39
Dizziness Dizziness Paul Chatrath Consultant ENT Surgeon Barking Havering & Redbridge Hospitals NHS Trust 21 st January 2009
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | francine-little |
| View: | 214 times |
| Download: | 0 times |

DizzinessDizziness
Paul ChatrathConsultant ENT Surgeon
Barking Havering & Redbridge Hospitals NHS Trust
21st January 2009

ObjectivesObjectives
DefinitionsDefinitions Clinical history & examinationClinical history & examination Multiple factorsMultiple factors Key conditions – BPPV, Meniere’s, Key conditions – BPPV, Meniere’s,
labyrinthitis, non-vestibularlabyrinthitis, non-vestibular

““Dizziness”Dizziness”
Presyncopal faintnessPresyncopal faintness Loss of balance/imbalanceLoss of balance/imbalance UnsteadinessUnsteadiness Light-headednessLight-headedness WhoozinessWhooziness VertigoVertigo Feeling of rotation or movementFeeling of rotation or movement
BalanceBalance
Vestibular systemVestibular system Peripheral vestibular (labyrinth)Peripheral vestibular (labyrinth) CerebellarCerebellar
Visual system - VORVisual system - VOR Proprioceptive system - VSRProprioceptive system - VSR

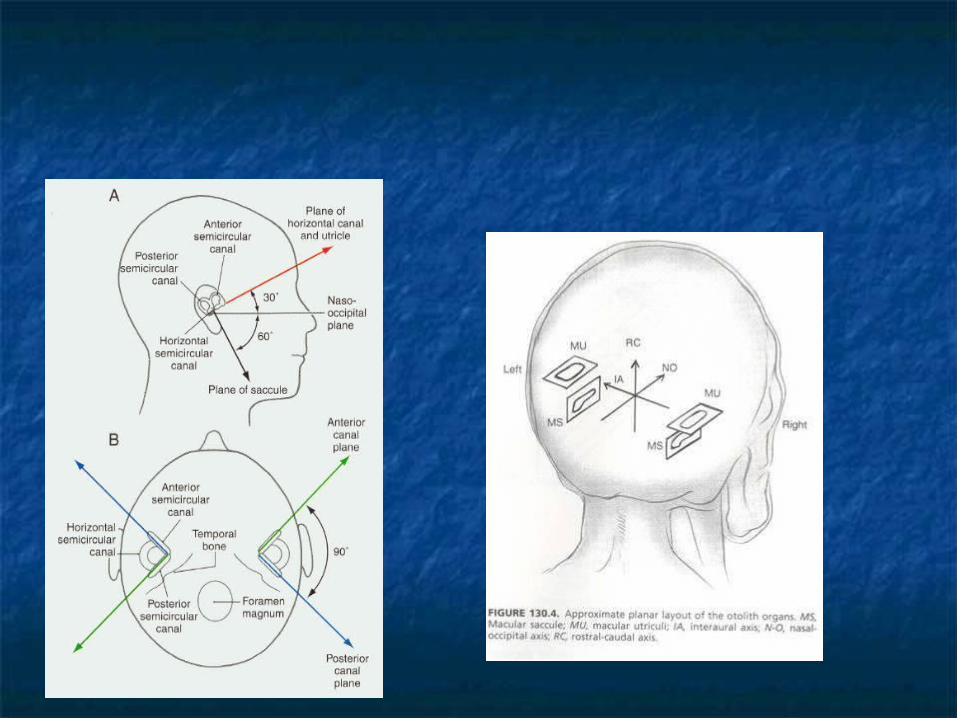
Vestibular LabyrinthVestibular Labyrinth
3 semicircular canals3 semicircular canals rotational movementrotational movement cupulacupula
2 otolithic organs - utricle & saccule2 otolithic organs - utricle & saccule linear accelerationlinear acceleration maculamacula

Clinical approachClinical approach
Vertigo vs dizzinessVertigo vs dizziness Vertigo – peripheral vestibular or Vertigo – peripheral vestibular or
cerebellarcerebellar Dizziness – non vestibularDizziness – non vestibular
Questions to establish causes for Questions to establish causes for each of theseeach of these

Vertigo vs DizzinessVertigo vs Dizziness
Definition of vertigo:Definition of vertigo: Illusion of movement of oneself or the Illusion of movement of oneself or the
surroundingssurroundings Typically rotatoryTypically rotatory Looking for vestibular causesLooking for vestibular causes
If no rotatory component:If no rotatory component: Likely to be nonspecific dizzinessLikely to be nonspecific dizziness Looking for non-vestibular causesLooking for non-vestibular causes

Vertigo vs Dizziness:Vertigo vs Dizziness: Unclear? Unclear?
Vertigo:Vertigo: RotatoryRotatory Worse on head movementsWorse on head movements Nausea/vomiting on head movementsNausea/vomiting on head movements
Vague descriptions: rarely true Vague descriptions: rarely true vertigovertigo

Vertigo - causesVertigo - causes
VestibularVestibular Viral labyrinthitisViral labyrinthitis BPPVBPPV Meniere’s diseaseMeniere’s disease Acute Otitis MediaAcute Otitis Media TraumaTrauma CholesteatomaCholesteatoma Drug inducedDrug induced PostsurgicalPostsurgical
CentralCentral MigraineMigraine Vertebrobasilar ischaemiaVertebrobasilar ischaemia MSMS TumoursTumours
Cerebellopontine angleCerebellopontine angle Acoustic neuromaAcoustic neuroma
BrainstemBrainstem CVACVA
PsychogenicPsychogenic
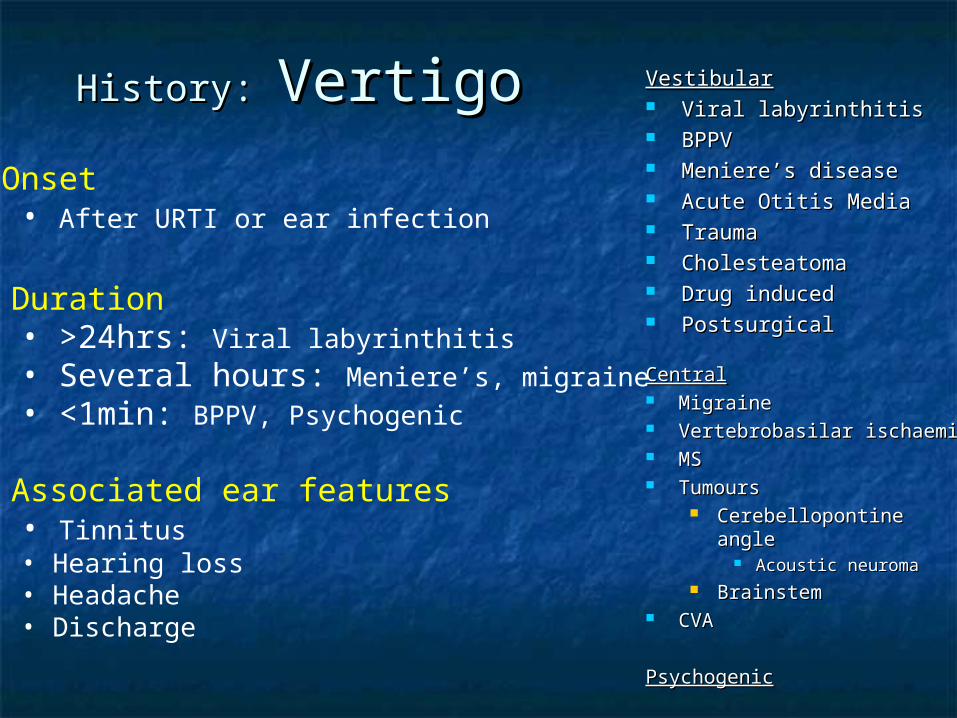
History: History: VertigoVertigo VestibularVestibular Viral labyrinthitisViral labyrinthitis BPPVBPPV Meniere’s diseaseMeniere’s disease Acute Otitis MediaAcute Otitis Media TraumaTrauma CholesteatomaCholesteatoma Drug inducedDrug induced PostsurgicalPostsurgical
CentralCentral MigraineMigraine Vertebrobasilar ischaemiaVertebrobasilar ischaemia MSMS TumoursTumours
Cerebellopontine angleCerebellopontine angle Acoustic neuromaAcoustic neuroma
BrainstemBrainstem CVACVA
PsychogenicPsychogenic
• Onset• After URTI or ear infection
• Duration• >24hrs: Viral labyrinthitis• Several hours: Meniere’s, migraine• <1min: BPPV, Psychogenic
• Associated ear features
• Tinnitus• Hearing loss• Headache• Discharge

History: History: VertigoVertigo VestibularVestibular Viral labyrinthitisViral labyrinthitis BPPVBPPV Meniere’s diseaseMeniere’s disease Acute Otitis MediaAcute Otitis Media TraumaTrauma CholesteatomaCholesteatoma Drug inducedDrug induced PostsurgicalPostsurgical
CentralCentral MigraineMigraine Vertebrobasilar ischaemiaVertebrobasilar ischaemia MSMS TumoursTumours
Cerebellopontine angleCerebellopontine angle Acoustic neuromaAcoustic neuroma
BrainstemBrainstem CVACVA
PsychogenicPsychogenic
• Associated central features• Face or arm weakness/numbness
• Frequency• Single: labyrinthitis, MS• Constant:
• decompensation• neurological• psychogenic
• Trauma• Drug history
• Aminoglycosides• Diuretics• Aspirin• Chemotherapy
• Surgery
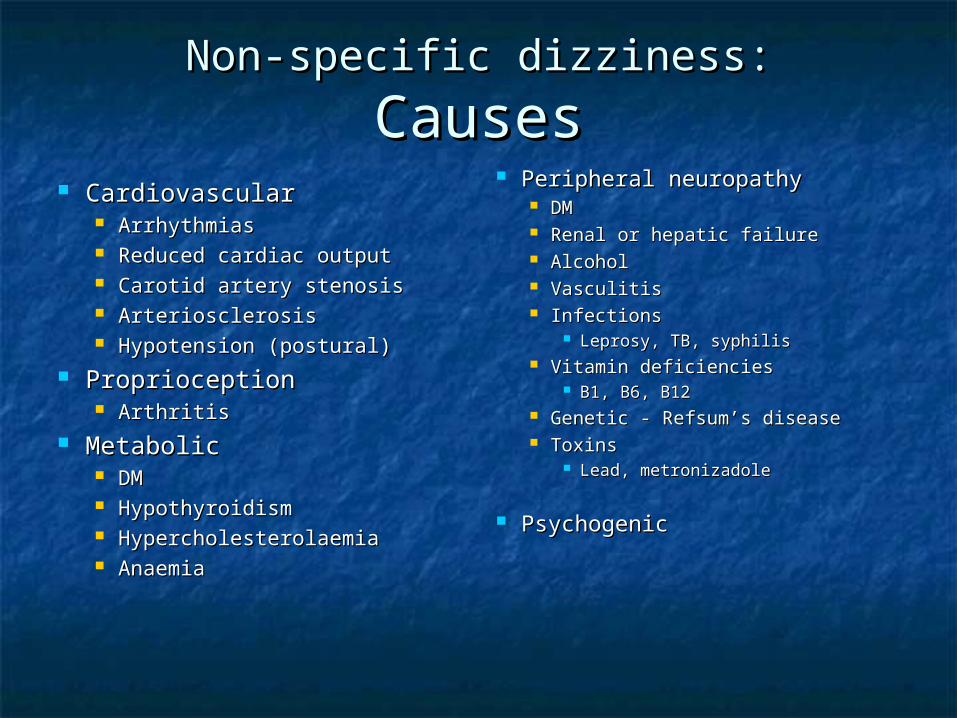
Non-specific dizziness:Non-specific dizziness:
CausesCauses CardiovascularCardiovascular
ArrhythmiasArrhythmias Reduced cardiac outputReduced cardiac output Carotid artery stenosisCarotid artery stenosis ArteriosclerosisArteriosclerosis Hypotension (postural)Hypotension (postural)
ProprioceptionProprioception ArthritisArthritis
MetabolicMetabolic DMDM HypothyroidismHypothyroidism HypercholesterolaemiaHypercholesterolaemia AnaemiaAnaemia
Peripheral neuropathyPeripheral neuropathy DMDM Renal or hepatic failureRenal or hepatic failure AlcoholAlcohol VasculitisVasculitis InfectionsInfections
Leprosy, TB, syphilisLeprosy, TB, syphilis Vitamin deficienciesVitamin deficiencies
B1, B6, B12B1, B6, B12 Genetic - Refsum’s diseaseGenetic - Refsum’s disease ToxinsToxins
Lead, metronizadoleLead, metronizadole
PsychogenicPsychogenic

ExaminationExamination EarsEars
TMsTMs
Cranial nervesCranial nerves All are useful!All are useful!
General General examinationexamination
Nystagmus: Nystagmus: ‘rhythmic ‘rhythmic oscillating involuntary movement oscillating involuntary movement of eyes’of eyes’
CerebellarCerebellar
PosturePosture Romberg’sRomberg’s Unterberger’sUnterberger’s
Hallpike’sHallpike’s

NystagmusNystagmus
Movement of the Movement of the eyes:eyes: RhythmicRhythmic OscillatingOscillating SynchronousSynchronous InvoluntaryInvoluntary
Two phasesTwo phases Slow phase Slow phase
(pathological)(pathological) Fast phase Fast phase
(corrective)(corrective) Direction described Direction described
in terms of fast in terms of fast phasephase

XL
NystagmusNystagmus
Eyes central Slow drift to rightRapid corrective flick to left
= Left nystagmus
L R
Normal labyrinths Abnormal Right Labyrinth

Vertigo:Vertigo:
Vestibular v CentralVestibular v CentralVestibularVestibular CentralCentral
Type of dizziness Vertigo Vertigo / Dizzy
Effect of head movement Worse Equivocal
Tinnitus/hearing loss May be present Absent
Compensation Occurs Does not occur
Nystagmus Horizontal Horizontal or vertical+ unilateral + bilateral+ away from affected ear

Vertigo:Vertigo:
CompensationCompensation Vestibular Vestibular
phenomenonphenomenon Steady Steady
accommodation to accommodation to the effects of vertigothe effects of vertigo
Gradual resolution of Gradual resolution of symptoms over timesymptoms over time
Typically occurs 6-12 Typically occurs 6-12 weeks after acute weeks after acute insultinsult
MechanismsMechanisms HabituationHabituation
Reduced output Reduced output good sidegood side
Increased output Increased output affected sideaffected side
Sensory substitutionSensory substitution Increased reliance Increased reliance
on eyes and on eyes and musculoskeletal musculoskeletal systemsystem

Vertigo:Vertigo:
CompensationCompensation Impaired Impaired
compensation due to:compensation due to: Poor visual acuityPoor visual acuity Musculoskeletal Musculoskeletal
problemsproblems Reduced peripheral Reduced peripheral
sensory inputsensory input Ongoing vestibular Ongoing vestibular
pathologypathology Medication (prolonged Medication (prolonged
stemetil)stemetil)
Rehabilitation:Rehabilitation: General fitnessGeneral fitness
Vision, walking stickVision, walking stick Physical programsPhysical programs
Cawthorne-CookseyCawthorne-Cooksey Psychological Psychological
supportsupport Specific exercisesSpecific exercises
Eg. Brandt-Daroff Eg. Brandt-Daroff exercises for BPPVexercises for BPPV

Cawthorne - CookseyCawthorne - Cooksey
Developed in 1940sDeveloped in 1940s Head movementsHead movements Balance tasksBalance tasks Coordination of eyes with headCoordination of eyes with head Total body movementsTotal body movements Eyes open & closedEyes open & closed Noisy environmentsNoisy environments Early exacerbation of vertigoEarly exacerbation of vertigo

InvestigationsInvestigations
Radiology Radiology (anatomical (anatomical imaging)imaging) MRI – good for IAM’sMRI – good for IAM’s CT – good for CT – good for
vestibular anatomyvestibular anatomy AudiogramAudiogram
Asymmetry needs Asymmetry needs further imagingfurther imaging
Tests of vestibular Tests of vestibular functionfunction ENGs ENGs
(electronystagmograp(electronystagmography)hy)
Caloric testsCaloric tests Rotation testsRotation tests

Symptomatic TxSymptomatic Tx
Acute phaseAcute phase PhenothiazinesPhenothiazines
ProchlorperazineProchlorperazine
(Stemetil)(Stemetil) AntihistaminesAntihistamines
Cinnarizine (Stugeron)Cinnarizine (Stugeron) Cyclizine (Valoid)Cyclizine (Valoid) Promethazine (Avomine)Promethazine (Avomine)
Histamine analoguesHistamine analogues Betahistine (Serc)Betahistine (Serc)
Longer term:Longer term: Depends on Depends on
specific conditionspecific condition

Caution:Caution:
ProchlorperazineProchlorperazine Powerful vestibular sedativePowerful vestibular sedative Suppresses acute vertiginous Suppresses acute vertiginous
symptomssymptoms
BUTBUT Also suppresses natural compensatory Also suppresses natural compensatory
responseresponse LT use: ‘non-specific dizziness’ LT use: ‘non-specific dizziness’
persistspersists

PsychogenicPsychogenic Type of dizziness: Type of dizziness: any (nonspecific or any (nonspecific or
vertigo)vertigo) Frequency: Frequency: constantconstant Duration:Duration: Typically brief <1min Typically brief <1min Trigger: Trigger: Stress, anxiety, crowdsStress, anxiety, crowds Associated features: Associated features: palpitations, palpitations,
sweating, tremorsweating, tremor Examination: Examination: NormalNormal

LabyrinthitisLabyrinthitis
OtiticOtitic InfectiveInfective
Viral (serous)Viral (serous) CMV, influenza, CMV, influenza,
adenovirusadenovirus Bacterial Bacterial
(suppurative)(suppurative) Strep pneumoniaeStrep pneumoniae HaemophilusHaemophilus MoraxellaMoraxella
Other causesOther causes cholesteatomacholesteatoma
Other sourceOther source MeningealMeningeal TBTB SyphilisSyphilis NeoplasiaNeoplasia HaematogenicHaematogenic
LabyrinthitisLabyrinthitis
HistoryHistory VertigoVertigo
>24hrs>24hrs VomitingVomiting Constitutional Constitutional
symptomssymptoms ExaminationExamination
NystagmusNystagmus Fast phase away from Fast phase away from
affected earaffected ear PyrexiaPyrexia
TreatmentTreatment Bed restBed rest Vestibular sedativesVestibular sedatives FluidsFluids Cawthorne-Cooksey Cawthorne-Cooksey
vestibular vestibular rehabilitation rehabilitation exercisesexercises

Meniere’s DiseaseMeniere’s Disease
Key features:Key features: VertigoVertigo
Hours not minutes or Hours not minutes or daysdays
Associated tinnitus Associated tinnitus and hearing lossand hearing loss
Before, during or Before, during or after vertigoafter vertigo
Other symptomsOther symptoms Pressure feelingPressure feeling NauseaNausea
AetiologyAetiology VascularVascular ‘‘Hydrops’Hydrops’
Natural historyNatural history One episodeOne episode EpisodicEpisodic Increasing Increasing
frequencyfrequency

Meniere’s Disease:Meniere’s Disease:
Medical therapyMedical therapy Salt restrictionSalt restriction DiureticsDiuretics
Thiazides - Na Thiazides - Na absorption in distal absorption in distal tubuletubule
Side effects - Side effects - hypokalemia, hypokalemia, hypotension, hypotension, hyperuricemia, hyperuricemia, hyperlipoproteinemiahyperlipoproteinemia
VasodilatorsVasodilators Betahistine, Betahistine,
cinnarizinecinnarizine Evidence – no RCTsEvidence – no RCTs
Cinnarizine > placeboCinnarizine > placebo Diuretics = placeboDiuretics = placebo Serc of marginal Serc of marginal
benefitbenefit Salt restriction of Salt restriction of
marginal benefitmarginal benefit

Meniere’s Disease:Meniere’s Disease:
Surgical therapySurgical therapy
Hearing preservationHearing preservation Vestibular preservationVestibular preservation
Endolymphatic sac Endolymphatic sac drainagedrainage
Intratympanic injection of Intratympanic injection of steroidsteroid
Vestibular destructionVestibular destruction VIII nerve sectionVIII nerve section
Hearing destructionHearing destruction Intratympanic injection Intratympanic injection
gentamicingentamicin
LabyrinthectomyLabyrinthectomy

ITAGITAG

BPPV:BPPV:Benign Paroxysmal Position Benign Paroxysmal Position
VertigoVertigo Calcific debris in Calcific debris in
semicircular canalssemicircular canals CupulolithiasisCupulolithiasis CanalolithiasisCanalolithiasis
VertigoVertigo Brief (<1min)Brief (<1min) On head turn in a On head turn in a
particular directionparticular direction Typically self-Typically self-
limitinglimiting
PrimaryPrimary SecondarySecondary
Trauma (HI)Trauma (HI) Prolonged bed restProlonged bed rest Otological condition Otological condition
(up to 70%)(up to 70%) LabyrinthitisLabyrinthitis
CentralCentral

BPPV:BPPV:Benign Paroxysmal Position Benign Paroxysmal Position
VertigoVertigo Posterior SCCPosterior SCC
In plane on lying in In plane on lying in bedbed
Hallpike’s testHallpike’s test Nystagmus on lying Nystagmus on lying
back to one sideback to one side
Problem: how to Problem: how to distinguish BPPV distinguish BPPV from central causesfrom central causes

BPPV:BPPV:Hallpike’s test – Character of Hallpike’s test – Character of
NystagmusNystagmus
BPPVBPPV CentralCentral
Latency 5-10s None
Adaptation Gone in 50s Persists
Fatiguable Yes No
Vertigo Always Absent
Direction Rotatory (geotropic) Variable
Incidence Common Rare

BPPV - EpleyBPPV - Epley
Epley, 1992

BPPV - Brandt & DaroffBPPV - Brandt & Daroff
Brandt & Daroff, 1980
MigraineMigraine Clinical featuresClinical features
family historyfamily history motion intolerancemotion intolerance Vertigo occurs with classical headacheVertigo occurs with classical headache ENT/vestibular examination usually NADENT/vestibular examination usually NAD
Lifestyle changeLifestyle change exercise, diet, avoidance of stimulantsexercise, diet, avoidance of stimulants
Medication:Medication: Abortive therapy eg. SumatriptanAbortive therapy eg. Sumatriptan Prophylactic therapy eg. B blockersProphylactic therapy eg. B blockers

Vertebrobasilar InsufficiencyVertebrobasilar Insufficiency
Vertigo, diplopia, dysarthria, ataxia, Vertigo, diplopia, dysarthria, ataxia, sensory and motor disturbancesensory and motor disturbance
NOTNOT synonymous with cervicogenic synonymous with cervicogenic vertigovertigo
30% of TIA’s30% of TIA’s AspirinAspirin

DizzinessDizziness
Paul ChatrathPaul ChatrathConsultant ENT SurgeonConsultant ENT SurgeonQueen’s/King George’s Queen’s/King George’s HospitalsHospitals
Any Questions?
Email:Email:[email protected]@bhrhospitals.nhs.uk
[email protected]@chatrath.com

A Final Thought......A Final Thought......
QQ In a patient with vertigo, if you In a patient with vertigo, if you had had only one question to ask him/her, only one question to ask him/her, what what would it be?would it be?
AA How long does the vertigo last for?How long does the vertigo last for?- BPPV- BPPV SecondsSeconds
- Meniere’s- Meniere’s HoursHours
- Labyrinthitis- Labyrinthitis DayDay

















