DOES URINE ALKALINIZATION PREVENT OR REDUCE THE SEVERITY OF RHABDOMYOLYSIS- INDUCED RENAL FAILURE IN POISONED PATIENTS? Allister Vale MD National Poisons Information Service (Birmingham Unit) and West Midlands Poisons Unit City Hospital, Birmingham, UK
Transcript
DOES URINE ALKALINIZATION PREVENT OR REDUCE THE SEVERITY OF
RHABDOMYOLYSIS-INDUCED RENAL FAILURE IN POISONED PATIENTS?
Allister Vale MD
National Poisons Information Service(Birmingham Unit) and West Midlands Poisons Unit
City Hospital, Birmingham, UK
RHABDOMYOLYSIS
Aetiology
Diagnosis
Complications
Pathogenesis of rhabdomyolysis-induced renal failure
Rationale for urine alkalinization and volume replacement
Experimental and clinical studies
RHABDOMYOLYSIS: AETIOLOGY
Trauma e.g. crush injuries
Drug-or other chemical-induced
Therapeutic
Poisoning
Primary caused by direct insult
Secondary e.g. local compression as a result of coma, seizures
RHABDOMYOLYSIS: DIAGNOSIS
Dissolution of striated muscle fibres, with leakage of muscle enzymes, myoglobin and other intracellular constituents
Creatine kinase activity > 5x normal (CK-MB fraction < 5%) 2-12 hours after precipitating cause
Creatine kinase activity may continue to rise > 24 hours
RHABDOMYOLYSIS: DIAGNOSIS
Transient increase in serum myoglobin soon after onset of rhabdomyolysis
Visible myoglobinuria (tea or coca-cola coloured urine)
Myoglobinuria >250 mg/L (normal < 0.5 mg/L) in presence of normal renal function
RHABDOMYOLYSIS: DIAGNOSIS
Absence of myoglobinuria does not exclude diagnosis
Positive urine dipstick for haem but no red cells on microscopic examination of urine
RHABDOMYOLYSIS: COMPLICATIONS
Acute renal failure
Nerve damage (compartment syndrome)
Hyperkalaemia (fatal dysrhythmias)
Hypocalcaemia (calcium binding by damaged muscle proteins and phosphates)
RHABDOMYOLYSIS: COMPLICATIONS
Increase in plasma urate concentration (> 750 μmol/L)
Increase in serum phosphate concentration (>2.5 mmol/L)
Increase in AST/ALT activities
Increase in lactic dehydrogenase and aldolase (specific for muscle) activities
RHABDOMYOLYSIS-INDUCED RENAL FAILURE
5-30 % of patients with rhabdomyolysis develop acute renal failure (Gabow et al, 1982; Ward, 1988)
Rhabdomyolysis accounts for 5-9 % of all cases of acute renal failure
(Grossman et al, 1974; Thomas and Ibels, 1985)
URINE ALKALINIZATION AND RHABDOMYOLYSIS-INDUCED RENAL FAILURE
Bywaters et al, 1944 recommended the use of "alkaline diuresis" to prevent renal failure in patients with crush syndrome
(Bywaters, 1990)
Since then, urine alkalinization has often been incorporated into treatment regimens
Is this management rational?
PATHOGENESIS OF RHABDOMYOLYSIS-INDUCED RENAL FAILURE
Tubular necrosis initiated by free-radical mediated lipid peroxidation
Renal vasoconstriction by several mechanisms
Tubular obstruction due to binding of free myoglobin to Tamm-Horsfall protein
Tubular obstruction due to hyperuricaemia
Compounded by hypovolaemia and aciduria
PATHOGENESIS OF RHABDOMYOLYSIS-INDUCED RENAL FAILURE
1.Tubular necrosis initiated by free-radical mediated lipid peroxidation
This involves redox cycling between two oxidation states of myoglobin haem: Fe3+ (ferric) and Fe4+ (ferryl)
(Moore et al, 1998; Holt and Moore,
2000)
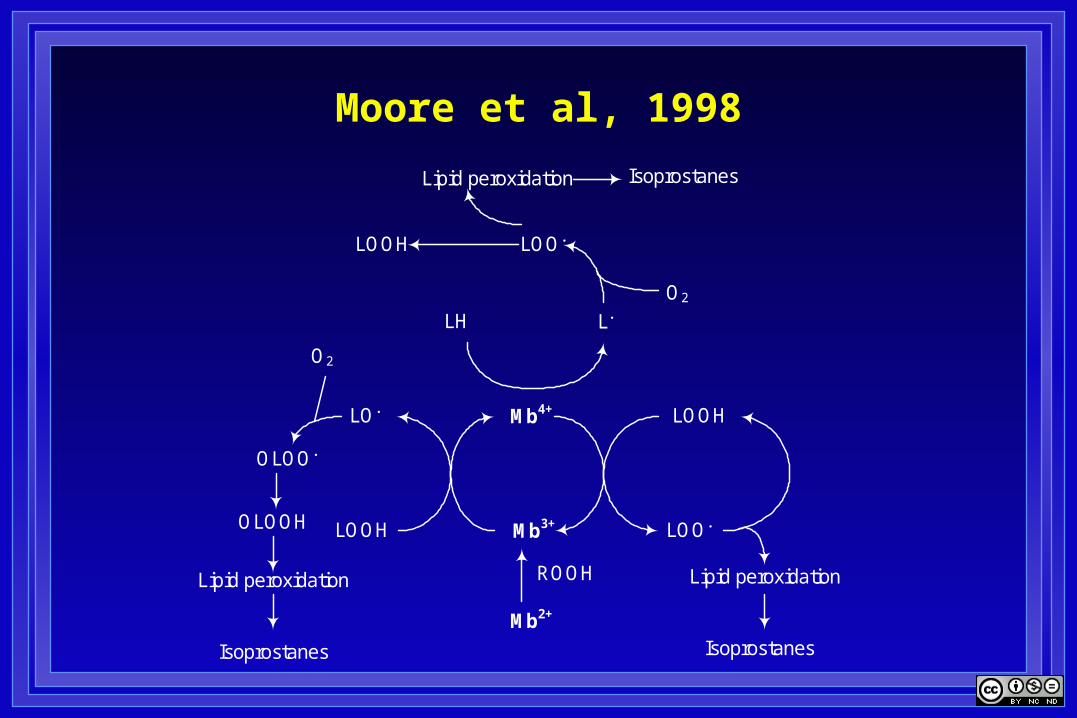
PATHOGENESIS OF RHABDOMYOLYSIS-INDUCED RENAL FAILURE
1.Tubular necrosis initiated by free-radical mediated lipid peroxidation
Ferryl (Fe4+) myoglobin can initiate lipid peroxidation
Its formation requires the presence of lipid hydroperoxides (LOOH)
PATHOGENESIS OF RHABDOMYOLYSIS-INDUCED RENAL FAILURE
1.Tubular necrosis initiated by free-radical mediated lipid peroxidation
Ferryl (Fe4+) myoglobin reacts with lipids (LH) and lipid hydroperoxides (LOOH) to form lipid alkyl (L.) and lipid peroxyl (LOO.) radicals
These radicals cause progressive tubular damage
Moore et al, 1998
LOO.LOOH
LH
O2
Lipid peroxidation
Mb3+
Mb2+
LOOH
LOO.
Lipid peroxidation
LO.
LOOH
OLOO.
O2
Lipid peroxidation ROOH
L.
OLOOH
IsoprostanesIsoprostanes
Isoprostanes
Mb4+
PATHOGENESIS OF RHABDOMYOLYSIS-INDUCED RENAL FAILURE
2. Renal vasoconstriction occurs due to:
Reduced circulating blood volume (hypovolaemia)
Activation of the sympathetic nervous system and renin-angiotensin system
Scavenging of the vasodilator, nitric oxide (NO), by myoglobin
PATHOGENESIS OF RHABDOMYOLYSIS-INDUCED RENAL FAILURE
2. Renal vasoconstriction occurs due to:
Release of isoprostanes formed as a result of free radical damage to phospholipid membranes
15-F2t isoprostane and 15-E2t isoprostane are
potent vasoconstrictors
PATHOGENESIS OF RHABDOMYOLYSIS-INDUCED RENAL FAILURE
3.Tubular obstruction occurs due to formation of tubular casts
Formed by binding of free myoglobin to Tamm-Horsfall protein (Uromodulin), most abundant renal glycoprotein
Zager, 1989
4.Tubular obstruction occurs due to urate crystal deposition (local inflammation)
RATIONALE FOR URINE ALKALINIZATION
Experimentally, urine alkalinization:
Suppresses the reactivity of ferryl (Fe4+) myoglobin
Inhibits the cyclical formation of lipid peroxide radicals and limits lipid peroxidation, so reducing tubular damage
Consistent with this, in isolated perfused kidneys, myoglobin induces vasoconstriction at acid pH
Heyman et al, 1997
RATIONALE FOR URINE ALKALINIZATION
Experimentally:
Urine alkalinization reduces binding of myoglobin to Tamm-Horsfall protein Zager, 1989
Urine alkalinization increases urate solubility Hediger et al, 2005
Acidosis exacerbates myoglobin toxicity in isolated perfused kidneys
RATIONALE FOR URINE ALKALINIZATION
Experimentally:
Acute or chronic exogenous acid loads prevent renal damage in vivo
This may reflect a beneficial effect of any volume replacement or solute load
Heyman et al, 1997
RATIONALE FOR URINE ALKALINIZATION
Experimentally:
Administration of a neutral non-reabsorbed solute prevented:
renal retention of myoglobin
renal damage to the same extent as urine alkalinization (pH ≥8)
Zager, 1989
URINE ALKALINIZATION: CLINICAL STUDIES
There are no adequately controlled studies
Two of the three studies involve traumatic rhabdomyolysis
Concomitant administration of mannitol in all three studies
URINE ALKALINIZATION: CLINICAL STUDIES
Eneas et al,1979
Retrospective review of 20 patients with myoglobinuria (13/20 poisoned with drugs and alcohol)
All patients received crystalloid solutions until volume deficits were corrected
URINE ALKALINIZATION: CLINICAL STUDIES
Eneas et al,1979
17/20 were administered:
Sodium bicarbonate 100 mEq in 1L 5% dextrose and mannitol 25 g
Infused at a rate of 250 mL/hr for 4 hr
URINE ALKALINIZATION: CLINICAL STUDIES
Eneas et al,1979
2/20 patients received intermittent injections of mannitol and sodium bicarbonate
1/20 patients received mannitol alone
Supplemental infusions given in many cases
URINE ALKALINIZATION: CLINICAL STUDIES
Eneas et al,1979
9/20 had increased urine output following treatment (Responders)
Treatment commenced < 48 hours in all cases (5/9 < 24 hours) after admission
None required dialysis and all survived
URINE ALKALINIZATION: CLINICAL STUDIES
Eneas et al,1979
11/20 no increase in urine output after treatment (Non-responders)
Treatment commenced < 48 hours in all cases (6/11 < 24 hours) after admission
10/11 required dialysis; one patient died
URINE ALKALINIZATION: CLINICAL STUDIES
Eneas et al,1979
The non-responders had significantly:
Higher peak creatine kinase activities
Higher serum phosphate concentrations
Higher haematocrit
URINE ALKALINIZATION: CLINICAL STUDIES
Eneas et al,1979
"These results demonstrate that some patients with myoglobinuria will respond to infusion of mannitol and sodium bicarbonate"
"This treatment may be effective in altering the clinical course of myoglobinuric acute renal failure"
URINE ALKALINIZATION: CLINICAL STUDIES
Homsi et al, 1997
Retrospective analysis of 24 patients admitted to an ITU with a diagnosis of traumatic rhabdomyolysis (CK >500 IU/L)
Muscle injury <48 hr previously
Serum [creatinine] < 272 µmol/L
URINE ALKALINIZATION: CLINICAL STUDIES
Homsi et al, 1997
15/24 patients were treated with:
saline 0.9% (mean 204 mL/hr over 60 hr),
mannitol (mean 56 g/day),
sodium bicarbonate (mean 225 mEq/day for a mean of 4.7 days)
9/24 patients received only saline (mean 206 mL/hr over 60 hr)
URINE ALKALINIZATION: CLINICAL STUDIES
Homsi et al, 1997
The initial creatine kinase activity was significantly higher in the group receiving mannitol and sodium bicarbonate
4/15 (27%) patients died in the mannitol and sodium bicarbonate group and 2/9 (22%) patients died in the saline only group (p > 0.05)
URINE ALKALINIZATION: CLINICAL STUDIES
Homsi et al, 1997
The authors claimed that progression to established renal failure could be avoided with prophylactic treatment
Once saline expansion was provided, the addition of mannitol and bicarbonate was unnecessary
URINE ALKALINIZATION: CLINICAL STUDIES
Brown et al, 2004
Retrospective review of 2,083 trauma admissions to an ICU of whom 85% had abnormal CK activities (CK >520 U/L)
Renal failure (plasma creatinine > 182 µmol/L) occurred in 10% of cases
CK activity of 5,000 u/L was the lowest activity associated with renal failure
URINE ALKALINIZATION: CLINICAL STUDIES
Brown et al, 2004
382/2,083 (18%) patients had CK activities > 5,000 IU/L
228/382 patients did not receive mannitol/sodium bicarbonate
154/382 patients received a bolus of mannitol 0.5 g/kg and sodium bicarbonate 100 mEq diluted in 1L 0.45 normal saline
URINE ALKALINIZATION: CLINICAL STUDIES
Brown et al, 2004
This was followed by mannitol 0.1 g/kg/hr and sodium bicarbonate 100 mEq (diluted in 0.45 normal saline 1L) at a rate of 2-10 mL/kg/hr
There was no significant difference in incidence of renal failure (22% vs 18%; p=0.27), dialysis (7% vs 6%; p=0.37) or mortality (15% vs 18%; p=0.37) between groups
URINE ALKALINIZATION: CLINICAL STUDIES
Brown et al, 2004
The administration of mannitol and sodium bicarbonate did not prevent renal failure, dialysis or mortality if CK >5,000 U/L
"The standard of administering sodium bicarbonate/mannitol to patients with post-traumatic rhabdomyolysis should be re-evaluated"
URINE ALKALINIZATION AND RHABDOMYOLYSIS-INDUCED RENAL FAILURE
Conclusions
Experimental data suggest:
Administration of sodium bicarbonate to produce urine alkalinization
Volume replacement
Can reduce the likelihood of rhabdomyolysis-induced renal failure
URINE ALKALINIZATION AND RHABDOMYOLYSIS-INDUCED RENAL FAILURE
Conclusions
Limited clinical data suggest that:
Early volume replacement is more important than urine alkalinization
In preventing rhabdomyolysis-induced renal failure
URINE ALKALINIZATION AND RHABDOMYOLYSIS-INDUCED RENAL FAILURE
Conclusions
There are no adequate data in poisoned patients
Rational basis for employing early volume replacement and probably urine alkalinisation
To reduce the severity or prevent the onset of rhabdomyolysis-induced renal failure