Diverse cutaneous side effects associated with BRAF inhibitor therapy: A clinicopathologic study Emily Y. Chu, MD, PhD, a Karolyn A. Wanat, MD, a Christopher J. Miller, MD, a Ravi K. Amaravadi, MD, b Leslie A. Fecher, MD, b Marcia S. Brose, MD, PhD, c Suzanne McGettigan, MSN, b Lydia R. Giles, BSN, b Lynn M. Schuchter, MD, b John T. Seykora, MD, PhD, a and Misha Rosenbach, MD a Philadelphia, Pennsylvania See related article on page 1375. Background: Vemurafenib, a novel selective small molecule inhibitor of BRAF, has recently been shown to be effective in the treatment of melanomas harboring the BRAF V600E mutation. Similar to the broad- spectrum RAF inhibitor sorafenib, vemurafenib induces development of squamous cell carcinomas and keratoacanthomas as a side effect of therapy. Objective: We sought to detail additional cutaneous adverse effects of vemurafenib and a similar BRAF inhibitor, dabrafenib. Methods: We evaluated the clinical and histologic feature of skin side effects developing on vemurafenib or dabrafenib therapy in 14 patients. Results: Eight patients developed one or more squamous cell carcinomas, and 11 patients formed benign verrucous keratoses. Eight patients developed single lesions and/or widespread eruptions with histopath- ologic findings of acantholytic dyskeratosis, consistent with warty dyskeratomas and Darier- or Grover-like rashes, respectively. One patient developed palmoplantar hyperkeratosis, and darkening of existing nevi and new nevi within 2 months of starting vemurafenib. Side effects presented as early as 1 week after beginning therapy, with a mean time of onset of 12.6 weeks in our cohort. Limitations: This study was limited by the small number of cases, all from a single institution. Conclusion: Selective BRAF inhibitor therapy is associated with the development of malignant and benign growths, including keratoacanthoma-like squamous cell carcinomas, warty dyskeratomas, and verrucous keratoses, along with widespread eruptions with histologic features of acantholytic dyskeratosis. Given the potential for malignant lesions to develop on treatment, awareness of potential adverse effects of these agents is necessary, and a low threshold for biopsy of new growths is recommended. ( J Am Acad Dermatol 2012;67:1265-72.) Key words: acantholytic dyskeratosis; BRAF; drug adverse effects; nevi; squamous cell carcinoma; verrucous keratosis; warty dyskeratoma. V emurafenib is a recently developed small molecule inhibitor of the serine/threonine kinase BRAF, a component of the RASeRAFeMEKeERK (mitogen-activated protein kinase [MAPK]) signaling pathway that effects cellu- lar processes including proliferation, survival, and From the Department of Dermatology, a Division of Hematolo- gy/Oncology, Department of Medicine, b and Department of Otorhinolaryngology, c Hospital of the University of Pennsylvania. Dr Fecher is currently affiliated with the Division of Hematolo- gy/Oncology, Department of Medicine, Indiana University, Indianapolis. Supported by the Skin Disease Research Center at the University of Pennsylvania. Disclosure: Dr Amaravadi is a consultant for and has received honoraria from Genentech. Dr Fecher is an investigator for Roche, Genentech, and GlaxoSmithKline, and has received research funding from those sources. Dr Schuchter is an investigator for Roche and GlaxoSmithKline, and has received grant funding from both sources. Drs Chu, Wanat, Miller, Brose, Seykora, and Rosenbach, Ms McGettigan, and Ms Giles have no conflicts of interest to declare. Accepted for publication April 8, 2012. Reprint requests: Emily Y. Chu, MD, PhD, Department of Dermatology, Hospital of the University of Pennsylvania, 2 Maloney Bldg, 3600 Spruce St, Philadelphia, PA 19104. E-mail: [email protected]. Published online May 21, 2012. 0190-9622/$36.00 Ó 2012 by the American Academy of Dermatology, Inc. doi:10.1016/j.jaad.2012.04.008 1265
Transcript
Diverse cutaneous side effects associated with BRAFinhibitor therapy: A clinicopathologic study
Emily Y. Chu, MD, PhD,a Karolyn A. Wanat, MD,a Christopher J. Miller, MD,a Ravi K. Amaravadi, MD,b
Leslie A. Fecher, MD,b Marcia S. Brose, MD, PhD,c Suzanne McGettigan, MSN,b Lydia R. Giles, BSN,b
Lynn M. Schuchter, MD,b John T. Seykora, MD, PhD,a and Misha Rosenbach, MDa
Philadelphia, Pennsylvania
See related article on page 1375.
From
gy
O
Pe
Dr F
gy
In
Supp
of
Discl
ho
Ro
re
Background: Vemurafenib, a novel selective small molecule inhibitor of BRAF, has recently been shownto be effective in the treatment of melanomas harboring the BRAF V600E mutation. Similar to the broad-spectrum RAF inhibitor sorafenib, vemurafenib induces development of squamous cell carcinomas andkeratoacanthomas as a side effect of therapy.
Objective: We sought to detail additional cutaneous adverse effects of vemurafenib and a similar BRAFinhibitor, dabrafenib.
Methods: We evaluated the clinical and histologic feature of skin side effects developing on vemurafenibor dabrafenib therapy in 14 patients.
Results: Eight patients developed one or more squamous cell carcinomas, and 11 patients formed benignverrucous keratoses. Eight patients developed single lesions and/or widespread eruptions with histopath-ologic findings of acantholytic dyskeratosis, consistent with warty dyskeratomas and Darier- or Grover-likerashes, respectively. One patient developed palmoplantar hyperkeratosis, and darkening of existing neviand new nevi within 2 months of starting vemurafenib. Side effects presented as early as 1 week afterbeginning therapy, with a mean time of onset of 12.6 weeks in our cohort.
Limitations: This study was limited by the small number of cases, all from a single institution.
Conclusion: Selective BRAF inhibitor therapy is associated with the development of malignant and benigngrowths, including keratoacanthoma-like squamous cell carcinomas, warty dyskeratomas, and verrucouskeratoses, along with widespread eruptions with histologic features of acantholytic dyskeratosis. Given thepotential for malignant lesions to develop on treatment, awareness of potential adverse effects of theseagents is necessary, and a low threshold for biopsy of new growths is recommended. ( J Am Acad Dermatol2012;67:1265-72.)
differentiation.1 The drug specifically targets tumorcells that harbor activating mutations in BRAF, mostcommonly the substitution of glutamic acid for valineat codon 600 (V600E).2 Vemurafenib was approvedby the Food and Drug Administration for treatmentof metastatic melanoma in August 2011, afterpromising tumor responses to the medication in
CAPSULE SUMMARY
d Selective BRAF inhibitors are known toproduce certain cutaneous adverseeffects such as keratoacanthomas,squamous cell carcinomas, andphotosensitivity.
d We describe 14 patients with diverse skinside effects related to BRAF inhibitortherapy, including verrucous keratoses,warty dyskeratomas, Darier- and Grover-like eruptions, eruptive and darkeningnevi, and squamous cell carcinomas.
d Cutaneous side effects appear to arise asa result of paradoxical activation ofmitogen-activated protein kinasesignaling in the setting of BRAF inhibitortherapy.
phase I, II, and III clinicaltrials.3-5 A similar selectiveBRAF inhibitor, dabrafenib(GSK2118436), is currentlybeing tested in clinical stud-ies for treatment of advancedstage and metastatic mela-noma, as a single agent andin combination with a MEKinhibitor, trametinib(GSK1120212).1,6,7
Several cutaneous adverseeffects of vemurafenib havebeen noted in earlier clinicalstudies.3,4 Photosensitivity,sometimes resulting in blis-tering reactions, has beendocumented.3,8 Palmar-plantar dysesthesia occurredin several patients.4 Keratosispilariselike eruptions occurin roughly one third of pa-tients treated.3,9 Lastly, squa-
mous cell carcinomas (SCCs) and keratoacanthomas(KAs) have been reported in 20% to 30% of patientstreated with vemurafenib.3,4
Here, we describe in detail the cutaneous sideeffects observed in 14 patients after initiation ofBRAF inhibitor therapy. These findings include thepreviously noted eruptive SCCs, and several addi-tional skin reactions, which will be discussed indetail.
REPORT OF REPRESENTATIVE CASESCase 1
A 47-year-old Caucasian woman (patient 1,Table I) was diagnosed with stage IV melanomawith lung involvement, and was found to haveV600E mutation in BRAF. Vemurafenib 960 mg twicedaily was initiated, and 12 weeks after beginningtherapy she noticed new scaly papules on the centralaspect of her chest (Fig 1, A), upper aspect of hershoulders, back, and face. Several biopsies wereperformed at these sites. A biopsy from a 2-mm,pink, hyperkeratotic papule on the central aspect ofher chest revealed an epidermal invagination featur-ing acantholysis and dyskeratosis and clefting ofthe suprabasilar epidermis, characteristic of warty
dyskeratomas (Fig 1, B). Histopathologic examina-tion of a papule on the patient’s face demonstrated abenign verrucous keratosis, and samples taken fromthe shoulder and back revealed SCCs (not shown).After 2 months of treatment with vemurafenib, thepatient had a 60% reduction of her tumor burdenbased on computed tomography examination, and
symptomatically experi-enced relief of her disease-related chronic cough andfatigue.
Case 2A 55-year-old Caucasian
woman (patient 7, Table I)had a history of multiple pri-mary melanomas on her ab-domen, arm, and elbow anddeveloped metastatic diseaseto her axillary lymph nodesand brain 1 month after de-tection of her third primarymelanoma. Tumor genotyp-ing revealed the BRAF V600Emutation. Vemurafenib wasstarted at a dose of 960 mgtwice a day, and she devel-oped a new rash on herchest, face, and arms 4weeks
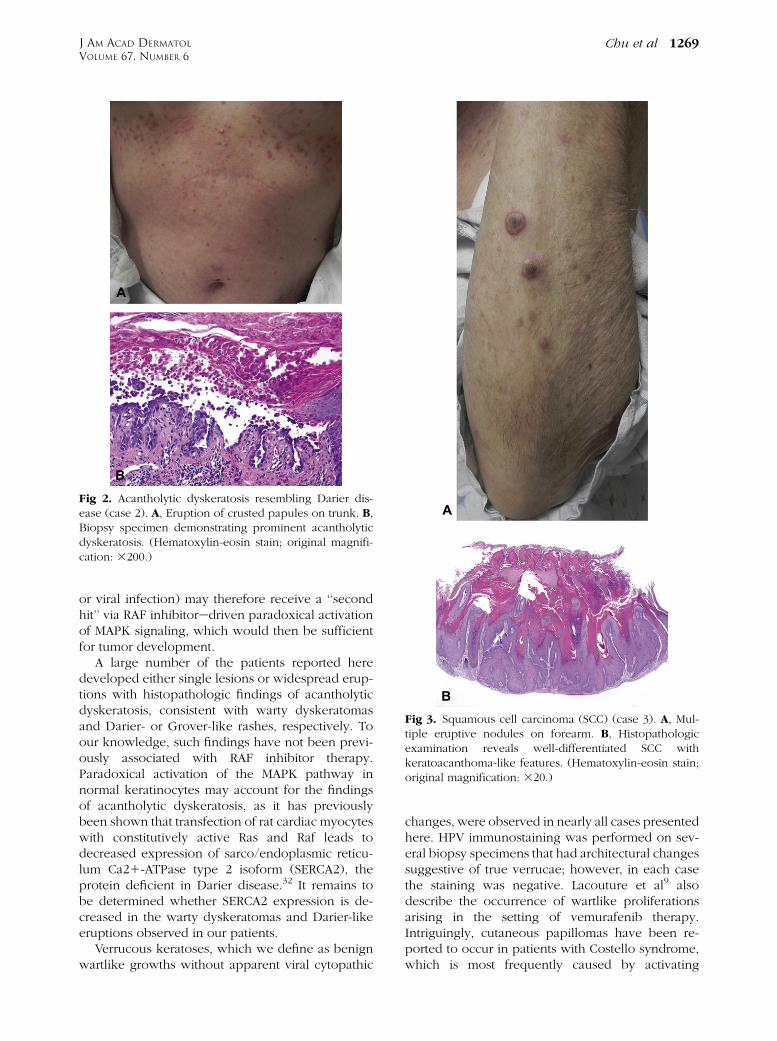
later. Of note, she had no history of nonmelanomaskin cancers. On physical examination, she hadmany erythematous, 2- to 3-mm scaly papules onher chest and abdomen (Fig 2, A), and a 1-cm dome-shaped hyperkeratotic, tender red papule on herarm. Histopathologic examination of the chest le-sions demonstrated acantholysis and dyskeratosisconsistent with Grover disease (also known as tran-sient acantholytic dyskeratosis) or Darier disease (Fig2, B). An additional biopsy specimen revealed a SCCon her arm (not shown). The acantholytic rash wasresponsive to treatment with triamcinolone 0.1%ointment, and the SCC was treated with wide localexcision.
Coincident with the development of her skinlesions, the patient noted a reduction in size of hersubcutaneous lymph nodes. However, her braindisease later progressed on therapy, and she subse-quently died.
Case 3An 83-year-old Caucasian woman (patient 13,
Table I) with a history of an aggressive melanomaon her scalp status-post excision was given thediagnosis of metastatic disease involving her lungsand left breast. She was initially treated with
Abbreviations used:
CFC: cardiofaciocutaneousKA: keratoacanthomaMAPK: mitogen-activated protein kinaseSCC: squamous cell carcinoma
J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Chu et al 1267
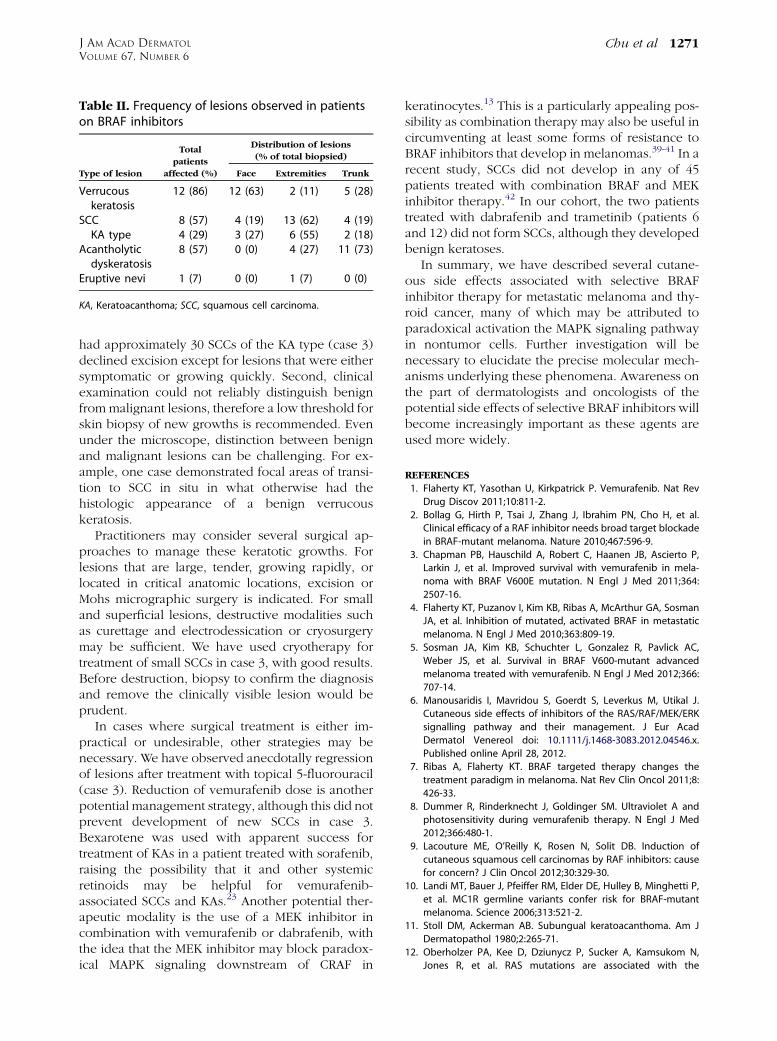
temozolomide and radiation therapy, with partialresponse. Vemurafenib was then started at 960 mgtwice daily after detection of BRAF V600K mutationin her tumor. After 1 week on the medication, shenoticed eruptive growths on her forehead, arms,legs, and back. She denied any history of non-melanoma skin cancers before starting vemurafenib.On physical examination, she had approximately 303- to 10-mm inflamed papules and nodules withkeratotic cores on the face, back, arms, and legs (Fig3, A), Biopsy specimens taken from multiple lesionsdemonstrated similar findings of large cup-shapedatypical proliferations of squamous epithelial cells,with central keratin-filled craters, diagnostic of SCCof the KA type (Fig 3, B). The patient’s SCCs were allwell differentiated, and exhibited moderate solarelastosis in the surrounding dermis. The lesionsranged from 2 to 3.5 mm in thickness, extendingfrom superficial to deep reticular dermis.
Marked reduction in size of the patient’s scalpmelanoma was observed after 4 weeks of treatment.Because of medication-related fatigue, the patient’sdose of vemurafenib was subsequently decreased to720 mg twice daily, but she continued to developadditional SCCs. The patient was prescribed topical5-fluorouracil to apply twice daily to SCCs indefi-nitely; several lesions have demonstrated regressionclinically on therapy.
Case 4A 57-year-old Chinese man (patient 14, Table I)
had a history of papillary thyroid cancer status-posttotal thyroidectomy, with involvement in his lymphnodes, jaw, and right parotid gland. He received butwas resistant to radioactive iodine andwas placed ona clinical trial of vemurafenib for his metastaticdisease after confirmation of a BRAF V600E muta-tion. After 8 weeks of treatment, he had a 22%reduction of tumor burden on computed tomogra-phy scan. At the same time, he developed severalnew papules on his face. He also noticed newpigmented macules on his palms. He denied historyof nonmelanoma skin cancers.
On physical examination, he had flesh-coloredand slightly erythematous verrucous papules on thenose and left cheek (Fig 4, A). He was also notedto have two new brown macules on his palm(Fig 5, A), and one on the plantar aspect of his
foot, on a background of new focal palmoplantarhyperkeratosis. He had multiple evenly pigmentednevi scattered on his trunk and arms (Fig 5, B), whichhad darkened after starting the medication. Thedarkening was marked, noted both by the patientand the clinician based on pretreatment and post-treatment evaluations. Histopathologic examinationof a facial papule demonstrated hyperkeratosis,acanthosis, and papillomatosis without apparentkoilocytic change, consistent with a verrucous ker-atosis (Fig 4, B). Biopsy specimen of a dark nevus onthe trunk revealed a junctional dysplastic nevus withmoderate atypia (not shown).
DISCUSSIONVemurafenib and dabrafenib commonly induce
cutaneous reactions. Each of the 14 patients (13 withmetastatic melanoma and one with metastatic thy-roid cancer) reported here developed one or moreskin side effects after initiation of vemurafenib ordabrafenib treatment, and 13 of the 14 exhibited atleast two different types of skin reactions (Table I).Verrucous keratoses weremost commonly observed,occurring in 12 of 14 patients. SCCs and acantholyticeruptions each appeared in 8 of the 14 patients(Table II). Patient 14, with metastatic papillarythyroid cancer, experienced darkening of hispre-existing nevi and eruption of several new nevion acral sites.
Interestingly, only 3 of the 8 patients who devel-oped a SCC on therapy had been given the diagnosisof a SCC before starting vemurafenib (patients 1, 2,and 7). Histologically, the SCCs observed in ourpatients were well-differentiated lesions. The SCCsbiopsied ranged from in situ carcinoma, to invasiveSCCs with a greatest thickness of 3.5 mm (data notshown). The thickest lesions extended to the mid todeep reticular dermis, and none demonstrated per-ineural invasion. All lesions occurred on a back-ground of solar elastosis, with most exhibitingmoderate sun damage (CSD 2, per the gradingscheme devised by Landi et al10). In 4 of 8 patientswith SCCs, at least one of their tumors exhibitedfeatures of a KA, with cup-shaped architecture andcentral keratin-filled crater. Whereas KAs classicallydemonstrate microabscesses composed of neutro-phils and/or eosinophils within epithelial nests,11
these features were not observed in the biopsyspecimens from this cohort.
Recent evidence suggests that SCCs and KAs arisespecifically in the setting of RAF inhibitor ther-apy.12,13 Sorafenib, a multikinase inhibitor withpan-RAF activity, has been demonstrated in multiplereports to induce SCCs and KAs.14-24 Sorafenib has amuch broader spectrum of action than vemurafenib
Table I. Characteristic of patients on BRAF inhibitors
Characteristic
Patient no.
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Age, y 46 64 47 60 54 53 55 58 69 77 68 64 83 57Sex F M F F F M F F F M F M F MTargeted therapy V V V V V D 1 T V V V V D D 1 T; V V VTime before first skinlesion, wk
D, Dabrafenib (GSK2118436); F, female; KA, keratoacanthoma; M, male; SCC, squamous cell carcinoma; T, trametinib (GSK1120212);
V, vemurafenib.
Fig 1. Warty dyskeratoma (case 1). A, New keratotic pap-ules on chest. B, Biopsy specimen demonstrating acanthol-ysis and dyskeratosis, consistent with warty dyskeratoma.(Hematoxylin-eosin stain; original magnification: 3200.)
J AM ACAD DERMATOL
DECEMBER 20121268 Chu et al
and dabrafenib, exhibiting activity against vascularendothelial growth factor receptor 1, 2, and 3;platelet-derived growth factor receptor-b; FMS-like
tyrosine kinase 3; c-kit; RET receptor tyrosine kinase;and all isoforms of RAF.25 Significantly, the multi-kinase inhibitor sunitinib, which targets many of thesame kinases as sorafenib (vascular endothelialgrowth factor receptor 1, 2, and 3; platelet-derivedgrowth factor receptor; c-kit; FMS-like tyrosine ki-nase 3; and RET tyrosine kinase) but not RAF, doesnot result in development of SCCs or KAs.13,26
Sorafenib is a nonselective inhibitor of wild-typeand mutated forms of RAF, with poor activity againstBRAF V600E tumor cells, and has been demonstratedto be an ineffective treatment for melanoma.7,27 Anestimated 6% to 7% of patients treated with sorafenibdevelop SCCs and KAs, which stands in contrast to20% to 30% of patients taking vemurafenib.3,4
The mechanism underlying development of SCCsin patients treated with RAF inhibitors is activelybeing investigated. Recent data suggest that phar-macologic RAF blockade in cells harboring wild-typeBRAF paradoxically increases signaling throughCRAF, which then increases MAPK signaling over-all.28-30 Arnault et al31 examined normal-appearingskin biopsy specimens from patients treated withsorafenib, finding increased Ki67 and phosphory-lated ERK staining in keratinocytes on histologicsections, compared with normal-appearing skintaken from placebo-treated patients. This suggeststhat MAPK signaling is in fact increased, presumablyleading to increased keratinocyte proliferation.Paradoxical activation of MAPK signaling by itselfmay not be sufficient to induce SCCs and KAs. To thisend, Oberholzer et al12 determined that RAS activat-ing mutations are more frequently found in SCCs andKAs from patients treated with vemurafenib (30%)and sorafenib (11%) compared with those fromcontrol patients (3.2%). Pre-existing RAS mutationsin keratinocytes (possibly induced by sun exposure
Fig 2. Acantholytic dyskeratosis resembling Darier dis-ease (case 2). A, Eruption of crusted papules on trunk. B,Biopsy specimen demonstrating prominent acantholyticdyskeratosis. (Hematoxylin-eosin stain; original magnifi-cation: 3200.)
or viral infection) may therefore receive a ‘‘secondhit’’ via RAF inhibitoredriven paradoxical activationof MAPK signaling, which would then be sufficientfor tumor development.
A large number of the patients reported heredeveloped either single lesions or widespread erup-tions with histopathologic findings of acantholyticdyskeratosis, consistent with warty dyskeratomasand Darier- or Grover-like rashes, respectively. Toour knowledge, such findings have not been previ-ously associated with RAF inhibitor therapy.Paradoxical activation of the MAPK pathway innormal keratinocytes may account for the findingsof acantholytic dyskeratosis, as it has previouslybeen shown that transfection of rat cardiac myocyteswith constitutively active Ras and Raf leads todecreased expression of sarco/endoplasmic reticu-lum Ca21-ATPase type 2 isoform (SERCA2), theprotein deficient in Darier disease.32 It remains tobe determined whether SERCA2 expression is de-creased in the warty dyskeratomas and Darier-likeeruptions observed in our patients.
Verrucous keratoses, which we define as benignwartlike growths without apparent viral cytopathic
changes, were observed in nearly all cases presentedhere. HPV immunostaining was performed on sev-eral biopsy specimens that had architectural changessuggestive of true verrucae; however, in each casethe staining was negative. Lacouture et al9 alsodescribe the occurrence of wartlike proliferationsarising in the setting of vemurafenib therapy.Intriguingly, cutaneous papillomas have been re-ported to occur in patients with Costello syndrome,which is most frequently caused by activating
Fig 4. Verrucous keratosis (case 4). A, Multiple verrucouspapules on face. B, Biopsy specimen of facial papulereveals hyperkeratosis, acanthosis, and papillomatosis inabsence of viral changes, all features of verrucous kerato-sis. (Hematoxylin-eosin stain; original magnification:340.)
Fig 5. Eruptive nevi and darkening nevi (case 4). A, Newnevi on palm developing on treatment with vemurafenib,and focal palmar hyperkeratosis. B, Nevi on trunk, whichdarkened after initiation of vemurafenib.
J AM ACAD DERMATOL
DECEMBER 20121270 Chu et al
germline HRAS mutations,33,34 and in those withcardiofaciocutaneous (CFC) syndrome, in whichactivating germline mutations in BRAF, MEK1,MEK2, and KRAS are the most common underlyinggenetic alterations.35 Papillomas are more commonin Costello syndrome, occurring most often on thenose and central aspect of the face.34 Histologically,the papillomas of Costello syndrome resemble theverrucous keratoses observed in our study, demon-strating verrucous epidermal hyperplasia withoutthe koilocytes and clumped keratohyalin granulesfound in common verrucae.36 It is interesting to notethat most of the verrucous keratoses observed in ourstudy were biopsied from the face (63%).
Eruptive nevi have been described in patientstreated with sorafenib, occurring on acral sites in onepatient.37 The patient presented in case 4 not onlydeveloped new acral nevi, but also experienceddarkening of pre-existing nevi. These findings againwarrant comparison with the inherited CFC syn-drome, in which a greater than average number ofnevi is a characteristic finding. Nevi in patients withCFC syndrome are typically evenly distributed acrossall body sites, and individually are uniformly pig-mented and medium to dark brown in color.35
Mild palmoplantar hyperkeratosis, accentuated atpressure points, affected the patient in case 4 afterstarting vemurafenib, and several other patients in
this practice. Palmoplantar hyperkeratosis is a fre-quent side effect of sorafenib therapy, in the contextof the hand-foot skin reaction.38 Drawing furtherparallels to Costello and CFC syndromes, focalpalmoplantar hyperkeratosis appears in both condi-tions often, in 76% and 36% of patients,respectively.34
Clinical management of the keratotic lesions pre-sents challenges. First, patients frequently presentwith such a high number of keratotic lesions thatsurgical management with excision may be imprac-tical or intolerable. For example, our patient who
Table II. Frequency of lesions observed in patientson BRAF inhibitors
KA, Keratoacanthoma; SCC, squamous cell carcinoma.
J AM ACAD DERMATOL
VOLUME 67, NUMBER 6Chu et al 1271
had approximately 30 SCCs of the KA type (case 3)declined excision except for lesions that were eithersymptomatic or growing quickly. Second, clinicalexamination could not reliably distinguish benignfrommalignant lesions, therefore a low threshold forskin biopsy of new growths is recommended. Evenunder the microscope, distinction between benignand malignant lesions can be challenging. For ex-ample, one case demonstrated focal areas of transi-tion to SCC in situ in what otherwise had thehistologic appearance of a benign verrucouskeratosis.
Practitioners may consider several surgical ap-proaches to manage these keratotic growths. Forlesions that are large, tender, growing rapidly, orlocated in critical anatomic locations, excision orMohs micrographic surgery is indicated. For smalland superficial lesions, destructive modalities suchas curettage and electrodessication or cryosurgerymay be sufficient. We have used cryotherapy fortreatment of small SCCs in case 3, with good results.Before destruction, biopsy to confirm the diagnosisand remove the clinically visible lesion would beprudent.
In cases where surgical treatment is either im-practical or undesirable, other strategies may benecessary. We have observed anecdotally regressionof lesions after treatment with topical 5-fluorouracil(case 3). Reduction of vemurafenib dose is anotherpotential management strategy, although this did notprevent development of new SCCs in case 3.Bexarotene was used with apparent success fortreatment of KAs in a patient treated with sorafenib,raising the possibility that it and other systemicretinoids may be helpful for vemurafenib-associated SCCs and KAs.23 Another potential ther-apeutic modality is the use of a MEK inhibitor incombination with vemurafenib or dabrafenib, withthe idea that the MEK inhibitor may block paradox-ical MAPK signaling downstream of CRAF in
keratinocytes.13 This is a particularly appealing pos-sibility as combination therapy may also be useful incircumventing at least some forms of resistance toBRAF inhibitors that develop in melanomas.39-41 In arecent study, SCCs did not develop in any of 45patients treated with combination BRAF and MEKinhibitor therapy.42 In our cohort, the two patientstreated with dabrafenib and trametinib (patients 6and 12) did not form SCCs, although they developedbenign keratoses.
In summary, we have described several cutane-ous side effects associated with selective BRAFinhibitor therapy for metastatic melanoma and thy-roid cancer, many of which may be attributed toparadoxical activation the MAPK signaling pathwayin nontumor cells. Further investigation will benecessary to elucidate the precise molecular mech-anisms underlying these phenomena. Awareness onthe part of dermatologists and oncologists of thepotential side effects of selective BRAF inhibitors willbecome increasingly important as these agents areused more widely.
REFERENCES
1. Flaherty KT, Yasothan U, Kirkpatrick P. Vemurafenib. Nat Rev
Drug Discov 2011;10:811-2.
2. Bollag G, Hirth P, Tsai J, Zhang J, Ibrahim PN, Cho H, et al.
Clinical efficacy of a RAF inhibitor needs broad target blockade
in BRAF-mutant melanoma. Nature 2010;467:596-9.
3. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P,
Larkin J, et al. Improved survival with vemurafenib in mela-
noma with BRAF V600E mutation. N Engl J Med 2011;364:
2507-16.
4. Flaherty KT, Puzanov I, Kim KB, Ribas A, McArthur GA, Sosman
JA, et al. Inhibition of mutated, activated BRAF in metastatic