
Research Question: Can PAS increase postural awareness in computer users?
Null-hypothesis: HO1: PAS does not increase postural awareness in computer users
2.2. Background and Justification
The UK Health and Safety Executive (HSE, 2006) has identified MSDs as a priority because
they affect large numbers of people across most industries and occupations. In 2003-4 the HSE
estimated that 4.7 million working days were lost through work-related MSDs, affecting the
upper limbs or neck.
The majority of computer professionals were found to have computer-related health problems
and the incidence of MSD increased with the amount of time spent working at a computer
(Talwar et al., 2009; Klussmann, et al. 2008).
According to Edmondston, et al. (2007), more than one quarter of office computer users suffer
from neck and shoulder girdle pain. Osteopathic philosophy asserts that environmental, social,
mental and behavioural factors contribute to the aetiology of disease and illness and need to be
addressed as part of any management plan. (Chila, 2010).
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
5/49
2.3. Posture Related Problems
Work related upper limb musculoskeletal disorders (WRMULSD) can occur as a result of
spending time at the workstation in a relatively fixed posture without taking adequate breaks.
The lack of movement affects the circulatory system with the reduced blood supply allowing the
build up of metabolites, excitation of nociceptors (Larsson et al., 2007) and causing the body’s
tissues to undergo physiological changes due to their viscoelastic properties (Norkin and
Levangie, 1992). A constant stretching load on muscle fibres can cause elongation or creep in
the muscle tissue resulting in a remodelling of the fibres and a new increased length affecting
the mechanism of proprioceptive control based on muscle spindle activity (Kumar 1993; Ming,
et al. 2004). This can adversely affect muscle function causing other muscles to compensate for
the loss of function resulting in repetitive strain and overuse problems (Chaitow, 2006; Szeto, et
al. 2009).
2.4. Posture Awareness
There is no consensual definition for posture awareness. Most of the literature refers to its role
in self-consciousness, some will approach a definition based on somatic proprioception and self-
specifying information (Bermúdez, 2009).
Symptomatic subjects (postural neck pain) tend to have a different perception of what ‘good
posture’ is, compared to asymptomatic subjects according to Edmondston, et al. (2007). He
studied the clinical relevance of the perception of own posture on sitting subjects. The postural
neck pain group understood ‘good posture’ as more cervico-thoracic extension; it was discussed
that this maintained posture for long work hours would contribute to the symptoms.
The ability to maintain a previously taught posture also deteriorates with time (Kumar, 1993).
The accuracy of repositioning the spine has been found to be reduced in those with a ‘slouched’
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
6/49
posture. Posture awareness was indicated as one of the strategies to prevent injuries (Dolan and
Green, 2006).
2.5. Exercises during work
The static loading posture, characteristic of computer users requires active breaks to encourage
circulation, oxygenation, concentration, muscle stretching and a better balance of proprioceptive
activity (Wilson, 2002).
Past research has shown that the use of regular breaks and exercises can reduce the impact of
work-related upper limb musculoskeletal disorders (WRULMSD) (Monsey, et al. 2003; van den
Heuvel et al., 2003; Trujillo and Zeng, 2006; Galinsky et al., 2000; Galinsky et al., 2007). None
of the studies reported any adverse effects resulting from the addition of stretching exercises to
the participants’ daily routine. Taking regular breaks is recommended by the HSE (2006).
2.6. Software reminders
The use of computer software as a means to educate the patient and to facilitate the practitioner-
patient collaboration has been tested and put into practice for over a decade. Problem-solving
exercises, the ability to retrieve, organize and analyse the data and persuasion have been found
to be very useful factors which can lead the way for new software tools to be developed
(Skinner et al., 1993; Buchanan and Carenini, 1998; Fogg, 2003). This interaction concept is
currently under study to provide counselling and reveal changes in cognitive and affective
attitudes (Becker et al., 2010). This interaction towards physical activity was the topic of
Monsey, et al. (2003) who looked at the use of computer reminder software to prevent repetitive
strain injuries and suggested that it could have an impact on the number of stretch breaks. It was
also concluded that using software to remind computer users to take breaks contributes to
perceived recovery from MSDs (Van den Heuvel, 2003).
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
7/49
Significant reduction in symptoms in school children was found when on-screen reminders were
used as a posture education tool in a study by Robbins, et al. (2009).
By taking short breaks and occasionally stretching, workers do more accurate work and as a
result are more productive, according to a study by Lang (1999).
2.7. Compliance with exercises
Compliance is defined as the extent to which patients adopt the behaviours recommended by
their practitioners. Non-compliance has been identified as one of the factors which have a
negative impact on treatment outcomes (Bassett and Petrie, 1999).
In the field of osteopathy, concerns with compliance have been raised. Studies run by osteopaths
in Australia suggest that positive attitude, more education, more positive health, sports and
exercise experiences are more likely to increase compliance with prescribed exercises, which
increases the probability of a successful treatment outcome (Wheller, et al., 2006; Howard and
Gosling, 2008).
Compliance with treatment can be enhanced if patients understand the rationale and the
importance of their role in recovery. The use of educational and behavioural modification
methods such as treatment goals is assumed to be a probable way of improving this
understanding (Sluijs and Knibbe 1991; Bassett and Petrie, 1999) as well as understanding what
their bodies are doing and what the effects of the exercises are (Chila, 2010).
It is recommended that exercise is prescribed with accompanying written and illustrated
instructions to increase compliance (Schneiders, 1998).
Motivation and compliance seem to be directly related (Friedrich, et al. 1998), therefore more
strategies and tools are needed for osteopaths and other health professionals to achieve greater
compliance from their patients.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
8/49
3. Methodology
3.1 Study design
This study was designed to collect primary data from computer users by means of 2
questionnaires during a period of 2 weeks. This period of time was chosen based on practical
limitations and the results of studies by Fenety and Walker (2002) and McLean, et al. (2001)
which found that 10 to 14 days was sufficient time to identify musculoskeletal changes
following exercises carried out by computer users.
This is one part of a study looking at the effectiveness of PAS on computer users and it shares
the methodology and data collection with another part which will look into the effects of PAS
on reported symptoms. This is a replicable study and was given clearance to be carried out by
Oxford Brookes University Ethics committee - SH&SC REC Study no. 2009/30.
The project was structured in 3 phases (Appendix G):
1 – Develop the PAS and documentation.
2 – Run a pilot study to assess the software and procedures.
3 – Run this study, collect the data and analyse it.
Phase 1 – The development of the Postural Awareness Software, information sheet, installation
information, consent form and supporting questionnaires.
a) Documented and tested the exercises that were incorporated into the PAS.
b) Designed an information sheet outlining the study.
c) Tested the software in different operating system environments.
d) Designed the questionnaires to meet our research questions and a few exploratory
questions.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
9/49
e) Produced a participant pack including an installation CD for the PAS and user
installation instruction sheet.
Phase 2 – The pilot study included user acceptance testing (UAT) of the software and a
questionnaire to highlight any problems.
a) Recruited participants for UAT which ran for 2 weeks. This involved a small number of
friends and colleagues with the main aim of obtaining feedback prior to producing a
final version of the software.
b) Logged and document any problems identified during the pilot.
c) Created a final version for the participant pack.
Phase 3 – Recruited volunteers, issued PAS package and collection of data.
a) Recruited participants that met the inclusion criteria for the study.
b) Carried out a short presentation of the PAS to familiarise the participant with the
software, demonstrated how to safely perform the exercises and then obtained their
written consent before issuing the PAS package.
c) Asked participants to fill in the first part of the questionnaire (Sections 1 and 2).
d) At the end of the trial period the participants were sent their participant codes by email
and asked to complete the on-line part of the questionnaire (Sections 3 & 4), including
feedback on the study itself.
e) Retrieved and analysed the data using Microsoft Excel for general demographics and
correlations and PRISM for the Wilcoxon signed-rank test.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
10/49
3.2 Software design
The PAS provides an on-screen prompt illustrating an exercise, instructions on how to execute it
and an option to change the time period between prompts.
It was written by the author of this study and compiled in Microsoft Visual Basic 6.0. The
software was originally designed for personal use, with a broader view that it could be a valid
tool to osteopaths or other health care professionals.
The software was designed and tested on Windows compatible machines running on 32 or 64-
bit versions of XP, Vista or 7 versions.
Fig 1. Screen-shot of PAS displaying a message with an exercise description and its corresponding image.
3.3 Questionnaire design
The questionnaire was based on one used by Mulligan (2009) and included demographics
questions, questions relating to the direct aim of the research and 3 more questions for
exploratory purposes. In all questions a comment box was added to retrieve participants’
opinions or remarks in their own words.
In order to quantify posture awareness, the reference used was a study by Garmer, et al. (2002).
A questionnaire using a simple subject rating scale (1-10) was used to validate the hand-strength
kit through the perceived awareness of strength. Kumar (1993) states that self-assessment and
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
11/49
reporting of posture can be found to be a reliable and valid technique to quantify posture
awareness.
Subjective posture awareness was compared before and after using PAS, retrospectively by
means of 2 5-point Likert scale questions (Questions 17 and 18 – Appendix E). The reason for
this was that any questions about posture and postural awareness asked before the use of PAS
would immediately make the participant more aware of their posture and could create
expectations which could potentially affect the outcome of the study.
Compliance could not be asked retrospectively or compared before and after the intervention, so
it was decided to ask the same question in 2 different formats (Questions 15 and 16 – Appendix
E), as 5-point Likert scale or percentage of use questions. The 5-point Likert scale method was
previously used by Howard and Gosling (2008) and the percentage one by Schneiders. et al,
(1998). Ideally the software would have been designed to retrieve user compliance data, but that
was not possible.
All the questions were validated by the pilot study and were designed according to the Oxford
Brookes University Ethical standards for research involving human participant’s code of
practice.
The decision to use a questionnaire was based on its growing use to assess the health of
individuals following a medical or psychosocial intervention. Classically more often employed
in clinical trials, they can be used to monitor individual patients with a clinical setting. Patient-
reported measures are increasingly being used in routine evaluation of health care (Neale,
2009).
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
12/49
3.4 Recruitment
Participants were recruited from Oxford Brookes University and Mill Court Clinic using leaflets
and posters. Sampling followed a mixed method using incidental sampling (through requests to
colleagues), volunteer sampling (based on people responding to the leaflet) and snowball
sampling (where key individuals were identified and asked to distribute the information sheet to
people who meet the criteria of the sample).
There was no payment or incentive for participation in the study and no feedback was given to
patients regarding their participation.
Potential participants that contacted the researchers were given a short presentation, with the
following steps:
• Presentation of the study and what would be required from the participant (Appendix A)
• Demonstration of how to perform the exercises (Appendix B) and make sure participant
can perform them safely and efficiently.
• Asked to sign the consent (Appendix F)
• Asked to fill in the questionnaire part 1 (Appendix D)
Once this was completed they were given the participant pack and an exercise hand-out. In
addition they were given the start and end dates for their involvement in the study.
3.5. Subjects
There were no exclusions based on ethnic group, religion or gender, with the aim of recruiting
computer using participants of all ages and from all occupations.
The target sample size was 75 participants with an estimated final sample size of 45 assuming
there was a 40% drop out rate as found in a similar study by Mulligan (2009).
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
13/49
Table 1- Inclusion / Exclusion Criteria
As an exploratory study, it was decided to keep open as many variables as possible so that any
tendencies emerging from the data could be interpreted and potentially better designed studies
could be created. No power calculations were performed.
3.6. Documents Used
These are the formats of the documents used during the study:
• Participant Information Sheet (both A4 and leaflet formats)
• Handout of the exercises (A4 format)
• PAS Installation Instructions (portable document format (PDF) and A4 formats)
• Initial Questionnaire (A4 format)
• Final Questionnaire (on-line – surveymonkey.com)
• Consent Form (A4 format)
• GANTT Project Plan (Excel spreadsheet)
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
14/49
4. Results
Although in this study a more quantitative approach to the data retrieved was used, participants
were encouraged to provide comments and additional feedback. Not many took that
opportunity, but some of those comments were taken into account in the discussion part of this
paper. Out of a total of 50 participants recruited, 41 finished the study; the drop out rate was
18% - the reasons for the drop out were not asked or given. Data has been cleaned and
anonymised prior to its analysis in Microsoft Excel and PRISM Software.
4.1. General Demographics
Table 2 - General demographics and type of computer use
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
15/49
4.2. Posture Awareness Data
In order to obtain a general overview of the posture awareness responses, we compared the
results before and after the intervention. This visual distribution illustrates a quite marked
difference in self-assessment of postural awareness after the use of PAS (chart 1 and 2).
Chart 1 - Postural Awareness, by scale, before and after usage of PAS.
Chart 2 - Postural Awareness, by participant, before and after usage of PAS
The visual analysis shows a clear quantitative difference after the use of PAS, but in order to
understand if the differences between the answers can be attributed to the intervention or
whether they could have occurred by chance alone, the non-parametric Wilcoxon signed-rank
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
16/49
test (non-Gaussian population for 2 paired groups) was performed, using PRISM Software, with
a significance level of ρ < 0.05 (Fisher and Foreit, 2002) and two-tailed ρ value. The result was
ρ = 0.0028 with pairing significantly effective (before and after measurement vary together)
proving the null-hypothesis wrong.
4.3. Exploratory Data
Chart 3 - Time frame used between reminders (Question 14 in appendix E)
This chart show a clear predominance of shorter breaks between the on-screen reminders, the
majority preferring 60 minutes.
Chart 4 – Percentage compliance with the PAS exercises (Question 15 in Appendix E)
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
17/49
Chart 5 – Compliance with the PAS exercises (Question 16 in Appendix E)
In order to understand if the compliance had an influence on the postural awareness results, we
compared its progression with the compliance results. The compliance questions were compared
and screened for possible discrepancies (chart 4 and 5).
It was concluded by a visual analysis that the participants’ perception of compliance in terms of
the percentage of times they did the exercises and their subjective assessment of compliance are
highly related. 51% of the participants showed a good compliance with the use of PAS.
Progression of awareness was then compared with compliance (difference between results of
questions 17 and 18 and question 16 in Appendix E) (Chart 6).
Chart 6 - Relation between compliance and prescribed exercises
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
18/49
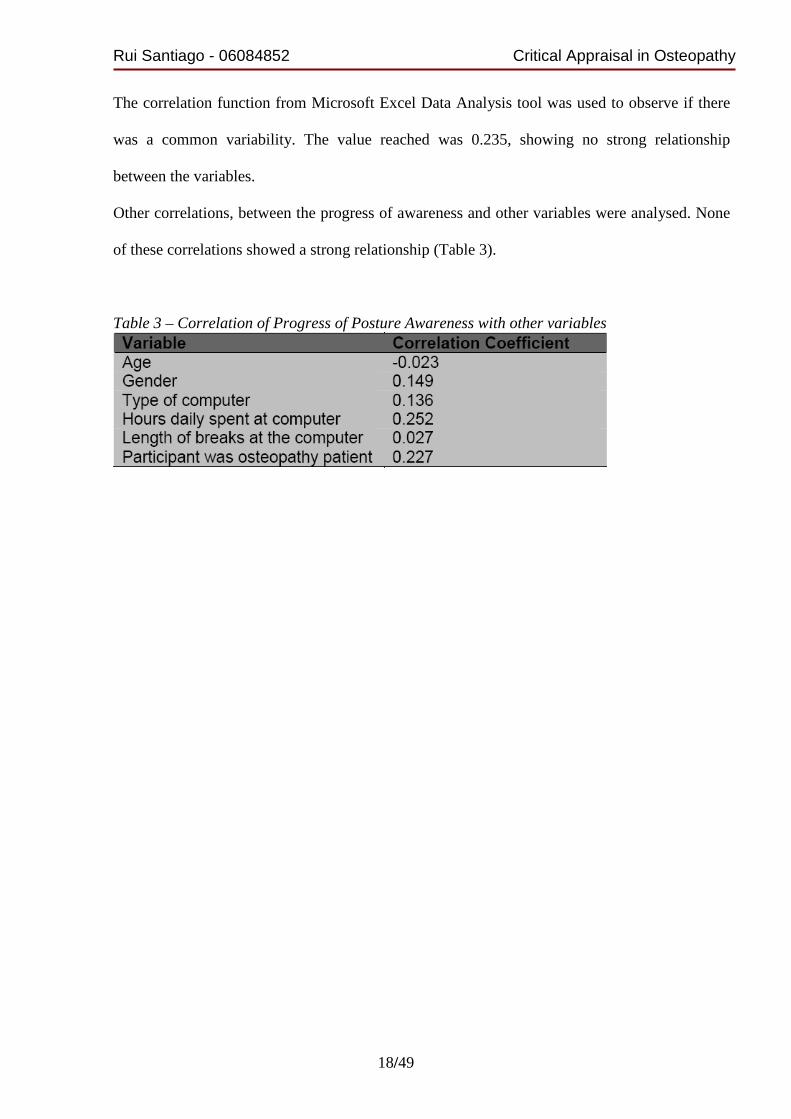
The correlation function from Microsoft Excel Data Analysis tool was used to observe if there
was a common variability. The value reached was 0.235, showing no strong relationship
between the variables.
Other correlations, between the progress of awareness and other variables were analysed. None
of these correlations showed a strong relationship (Table 3).
Table 3 – Correlation of Progress of Posture Awareness with other variables
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
19/49
5. Discussion
This study showed a significant increase in the reported awareness of posture among computer
users after the use of PAS for 2 weeks.
5.1. Relationship between awareness and symptoms
In the other part of this study, which shares the same methodology and looked at symptoms, it
was found that after the use of the PAS, there were more reported symptoms in some areas of
the body and less in others. This is not a complete surprise. Coury (1998) found that, in a study
of sedentary workers following a self-administered preventive programme concentrating on
their perception of any MSD, the participants reported more symptoms. The likelihood that this
was due to an increased awareness was discussed. On the other hand, when used on children,
there was a significant reduction of MSD symptoms reported (Robbins et al., 2009). The fact
that postural awareness may increase symptom awareness in adults is a new field to be studied.
5.2. Exploratory Questions
Some questions were designed to retrieve data which could help in formulating future research
questions.
Postural Awareness
All the variables compared with the progression of awareness through the correlation function
showed very low relationships. Correlation was higher in participants who spent more hours in
front of a computer or were osteopathy patients. In future studies, narrowing of these variables
may help to attain a clearer picture of which variables influence subjective postural awareness.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
20/49
Compliance with exercise prescription
A correlation between the participants compliance and the progression of awareness, was not
found (chart 6), showing that compliance might not have an influence on the postural awareness
outcome. The present workload of the participants was the most commented dissuasive factor
for their full compliance with the software.
Exercise breaks at work
Work breaks could be used in a way to promote health by means of exercise; it is an opportunity
yet untapped to reduce unhealthy behaviours and promote healthy ones (Wendell, 2005). A
systematic review by Brewer, et al. (2006) of the effect of office interventions on
musculoskeletal and visual health concluded that rest breaks combined with exercise had no
effect. This contrasts with studies by Henning, et al. (1997), Fenety and Walker (2002),
Saltzman (2002) and Lacaze, et al. (2010) which found that regular rest breaks and exercise
could reduce musculoskeletal discomfort. It is worth noting that the Brewer review found that
the “evidence was insufficient” to draw conclusions about the benefits of rest breaks and
exercise training rather than stating that the interventions were ineffective. 61% of the
participants in this study, take breaks every 1-2 hours. PAS may have the potential to help
introducing more exercise breaks during work.
Length of break
Analysis of the used time frame (chart 3) showed that most participants opted for 60 minutes.
This was the value by default presented by the software; therefore it is not conclusive if it was
always adjusted to personal needs.
Taking short breaks for at least every hour was highlighted (Ming et al., 2004) as one of the
methods of preventing development of WRMULSD.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
21/49
Continuous computer user discomfort can be moderated by short rest breaks at 10 to 15 minutes
intervals for a period of 20 seconds and by continuous feedback about rest break behaviour with
untoward effects on performance, well-being or acceptance (Henning et al., 1996; Henning et
al., 1997).
Qualitative data
It showed very distinct user types revealing various difficulties, mostly concerning work load,
tiredness and work station set-up preventing some exercises.
Compliance with the exercises seemed to be greater after long periods in front of the computer
when compared with short ones.
Other comments acknowledged how surprised some participants were with their own posture
when the reminder was presented, some even changed the prescribed exercises to others that
worked better for them and used the reminder to do them, to just relax or as an opportunity to
get up and walk around.
As participants spent more time thinking about their posture and the exercises they raised
concerns about ergonomic factors.
Another observation was that more time using the software might be needed to feel the benefits
to their postures.
5.3. Study limitations
These are the most relevant methodological limitations found in this study:
Control group
This approach was considered not viable for an undergraduate level project.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
22/49
The use of a control group should however be considered as a requirement for any future
studies, as it would reduce the risk of bias.
Blindness
Ideally, double blindness would have been used in this study, but the absence of a control group
and the limited resources available made it not viable. It would have required that both the
investigators and the participants were unaware of the group to which the patient was assigned
to prevent being influenced by that knowledge.
It is particularly important to decrease the chance of bias in a study when the outcomes are
subjective, as in this case (Neale, 2009).
Sample size
The sample size of 50 participants was considered appropriate for this study, nevertheless it is
very small. Future studies should aim to a much bigger sample size, if possible from different
geographic and cultural areas. When targeting a specific population and intervention, sample
size should be calculated.
Participants who were patients
Some participants were receiving osteopathic treatment (39%), which could influence the results
and reduce the chance that the intervention alone was causing the results.
As an exploratory variable, a correlation was not found between the postural awareness
progression and the fact that those participants were patients.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
23/49
Subjectivity
The information obtained from this study is completely dependent on the subjectivity of the
participants’ responses, therefore more objective means of evaluating patients postural
awareness would have to be considered and introduced.
Computer user profile
Although not explicit in the questionnaire, some participants chose both options for the type of
computer used. Another volunteered the option of using a laptop with desktop set-up. These are
variables that need to be considered in further studies.
5.4. Clinical implications
From the qualitative data and the recruitment experience, the enthusiasm of the participants for
using PAS was clear. Clinically, it would work as an extra tool available to the osteopath to
address computer use as a maintaining factor.
PAS seems to have a good effect on patients’ compliance with exercises or advice given by the
clinician, opening doors to a treatment outside the treatment room paradigm.
It can be used preventively, as discussed before, through increased awareness, or by earlier
interpretation of symptoms, preventing more severe conditions.
The idea is that it would be free to the patient and it would include general exercises / advice to
the computer user or tailored to patient specific complaints / biomechanical factors / work type /
work station limitations / periodic work load increase.
Following participation, when asked if they kept using PAS, out of a total of 39 answers, 69%
declared that they are still using it and some even passed it on to family, friends and work
colleagues.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
24/49
5.5. Suggestions for future research
Future studies, using this technology (with the necessary alterations) should consider the
following:
• Can PAS increase compliance with postural advice in asymptomatic computer users?
• Can PAS increase compliance with prescribed exercises in asymptomatic computer
users?
• Study the effectiveness of stretches and exercises commonly prescribed by Osteopaths to
computer users.
• Comparative study of optimal length of breaks for the computer user.
• Study of the optimal PAS use time to increase the awareness of posture.
For the reasons presented above, having a tool which may involve, help and motivate the patient
in their own recovery, is present during the work time and makes the patient also responsible for
their improvement could be a tool for osteopaths.
This study may represent the start of a process of validation of PAS as a therapeutic tool for
osteopaths or other health care professions. There are several commercial packages available for
office workers, but none as a tool that osteopathy or other health care professions could use to
adapt to the patient’s specific needs.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
25/49
6. Conclusion
Posture associated problems are a very common precursor to WRMULSD in computer users.
This was the first study looking at postural awareness, completely developed and conducted by
osteopathy students and using exercises commonly prescribed in an osteopathic clinic.
It was concluded that software reminders with exercises can be a useful tool for osteopaths to
use in a clinical setting, involving the patients in their treatment and management. The scope of
the study focused mostly on the awareness of posture, but the potential for more studies with
this type of population, using this technology appears to be considerable and should be
explored.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
26/49
7. Acknowledgements
I would like to thank my supervisor, Philip von Hauenschild, for his advice and support
throughout this study and for agreeing to be our supervisor when, at a critical time, we were left
without one.
I would also like to thank Dona Williams for her precious help at Mill Court Clinic, setting up
the interviews.
Many thanks to the participants, who gave their time generously; this study would not have been
possible without them.
Also, my thanks to the Brookes University ethics committee team, for their guidance during the
approval of the ethics application for this study.
Finally to my friend and colleague Bob Allen, for all his patience and perseverance during all
the difficulties and the busier moments designing and running this study.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
27/49
8. References
. Bassett S. F. and Petrie J. K. J. (1999). The Effect of Treatment Goals on Patient Compliance
with Physiotherapy Exercise Programmes. Physiotherapy 85(3), pp.130-137.
. Becker A., Herzberg D., Marsden N., Thomanek S., Jung H., Leonhardt C. (2010). A new
computer-based counselling system for the promotion of physical activity in patients with
chronic diseases - Results from a pilot study. Patient Educ Couns,
doi:10.1016/j.pec.2010.05.024.
. Bermúdez, J. L. (2009). Self: Body awareness and Self-awareness. Encyclopaedia of
Consciousness ,pp.289-300.
. Brewer S., Eerd D., Amick B. C. III, Irvin E., Daum K., Gerr F., Moore J., Cullen K. &
Rempel D. (2006). Workplace interventions to prevent musculoskeletal and visual symptoms
and disorders among computer users: A systematic review. Journal of Occupational
Rehabilitation.16, pp.317-350.
. Buchanan B. G. and Carenini G. (1998). Designing computer-based frameworks that
facilitate doctor–patient collaboration. Artificial Intelligence in Medicine. 12,pp.169-191.
. Chaitow L. (2006). Muscle Energy Techniques. 3rd ed. London: Elsevier, Churchill-
Livingstone.
. Chila A. G. (2010). Foundations of Osteopathic Medicine. 3rd ed. Philadephia: Lippincott
Williams & Wilkins.
. Coury H .J. C. G. (1998). Self-administered preventive programme for sedentary workers:
reducing musculoskeletal symptoms or increasing awareness? Applied Ergonomics.
29(6),pp.415-421.
. Dolan K. J. and Green A. (2006). Lumbar spine reposition sense: The effect of a ‘slouched’
posture. Manual Therapy. 11,pp.202–207.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
28/49
. Edmondston S. J., Chan H. Y., Ngai G. C. W., Warren M. L. R., Williams J. M., Glennon S.
and Netto K. (2007) Postural neck pain: An investigation of habitual sitting posture, perception
of ‘good’ posture and cervicothoracic kinaesthesia. Manual Therapy. 12,pp.363–371.
. Fenety A. & Walker J. (2002). Short-term effects of workstation exercises on musculoskeletal
discomfort and postural changes in seated video display unit workers, Physical Therapy.
82(6),pp.578–589.
. Fisher A. and Foreit J. (2002). Designing HIV/AIDS Intervention Studies: An
Operations Research Handbook. Washington, DC: Population Council
. Fogg B. J. (2003). Persuasive Technology - Using Computers to Change What We Think and
Do. California: Elsevier – Morgan Kaufmann.
. Friedrich M., Gittler G., Halberstadt Y., Cermak T. and Heiller I. (1998). Combined exercise
and Motivation program: Effect on the compliance and level of disability of patients with
chronic back pain: A romdomized controllled trial. Arch Phys Med Rehabil. 79,pp.475-87.
. Health and Safety Executive (2006). Working with VDUs [Online]. Available at:
http://www.hse.gov.uk/msd/dse/ (Assessed: 20 April 2010).
. Henning R., Jacques P., Kissel G., Sullivan A. and Alter S. (1997). Frequent short rest breaks
from computer work: Effects on productivity and well-being at two field sites, Ergonomics.
40,pp.78–91.
. Henning R., Callagham E., Ortega A., Kissel G., Guttman J. and Braun H. (1996).
Continuous feedback to promote self-management of rest breaks during computer use,
international Journal of industrial Ergonomics. 18(1),pp.71–82.
. Howard D. B. and Gosling C. M. C. (2008). A short questionnaire to identify patient
characteristics indicating improved compliance to exercise rehabilitation
programs: A pilot investigation. International Journal of Osteopathic Medicine. 11,pp.7-15.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
29/49
. Galinsky T.L., Swanson N.G., Sauter S.L., Hurrell J.J. and Schleifer L.M. (2000). A filed
study of supplementary rest breaks for data entry operators. Ergonomics. 43(5),pp.622-38.
. Galinsky T.L., Swanson N.G., Sauter S.L., Dunkin R., Hurrell J.J. and Schleifer L.M. (2007).
Supplementary breaks and stretching exercises for data entry operators: a follow-up field study.
Am J Ind Med. 50(7),pp.519-27.
. Garmer K., Sperling L. and Forsberg A. (2002). A hand-ergonomics training kit: development
and evaluation of a package to support improved awareness and critical thinking. Applied
Ergonomics. 33,pp.39–49.
. Kumar S. (1993). Perception of posture of short duration in the spatial and temporal domains.
Applied Ergonomics. 24(5),pp.345-350.
. Lacaze D.H., Sacco ide C., Rocha L.E., Pereira C.A. and Casarotto R.A. (2010). Stretching
and joint mobility exercises reduce call-center operators’ musculoskeletal discomfort and
fatigue. Clinics. 65(7),pp.657-62.
. Lang S. S. (1999). When workers heed computer's reminder to take a break, their productivity
jumps - Cornell study finds [Online]. Available at: www.rsiguard.com/cornell.htm/ (Assessed:
02 February 2011).
. Larsson B., Søgaard K. and Rosendal L. (2007). Work related neck-shoulder pain; a review on
magnitude, risk factors, biochemical characteristics, clinical picture and preventive
interventions. Best Practice in Clinical Rheumatology. 21,pp.447-464.
. Levangie P. and Norkin C. (2005). Joint Structure & Function: A comprehensive analysis. 4th
ed. Philadelphia: F. A. Davis Company.
. McLean L Tingley M, Scott R and Rickards J (2001). Computer terminal work and the benefit
of microbreaks. Applied Ergonomics. 32,pp.225-237.
. Ming Z., Narhi m. and Siivola J. (2004). Neck and Shoulder Pain due to computer use.
Pathophisiology. 11,pp.51-56.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
30/49
. Monsey M., Ioffe I., Beatini A., Lukey B., Santiago A. and James A. (2003). Increasing
compliance with stretch breaks in computer users through reminder software. Work.
21(2),pp.107-11.
. Mulligan J. (2009). Does Attitude affect risk. Master Thesis. University college London.
. Neale J. (2009). Research Methods for health and social care. New York: Palgrave Macmillan
. Oxford Brookes University Ethical standards for research involving human participants -
Code of practice. [Online]. Available at:
http://www.brookes.ac.uk/res/policy/ethics_codeofpractice.pdf (Assessed: 10 March 2010).
. Robbins M., Johnson I. P. and Cunliffe C. (2009). Encouraging good posture in school
children using computers. Clinical Chiropractic. 12,pp.35-44.
. Saltzman A. (1998). Computer user perception of the effectiveness of exercise mini-breaks
[Online]. Available at: http://www.paratec.com/research.htm/ (Assessed: 25 April 2010).
. Schneiders A. G., Zusman M. and Singer K. E. (1998). Exercise therapy compliance in acute
low back pain patients. Manual Therapy. 3(3),pp.147-152.
. Sluijs E. M. and Knibbe J. J. (1991). Patient compliance with exercise: different theoretical
approches to short-term and long-term compliance. Patient education and counselling.
17,pp.191-204.
. Skinner C. S., Siegfried J. C., Kegler M. C. and Strecher V. J. (1993). The potential of
computers in patient education. Patient Education and Counseling. 22,pp.27-34.
. Szeto G. P. Y., Straker L. M., and O’Sullivan P. B. (2009). Neck-shoulder muscle activity in
general and task-specific resting postures of symptomatic computer users with chronic neck
pain. Manual therapy. 14,pp.338-345.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
31/49
. Trujillo L. & Zeng X. (2006). Data entry workers perceptions and satisfaction response to the
"stop and stretch" software program. Work.27(2),pp.111-21.
. van den Heuvel S., de Looze M., Hildebrandt V., Thé K. (2003). Effects of software programs
stimulating regular breaks and exercises on work-related neck and upper-limb disorders. Scand
J Work Environ Health. 29(2),pp.106-16.
. Wendell C. (2005). Transforming work breaks to Promote Health. American Journal of
Preventive Medicine. 29(5),pp.461-465
. Wilson A. (2002). Effective management of musculoskeletal injury. London: Churchill
Livingstone.
. Wheller R., Gosling C. and Herman N. (2006). Patient compliance to exercise prescription at
the Victoria University Osteopathic Medicine Clinic. International Journal of Osteopathic
Medicine. 9,pp.27-46.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
32/49
Appendix A – Participant Information Sheet
Information Sheet
Title: A study of Postural Awareness and the incidence of musculoskeletal disorders in computer users. Student investigators: Rui Santiago & Bob Allen Research Supervisor: Philip Von Hauenschild Academic institution: Oxford Brookes University Date: 14th September, 2010 You are being invited to take part in a research project. Here is some information to help you decide whether to do so. Please take the time to read this information carefully and discuss it with friends or relatives if you wish. If there is anything you do not understand, or if you would like more information, please do not hesitate to contact us. What is the purpose of the study? The UK Health and Safety Executive (HSE) have identified musculoskeletal disorders (MSD) as a priority because they affect large numbers of people across most industries and occupations and more importantly it is possible to prevent or minimise their effects. A number of approaches have been used to reduce the incidence of work-related upper limb musculoskeletal disorders (WRULMSD) including the use of shoulder exercises, real-time visual feedback to improve posture and neural stretching of the upper limbs. The postural awareness software (PAS), that has been developed for this study, will provide regular on-screen prompts to remind the computer user to check their posture and it will display stretching exercises that will help to reduce any muscular tension. The study aims to consider:
• Whether Postural Awareness Software (PAS) can have an effect on the self-awareness of posture in computer users?
• Is compliance with prescribed exercises affected by the use of PAS? • Can the use of PAS reduce the severity of WRULMSD in computer users?
This study will indicate whether PAS is a valid tool for increasing postural awareness in computer users and whether it can affect the incidence of WRULMSD.
Why have I been invited to participate? We are looking for participants who currently use a computer on a daily basis and would be prepared to take part in our study. The PAS needs to be installed on a computer running a 32 or 64 bit, Windows-based operating system i.e XP, Vista or Windows 7.
Do I have to take part? The decision to participate in this study is entirely voluntary. You will be asked to sign a consent form, however, as a volunteer you can opt out at any time without having to give a reason.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
33/49
What would happen to me if I take part? Anyone agreeing to take part in the study will be invited to attend a one-to-one meeting, either in Mill court Osteopathic Clinic or the School of Health and Social Care at Oxford Brookes University. The meeting, will not last more than 20 minutes, where you will be given a brief overview of the study together with an:
• explanation and demonstration of good posture with some exercises at the computer and a printed copy for you to take away.
• information pack containing a CD ROM of the PAS and installation instructions.
If you are happy with the information provided and wish to take part in the study you will be asked to sign a consent form and then to complete Part 1 of the questionnaire (Sections 1 & 2).
The study will last 2 weeks beginning with the installation of the software. After that period, you will be asked to complete Part 2 (Sections 3 & 4) of the questionnaire which will be on-line (we will email you a link allowing access after 2 weeks of software use).
What happens at the end of the study? After the completion of Part 2 of the questionnaire, your participation ends. You will have the option to keep the software at no charge or you can easily remove it from your computer (details on uninstalling the software are included in the installation instructions handout). We will still be available to be contacted if you have any questions and we will welcome your feedback about the study.
What are the possible benefits of taking part? The use of the PAS is to encourage you to maintain good posture and to take regular rest breaks with exercise, during computer use. Your participation in this study will also contribute to additional knowledge in this field. Risks and potential discomfort To minimise the possibility of any discomfort during the study the initial meeting will be used as an opportunity to ensure participants can carry out the exercises safely and correctly. The PAS has been thoroughly tested for safety both to the user and their computer. Would my taking part in the study be kept confident ial? All data will be collected and stored in accordance with the Data Protection Act 1998 and it will not be possible to identify any participant from any publication. The data will be held in a secure password-protected environment and will only be accessible to the students. Who has approved the study? Oxford Brookes University SH&SC Research Ethics Committee has reviewed the study – Project number: 2009/30. Please note that if you have any concerns about the conduct of this research project you can contact the Chair of the SH&SC Research Ethics Committee at Oxford Brookes University at the following email address: [email protected]
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
34/49
What will happen to the results of the research stu dy? The results of the study will be used for the dissertation project of the 2 students and may also be published in a related journal. Participants can contact the students directly if they would like a copy of the results. Who can I contact if I have any further questions? Research Students Rui Santiago
Project supervisor Philip Von Hauenschild Associate Lecturer in Osteopathy at Oxford Brookes University Telephone: 07590283720 Email [email protected]
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
35/49
Appendix B – Exercises Handout
Exercises
The following exercises are provided as a printed reference covering the exercises that are included in the Postural Advice Software.
Very Important: Please note that you may feel a small degree of discomfort while performing these exercises as they will be stretching and moving muscles that are not used to this type of movement. However, if at any point you experience any pain then stop and note which exercise caused the discomfort. When you have the opportunity please contact one of the researchers who will be able to provide you with relevant information regarding what caused the discomfort and will advise you on what can be done to avoid it happening again.
Back
• Move one arm at time, in all directions for 10 seconds. • Then, hold at the end of each movement for 10 seconds. • Move your arms in opposite directions i.e. one arm up and the other
arm down and hold for 10 seconds. Change arms and repeat.
Shoulders
• Roll your shoulders slowly to the front and then to the back. • Draw both shoulders back for 10 seconds and then forward for
another 10 seconds. • Link your fingers behind your neck, bring elbows together and slowly
make a figure of 8. Do this 10 times in one direction then the other.
Hands and Wrists
• Put your palms together, elbows pointing to the sides, push together gently for 10 seconds.
• Repeat with the backs of your hands together. • With your arms in front of your body open and close your fingers 10
times. • Interlock your fingers, keep wrists and forearms together, and make
circles with your wrists.
Shoulders and Back
• Place your hands on your waist with your thumbs to the back, then move your elbows back, for a stretch in your shoulders. Hold for 10 seconds
• Change your hand position so that thumbs are to the front and do it with the elbows to the front. Hold for 10 seconds
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
36/49
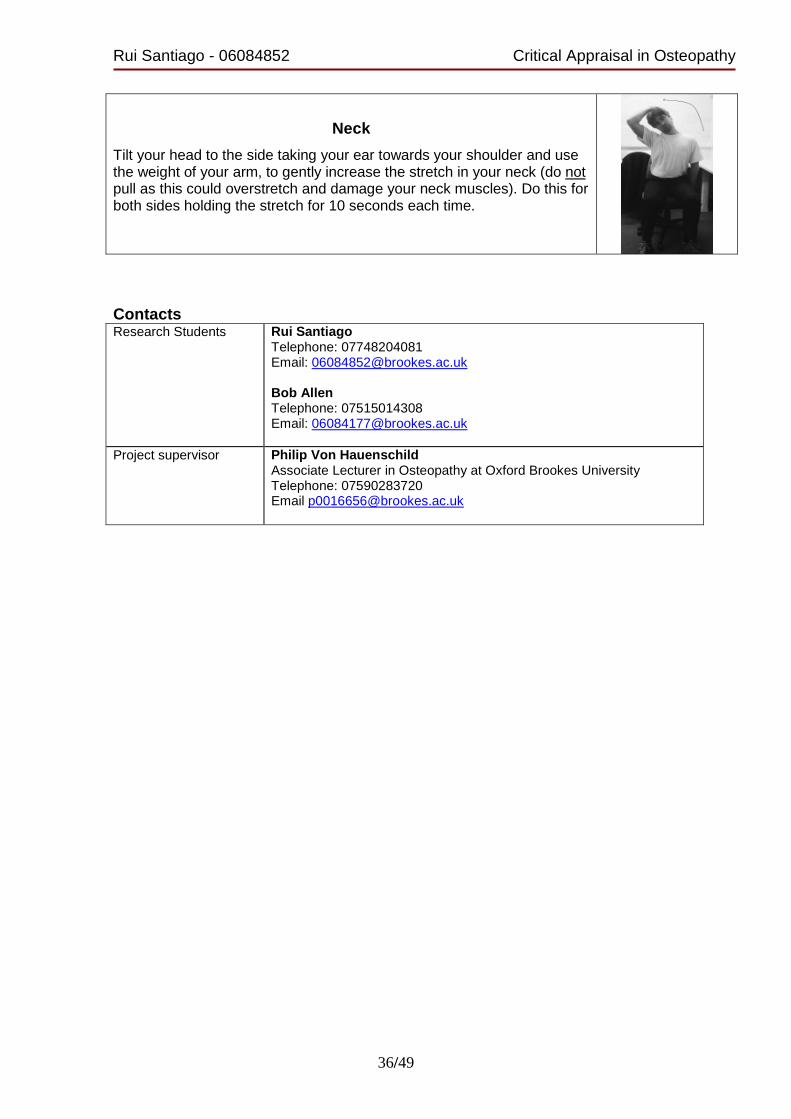
Neck
Tilt your head to the side taking your ear towards your shoulder and use the weight of your arm, to gently increase the stretch in your neck (do not pull as this could overstretch and damage your neck muscles). Do this for both sides holding the stretch for 10 seconds each time.
Project supervisor Philip Von Hauenschild Associate Lecturer in Osteopathy at Oxford Brookes University Telephone: 07590283720 Email [email protected]
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
37/49
Appendix C – PAS installation instructions
Introduction The Postural Awareness Software (PAS) used in this study was created to support the maintenance of good posture while using a computer and to provide stretching/ strengthening exercises to help reduce the incidence of work-related upper limb musculoskeletal disorders (WRULMSD). Once installed the software will provide the computer user with regular reminders to check that they are maintaining ‘good posture’ (refer to the information sheet for more details on what a good posture is). The computer user will also be given exercises to help relieve any existing muscular aches and pains and to reduce the incidence of any new problems. Technical Requirments Installation The PAS can run on Windows based machines running 32 or 64-bit versions of either XP, Vista or Windows 7. To install the software please find the file ‘setup.exe’ inside the PAS V3.2 folder in the CD-ROM. Click twice on the file and the installation should start immediately. If there is any difficulty or problems concerning the installation please contact one of the research students. Running PAS for the first time After the software is initially installed, the user should go to Startup -> Programs -> PAS and click on the face icon. You will only need to do this once then the program will load automatically each time you restart your computer. The PAS dialog box will be shown immediately, allowing you to set the time between reminder messages from the default period of 20 minutes up to a maximum of 120 minutes. Once you have selected the time interval that you want please click on the Update button to save the changes, if you don’t click the Update button it will run on the previously selected interval. Using PAS The PAS is set to auto-run which means that it will automatically be running in the background each time you start your computer. The dialog box will be shown after the time period that you selected previously and when you have reviewed your posture and completed the exercise click on the OK button. The next exercise will appear after the pre-set time period. Uninstalling PAS To disable this software you need to start the Windows Task Manager using the keys [ctrl+alt+del] and on the Applications tab, choose PAS and click the ‘Stop Task’ button.
Fig 1. Screen-shot of the PAS software. Displaying a message with postural advice and an exercise description with its corresponding image.
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
38/49
In the Windows Control Panel, accessible from the Start button, choose ‘Add/Remove’ programs. A list of programs will be shown, choose PAS and click ‘Change/Remove’ and the software will be uninstalled. Final Note Although the PAS has been thoroughly tested for compatibility with the Windows operating system if you have any concerns related to the running of the software, please contact one of the research students who will be happy to help. Contacts Research Students Rui Santiago
Project supervisor Philip Von Hauenschild Associate Lecturer in Osteopathy at Oxford Brookes University Telephone: 07590283720 Email [email protected]
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
39/49
Appendix D – Initial Questionnaire
Please note that Sections 1-2 of this questionnaire should be completed at the start of the study prior to instal ling and using the Postural Awareness Software. If you have any questions or need any additional in formation regarding this request please do not hesitate to co ntact us.
----------------------------//---------------------------- SECTION 1: General This section asks about you, your job and your comp uter use. � If you are completing the questionnaire by hand, please circle your response(s) � Where a COMMENT space is provided please add any additional information which you feel may be relevant or which allows you to explain your response more fully. 1. Name: ___________________________________
3. Gender a) Female b) Male 4. Age a) 18-20 b) 21-30 c) 31-40 d) 41-50 e) 51-60 f) 61-65 g) Over 65 5. What type of computer do you use? a) Desktop computer b) Laptop computer (Notebook, Netbook etc.) 6. How long do you spend at your work computer duri ng a typical day? a) Less than one hour b) Between one and three hours c) Between three and six hours d) Between six and eight hours e) More than eight hours 7. What might be the longest time you spend working at your computer before taking a break, e.g. short break away from the computer fo r telephone calls, paperwork, filing, photocopying, comfort break?
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
40/49
a) Less than one hour b) Between one and two hours c) Between two and three hours d) Three hours or more COMMENT: 8. Do you have any upper body symptoms which you at tribute to or which you believe may be aggravated by computer use in the la st 6 months? (For the purpose of this study symptoms refers to upper body related problems which might include: headaches, eyestrain, muscle aches, joint pain, pins and needles etc.) a) Yes b) No c) Prefer not to answer If you answered (b) “No” or (c) “Prefer not to answ er” to Question 8 you have now completed Part1 of the survey. A link to allow completion of Part2 of the survey w ill be emailed to you 2 weeks after installation and use of the PAS s oftware. Thank you for your time. SECTION 2: Symptoms This section asks about any symptoms that you belie ve may have been caused or aggravated by computer use.
9. Which of the following statements describe(s) yo ur symptoms. …. (Please select all that apply) a) Chronic (the discomfort/ pain is long-lasting, recurrent in nature) b) Acute (the discomfort/ pain started recently, rapid onset, short-lasting) c) Severe (the discomfort/ pain is intense, debilitating) d) The discomfort/ pain is episodic (triggered by certain activities, postures, types of work, amount of work) e) The discomfort/ pain generally wears off overnight or across a weekend f) The discomfort/ pain wears off only with rest, e.g. when on a holiday g) The discomfort/ pain is permanent: may change in intensity, but does not wear off 10. Please indicate which area(s) bother you (Please select all that apply) a) Head (e.g. headache, migraine) b) Eyes (e.g. hot, sore, tired, stinging, dry, weeping eyes; eyestrain)
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
41/49
c) Neck d) Shoulder(s) e) Middle of back f) Lower back g) Upper arm(s) h) Forearm(s) i) Wrist(s) j) Hand/ Finger(s) 11. Please indicate which area bothers you the MOST (Please select just ONE) a) Head (e.g. headache, migraine) b) Eyes (e.g. hot, sore, tired, stinging, dry, weeping eyes; eyestrain) c) Neck d) Shoulder(s) e) Middle of back f) Lower back g) Upper arm(s) h) Forearm(s) i) Wrist(s) j) Hand/ Finger(s) k) Other…. Please explain: 12. For the area which bothers you MOST, which of the following describe(s) your symptoms (Please select all that apply): a) Dull ache b) Burning c) Cramping/ tight muscles d) General discomfort e) Numbness/ loss of feeling f) Sharp pain g) Joint stiffness h) Swelling i) Tingling/ pins and needles j) Muscle weakness k) Other…. Please explain:
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
42/49
YOU HAVE REACHED THE END OF PART 1 OF THE QUESTIONN AIRE.
THANK YOU VERY MUCH FOR YOUR TIME
If you have any questions or need any additional in formation regarding this questionnaire please do not hesitate to contact us. Research Students Rui Santiago
Project supervisor Philip Von Hauenschild Senior lecturer in Osteopathy at Oxford Brookes University Telephone: 07590283720 Email: [email protected]
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
43/49
Appendix E – Final Questionnaire
SECTION 3: Postural awareness and compliance Sections 2 asked for some information about your sy mptoms. Sections 3 & 4 will help us to identify any changes to your posture and compliance that may have taken place since using th e PAS. 13. Code: ___________________________________ (This unique code will be sent to the participant by email, after 2 weeks of PAS use. It was created to allow the linking of data from each participant before and after the use of the PAS without them having to input personal data on the internet.) 14. Which timings between on-screen reminders did you use most often? a) 20-39 b) 40-59 c) 60 d) 61-80 e) 81-100 f) 101-120 COMMENT: 15. Did you check your posture and perform the exe rcises completely when prompted to by the software? a) 1 - Never (0%) b) 2 - Rarely (1-30%) c) 3 - Some of the exercises (31-60%) d) 4 - Most of the exercises (61-99%) e) 5 - Always (100%) COMMENT: 16. How do you rate your compliance with the on-sc reen postural advice and exercises given by the software? a) 1 - Very Poor b) 2 - Poor c) 3 - OK d) 4 - Good
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
44/49
e) 5 - Very Good COMMENT: 17. How do you rate your awareness of your posture at the computer before using the software? a) 1 - Very Poor b) 2 - Poor c) 3 - OK d) 4 - Good e) 5 - Very Good COMMENT: 18. How do you rate your awareness of your posture at the computer after using the software? a) 1 - Very Poor b) 2 - Poor c) 3 - OK d) 4 - Good e) 5 - Very Good COMMENT: SECTION 4: Symptoms update Section 2 asked for some information about any symp toms which you attribute to or you believe may be aggravated by co mputer use. Section 4 will help to identify any changes to your symptoms since using the PAS. 19. Which of the following statements describe(s) y our current symptoms …. (Please select all that apply)
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
45/49
a) Chronic (the discomfort/ pain is long-lasting, recurrent in nature) b) Acute (the discomfort/ pain started recently, rapid onset, short-lasting) c) Severe (the discomfort/ pain is intense, debilitating) d) The discomfort/ pain is episodic (triggered by certain activities, postures, types of work, amount of work) e) The discomfort/ pain generally wears off overnight or across a weekend f) The discomfort/ pain wears off only with rest, e.g. when on a holiday g) The discomfort/ pain is permanent: may change in intensity, but does not wear off 20. Please indicate which area(s) bother you (Please select all that apply) a) Head (e.g. headache, migraine) b) Eyes (e.g. hot, sore, tired, stinging, dry, weeping eyes; eyestrain) c) Neck d) Shoulder(s) e) Middle of back f) Lower back g) Upper arm(s) h) Forearm(s) i) Wrist(s) j) Hand/ Finger(s) 21. Please indicate which area bothers you the MOST (Please select just ONE) a) Head (e.g. headache, migraine) b) Eyes (e.g. hot, sore, tired, stinging, dry, weeping eyes; eyestrain) c) Neck d) Shoulder(s) e) Middle of back f) Lower back g) Upper arm(s) h) Forearm(s) i) Wrist(s) j) Hand/ Finger(s) k) Other…. Please explain: 22. For the area which bothers you MOST, which of the following describe(s) your symptoms (Please select all that apply): a) Dull ache b) Burning c) Cramping d) Discomfort e) Numbness
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
YOU HAVE REACHED THE END OF THE QUESTIONNAIRE. THANK YOU VERY MUCH FOR YOUR TIME
If you have any questions or need any additional in formation regarding this questionnaire please do not hesitate to contact us. Research Students Rui Santiago
Project supervisor Philip Von Hauenschild Senior lecturer in Osteopathy at Oxford Brookes University Telephone: 07590283720 Email: [email protected]
Rui Santiago - 06084852 Critical Appraisal in Osteopathy
47/49
Appendix F – Consent Form
CONSENT FORM Please initial box
1. I confirm that I have read and understood the information
sheet for the above study and have had the opportunity to ask questions.
2. I understand that my participation is voluntary and that I am free to withdraw at any time, without giving reason.
3. I agree to take part in the above study.
Please tick box Yes No
4. I understand that my participation will not affect any current or future treatment or programme of studies at OBU.
5 I have the authority (or can obtain permission) to install the Postural Awareness Software on my computer.
6 I understood the postural advice given and how to safely perform the exercises.
7 I understand that the information I submit during the study may be published in the study report and that, on request, I will be sent a copy. Confidentiality and anonymity will be maintained and it will not be possible to identify me from any publications.
8 I agree that I can be contacted if the researchers require clarification on any of the information collected during this study.
Name of Participant Date Signature Name of Researcher Date Signature
Postural awareness and the incidence of musculoskeletal disorders in computer users (SH&SC REC Study no. 2009/30)
Rui Santiago - 06084852 Critical Appraisal in Osteopathy