38
DM & CKD Dr. Shahrzad Shahidi Professor of Nephrology Isfahan University of Medical Sciences
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | russell-murphy |
| View: | 217 times |
| Download: | 0 times |

DM & CKD
Dr. Shahrzad ShahidiProfessor of Nephrology
Isfahan University of Medical Sciences


CKD Kidney damage for ≥ 3 months, defined by
structural or functional abnormalities of the kidney, ± decreased GFR, manifest by either:
Albuminuria (AER ≥ 30 mg/24 hs; ACR ≥ 30 mg/g Cr) Urine sediment abnormalities Electrolyte & other abnormalities due to tubular
disorders Abnormalities detected by histology Structural abnormalities detected by imaging Hx of kidney transplantation GFR < 60 mL/min/1.73 m2 for ≥ 3 months ± kidney
damage
3

If no other markers of
kidney disease, no CKDModerately increased
riskHigh risk
Very high risk
4

Diabetic Nephropathy
Incidence of ESRD Resulting from Primary
Diseases (1998)
43%
23%
12%
3%
19%
Diabetes
Hypertension
Glomerulonephritis
Cystic Kidney
Other Causes
Over 40% of new cases of end-stage renal disease (ESRD) are attributed to diabetes.
The 5-year mortality rate for a
dialysis patient with diabetic
nephropathy is 93%.
Dialysis for one patient costs
over $50,000 annually.

Diabetic NephropathyDN occurs in 35-40% of patients with
type I diabetes (IDDM) whereas it occurs only in 15-20% of patients with type II diabetes (NIDDM).
Definition or Criteria for diagnosis of DN Presence of persistent proteinuria in sterile
urine of diabetic patients with concomitant diabetic retinopathy & HTN.
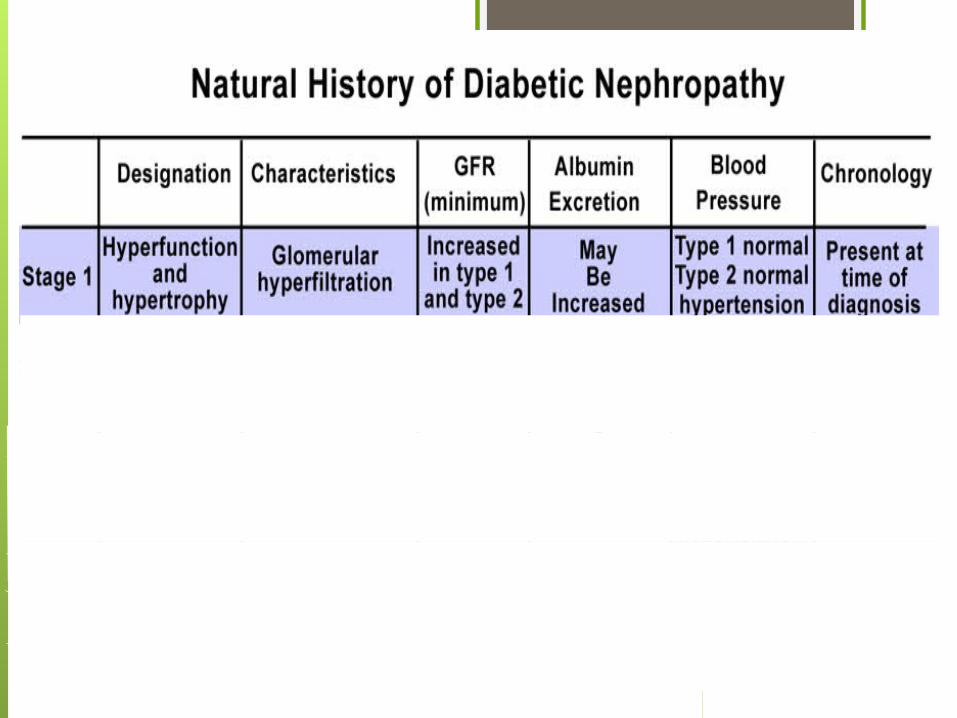

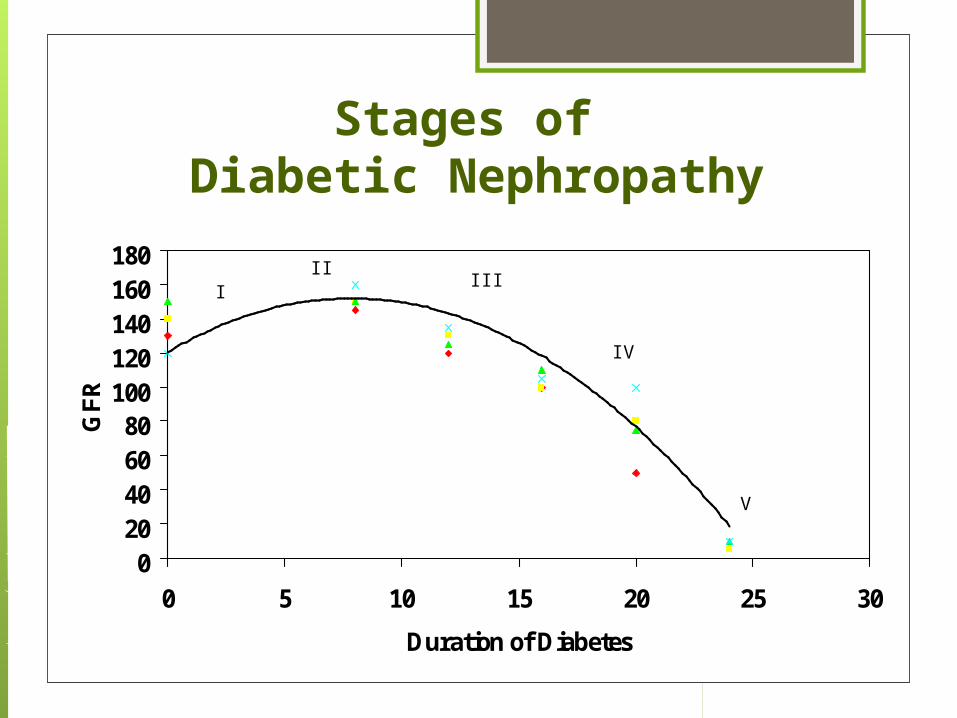
Stages of Diabetic Nephropathy
020406080
100120140160180
0 5 10 15 20 25 30
Duration of Diabetes
GF
R
III
III
IV
V

Nephropathy Risk Factors
DM Type & DurationPoor diabetic controlHTNRace (Aboriginal > Indian > Caucasian)SmokersFamily history

Nephropathy Risk Factors
ModifiableHbA1c, BP & total cholesterol Obesity, smoking
Non-modifiableAge, ethnicity
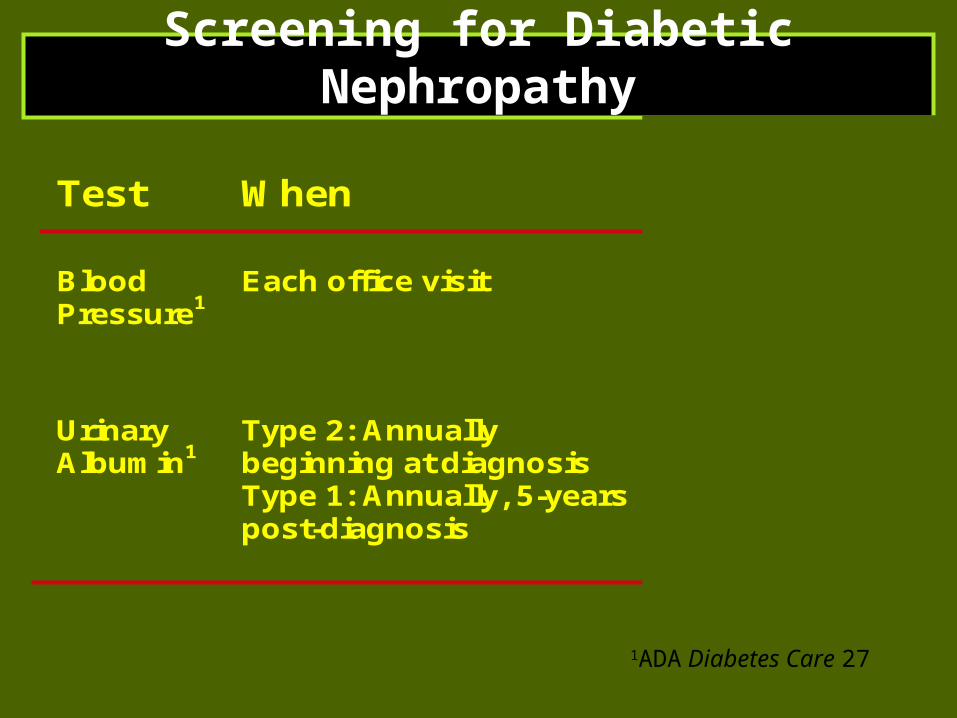
Screening for Diabetic Nephropathy
Test When Normal Range
BloodPressure1
Each office visit <130/80 mm/Hg
UrinaryAlbumin1
Type 2: Annuallybeginning at diagnosisType 1: Annually, 5-yearspost-diagnosis
<30 mg/day<20 g/min<30 g/mgcreatinine
1ADA Diabetes Care 27

Screening Measurements of urinary ACR in a spot urine sample.
Measurement of serum Cr & estimation of GFR.

How are we doing?
Studies show that primary care physicians screen only 20% of their
diabetic patients for diabetic nephropathy

MicroalbuminuriaSpot AM urine: Alb/Cr ratio 30-300
mg/g Cr*Timed urine collection: 20-200µg
albumin/min24 hour urine collection: 30-300 mg
albumin in 24 hours
*This is the most practical test
Incipient Nephropathy
IDDM2 out of 3 urine tests + for microalbuminuria Presence of proliferative diabetic retinopathy 80-90% of type 1 patients with microalbuminuria will progress to DN

Incipient Nephropathy
NIDDM2 out of 3 urine tests + for
microalbuminuria (start screening at the time of diagnosis of DM)
Presence of diabetic retinopathy20-30% may have diabetic nephropathy
but not diabetic retinopathy25% may have a diagnosis of
nephropathy other than diabetic nephropathy
Q. Which features are typical of diabetic CKD at presentation ?
Haematuria NoSmall scarred kidneys NoProgress to ESKD in <2yrs NoAssociated retinopathy Yesβ-blockers better than ACE-I Rx No

Other cause(s) of CKD should be considered in the presence
of any of the following circumstances:
Absence of diabetic retinopathyLow or rapidly decreasing GFRRapidly increasing Pruria or nephrotic
syndromeRefractory HTNPresence of active urinary sedimentSigns or symptoms of other systemic disease>30% reduction in GFR within 2-3 ms after
initiation of an ACE I or ARB.

Treatment of Diabetic Nephropathy (cont.)
Glycemic Control Preprandial plasma glucose 90-130 mg/dl
A1C ~ 7.0%Peak postprandial plasma glucose <180
mg/dl
Self-monitoring of blood glucose (SMBG)Medical Nutrition Therapy
Target dietary Pr intake for people with DM & CKD stages 1-4 should be the RDA of 0.8 g/kg/d.

Management of Hyperglycemia & General
Diabetes Care in CKDTarget HbA1c of ~ 7.0% to prevent or
delay progression of the microvascular complications of DM, including DKD.
Not treating to an HbA1c target of <7.0% in patients at risk of hypoglycemia.
Target HbA1c be extended above 7.0% in individuals with co-morbidities or limited life expectancy and risk of hypoglycemia.
Metformin in CKDNo hypoglucemia or weight gain InexpensiveBUT:
Renally-excreted Excess doses → anorexia, diarrhea Dose adjust to GFR: 2g to 250mg/day Protocol says
eGFR 30 – 45 max 1gm/day Cease when eGFR <30 but…
Risk of fatal lactic acidosis if unwell
Management of Dyslipidemia in Diabetes &
CKDUsing LDL-C lowering medicines, such
as statins or statin/ezetimibe combination, to reduce risk of major atherosclerotic events in patients with diabetes & CKD, including those who have received a kidney transplant.
Not initiating statin therapy in patients with diabetes who are treated by dialysis

Management of Albuminuria in Normotensive Patients with
Diabetes
Not using an ACE-I or an ARB for the primary prevention of DKD in normotensive normoalbuminuric patients with diabetes.
Using an ACE-I or an ARB in normotensive patients with diabetes & albuminuria levels >30 mg/g Cr who are at high risk of DKD or its progression.

BP management inCKD ND patients with DM
Adults with DM & CKD ND with urine albumin excretion < 30 mg/d whose office BP is consistently > 140 mmHg systolic or > 90 mmHg diastolic be treated with BP lowering drugs to maintain a BP that is consistently ≤140 mmHg systolic & ≤ 90 mmHg diastolic.
Adults with DM & CKD ND with urine albumin excretion > 30 mg/d whose office BP is consistently >130 mmHg systolic or > 80 mmHg diastolic be treated with BP lowering drugs to maintain a BP that is consistently ≤130 mmHg systolic & ≤ 80 mmHg diastolic.
ARB or ACE-I be used in adults with diabetes & CKD ND with urine albumin excretion of ≥ 30 mg/d.
Diabetes & ESRD
Reducing insulin requirementsDifficult vascular accessAccelerated macrovascular diseaseAdvanced microvascular diseaseFrequent sepsisSilent ischaemia2-3 x death rate vs non-DM patients

How can DM effect Dialysis?
Autonomic neuropathy – may suffer hypotension increased by large fluid shift in HD
Uncontrolled BS – may absorb some glucose in PD fluid
Severe PVD – difficult to get vascular access for HD
PVD may also affect peritoneum & reduce PD success
Increased risk of infections – problem in both Transplants – new kidneys develop nephropathy,
hence good glycaemic control important
Case #1Your first pient is a 25 y old young
man with a 5 year Hx of type 1 DM.His urine dipstick is negative for Pr. Spot AM urine Alb/Cr ratio is 19 mg/g Cr.
His BP is 112/66 mmHg. His HbA1C is 6.9%.

Which is (are) true?
1. The patient has early or incipient diabetic nephropathy.
2. The patient should maintain a HbA1C of less than 7 to help protect his kidneys.
3. You should start the patient on an ACE inhibitor to protect his kidneys.
4. All of the above are true.

Patient #2 43 y old woman with a 6 year
Hx of type 2 DM. A urine dipstich shows trace PrSpot AM urine ACR 390 mg/g Cr
BP is 135/80 HbA1C is 6.7%

Which is (are) not true?
1. You should check the patient’s serum Cr & K.
2. You should start the patient on an ACEI if her K & Cr are okay.
3. You should check a 24 hour urine for total Pr & Cr clearance.
4. The patient has overt diabetic nephropathy & should be referred to a nephrologist.

Case #360 y old man with HTN, dyslipidemia
& newly diagnosed type 2 DM. A urine dip shows 2+ Pr He has a fever & his HbA1C is 10.3%
BP is 140/88 He is taking HCTZ & Glipizide

Which is (are) true?
1. You should get the patient’s diabetes under better control before rechecking his urine.
2. A fever will not cause proteinuria.3. The patient’s BP is under good
control.4. You should check the patient’s K
& Cr.

Case #3
3 months later with exercise, metformin & Enalapril your patient’s HbA1C is now 7.5 & his BP is 135/85.
A urine dip now shows 1+ protein.
Which is (are) true?
1. You should check a 24 hour urine for total Pr & Cr. cl.
2. A spot AM urine ACR correlates well with a 24 hour urine for total Pr
3. The patient likely already has diabetic nephropathy & should be referred to a nephrologist.

Use the Algorithm!
Check all your diabetic patients annually for renal disease .
Help your diabetic patients’ protect their kidneys by helping them keep their diabetes under control.
Help your diabetic patients protect their kidneys by helping them keep their BP under control.




![WHITTAKER MODELS FOR REAL GROUPSfshahidi/articles/Shahidi [1980, 27pp]---Whitt… · WHITTAKER MODELS FOR REAL GROUPS FREYDOON SHAHIDI Introduction. Whittaker functions were first](https://static.documents.pub/doc/80x56/5f6ff2171fdfde08b537c325/whittaker-models-for-real-fshahidiarticlesshahidi-1980-27pp-whitt-whittaker.jpg)














