38
Does monitoring cardiac output influence outcome? David Bennett St George’s Hospital London
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | amelia-garrison |
| View: | 219 times |
| Download: | 0 times |

Does monitoring cardiac output
influence outcome?
David Bennett St George’s HospitalLondon

Disclosures
•I act as a consultant for Deltex and Lidco
•Can cardiac output (CO) be accurately assessed clinically?•Why are there so many different technologies for measuring CO?
•Does monitoring CO, particularly with PAC increase morbidity and/or mortality?
•Does monitoring CO or surrogate have prognostic value?•Does targeting CO improve outcome?
•or •Because we believe the data to be clinically relevant?
Questions to be posed
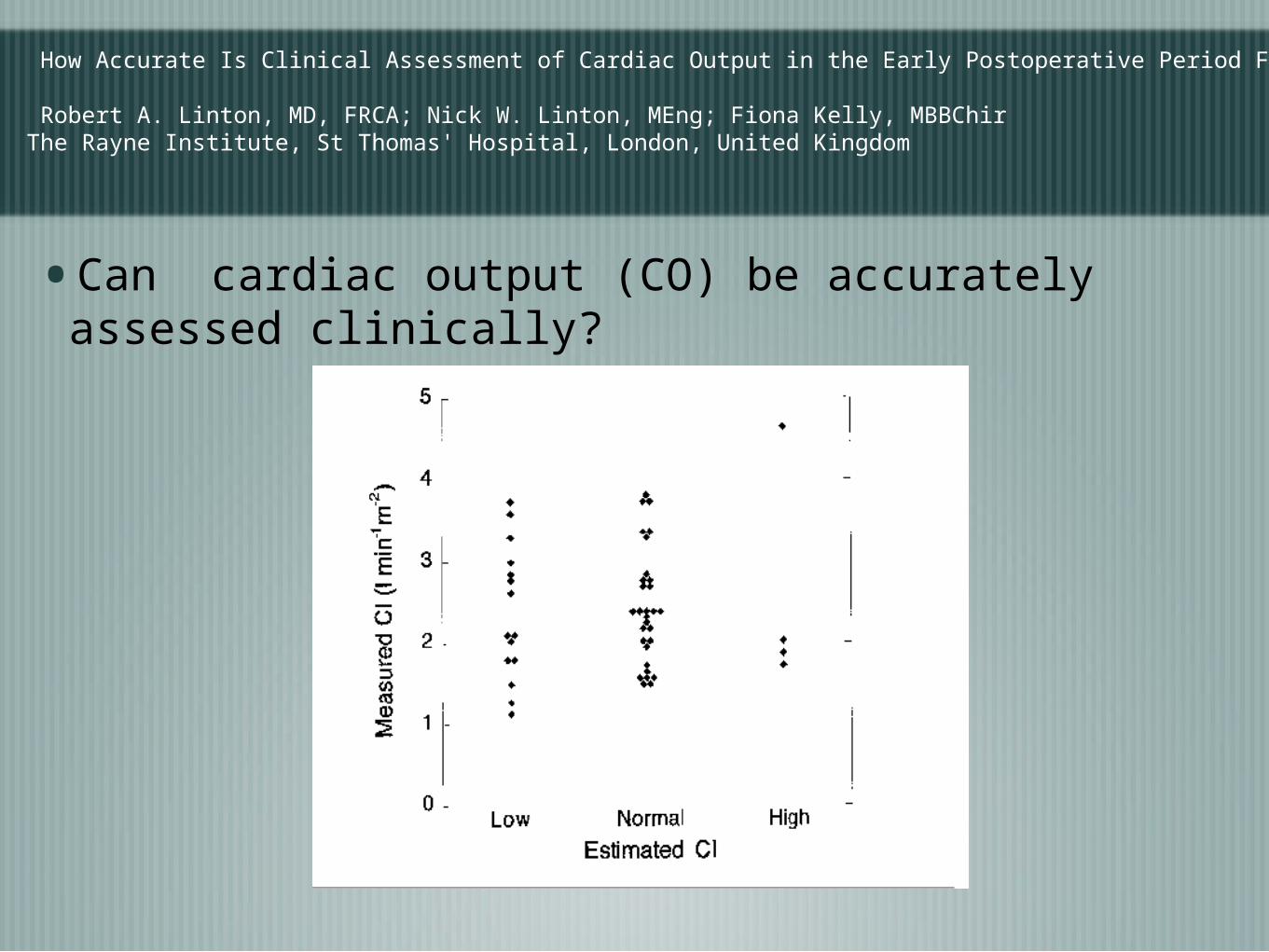
How Accurate Is Clinical Assessment of Cardiac Output in the Early Postoperative Period Following Cardiac Surgery?
Robert A. Linton, MD, FRCA; Nick W. Linton, MEng; Fiona Kelly, MBBChirThe Rayne Institute, St Thomas' Hospital, London, United Kingdom
•Can cardiac output (CO) be accurately assessed clinically?
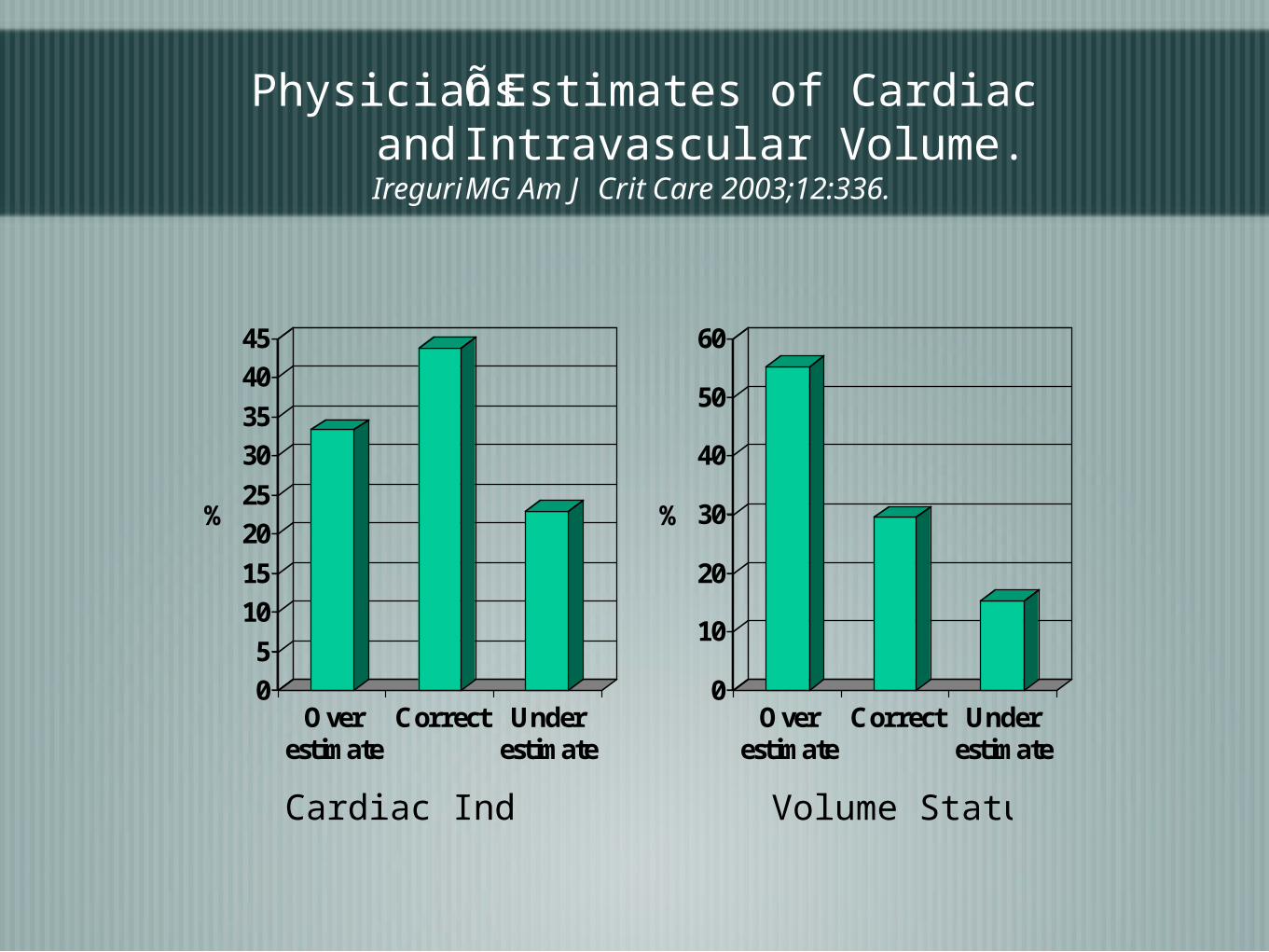
PhysiciansÕ Estimates of Cardiac Indexand Intravascular Volume.Ireguri MG Am J Crit Care 2003;12:336.
0
5
10
15
20
25
30
35
40
45
%
Overestimate
Correct Underestimate
0
10
20
30
40
50
60
%
Overestimate
Correct Underestimate
Cardiac Index Volume Status

Why are there so many different technologies for measuring CO?
Fick: Direct, Indirect
Dilution tehniques:
ICG,
Hot and cold, intermittent and semi-continuousScvO2 and SvO2
ECHO
Oesophageal, Supra-sternal Doppler
Impedance cardiography
Pulse contour analysis
C02 rebreathing

Conners AF,Jr, Speroff T, Dawson NV, Thomas C, et al: The effectiveness of right heart catheterizaion in the initial care of critically ill patients. JAMA 1996; 276: 899-97
Does monitoring CO, particularly with PAC increase morbidity and/or mortality?

The incidence of major morbidity in critically ill patients managed with pulmonary artery catheters:
A meta-analysisIvanov, Rada MD; Allen, Jill MSc; Calvin, James E. MD, FACC, FRCPC
28(3), March 2000, pp 615-619CCM

Impact of the Pulmonary Artery Catheter in Critically Ill PatientsMeta-analysis of Randomized Clinical TrialsMonica R. Shah, MD, MHS, MSJ; Vic Hasselblad, PhD; Lynne W. Stevenson, MD; Cynthia Binanay, RN, BSN; Christopher M. O’Connor, MD; George Sopko, MD, MPH; Robert M. Califf, MD JAMA. 2005;294:1664-1670.

Impact of the Pulmonary Artery Catheter in Critically Ill PatientsMeta-analysis of Randomized Clinical TrialsMonica R. Shah, MD, MHS, MSJ; Vic Hasselblad, PhD; Lynne W. Stevenson, MD; Cynthia Binanay, RN, BSN; Christopher M. O’Connor, MD; George Sopko, MD, MPH; Robert M. Califf, MD JAMA. 2005;294:1664-1670.

508 240 205 194 188 186 183
506 232 191 179 174 168 166
No PAC
PAC
No PAC
PAC
0.00
0.25
0.50
0.75
1.00
P(s
urv
iva
l)
0 15 30 45 60 75 90Time from randomisation (days)
Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man): a randomised controlled trial.Harvey S, Harrison DA, Singer M, Ashcroft J, Jones CM, Elbourne D, Brampton W, Williams D, Young D, Rowan K; PAC-Man study collaboration.: Lancet. 2005 Aug 6-12;366(9484):472-7.

Does monitoring CO or a surrogate have prognostic value?

Effect of Oxygen Delivery on Mortalityand Morbidity in High Risk Surgery.
Shoemaker Chest. 1988: 94; 1176
0
10
20
30
40
50
60
70
%
<300 301-400 401-500 >501
% Mortality
0
10
20
30
40
50
60
% o
f P
atie
nts
<400 400-500 500-600 >600
DO2 l/min/m2
% Patients with Morbidity
Does monitoring CO or a surrogate have prognostic value?

Does monitoring CO or surrogate have prognostic value?
0
50
100
150
200
250
0 200 400 600 800 1000 1200 1400
Non Responders0
50
100
150
200
250
300
350
0 200 400 600 800 1000 1200 1400
Oxygen delivery L/min/m2
Oxygen c
onsu
mpti
on L
/min
/m2
Responders
Before dobutamine
After dobutamine
Rhodes A. CCM 1999; 11; 2361

cc
Outcome of Patients
Responders Non Responders
PredictedMortality %
39 58
Actualmortality %
14 90.9
Rhodes A. CCM 1999; 11; 2361

Impact of LOW Post-Operative Central Venous Oxygen Saturation on Morbidity & Mortality in Surgical
PatientsV PRIYA*, J V DIVATIA, RASHMI S, R SAREEN
ScvO
2 at 2
hou
rs :
95%
CI
Low (n = 51)Normal (n = 32)90
80
70
60
76.8 + 5.7
63.9 + 8.9
p = 0.00*
ScvO2 at 2 hrs
80
78
76
74
72
70
68
66
ScvO
2 at 1
2 ho
urs
: 95%
CI
76.2 + 4.1
68.7 + 6.1
Low (n = 51)Normal (n = 32)
ScvO2 at 12 hrsp = 0.00*

0.03*13 (26%)2 (9%)Anastomotic leak (no. of pts)
0.163 (6%)0 (0%)Hospital mortality (no. of pts)
0.002*17.8 + 10.513.5 + 5.0Hospital stay (days, Mean+SD)
0.163 (6%)0 (0%)ICU mortality (no. of patients)
0.009*5.6 + 6.71.7 + 2.5ICU stay (days, Mean+SD)
0.009*3.5 + 6.10.59 + 1.5Days on ventilator (Mean+SD)
p ValueLow (n=51)Normal (n=32)
OUTCOME

DO2 does not always correlate with CO
20 30 40 50 60 70 80 90 1000
100
200
300
400
500
600
700
800
900
1000
1100
1200
Central Venous Saturation
Oxygen Delivery Index
Relationship Between Central Venous OxygenSaturation and Oxygen Delivery.
DO2 I ml/min/m2
•Does targeting CO improve outcome?

Meta-analysis of hemodynamic optimization: relationship to methodological qualityMartijn Poeze, Jan Willem M Greve and Graham RamsayCritical Care 2005, 9:10.1186/cc3902)This article is online at: http://ccforum.com/content/9/6/R771 R771-R779 (DOI
Control
Treatment
% Mortality
10.4 4.7
Peri-operative

Wilson et al:- BMJ :1999 318 1099
Days
*
% Surviving

Meta-analysis of hemodynamic optimization: relationship to methodological qualityMartijn Poeze, Jan Willem M Greve and Graham RamsayCritical Care 2005, 9:10.1186/cc3902)This article is online at: http://ccforum.com/content/9/6/R771 R771-R779 (DOI
Control
Treatment
% Mortality
54 53
Sepsis

Hayes, M A. Timmins, A C. Yau, E H. Palazzo, M. Hinds, C J. Watson, D.Title Elevation of systemic oxygen delivery in the treatment of critically ill patientsSource New England Journal of Medicine. 330(24):1717-22, 1994 Jun 16.
% Mortality

ScvO2%ScvO2%
HoursHours
* * * * *
Early goal-directed therapy in the treatment of sepsis and septic shock: An outcome evaluation of early intervention
Rivers et al N Eng J Med 2001 345 19
Early goal-directed therapy in the treatment of sepsis and septic shock: An outcome evaluation of early intervention
Rivers et al N Eng J Med 2001 345 19

MortalityControl n (%)
Treatmentn (%)
p
In-hospital:All patients
59 (46.5)
38 (30.5) 0.009
Severe sepsis 19 (30) 9 (14.9) 0.06
Septic shock40
(56.8)29 (42.3) 0.04
Septic syndrome
44 (45.4)
35 (35.1) 0.01
Early goal-directed therapy in the treatment of sepsis and septic shock: An outcome evaluation of early intervention
Rivers et al N Eng J Med 2001 345 19
Early goal-directed therapy in the treatment of sepsis and septic shock: An outcome evaluation of early intervention
Rivers et al N Eng J Med 2001 345 19

* * * * * * *DO
2I
ml/min/
m2
Hours
Early goal -directed therapy after major surgery reduces complications and duration of hospital stay
Pearse et al Critical Care 2005 9 R687 -693

Number of infections
EGDT
Control
p
Number of complications / patient
0 (0-4)
mean 0.7
1 (0-5)
mean 1.5
0.002
*
***
*
*

Control
n=60
EGDTn=62
Difference
% Reducti
on
Median14(6-188)
11(0.4-110)
3 21
Mean 29.5 17.5 12.0 41
Total 1770 1085 685 39

Chittock DR. Dhingra VK. Ronco JJ. Russell JA. Forrest DM. Tweeddale M. Fenwick JC. Severity of illness and risk of death associated with pulmonary artery catheter use.[see comment]. Critical Care Medicine. 32(4):911-5, 2004 Apr.

Does goal directed therapy using the oesophageal Doppler reduce surgical mortality and morbidity?Hamilton M. A.1, Grocott M. P. W.1, Mythen M1, Bennett D2
Mean reduction in LOS of 4 days (25%)

Conclusions
•Cardiac output is a frequently measured variable
•There are several technologies allowing it’s measurement
•Despite earlier claims it is unlikely that measuring CO particularly with the PAC is harmful
•Low CO and it’s failure to respond to treatment has prognostic significance
•There is now reasonable evidence suggesting that targeting CO very early in the course of critical illness is of real benefit
•This is particularly so in patients undergoing major surgery where increasing DO2 to a target value has profound beneficial effects
•


META-ANAYSIS OF HEMDYNAMIC OPTIMIZATION IN HIGH RISK PATIENTSJack W. Kern1,2,3, Pharm D, William C Shoemaker2,3, MDCCM 2001

In all patients maintain SaO2 ≥94%, Hb≥ 8g.dl-1 , Temp.at 37oC. HR≤100 or <20% above baseline. MAP 60-100 mmHg
In all patients maintain SaO2 ≥94%, Hb≥ 8g.dl-1 , Temp.at 37oC. HR≤100 or <20% above baseline. MAP 60-100 mmHg
Patient identification. Written informed consent. Lines inserted. Surgery. RandomisationPatient identification. Written informed consent. Lines inserted. Surgery. Randomisation
Admit to ICU. Monitor cardiac output in all patients using Lidco. Data concealed from clinical staff
Admit to ICU. Monitor cardiac output in all patients using Lidco. Data concealed from clinical staff
CONTROL GROUPCONTROL GROUP
Fluid challenge with 250 ml bolus IV colloid until sustained 2mm Hg rise in CVP is
achieved for ≥20 min. Repeat if CVP falls
Fluid challenge with 250 ml bolus IV colloid until sustained 2mm Hg rise in CVP is
achieved for ≥20 min. Repeat if CVP falls
If CI <2.5l min-1m2 commence epinephrine, if > 2.5l min-1m2 continue current treatment
If CI <2.5l min-1m2 commence epinephrine, if > 2.5l min-1m2 continue current treatment
If urine output <0.5ml kg -1 hr-1 for 2 hours or consecutive hourly lactate rises to >2 mmol l -1 then CI revealed
to clinical staff
If urine output <0.5ml kg -1 hr-1 for 2 hours or consecutive hourly lactate rises to >2 mmol l -1 then CI revealed
to clinical staff
EGDT GROUPEGDT GROUP
Fluid challenge with 250 ml bolus IV colloid until sustained 10% rise in SV for ≥20 min.
Repeat if SV falls
Fluid challenge with 250 ml bolus IV colloid until sustained 10% rise in SV for ≥20 min.
Repeat if SV falls
If DO2 <600ml min -1 m2 start dopexamine at 0.25µg kg -1 min -1 and increase to maximum of
0.25µg kg -1 min -1 until DO2 reaches target value. Dose reduced if tachycardia or myocardial
ischemia develops
If DO2 <600ml min -1 m2 start dopexamine at 0.25µg kg -1 min -1 and increase to maximum of
0.25µg kg -1 min -1 until DO2 reaches target value. Dose reduced if tachycardia or myocardial
ischemia develops
After 8 hours study period ends all decisions taken by clinical staff. Patient followed for hospital morbidity and 60 day mortality
After 8 hours study period ends all decisions taken by clinical staff. Patient followed for hospital morbidity and 60 day mortality

Crit Care Med. 2005 May;33(5):1119-22.
Pinsky MR, Vincent JL.

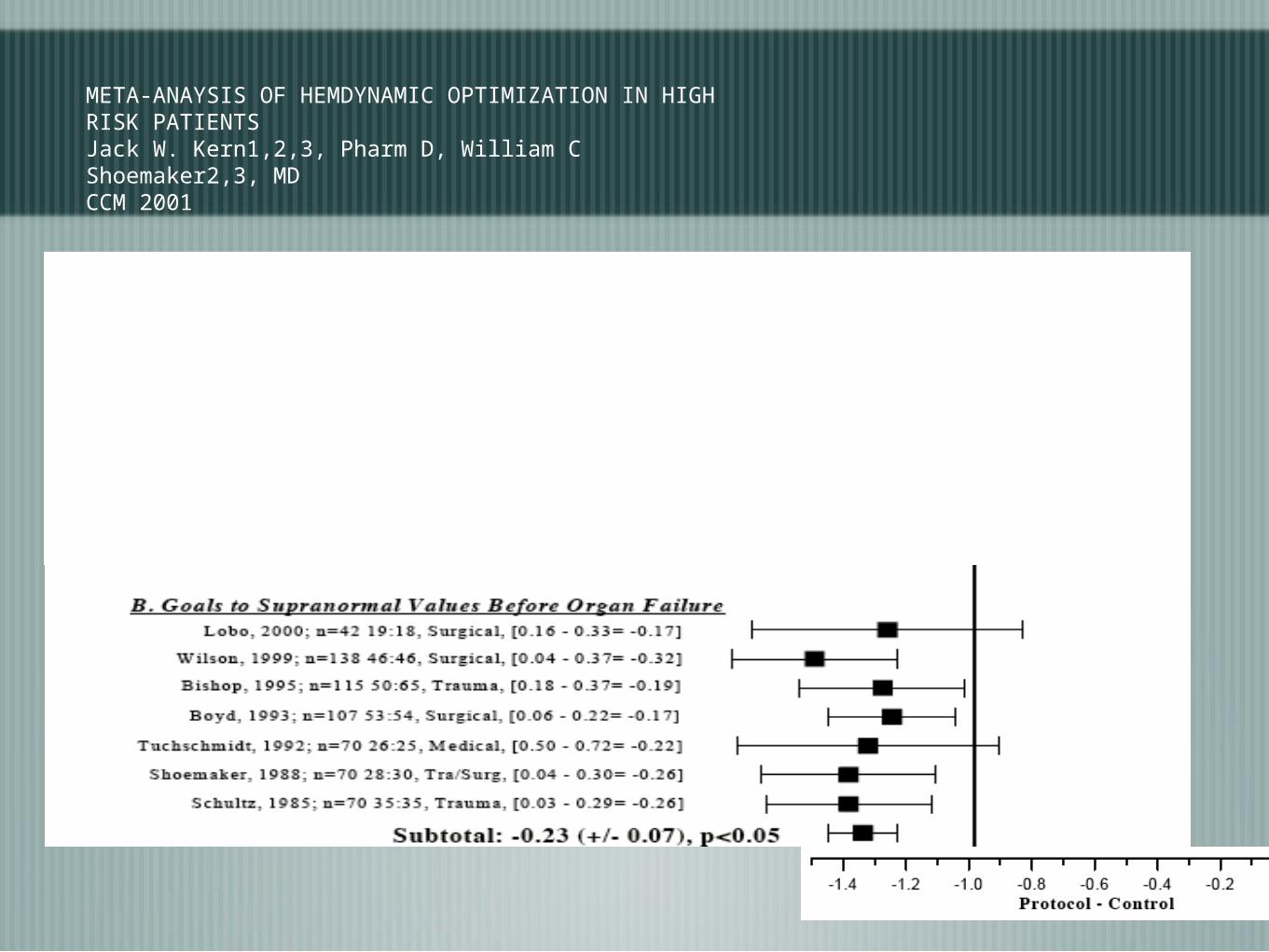
META-ANAYSIS OF HEMDYNAMIC OPTIMIZATION IN HIGH RISK PATIENTSJack W. Kern1,2,3, Pharm D, William C Shoemaker2,3, MDCCM 2001

•Audit of >53,000 trauma patients in USA
•Older patients with severe injury and shock had a survival benefit when managed with PAC
•Odds ratio, 0.33; 95% confidence interval, (ratio 0.17-0.62)
•
1: Crit Care Med. 2006 Apr 4; [Epub ahead of print]Related Articles, Links
Pulmonary artery catheter use is associated with reduced mortality in severely injured patients: A National Trauma Data Bank analysis of 53,312 patients*
Friese RS, Shafi S, Gentilello LM.

















