23


Does Managed Care Reduce Federal Spending?
Evidence from Medicare
Lauren Hersch Nicholas
University of Michigan
Population Studies Center Research Report 09-671
Lauren Hersch Nicholas, University of Michigan. Email: [email protected]. This work has benefited from helpful comments from Sherry Glied, Janet Currie and Irv Garfinkel. I thank the Agency for Healthcare Research and Quality (grant R36HS016836-01A1), the John A. Hartford Foundation, and the National Institute on Aging (grant ) for financial support. This research does not represent the official views of the funders.

Does Managed Care Reduce Federal Spending? 2
ABSTRACT Although Medicare Managed Care (MMC) was introduced as a way to reduce costs, the effect of the program on total Medicare spending is unknown. Current literature has focused on three conflicting sets of findings including spillover effects from managed care which reduce total Medicare spending and positive selection into managed care and overpayments to managed care plans relative to Fee-for-Service (FFS) spending, which increase spending. This research reconciles these results by examining the effects of Medicare managed care penetration on total county-level Medicare spending for elderly beneficiaries from 1999 - 2004. Using an instrumental variables approach, I find that a one percentage point increase in Medicare managed care penetration increases total county Medicare spending by 1.1 percent, $2.6 billion in 2004 dollars. There is no evidence of cost-reducing spillovers from MMC penetration to FFS. Increases in FFS spending likely caused by positive selection into MMC account for 40 percent of the increase in costs, the remainder is built in by federal payment policy to MMC plans.

Does Managed Care Reduce Federal Spending? 3
INTRODUCTION
Medicare trustees have repeatedly called attention to the impending financing problems
in the Medicare program and highlighted the need to reduce spending growth. In 2008, the
Trustees issued a “Medicare Funding Warning,” which requires the President to submit
legislation to Congress to be considered on an expedited basis to reduce the share of Medicare
financing coming from general revenue (Boards of Trustees, 2008). To achieve this goal,
policymakers must find ways to reduce Medicare costs or increase dedicated funding by raising
payroll taxes on current workers or increasing premiums and cost-sharing charged to
beneficiaries. With the latter options likely to be politically unpopular, reforms to reduce
program costs may play an important role in shaping Medicare’s future and ensuring continuing
benefit availability for the elderly and disabled.
Managed care is believed to be one way to control Medicare costs without reducing
benefits. Medicare beneficiaries enrolling in the Medicare managed care (MMC) program
currently known as Medicare Advantage accept managed care network restrictions in exchange
for plans offering reduced cost sharing or extra benefits. This has been a way for lower-income
beneficiaries without access to other supplemental insurance to gain additional benefits and
services, though critics point out that the program does not necessarily target benefits to those
with the greatest medical or financial need (GAO, 2008). While MMC was introduced as a way
to reduce costs, the effect of the program on total Medicare spending is unknown. Existing
empirical literature has focused on three conflicting effects: spillover effects from managed care
which reduce total Medicare spending and positive selection into managed care and
overpayments to managed care plans relative to Fee-for-Service (FFS) spending, which increase
total Medicare spending. This research captures the net of all thee effects by examining the
effects of Medicare managed care penetration on total county-level Medicare spending for
elderly beneficiaries.
Managed care organizations can affect the treatment of managed care enrollees and
“spillover” to influence the treatment of non-managed care patients in the same market through
several channels. Baker (1997) classifies these effects as those resulting from competition,
changes in market structure, learning and practice association effects. Several papers have noted
that Medicare-specific spillovers are likely to operate primarily through learning and practice

Does Managed Care Reduce Federal Spending? 4
effects since the Medicare market share is unlikely to be large enough to alter the structure of
most markets (Welch, 1994, Baker, 1997). Managed care companies provide incentives to treat
covered patients certain ways, which may cause spillovers for non-managed care patients if
providers treat all patients in a similar fashion. Models of physician learning suggest diffusion of
managed care practices across provider groups (Phelps, 1992; Baker, 1997).
Earlier studies have found significant spillover effects of Medicare managed care in FFS
expenditures, hospital costs, and treatment patterns (Baker, 1997; Gaskin and Hadley, 1997;
Bundorf et al., 2004). Welch (1994) showed that early MMC activity decreased overall
Medicare spending; a 10 percent increase in MMC enrollment was associated with a weakly
significant decline in per-beneficiary Medicare spending of 1.2 to 3.9 percent in MSA-level data
from 1984-1987. A related literature has considered the effects of market level managed care
penetration (including commercial, Medicare and Medicaid penetration) on market level and
Medicare-specific outcomes, particularly showing that higher HMO penetration is generally
associated with increased use of preventative services for HMO and non-HMO enrollees (Baker
et al., 2004; Zhan et al, 2003). Emphasizing preventative care is one way that managed care may
cause cost-reducing spillovers.
The existing spillover literature relies on older data; the most current of these (Chernew
et al, 2008) uses individual-level data for FFS beneficiaries through 2001. Since then, managed
care generally and Medicare managed care particularly have evolved to include more flexible
variants such as Preferred Provider Organizations and private Fee-for-Service plans. Network,
gatekeeper and prior authorization practices have become less restrictive following the managed
care backlash (Encinosa and Hagan, 2006; Federman and Siu, 2004). Under this environment,
spillover effects may be less likely as practice styles under managed care and FFS converge.
Bundorf et al. show that competitive managed care markets increase FFS costs, suggesting that
spillover effects are unlikely in markets where plans must compete for providers since plans will
have less leverage to influence behavior. Spillovers from MMC penetration may instead lead to
increased costs in FFS if providers induce demand from non-managed care patients to make up
for lost revenue (McGuire and Pauly, 1991).
A second body of research has considered the role of positive selection into Medicare
managed care and plan payment policy in raising Medicare costs. This occurs when payments to
managed care plans exceed the costs of covering beneficiaries who choose MMC plans under

Does Managed Care Reduce Federal Spending? 5
FFS. Prior to 1998, plans received fixed per-beneficiary payments set at 95 percent of expected
county-level FFS spending. However, MMC enrollees were healthier than FFS stayers on
average, with costs for the average Medicare managed care enrollee estimated at between 85 and
87 percent of average county costs (CMS, 1999). Buntin et al. (2004) show that this is partially
because of lower enrollment of decedents, who are very costly on average, in MMC plans.
The 1997 Balanced Budget Act (BBA) divorced MMC payment rates from average
county costs as a way to reduce geographic variation in payments and overpayments to plans
(Berenson, 2004). However, subsequent reforms to encourage continued plan participation
resulted in plan payment rates that exceeded average FFS spending in every county by 2004
(Biles et al., 2004b). MMC plan payment rates are currently 113 percent of average FFS costs
(MedPAC, 2008). Although only a minority of beneficiaries choose the MMC option,
enrollment has been rapidly growing in recent years and currently covers more than twenty
percent of the Medicare population. The MMC program will only reduce overall Medicare
spending if spillover effects from MMC to FFS are large enough to counteract the higher
payments to plans for these enrollees.1
I directly test whether MMC penetration affects total spending by regressing logged
average per enrollee spending (a weighted average of FFS spending and the MMC payment rate)
at the county level on MMC penetration and other county level characteristics using data from
1999 through 2004. Using an instrumental variables approach that identifies managed care
penetration using variation in expected plan profits caused by the BBA legislation and Centers
for Medicare and Medicaid Services (CMS) projections, I find that a one percentage point
increase in MMC penetration increases average per-beneficiary Medicare spending by 1.1
percent, about $72 in 2004.
DATA
I use six years of county-level Medicare spending, payment rate and enrollment data from
the Centers for Medicare and Medicaid Services merged with county-level health systems
characteristics from the Area Resource File and Health Leaders Interstudy data. The sample
includes 3,108 counties within the continental United States observed annually between 1999
1 Higher payments result mechanically through the legislated rates and from any remaining positive selection that is not addressed by risk-adjustment at the individual level.

Does Managed Care Reduce Federal Spending? 6
and 2004. The key dependent variable is average per-enrollee Medicare spending. This is a
weighted average of average FFS spending (normalized to reflect spending for a beneficiary of
“average” risk2) and Federal spending on MMC enrollees, which is the MMC payment rate
inflated to account for double payments of graduate medical education for MMC enrollees
calculated as follows
AveSpendc,t = λc,t *(Rate c,t*(1+.65*GME c))+((1-λc,t)*FFSc,t/Democ,t) (1)
where λ denotes the MMC penetration rate, Rate is the MMC plan payment rate for an average
(risk score = 1), GME is the graduate medical education carve-out factor, FFS is average per
capita FFS spending, and Demo is the average demographic risk score of FFS enrollees in the
county calculated by CMS.3 Normalizing by risk score enables direct comparison of
beneficiaries across MMC and FFS within and across counties, addressing the selection bias that
could result from healthier beneficiaries living in counties that may have higher rates of managed
care penetration (Spitalnic, 2008).
Table 1 presents descriptive statistics. Average monthly per-enrollee spending is $545
during the study period, and exhibits a right-skew characteristic of health expenditure data,
reaching a maximum value of $1,067 in Miami-Dade county in 2004. Average monthly per-
enrollee total Medicare spending is slightly higher than average FFS per enrollee spending $521
per month). This reflects the concentration of MMC enrollment in urban areas with higher costs
of care as well as higher payments to managed care plans relative to FFS in some years. By
2004, payments to plans averaged 107 percent of FFS spending in the same counties (MedPAC,
2004). MMC penetration averages 15 percent nationwide.
I control for average demographic characteristics of Medicare beneficiaries which will
affect demand for managed care and the cost care including age, sex, race, the portion of elderly
beneficiaries eligible for Medicaid and the proportion disabled prior to age 65. County
2 The Centers for Medicare and Medicaid Services assign risk beneficiaries scores which are used to risk adjust payments to plans. During the study period, these are largely based on demographic characteristics and eligibility for other Federal programs. A score of 1 corresponds to average risk, with lower scores indicating healthier beneficiaries. 3 Graduate medical education payments essentially paid twice for MMC enrollees. They are built into the MMC payment rates, but also reimbursed by CMS directly for MMC enrollees. In order to account for full Federal spending, it is necessary to account for the GME double payments (Spitalnic, 2008). Following guidance from MedPAC, I estimate the additional GME amount as two-thirds of the county-level GME carve-out factor (see Biles et al., 2004b for more on this methodology).
Does Managed Care Reduce Federal Spending? 7
characteristics are calculated using CMS enrollment data for FFS and MMC enrollees.
Additional county level variables which have been shown to affect managed care penetration and
health care costs in other studies are included from the Area Resource File including per capita
income, number of total physicians, general practitioners, hospitals and ambulatory surgery
centers per capita (Abraham et al., 1999; Cawley et al., 2005; Chernew et al., 2008; Zhan et al.,
2004).
METHODS
Empirical Approach
County-level Medicare spending and enrollment data are used to estimate regressions of
the form
ln(AveSpendc,t) = γMMCPenc,t + βXc,t + C + Y + εc,t (2)
where AveSpend indicates total average Medicare spending on elderly beneficiaries in the
county, X is a vector of Medicare beneficiary and county health systems characteristics, C is a
vector of county effects and Y is a vector of year effects. Since average per-beneficiary
Medicare spending is is heavily skewed to the right, I take the natural log to normalize the
distribution.
Endogeneity of Managed Care Penetration
As earlier papers have noted, while inclusion of county fixed effects address time-
invariant county-level omitted variables, it is likely that other, time-varying unobserved county
level factors affect both MMC penetration and total county spending, resulting in correlation
between εc,t and MMCPenc,t (Baker, 1997; Chernew et al., 2008). An estimation strategy that
does not address this endogeneity will result in biased estimates of γMMC. Estimates may be
biased upward if plans are more likely to enter markets (and attract beneficiaries) with high
average health care spending and utilization, or biased downward if higher penetration counties
are healthier and lower cost. This is addressed through the use of an instrumental variables
strategy to identify county-level MMC penetration.
The IV approach requires one or more instruments which affect MMC penetration and
only affect average total Medicare spending through their effect on penetration. Under the BBA
Does Managed Care Reduce Federal Spending? 8
payment regime, county-level payment rates to MMC plans are set by a Federal formula. I use
an estimate of expected HMO profits in a particular county-year based on these payment rates
and information released by CMS in the Fall of the preceding year. Each year, CMS reports
payment rates to plans and methodology for calculating the county-specific blend rate, which is
based on national and local estimates of FFS spending trends. These data enable a calculation of
expected average county FFS spending for the coming year.4 The difference between the plan
payment rate and the projection provide a rough measure of expected per enrollee profit (loss) to
the managed care plan.5 MMC penetration should increase in areas where plans expect higher
profits, since this may improve plan availability and benefit package generosity. Projections of
greater profit should only affect actual average per-enrollee spending through the effect on
managed care penetration, which will affect both true average FFS spending and the proportion
of beneficiaries whose care cost are set at the MMC payment rate.
MMCPenc,t = α1Exp_Pinc,t + βXc,t + C + Y + ηc,t (3)
Fitted values from Equation (3) are used to generate unbiased estimates of the effect of
MMC penetration on total Medicare spending. Models are estimated with and without
commercial HMO penetration, which may also create system-level spillovers which affect total
Medicare costs, but may be jointly determined with MMC penetration (Abraham et al., 2000).6
All models are estimated using analytic weights based on the number of Medicare beneficiaries
in the county to improve reliability since average spending values in smaller counties are
sensitive to a small number of very high-spending FFS enrollees. Standard errors are robust to
heteroskedasticity and county autocorrelation.
Spillovers to FFS
MedPAC, the Congressional oversight agency for the Medicare program has a supported
a principle of fiscal neutrality for the MMC program, arguing that managed care provides an
4 At the national level, this methodology accurately predicts average FFS spending, though there is considerable variation in accuracy at the county level. 5 This calculation cannot account for firm-specific factors such as administrative costs that would affect the true profit amount. See MedPAC (1999) for further details on calculation methodology. 6 Previous papers have instrumented for commercial managed care using the number of large employers in the county or MSA. During the study period, there is insufficient variation in this measure to identify HMO penetration.

Does Managed Care Reduce Federal Spending? 9
important choice for beneficiaries, but per-enrollee outlays for Medicare should be the same
whether the beneficiary chooses MMC or FFS (MedPAC, 2008). Chernew et al. (2008) point
out that optimal MMC payment strategies should account for spillovers to FFS with higher
payments to MMC plans to further encourage enrollment. Higher payment rates may raise costs
by more than can be offset by enrollment-related spillover effects. An overall reduction is
spending is most plausible in years where managed care payment rates are close to average FFS
spending. In years where MMC payment rates exceed average FFS spending, spillover effects
must be large in magnitude to counteract the mechanical increase in spending induced by moving
a beneficiary into MMC and lower costs on net.
To further understand the mechanics of the relationship between payment rates and the
components of total Medicare spending, I replicate Chernew et al.’s models using county-level
FFS data.
ln(AveFFSc,t) = γMMCPenc,t + βXc,t + C + Y + εc,t (4)
I estimate IV models using expected profit as well as the MMC payment rate to instrument for
MMC penetration.
Robustness Checks
I consider several robustness tests of these results. I first limit the sample to counties
with MMC penetration rates of at least 10% since higher levels of managed care activity may be
necessary to influence market dynamics. Several other checks are performed using the full
sample. I include the Herfindahl Index calculated for the MMC market to determine whether the
the MMC term is proxying for another market factor. I also estimate Models (2) and (3) for
inpatient (Part A) and outpatient (Part B) expenditures separately since the managed care effect
may be heterogeneous across types of utilization, for example influencing practice styles that
reduce inpatient utilization and increase outpatient preventative service use.
Use of the log transformation for average Medicare spending introduces potential bias
because of the heteroskedasticity in these data. Several recent papers recommend use of General
Linear Models, which instead model the expected conditional mean, E(Spend) = exp(Xβ) to
avoid this bias (Mullahy 1998; Manning and Mullahy, 2001; Buntin and Zaslavsky, 2004; Afifi
et al., 2007). Following diagnostic procedures recommended in Manning and Mullahy (2001), I
re-specify Equation (3) as a GLM model with a log link and a gamma distribution.

Does Managed Care Reduce Federal Spending? 10
RESULTS
OLS Results
In the base specification of Equation (2), a one percentage point increase in MMC
penetration is associated with a 0.3% increase in total average Medicare per-enrollee spending
(Table 2). The OLS results unexpectedly suggest that total Medicare spending is lower in
counties with older beneficiaries and those with a larger proportion of Blacks. All coefficients
are robust to the inclusion of commercial HMO penetration, which has a negative effect on
average spending (i.e. through spillovers from commercial managed care activity). I will thus
interpret specifications including this variable due to its theoretical relevance.
Endogeneity of MMC
As previously discussed, this may overstate or understate the true effect of MMC
penetration. Expected MMC plan profit can be used to instrument for MMC penetration. In the
first stage, a $1 increase in expected MMC plan profit per enrollee per month increases MMC
enrollment by .03 percentage points. This relationship is statistically significant, and the first
stage F statistic of 43.9 exceeds the minimum value of 10 suggested by Staiger and Stock (1997)
to avoid the weak instruments problem.
The second requirement of the instrument requires that expected profits only affect total
Medicare spending through the effect on MMC enrollment. If this were a true measure of the
difference between MMC and FFS spending, it would mechanically increase or decrease average
spending in proportion to MMC penetration. By using an estimate made before actual FFS
spending occurs, we avoid this concern. The actual difference between MMC and FFS spending,
and resulting average spending calculation, will reflect FFS spending based on the enrollment
response to managed care availability. If plans anticipate higher payments relative to the cost of
providing care, they are required to offer additional benefits. These benefits may attract sicker
FFS enrollees to MMC, lowering average FFS spending.
IV results show that MMC penetration plays a larger role in increasing total average
Medicare spending than the OLS results indicate. Table 2 presents both sets of results. A one
percentage point increase in MMC penetration increases total average spending by 1.1 percent,
or $72 per year. This is economically as well as statistically significant; in 2004 this corresponds

Does Managed Care Reduce Federal Spending? 11
to a $2.6 billion increase in Medicare spending for every one percentage point increase in MMC
penetration. I find small spillover effects from commercial HMO penetration; a 10 percentage
point increase in commercial enrollment decreases average Medicare spending by 0.9 percent.
Spillovers to FFS
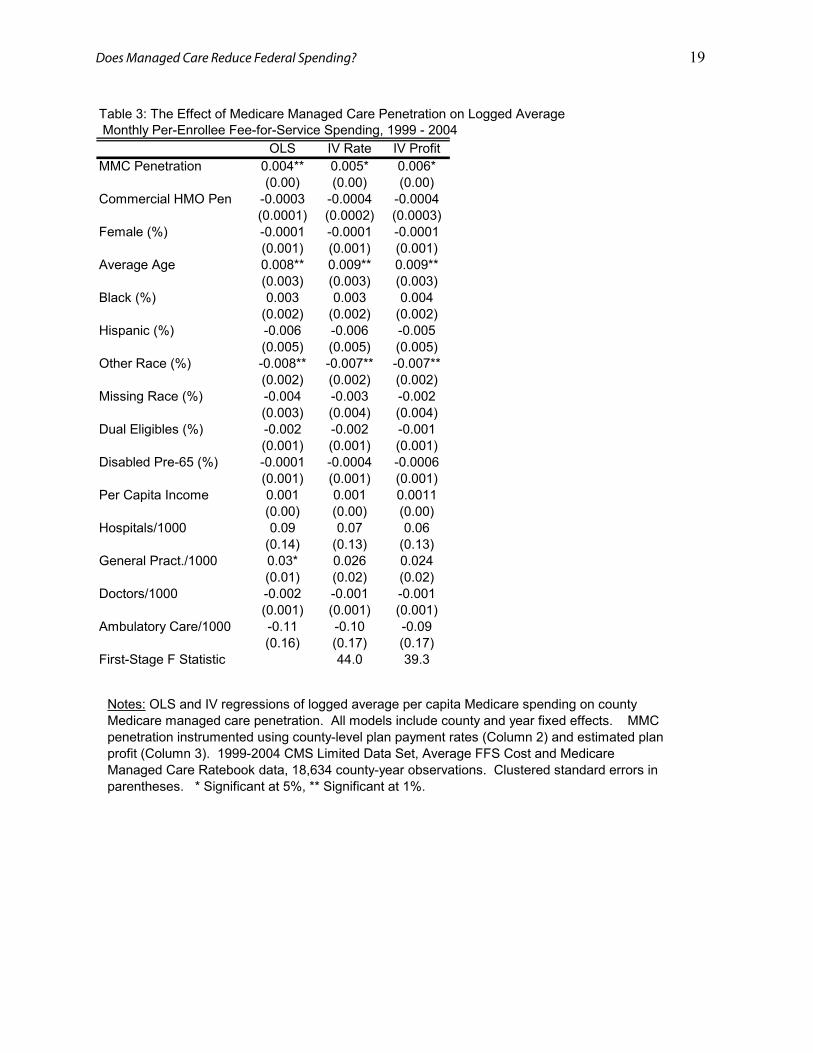
I find no evidence that spillover effects from MMC penetration persist in recent years.
OLS and IV estimates using the MMC payment rate and the estimated profit measure are similar,
finding that a one percentage point increase in MMC penetration increases average FFS spending
by 0.5 percent (Table 3). Spillovers are unlikely in a period where plans are less able to
influence physician practice, particularly if positively selected MMC enrollees require less health
care. With 85 percent of the sample remaining in FFS during the study period, the IV estimates
indicate that between 35 and 46 percent of the increase in average spending due to MMC
penetration can be attributed to effects on FFS spending. Average FFS costs would be lower if
the healthiest enrollees remained in the risk pool. The remainder of the increase likely results
from BBA and MMA payment policy to plans.
Robustness
Table 4 reports several robustness checks. While Baker (1997) showed that spillovers
were greatest in markets with at least 15 percent penetration, I find that MMC penetration further
increases average total spending in markets with greater MMC activity. In markets with
penetration rates of at least 10 percent, each 1 percent increase raises average spending by 2.8
percent, more than double the point estimate using all counties.
Results are unchanged when I control for the degree of competition of the MMC market
using the Herfindahl index, although I replicate Bundorf et al.’s (2004) finding of higher
spending in more competitive markets.
MMC penetration increases spending on both inpatient and outpatient care. The increase
in Part B (outpatient) spending is larger (1.9 percent versus 1 percent), though outpatient
spending accounts for only 40 percent of total average spending.
Findings are also robust to the GLM specification. The IV coefficient corresponds to a
1.2 percent increase in total average spending for every 1 percent increase in MMC penetration.

Does Managed Care Reduce Federal Spending? 12
CONCLUSION
Though Medicare managed care was introduced as a way to reduce total Medicare
spending, recent work highlights the effects of plan payment policy on raising program spending.
MedPAC, the Congressional oversight agency for the Medicare program has advocated reducing
payments to MMC plans, though some analysts suggest that high payment rates may be optimal
to encourage enrollment due to cost-reducing spillovers to the FFS sector (MedPAC, 2008;
Chernew et al., 2008). I test these competing hypotheses by focusing on the effect of MMC
penetration on total average Medicare spending and find that between 1999 -2004 MMC is not
reducing total Medicare spending. A one percentage point increase MMC penetration increases
average Medicare costs by $72 per beneficiary per year.
As this paper relies on aggregate, county level data, several important questions remain
unanswered that should guide policy implications of these findings. Although the additional
spending associated with a 1 percentage point increase in MMC is relatively trivial, large
increases in enrollment, such as moving from 10 percent to 20 percent at the county level
become economically significant, particularly given Medicare’s projected funding shortfalls.
Higher spending on MMC plans partially covers reduced cost sharing for enrollees. A recent
GAO (2008) report found that average out-of-pocket spending for MMC enrollees was 42
percent of what it would have been had they remained in FFS, but cautioned that spending is not
lower for all enrollees. MMC payment policy concentrates additional benefits on these
enrollees, but increases spending (through Part B premiums) for all beneficiaries. Thus it is
important to understand who the marginal Medicare beneficiary is who in induced to join MMC
by the payment policy variables considered. Increased spending on MMC is likely to be more
attractive if the program is an effective way to target lower-income Medicare beneficiaries
whose income is too high for Medicaid but face significant out-of-pocket health care costs, for
example.
Several recent changes to the MMC program raise questions about the generalizability of
these results to more recent years. Payments to MMC plans have further increased as a
percentage of average FFS spending. On average payment rates were 107 percent of expected
FFS spending in 2004, this figure has increased to 113 percent in 2008 (MedPAC, 2004; 2008).
As payments rates for MMC enrollees rise relative to FFS costs, the estimated effect of MMC
penetration on total average spending should rise relative to these results. During the study

Does Managed Care Reduce Federal Spending? 13
period, virtually all MMC enrollees are enrolled in an HMO. Most of the recent growth in
enrollment has been in less restrictive forms of managed care including preferred provider
organizations and private fee-for-service plans. The latter options due little care management or
coordination of care, so it is unlikely that higher penetration of these plans will generate spillover
effects to FFS. In light of these factors, estimates should be viewed as a lower bound estimate of
the current relationship between managed care penetration and Medicare spending.
While the MMC program did not reduce Federal Medicare spending during the study
period, it is likely to have reduced individual out-of-pocket spending for some beneficiaries. The
program has been characterized by geographic inequity in financing and benefit provision (Biles
et al., 2004a). Thus the benefits of the program are neither uniform for all Medicare
beneficiaries or across those enrolling in the program. As policymakers consider new ways of
reducing costs in the Medicare program, there is a clear need to assess whether alternatives to
MMC can more efficiently target additional program spending to low-income beneficiaries
(GAO, 2008). The Medicare Trustees have charged Congress and the President to identify ways
of improving Medicare’s financing. Results of this paper suggest that initiatives to bolster the
role of managed care, one of the few large-scale reforms tested thus far, will not be an effective
way of meeting this goal.

Does Managed Care Reduce Federal Spending? 14
REFERENCES
Abraham, J., A. Arora, M. Gaynor and D. Wholey. (2000). “Enter at your own risk: HMO participation and enrollment in the MedicareRisk market.” Economic Inquiry, 38, 3 385-401.
Afifi, A. A., J. B. Kotlerman, S. L. Ettner, and M. Cowan. (2007). “Methods for improving regression analysis for skewed continuous or counted responses,” Annual Review of Public Health, 28, 95-111.
Baker, L. C. (1997). “The effect of HMOs on fee-for-service health care expenditures: evidence from Medicare,” Journal of Health Economics, 16, 453-481.
Baker, L.C., K.A. Phillips, J.S. Haas, S. Liang and D. Sonneborn. (2004). “The effect of area HMO market share on cancer screening,” Health Services Research, 39, 6, 1751–1772.
Batata, A. (2004). “The effect of HMOs on fee-for-service health care expenditures: evidence from Medicare revisited,” Journal of Health Economics, 23, 6, 951-963.
Berenson, R. A. (2004). “Medicare Disadvantaged and the search for the elusive ‘level playing field’,” Health Affairs, W4-572 – W4-585.
Biles, B., G. Dallek, and L. Nicholas (2004a). “Medicare Advantage: Déjà Vu All Over Again? Health Affairs, W4-586 – W4-597.
Biles, B., L. H. Nicholas, and B. Cooper. (2004b). “The Cost of Privatization: Extra Payments to Medicare Advantage Plans: 2005 Update.” New York: The Commonwealth Fund.
Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. (2008). 2008 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Funds. Available at http://www.cms.hhs.gov/ReportsTrustFunds/downloads/tr2008.pdf. Accessed 24 April 2008.
Bound, J., D. A. Jaeger and R. Baker (1995). “Problems with instrumental variables estimation when the correlation between the instruments and the endogenous explanatory variable is weak,” Journal of the American Statistical Association, 90, 433-450.
Bundorf, M. K., K. A. Schulman, J. A. Stafford, D. Gaskin, J. G. Jollis, and J. J. Escare (2004). “Impact of Medicare managed care on the treatment, costs, and outcomes of Fee-for-Service Medicare patients with acute myocardial infarction,” Health Services Research, 39, 1, 131-152.
Buntin, M. B. and A. M. Zaslavsky. (2004). “Two much ado about two-part models and retransformation?: Comparing methods of modeling Medicare expenditures,” Journal of Health Economics, 23, 3, 525-542.
Buntin, M. B., A. Garber, M. McClellan and J.P. Newhouse. (2004). “The costs of decedents in the Medicare program: Implications for payments to Medicare+Choice plans,” Health Services Research, 39, 1, 111-130.
Centers for Medicare and Medicaid Services Office of Public Affairs (1999). Fact Sheet: Managed care and Medicare, Accessed 5 May 2006.
Centers for Medicare and Medicaid Services Office of Public Affairs (2005b). Fact sheet: “Health status of beneficiaries enrolled in Medicare Advantage plans appears more similar to beneficiaries in Fee-for-Service.” Available online. Accessed 3 April 2, 2007.
Chernew, M., P. DiChicca and R. Town (2008). “Managed care and medical expenditures of Medicare beneficiaries,” NBER Working Paper 13747.
Congressional Budget Office (2007). “The Medicare Advantage program: Trends and options,” Testimony before the Subcommittee on Health, Committee on Ways and Means, U.S. House of Representatives. 21 March 2007.
Encinosa, W. and M. Hagan. (2006). “AHRQ research on health care markets,” Medical Care Research and Review, 63, Supplement 6, 3S-8S.
Does Managed Care Reduce Federal Spending? 15
Federman, A.D. and A. L. Siu. (2004). “The challenge of studying the effects of managed care as managed care evolves,” Health Services Research, 39, 1, 7-12.
Fisher, E. S., D.E. Wennberg, T. A. Stukel, D. J. Gottlieb, F. L. Lucas, E. L. Pinder (2003). “The implications of regional variations in Medicare spending. Part 1: The content, quality, and accessibility of care,” Annals of Internal Medicine, 138, 4, 273-287.
Fisher, E. S., D.E. Wennberg, T. A. Stukel, D. J. Gottlieb, F. L. Lucas, E. L. Pinder (2003). “The implications of regional variations in Medicare spending. Part 2: Health outcomes and satisfaction with care,” Annals of Internal Medicine, 138, 4, 288-298.
Gaskin, D.J. and J. Hadley (1997). “The impact of HMO penetration on the rate of hospital cost inflation, 1985-1993,” Inquiry, 34, 205 -216.
General Accounting Office (2008). “Medicare Advantage: Higher spending relative to Medicare Fee-for-Service may not ensure lower out-of-pocket costs for Beneficiaries,” Testimony before the Subcommittee on Health, Committee on Ways and Means, U.S. House of Representatives. 28 February 2008.
Greene, W.H. (1997). Econometric Analysis. Upper Saddle River: Prentice Hall. Hardin, J. W. (2002). “The robust variance estimator for two-stage models,” The Stata Journal, 2, 3, 253-
266. Hardin, J. W., H. Schmeidiche, and R. J. Carroll. (2003). “Instrumental variables, bootstrapping, and
generalized linear models, The Stata Journal, 3, 4, 351-360. Hole, A. R. (2006). “Calculating Murphy-Topel variance estimates in Stata: A simplified procedure,”
Stata Journal, 6, 4, 521-529. Manning, W. G. (1998). “The logged dependent variabl, heteroskedasticity, and the retransformation
problem,” Journal of Health Economics, 17, 3, 283-295. Manning, W. G., A. Basu and J. Mullahy (2005). “Generalized modeling approaches to risk adjustment
of skewed outcomes data,” Journal of Health Economics, 24, 3, 465-488. Manning, W. G. and J. Mullahy. (2001). “Estimating log models: to transform or not to transform?”
Journal of Health Economics, 20, 4, 461-494. McGuire, T. G. and M. V. Pauly. (1991). “Physician response to fee schedules with multiple payers,”
Journal of Health Economics, 10, 4, 385 – 410. MedPAC. (1999). Report to the Congress: Medicare Payment Policy. Washington, DC: MedPAC. MedPAC. (2008). Report to the Congress: Medicare Payment Policy. Washington, DC: MedPAC. Mullahy, J. (1998). "Much ado about two: reconsidering retransformation and the two-part model in
health econometrics," Journal of Health Economics, 17, 3, 247-281. Phelps, C. (1992). “Diffusion of information in medical care,” Journal of Economic Perspectives, 6, 1,
23-42. Shang, B. and D. Goldman. (2008). “Does age or life expectancy better predict health care
expenditures?” Health Economics, 17, 4, 487-501. Spitalnic, P. (2008). Note to Medicare Advantage organizations and other interested parties. Available at
http://www.cms.hhs.gov/MedicareAdvtgSpecRateStats/Downloads/FFS-Data-2006.pdf. Accessed 7 March 2008.
Staiger, D. and J. H. Stock. (1997). “Instrumental variables regression with weak instruments,” Econometrica, 65, 556-587.

Does Managed Care Reduce Federal Spending? 16
Stock, J. H. and M. Yogo. (2005). “Testing for weak instruments in linear IV regression,” in D.W.K. Andrews and J.H. Stock, eds. Identification and Inference for Econometric Models, New York: Cambridge University Press.
Stock, J.H., J. H. Wright, M. Yogo. (2002). “A survey of weak instruments and weak identification in generalized method of moments,” Journal of Business & Economic Statistics, 20(4), 518-529.
Welch, J.P. (1994). “HMO market share and its effect on local Medicare costs,” in H. Luft, ed., HMOs and the elderly, Ann Arbor: Health Administration Press, 231-249.

Does Managed Care Reduce Federal Spending? 17
Table 1: Summary StatisticsMedicare Spending and Beneficiary Characteristics 1999 - 2004
Average Total Medicare Spending 544.58(120.97)
MMC Penetration 0.15(0.15)
MMC Payment Rate 559.83(96.45)
Average FFS Spending 521.48(126.19)
Simulated MMC Expected Profits 15.80(40.60)
Commercial HMO Pen 0.25(0.17)
Female (%) 0.58(0.03)
Average Age 74.58(0.70)
Black (%) 0.08(0.10)
Hispanic (%) 0.02(0.04)
Other Race (%) 0.03(0.05)
Missing Race (%) 0.003(0.003)
Dual Eligibles (%) 0.12(0.07)
Disabled Pre-65 (%) 0.07(0.03)
Urban County 0.71(0.45)
Average Income ($1,000) 29.83(9.27)
Hospitals/1000 0.02(0.03)
General Pract./1000 0.24(0.12)
Doctors/1000 2.52(1.83)
Ambulatory Care/1000 0.01(0.01)
Notes: Standard deviations in parentheses. Spending variables expressed in average nominal dollars per Medicare beneficiary per month. 1999-2004 CMS Limited Data Set, Average FFS Cost and Medicare Managed Care Ratebook data, 18,634 county-year observations.

Does Managed Care Reduce Federal Spending? 18
Table 2: The Effect of Medicare Managed Care Penetration on Logged Average Monthly Per-Enrollee Medicare Spending 1999 - 2004
OLS IV OLS IVMMC Penetration 0.003** 0.011** 0.003** 0.011**
(0.0003) (0.002) (0.0003) (0.002)Commercial HMO Pen -0.0002 -0.0009**
(0.0001) (0.0003)Female (%) -0.0003 -0.0001 -0.0003 -0.0001
(0.001) (0.001) (0.001) (0.001)Average Age -0.01** -0.01 -0.01** -0.006
(0.003) (0.004) (0.003) (0.004)Black (%) -0.003* 0.0006 -0.003* 0.0007
(0.001) (0.002) (0.001) (0.002)Hispanic (%) -0.01** -0.01* -0.01** -0.009*
(0.003) (0.004) (0.003) (0.004)Other Race (%) -0.007** -0.004 -0.007** -0.004
(0.002) (0.002) (0.002) (0.002)Missing Race (%) -0.002 0.003 -0.002 0.004
(0.003) (0.005) (0.003) 0.0002Dual Eligibles (%) -0.002* 0.0002 -0.002* 0.0002
(0.001) (0.001) (0.001) (0.001)Disabled Pre-65 (%) 0.003** 0.0007 0.003** 0.0009
(0.001) (0.001) (0.001) (0.001)Per Capita Income -0.0009 -0.0002 -0.0008 -0.0001
(0.001) (0.001) (0.001) (0.001)Hospitals/1000 0.05 -0.1 0.05 -0.1
(0.13) (0.15) (0.13) (0.15)General Pract./1000 0.03* 0.01 0.03* 0.01
(0.014) (0.017) (0.014) (0.017)Doctors/1000 -0.001 0.0004 -0.001 0.0003
(0.001) (0.001) (0.001) (0.002)Ambulatory Care/1000 -0.06 0.03 -0.06 0.03
(0.15) (0.19) (0.15) (0.19)First-Stage F Statistic 38.7 43.9
Notes: OLS and IV regressions of logged average Medicare spending on county Medicare managed care penetration. All models include county and year fixed effects. IV models instrument for MMC penetration using predicted HMO profit. 1999-2004 CMS Limited Data Set, Average FFS Cost and Medicare Managed Care Ratebook data, 18,634 county-year observations. Cluster-robust t-statistics in parentheses. * Significant at 5%, ** Significant at 1%.
Does Managed Care Reduce Federal Spending? 19
Table 3: The Effect of Medicare Managed Care Penetration on Logged Average Monthly Per-Enrollee Fee-for-Service Spending, 1999 - 2004
OLS IV Rate IV ProfitMMC Penetration 0.004** 0.005* 0.006*
(0.00) (0.00) (0.00)Commercial HMO Pen -0.0003 -0.0004 -0.0004
(0.0001) (0.0002) (0.0003)Female (%) -0.0001 -0.0001 -0.0001
(0.001) (0.001) (0.001)Average Age 0.008** 0.009** 0.009**
(0.003) (0.003) (0.003)Black (%) 0.003 0.003 0.004
(0.002) (0.002) (0.002)Hispanic (%) -0.006 -0.006 -0.005
(0.005) (0.005) (0.005)Other Race (%) -0.008** -0.007** -0.007**
(0.002) (0.002) (0.002)Missing Race (%) -0.004 -0.003 -0.002
(0.003) (0.004) (0.004)Dual Eligibles (%) -0.002 -0.002 -0.001
(0.001) (0.001) (0.001)Disabled Pre-65 (%) -0.0001 -0.0004 -0.0006
(0.001) (0.001) (0.001)Per Capita Income 0.001 0.001 0.0011
(0.00) (0.00) (0.00)Hospitals/1000 0.09 0.07 0.06
(0.14) (0.13) (0.13)General Pract./1000 0.03* 0.026 0.024
(0.01) (0.02) (0.02)Doctors/1000 -0.002 -0.001 -0.001
(0.001) (0.001) (0.001)Ambulatory Care/1000 -0.11 -0.10 -0.09
(0.16) (0.17) (0.17)First-Stage F Statistic 44.0 39.3
Notes: OLS and IV regressions of logged average per capita Medicare spending on county Medicare managed care penetration. All models include county and year fixed effects. MMC penetration instrumented using county-level plan payment rates (Column 2) and estimated plan profit (Column 3). 1999-2004 CMS Limited Data Set, Average FFS Cost and Medicare Managed Care Ratebook data, 18,634 county-year observations. Clustered standard errors in parentheses. * Significant at 5%, ** Significant at 1%.

Does Managed Care Reduce Federal Spending? 20
Table 4: Robustness Checks: The Effect of Medicare Managed Care Penetrationon Average Per-Enrollee Medicare Spending, 1999 - 2004
ln(Spend) ln(spend) ln(Part A) ln(Part B) IV GLMMMC Penetration 0.028** 0.012** 0.01** 0.019** 1.012**
(0.011) (0.002) (0.003) (0.003) (0.001)Herfindahl Index 0.017**
(0.006)Included Counties Pen>=10% All All All All
Source: 1999-2004 CMS Limited Data Set, Average FFS Cost and Medicare Managed Care Ratebook data, Area Resource File, Health Leaders Interstudy data.Notes: IV regressions of logged average per capita Medicare spending on county Medicare managed care penetration. All models include county and year fixed effects. MMC penetration instrumented using estimated plan profit. Column 1 limits the sample to counties with at least 10% MMC penetration. Columns 3 and 4 examine average Part A (inpatient) and Part B (outpatient) spending seperately. Column 5 estimates an IV GLM model with a log link on untransformed spending. 1999-2004 CMS Limited Data Set, Average FFS Cost and Medicare Managed Care Ratebook data, 18,634 county-year observations. Clustered standard errors in parentheses. * Significant at 5%, ** Significant at 1%.

Does Managed Care Reduce Federal Spending? 21
Appendix Table 1: First Stage Relationships between Medicare PaymentPolicy Variables and Medicare Managed Care Penetration, 1999 - 2004
MMCPen MMCPenEstimated Profit 0.03**
(0.004)Payment Rate 0.03**
(0.004)Commercial HMO Pen. 0.08** 0.08**
(0.02) (0.02)Female (%) -0.04 -0.04
(0.05) (0.05)Average Age -0.56 -0.54
(0.33) (0.33)Black (%) -0.37* -0.39*
(0.15) (0.15)Hispanic (%) 0 -0.07
(0.41) (0.40)Other Race (%) -0.29 -0.31*
(0.16) (0.15)Missing Race (%) -0.69* -0.71*
(0.30) (0.30)Dual Eligibles (%) -0.11 -0.12
(0.09) (0.09)Disabled Pre-65 (%) 0.28** 0.28**
(0.08) (0.08)Per Capita Income -0.05 -0.05
(0.09) (0.09)Hospitals/1000 16.4 16.85
(10.42) (10.46)General Pract./1000 1.57 1.68
(1.23) (1.24)Doctors/1000 -0.12 -0.12
(0.12) (0.12)Ambulatory Care/1000 -14.55 (13.73)
(15.57) -15.52
Notes: First stage regressions of Medicare managed care penetration rates on 1- expected HMO per enrollee profit and 2- MMC payment rate. All models include county and year fixed effects. 1999-2004 CMS Limited Data Set, Average FFS Cost and Medicare Managed Care Ratebook data, 18,634 county-year observations. Robust t-statistics in parentheses. * Significant at 5%, ** Significant at 1%.


















