“ “ Does the Benefit Does the Benefit Associated with Associated with Treating Treating Hypertension Apply Hypertension Apply to Children?" to Children?" Ronald Portman, MD Ronald Portman, MD Professor and Director Professor and Director Division of Pediatric Nephrology and Division of Pediatric Nephrology and Hypertension Hypertension University of Texas -Houston University of Texas -Houston Past-Chair, International Pediatric Past-Chair, International Pediatric Hypertension Association Hypertension Association
Transcript
““Does the Benefit Does the Benefit Associated with Treating Associated with Treating Hypertension Apply to Hypertension Apply to
Children?" Children?"
““Does the Benefit Does the Benefit Associated with Treating Associated with Treating Hypertension Apply to Hypertension Apply to
Children?" Children?" Ronald Portman, MDRonald Portman, MD
Professor and DirectorProfessor and DirectorDivision of Pediatric Nephrology and Division of Pediatric Nephrology and
HypertensionHypertensionUniversity of Texas -HoustonUniversity of Texas -Houston
Past-Chair, International Pediatric Past-Chair, International Pediatric Hypertension Association Hypertension Association
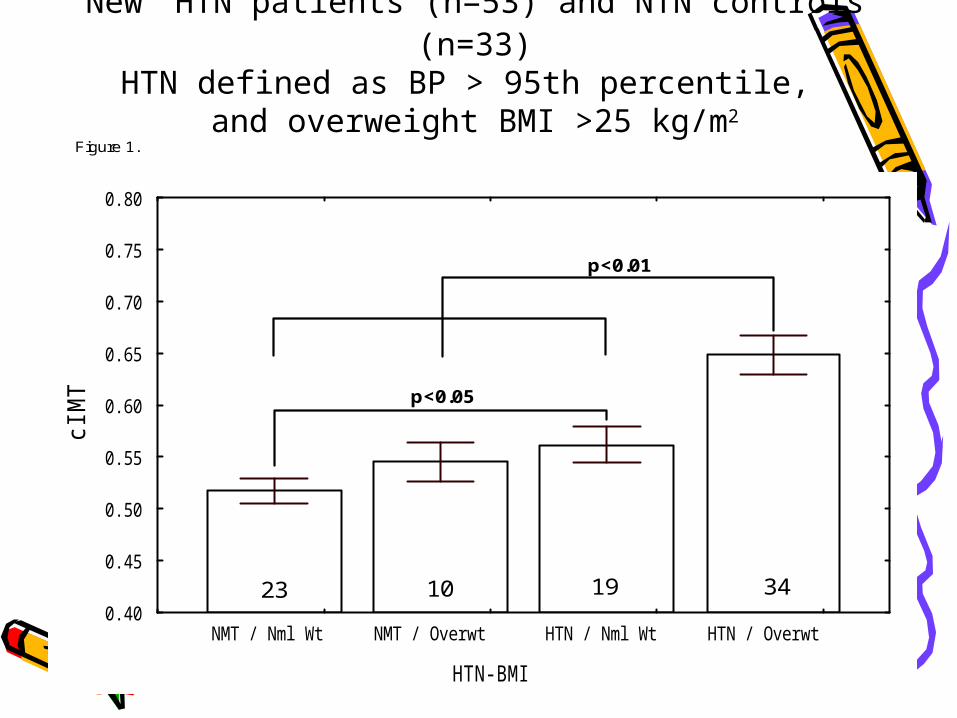
New HTN patients (n=53) and NTN controls (n=33)HTN defined as BP > 95th percentile,
and overweight BMI >25 kg/m2
ESCAPE TRIAL
– CKD patients n=352; Age 3-18 yo; European Multi-center Trail
– GFR 11-80 cc/min/1.73m2 – 6 months duration of study; ramipril 6 mg/m2;
no placebo– BP was reduced by 7.1 ± 8.0 mmHg in all
groups– Higher the initial BP and greater the
proteinuria; the greater the BP lowering effect– 87.3% of patients achieved normotension with
56% less than the 50th percentile– Proteinuria reduced in 50% of patients
•Wuehl et al. Kidney International 2004;66:768-776
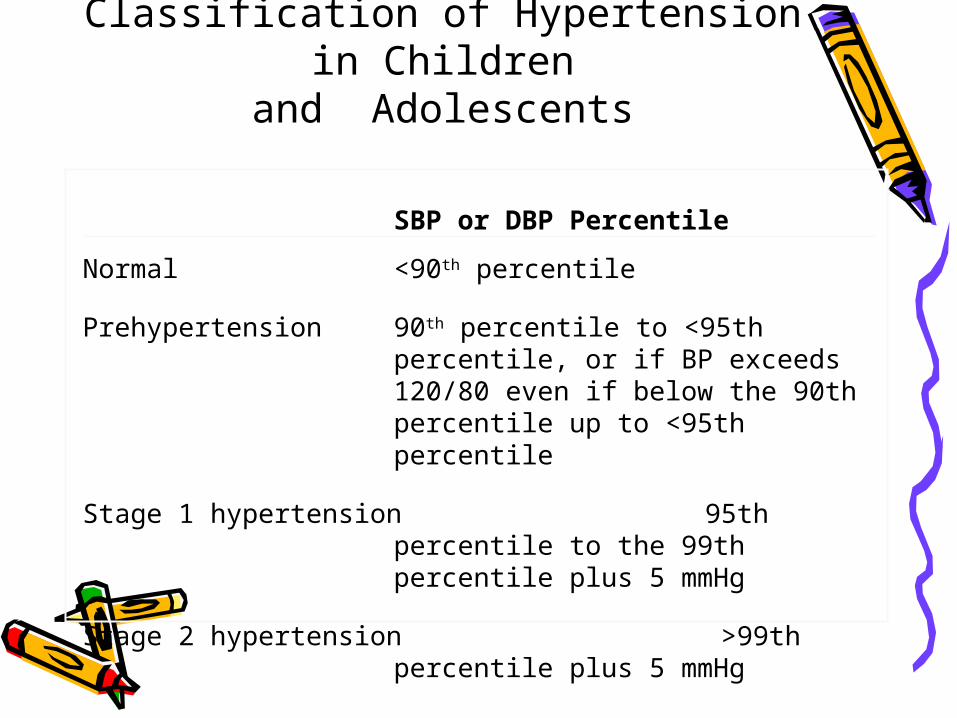
Classification of Hypertension in Children
and Adolescents: Therapy Recommendations
Pharmacologic Therapy
Normal None
Prehypertension Do not initiate therapy unless there are compelling indications such as chronic kidney disease (CKD), diabetes mellitus, heart failure, left ventricular hypertrophy (LVH).
Stage 1 hypertension Initiate therapy based on indications
Stage 2 hypertension Initiate therapy
All patients to receive Therapeutic Life-style Changes (TLC)
Indications for Antihypertensive Drug Therapy in Children
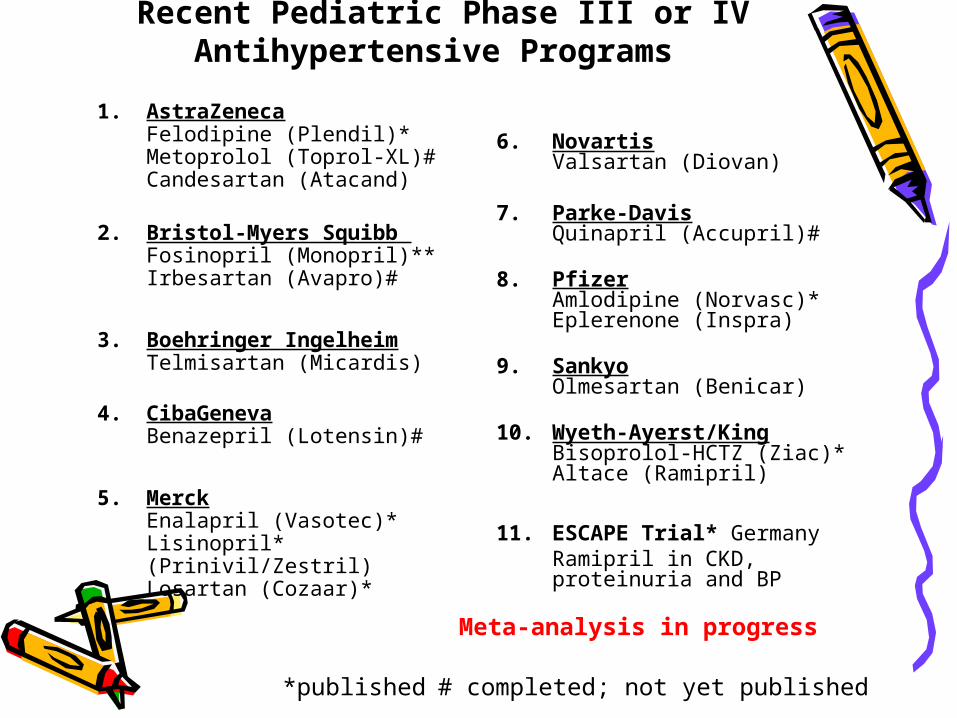
11. ESCAPE Trial* GermanyRamipril in CKD, proteinuria and BP
*published
Meta-analysis in progress
# completed; not yet published
The Agency can require studies of antihypertensive drugs in children prior to approval for use in
adults. Should they do this?
• First question: are antihypertensive drugs used in children and their use warranted?
• Yes, but is there proof of efficacy beyond BP lowering? Not yet.
• Should they do this? No• Any new compound should be thoroughly
tested for safety and efficacy in adults first unless compelling indication
• However, pediatric studies must be done after adult approval
The Agency can also promote studies in children by granting additional exclusivity for
assessing the effects of antihypertensive drugs in children.
Should they do this?
• Yes• This program has yielded
tremendous knowledge about pediatric hypertension
FDAMA• Studies for exclusivity: safety and efficacy
– Initial dose ranging studies had low expectations
– Pharmacokinetic studies required for each drug
– New set of FDA written requests required an interpretable study (age 6-16 yrs) 40-60% African American
• Sub-studies for end organ damage, metabolic effects• Encouragement to obtain labeling • Compounding of pediatric dosage forms• Year long safety study• Beginning to examine effects on development
– Examining younger age groups (1-5 years old)– New study with end point other than BP
lowering
Is study of effects on blood pressure adequate?
• Not anymore
FDAMA: The Next Generation• Studies designed to determine optimum
dose or use; not just an ‘effective’ dose• Study to determine the most effective
drug for pediatric hypertension• Studies to determine EOD and disease
reversibility• Studies using other end points beside BP
lowering• Studies for long-term BP control• Studies of antihypertensive combinations
FDAMA: The Next Generation
• Examine specific therapies for most prevalent diseases such as obesity, CKD
• Commercially available preparations as no medicaid funding for drug compounding
• Begin to examine neonatal/infant hypertension
• PREVENTION
Does the benefit associated with treating hypertension in children Does the benefit associated with treating hypertension in children apply to adults?"apply to adults?"