27
DOLS and Liberty Protection Safeguards Dr Camilla Herbert Consultant Clinical Neuropsychologist BPS Introduction to Mental Capacity 26 th April 2019

DOLS and Liberty
Protection Safeguards
Dr Camilla Herbert
Consultant Clinical Neuropsychologist
BPS Introduction to Mental Capacity 26th April 2019

Aims
To present the key points regarding the
Deprivation of Liberty Safeguards
To highlight the problems and why DOLS are
considered ‘unfit for purpose’
To update around status of legislation for Liberty
Protection Safeguards

Grounds for Legal detention
Legal entitlement to restrict someone’s liberty
Prison/criminal offences
Mental Health Act
Deprivation of Liberty Safeguards (DOLS)
The Bournewood Case
HL was an autistic man who had profound learning disabilities and who lacked capacity to consent to, or to refuse, admission to hospital for treatment (1997). HL never attempted to leave the hospital, but his carers were prevented from visiting him in order to prevent him leaving with them. This was challenged through the High Court, Court of Appeal and House of Lords, before being considered at the European Court of Human Rights.
The ECtHR in October 2004 held that he was deprived of his liberty when he was admitted, informally, to Bournewood Hospital.
The ECtHR held that the manner in which HL was deprived of liberty was not in accordance with “a procedure prescribed by law” and breached Article 5(1) of the European Convention on Human Rights (ECHR)

Deprivation of Liberty Safeguards
The Deprivation of Liberty Safeguards were passed by Parliament in April 2007 and provide safeguards for people who lack mental capacity and whose care or treatment necessarily involves a deprivation of liberty within the meaning of Article 5 of the ECHR, but who either are not, or cannot be, detained under the MHA 1983.
DOLS do not apply in Scotland/Northern Ireland
They were implemented in England and Wales from 1st April 2009 but case law has significantly changed how they are applied, particularly from March 2014 – “a gilded cage is still a cage”
The DOLS legislation is acknowledged to be ‘not fit for purpose’ and there is new legislation in Parliament awaiting final approval (Liberty Protection Safeguards) but until this Bill becomes law and is enacted we have to work within the existing legislation.
Definition of Deprivation of Liberty
“.. To determine whether there has been a deprivation of liberty, the starting-point must be the specific situation of the individual concerned and account must be taken of a whole range of factors arising in a particular case such as the type, duration, effects and manner of implementation of the measure in question. The distinction between a deprivation of, and restriction upon, liberty is merely one of degree or intensity and not one of nature or substance (ECtHR HL v UK 2004))
Case law has provided guidance as to what constitutes a deprivation of liberty under DOLS

DoLs apply to…
Anyone caring for people in care homes or hospitals where service users lack capacity to consent to placement, and the individual could be said to be being deprived of their liberty, whatever the reason for that situation.
The patients most likely to be affected are those with severe learning disabilities or autism, brain injury, or dementia
DOLS themselves do not apply in a person’s own home or day centre but an alternative process of requesting an order of the Court of Protection can be used.

DoLs Assessment
There are six assessments to be completed including age, eligibility, no refusals, mental health, mental capacity and best interests
Assessments to be completed within 21 days
Minimum of two assessors and all must be trained in DOL safeguards
Mental health and best interests assessors must be different people
The assessors must have relevant experience with client group….

The six assessments
1. Age – 18 or over
2. Eligibility – relates to the person’s status or potential
status under the MHA 1983 ie whether the person should
be covered by that Act rather than the MCA, or would be
inconsistent with that Act
3. No refusals – to establish whether there is another
authority for decision making for that person eg a valid
advance decision, a valid decision by an LPA or Deputy
appointed by the Court of Protection

4. Mental Capacity Assessment
To determine whether the person lacks capacity to consent to the arrangements proposed for their care; using the definitions set out under the MCA (2005)
can be undertaken by anyone eligible to act as Mental Health or Best Interests Assessor;
Assessor can be someone who knows the person

5. Mental Health Assessment
To identify whether the person is suffering from a mental disorder within the meaning of the MHA 1983 ie any disorder or disability of mind, apart from dependence on alcohol or drugs, and includes learning disabilities. It is not a determination of the need for mental health treatment;
To be carried out by a doctor who is either approved under section 12 of MHA or be a registered medical practitioner with experience in diagnosis and treatment of mental disorder; and must have completed appropriate MCA 2005 mental health assessor training;
Assessor can be familiar with person concerned.
6. Best Interests assessment
To determine whether a deprivation of liberty is or is likely to occur
If so, is it
in the best interests of the person,
is it necessary to prevent harm to the person, and
is it a proportionate response
To be undertaken by an AMPH or social worker, nurse, OT, or chartered psychologist with the skills and experience required by the regulations and who has completed the approved training
Best Interest Assessor can be an employee of the managing authority or supervisory body but must not be involved in the care or treatment of the person, nor in decisions about their care

Deprivation of Liberty March 2014
‘Cheshire West’ Supreme Court Judgement:
Is the person subject to continuous supervision and control
Is the person free to leave (would you prevent the person from leaving if they tried to)
• Not relevant
compliance or lack of objections
the relative normality of the placement
the reason or purpose behind the particular placement
ALSO: applies only where carers/care package is funded by State, ie excludes any privately funded care packages
Effects
Patient need not be trying to leave to be subject to DOLS;
Comparison should be with the expectation of liberty of
any other adult and not with a similarly disabled person in
a similar care setting.
Brought Supported Living and Shared-Lives into the scope
of the legislation, though not of the DOLS Schedules
(different process but with same aims);
Underlined the importance of the State’s involvement;
Massive increase (x10 in West Sussex) in DOLS applications
post Cheshire West;
14

DOLS reviews/Liberty Protection
Safeguards
Law Commission Mental Capacity Act and
Deprivation of Liberty Consultation (2015)
Law Commission Mental Capacity Act and
Deprivation of Liberty Report (2017)
Joint Committee on Human Rights agreed system
is broken and should be replaced June 2018)
Mental Capacity (Amendment) Bill July 2018

Progress through Parliament
House of Lords July 2018 - Autumn 2018 – 1st and 2nd readings; committee
stage and report stage
House of Commons stages – Jan – March 2019 - 1st and 2nd readings; committee
stage and report stage – including a definition of deprivation of liberty
HoL made two amendments – including a different definition of deprivation
of liberty
2nd April 2019 – HoC rejected Lords’ proposed definition
The House of Lords considered and agreed to the Commons amendments
on 24 April.
The Bill awaits Royal Assent - the final stage of a Bill's passage through
Parliament when the Bill becomes an Act (law).
House of Lords Hansard 24th April 2019
The meaning of a deprivation of liberty will remain as defined under Article 5
of the European Convention on Human Rights, as it is under Section 64(5) of
the Mental Capacity Act.
I assure noble Lords that the Government are still committed to providing
clarification regarding the meaning of a deprivation of liberty for both people
and practitioners. Amendment 1C makes it clear that the code of practice
must lay out in clear terms, and provide detail of, when a deprivation of
liberty is and is not occurring; this guidance will reflect existing case law,
including the Ferreira decision, which addresses the provision of life-
sustaining treatment. We will set out the meaning of a deprivation of liberty
in a positive framing and in a way that is clear for people and practitioners.
We will also include case studies in the code to help illustrate this.

House of Lords Hansard 24/4/19
The first is about when the code of practice will be published. Obviously, as
the noble Baroness, Lady Finlay, pointed out, the department is collaborating
very closely with the sector in the preparation of the code; that is already
happening. We are working with many organisations and individuals. The
drafting will be considered by expert reference groups and people with lived
experiences, to ensure that we get the most practical and workable code of
practice. The department has already convened a working group involving a
wide range of stakeholders. We expect to have output from the working group
by this summer. After Royal Assent, I will place a letter in the Commons
Library as requested; this will contain timescales for the code of practice,
including when a draft code will be published for consultation. I hope that is
reassuring.
Baroness Blackwood of North Oxfordshire

How do the LPS differ from DOLS?
LPS will be used in any care setting, including supported living, extra care accommodation and domestic settings such as a person’s own home (DoLS is restricted to care homes and hospitals
Responsible body: this will be the commissioner or funder of care who will organise assessments, reviews, authorisations, renewals and monitoring. NHS Trusts, private hospitals, CCGs, health boards and LAs will have a greater list of duties.
Conveyance: LPS includes the explicit power to transport (convey) a person between places LPS will apply to any care setting (not just hospitals and care homes)
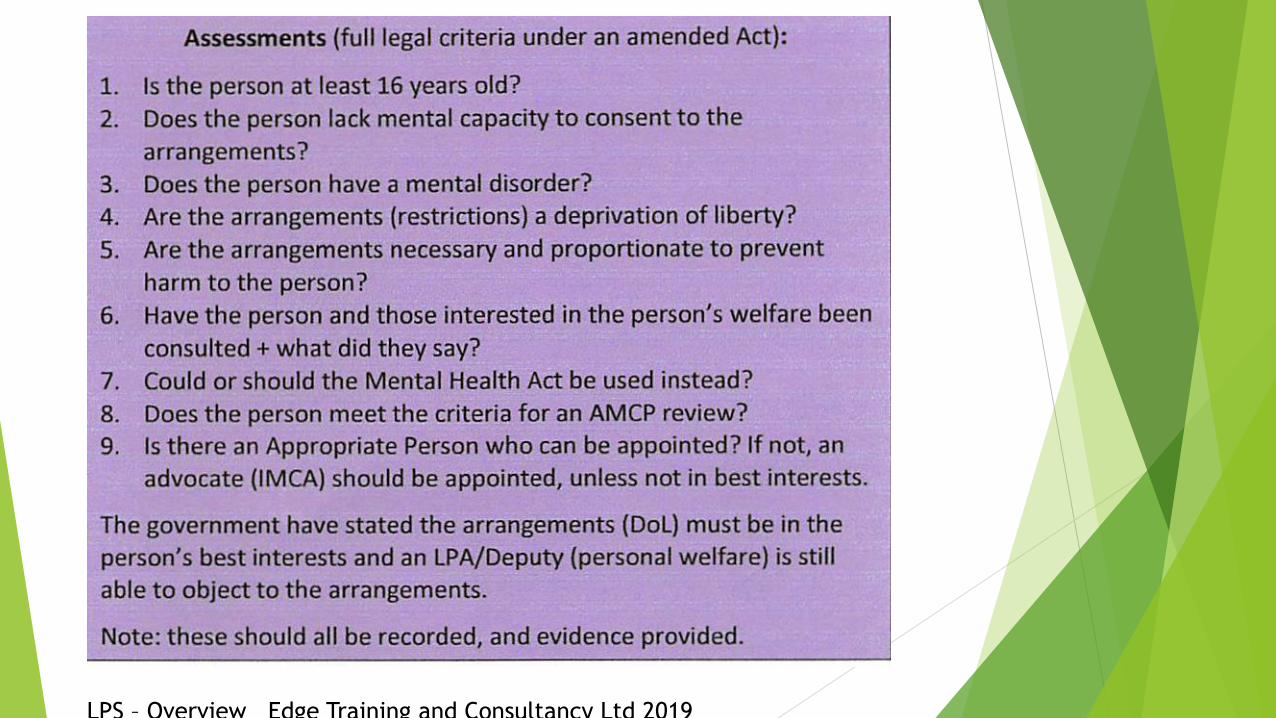
Age: LPS will apply from age 16 (currently 18+ for DOLS)
Best Interests Assessment: removed in the LPA as a standalone assessment but will still be required as part of the wider MCA within which LPS will sit
Taken from Edge Training and Consultancy Ltd January 2019 ‘What stays and what changes’ www.edgetraining.org.uk
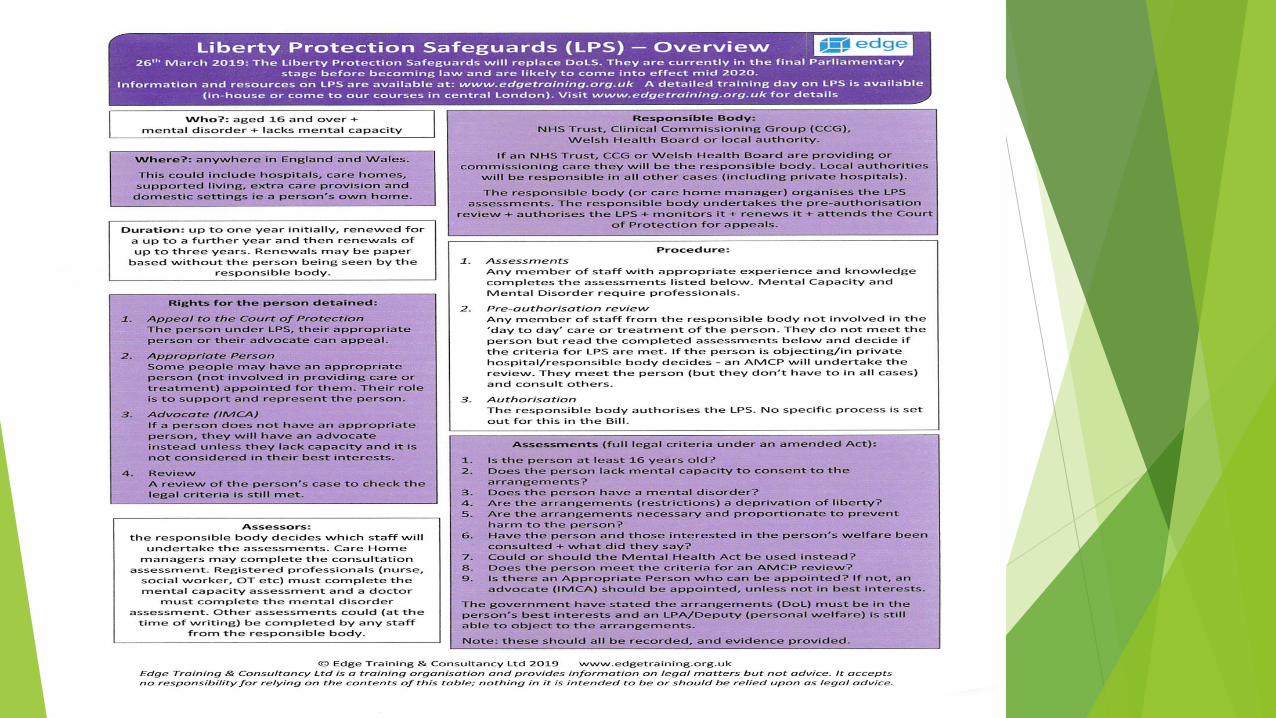

LPS – Overview Edge Training and Consultancy Ltd 2019
LPS –Overview Edge Training and Consultancy Ltd 2019
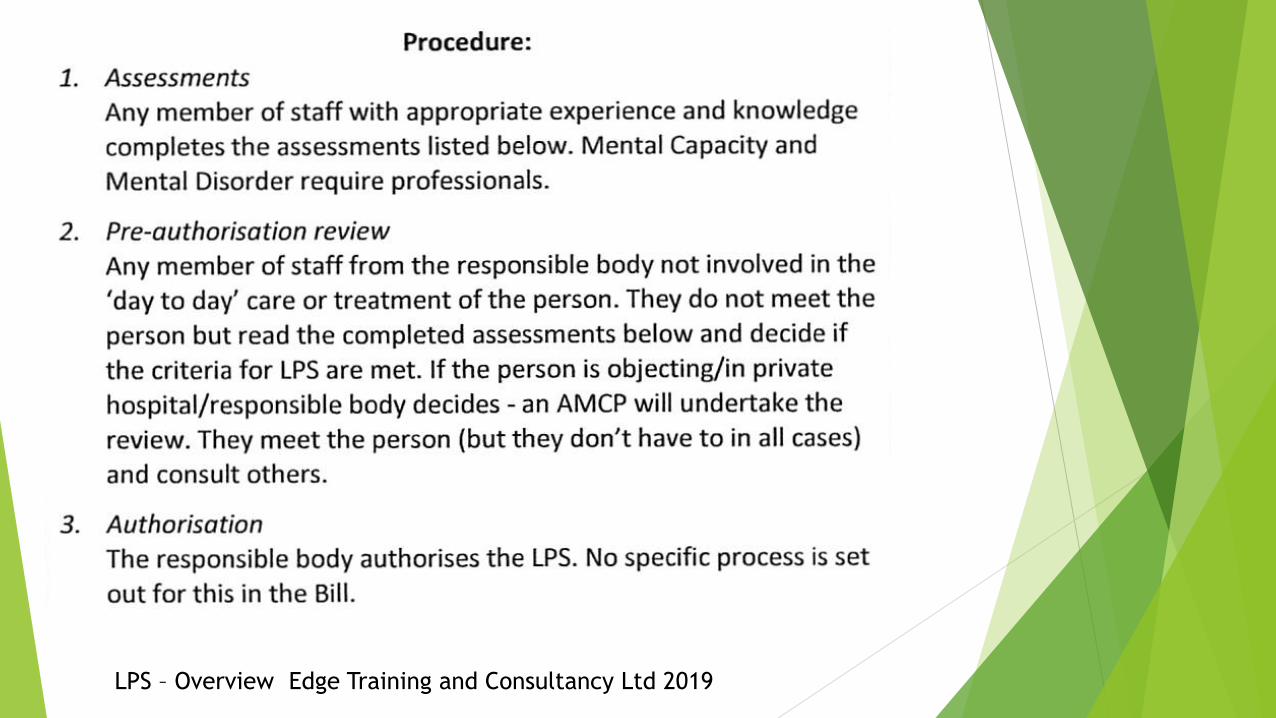
LPS – Overview Edge Training and Consultancy Ltd 2019

LPS – Overview Edge Training and Consultancy Ltd 2019
LPS – Overview Edge Training and Consultancy Ltd 2019
Summary
DOLS are ‘unfit for purpose’ but remain in place in
England and Wales until new legislation is enacted
Case law continues to evolve – check 39 Essex Street
website and/or Edge Training website
Liberty Protection Safeguards are on the cusp of being
passed through Parliament; and will then be given a date
for ‘enactment’ and a Code of Practice will be published
If you are working with people with brain injury,
dementia, intellectual disability, autism in any setting
then you will need to be aware of LPS which will operate
alongside care planning for people who lack the capacity
to consent to their placement, care or treatment.

Website resources
https://services.parliament.uk/bills/2017-19/mentalcapacityamendment.html
www.mentalhealthlaw.co.uk
https://www.39essex.com
http://www.edgetraining.org.uk/

















