50
Donna E. Reece, M.D. Princess Margaret Hospital T t ON T oronto, ON 16 October 2008 16 October 2008

Donna E. Reece, M.D.Princess Margaret Hospital
T t ONToronto, ON
16 October 200816 October 2008

Multiple Myeloma in Canadap y
Incidence 4/100,0002,000/yr in Canada
Prevalence6500/yr in Canada6500/yr in Canada
1000 deaths per yearMedian age 65 yrsg yIncidence in younger adults appears to be i iincreasing
Kyle RA, Rajkumar SV. N Engl J Med 2004;351:1860–73Canadian Cancer Statistics; 2007. Available at www.cancer.ca

Multiple MyelomaMultiple Myeloma
Marrow plasma cells > 10% Symptomatic myeloma =“CRAB”
Anemia (Hgb < 100)Bone lesionsCreatinine (> 176 umol/L)Creatinine (> 176 umol/L)Calcium > 2.8 mmol/L

Interaction between Myeloma Cell and Bone M Mi i tMarrow Microenvironment

Advances in Prognosis
International Staging System (ISS)Stage Criteria MedianStage Criteria Median
I Serum β2-microglobulin <3.5 mg/L 62 mo.Serum albumin ≥ 3.5 g/dL
II Not stage I or III 44 mo.
III Serum β2-microglobulin ≥ 5.5 mg/L 29 mo.
Cytogenetic abnormalities
t(4;14)=15% p53 deletion=10%

Factors Affecting Myeloma Management in Canada
D il bilitDrug availabilityApproval from Health CanadaFunding from provinces
Myeloma drugs approved in Canadaye o a d ugs app o ed Ca adaMelphalanCyclophosphamideBisphosphonates (pamidronate, zolendronic acid, clodronate)Bortezomib (2nd line +)Bortezomib (2 d line +)Bortezomib + melphalan + prednisone (1st line therapy without ASCT)Lenalidomide for relapsed myeloma
Access programsSAP for thalidomide (but no funding)EAP for lenalidomide is closingTrial of bortezomib + melphalan + prednisone (limited number of centers)

Results of “Traditional” Initial TherapypyOverview
Dex-based induction+
Melphalan + Prednisoneuntil plateau
ASCT
Overall response rate 80% Overall response rate 40 50%Overall response rate 80%CR/nCR 20%-30%Median PFS 20-36 mos
Overall response rate 40-50%CR/nCR 5%Median PFS 12-15 mosed a S 0 36 os
Median OS 48-60 mosMedian PFS 12 15 mosMedian OS 30-36 mos

Efforts to Improve Initial TherapyEfforts to Improve Initial Therapy
ASCT Melphalan + Prednisone
O ti i ASCT ( iTandem ASCTMaintenance therapy using novel agents
Optimize ASCT (eg. using melphalan 100 mg/m2)Add novel agents to M+Pnovel agents
New induction regimens containing novel agents
Add novel agents to M PUse IMiD + dexamethasone
Novel Agents in Multiple MyelomaNovel Agents in Multiple Myeloma
Thalidomide Bortezomib LenalidomideThalidomide Bortezomib Lenalidomide
EffiEfficacy:- As single agents, with steroids, in combinations
- As initial therapy or for relapsed/refractory MMAs initial therapy or for relapsed/refractory MM

Novel Agents in MyelomaAgent Class Effects ToxicityAgent Class Effects ToxicityThalidomide IMiD Decreased adhesion,
cytokines production,angiogenesis
Teratogenicity, PN, sedation, rash, constipation, DVTangiogenesis
Increased anti-myeloma immunitymyeloma immunity
Bortezomib Proteasomeinhibitor
Decreased adhesion, cytokine production,
Fatigue, PN, GI toxicity inhibitor y p ,
angiogenesis, NFkB, DNA repair
Decrease in neutrophils, platelets and lymphocytes
Lenalidomide
(CC-5013)
IMiD Decreased adhesionIncreased T cell proliferation, NK cell
t t i it IFN d
Myelosuppression, DVT
( )cytotoxicity, IFN-γ and IL-2

Activity of Novel Agents in Relapsed/Refractory Myeloma PatientsMyeloma Patients
Agent CR/nCR PR Overall
Thalidomide1
Thalidomide +Dex2
< 5%< 5%
28%40-50%
30%50%Thalidomide +Dex < 5% 40 50% 50%
Bortezomib3,4
B t ib + D 5 6
5% / 5%5% / 5 10%
20-25%35 55%
30-40%40 50%Bortezomib + Dex5,6 5% / 5-10% 35-55% 40-50%
Lenalidomide76% 18% 25 40%Lenalidomide
Lenalidomide + Dex8,9
6%19%
18%51%
25-40%70%
1Glasmacher A, et al,Br J Haematol 132: 584-593,2005;2 Palumbo A, et al. Hematol J 2004; 5:31 8-320; 3Richardson PG, et al. N Engl J Med 352:2487-98, 2005; 4Richardson P, et al. Blood 110:3557-60, 2007; 5Jagannath S et al. Haematologica 91:929-32, 2006;6Kropff MH, et al. Leuk Res 29:587-90, 2005; 7Richarson PG, et al. Blood 108; 3458-64, 2006; Weber DM, et al. N Engl J Med 357:2133-42, 2007; Dimopoulos M, et al. N Engl J Med 357:2123-32, 2007.

The Changing Landscape of Therapyg g p pyInitial Myeloma Therapy in Canada
Elderly patients ineligible for ASCTInduction therapy before ASCTInduction therapy before ASCTInitial therapy in “transplant uncertain” patients
Non-melphalan containing therapyNon melphalan containing therapyMay be of 2 broad types
Continuous “suppressive” therapy with IMiDs + steroidsCombination therapy with novel agents
High overall and CR/nCR rates

IMF 99-06: Treatment of Newly Diagnosed Myeloma Patients 65–75 Years
N=500
3 232
2
MP ArmStandard MP
at 6-wk intervals x 12
MP-Thal Arm MP as Arm 1 + Thal at MTD but ≤400 mg/day,
MEL100 x 2 ArmVADx2; cyclophosphamide 3 g/m2; Melphalan, 100 mg/m2
stopped at end of MP
Facon T et al. Lancet 2007;360:1209-1218.
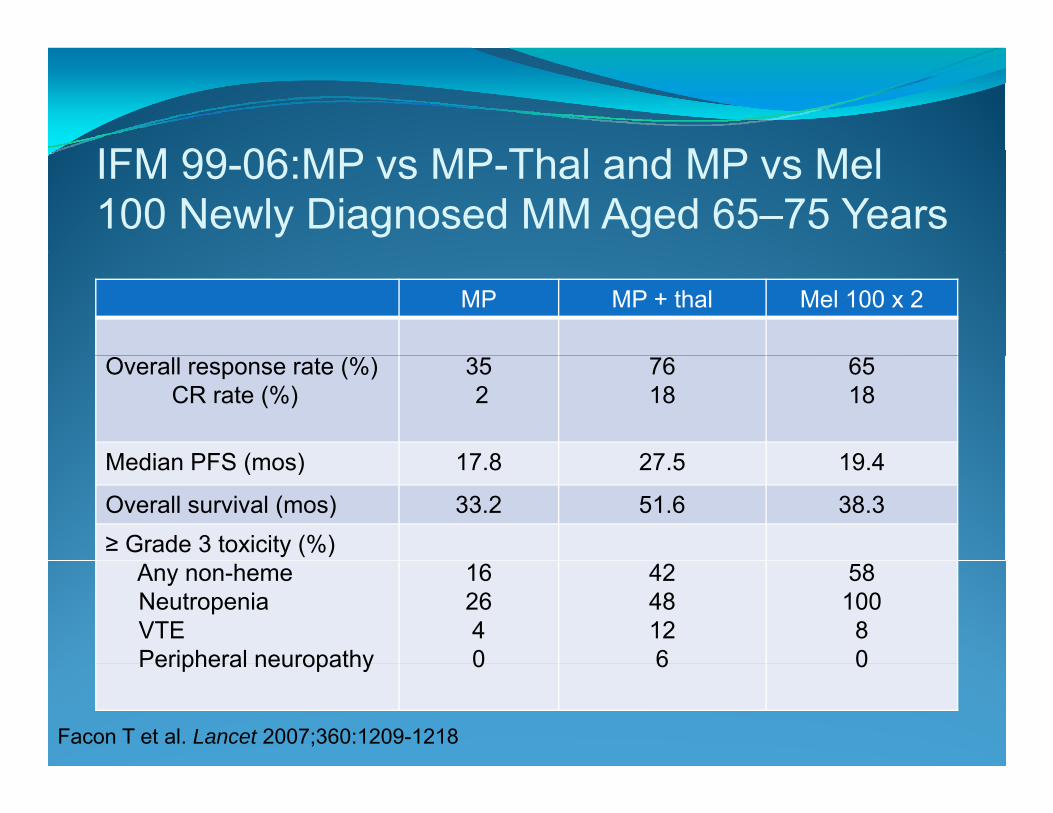
IFM 99 06 MP MP Th l d MP M lIFM 99-06:MP vs MP-Thal and MP vs Mel 100 Newly Diagnosed MM Aged 65–75 Years
MP MP + thal Mel 100 x 2
Overall response rate (%)CR rate (%)
352
7618
6518
Median PFS (mos) 17 8 27 5 19 4Median PFS (mos) 17.8 27.5 19.4
Overall survival (mos) 33.2 51.6 38.3≥ Grade 3 toxicity (%)
Any non-hemeNeutropeniaVTEPeripheral neuropathy
162640
4248126
58100
80Peripheral neuropathy 0 6 0
Facon T et al. Lancet 2007;360:1209-1218
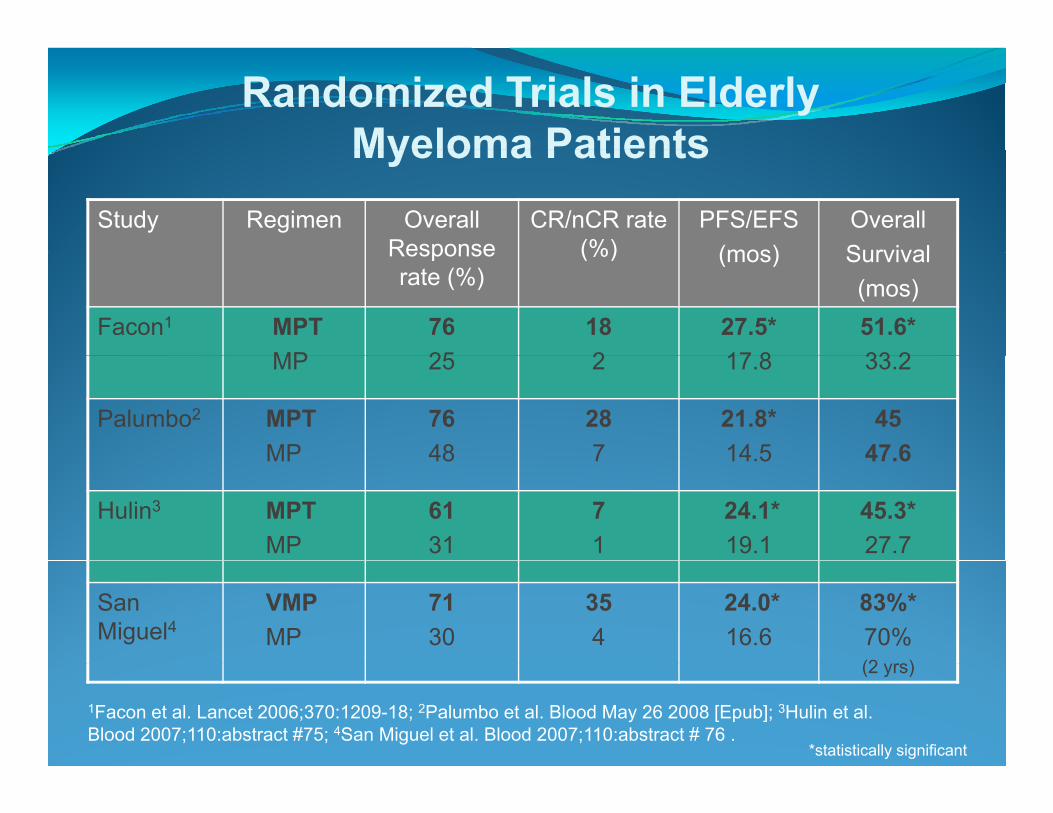
Randomized Trials in Elderly Myeloma PatientsMyeloma Patients
Study Regimen Overall Response
CR/nCR rate (%)
PFS/EFS(mos)
OverallSurvivalResponse
rate (%)(%) (mos) Survival
(mos)Facon1 MPT
MP7625
182
27.5*17 8
51.6*33 2MP 25 2 17.8 33.2
Palumbo2 MPTMP
7648
287
21.8*14 5
4547.6MP 48 7 14.5 47.6
Hulin3 MPTMP
6131
71
24.1*19.1
45.3*27.7
San Miguel4
VMPMP
7130
354
24.0*16.6
83%*70%(2 )(2 yrs)
1Facon et al. Lancet 2006;370:1209-18; 2Palumbo et al. Blood May 26 2008 [Epub]; 3Hulin et al. Blood 2007;110:abstract #75; 4San Miguel et al. Blood 2007;110:abstract # 76 .
*statistically significant

Randomized Trials in Elderly Myeloma Patients: Toxicity ComparisonsToxicity Comparisons
Study Rx Duration of Rx
Thaldose
≥ Gr 3 non-heme toxicity
≥ Gr 3 Neutropenia
VTE(%)
≥ Gr 3 PNof Rx dose
(%) heme toxicity
(%)Neutropenia
(%)(%) PN
(%)
Facon1 MPT 72 400 mg 42 48 12 6Facon MPTMP
7272
400 mg 4216
4826
124
60
Palumbo2 MPT 52 100 mg 49 16 12 10MP 52+ 25 17 2 1
Hulin3 MPTMP
7272
100 mg 5315
15 74
22MP 72 15 4 2
San Miguel4
VMPMP
5454
‐‐ 4636
4038
11
140
1Facon et al. Lancet 2006;370:1209-18; 2Palumbo et al. Lancet 2006; 367:825-31; 3Hulin et al. Blood 2007;110:abstract #75; 4San Miguel et al. Blood 2007;110:abstract # 76 .
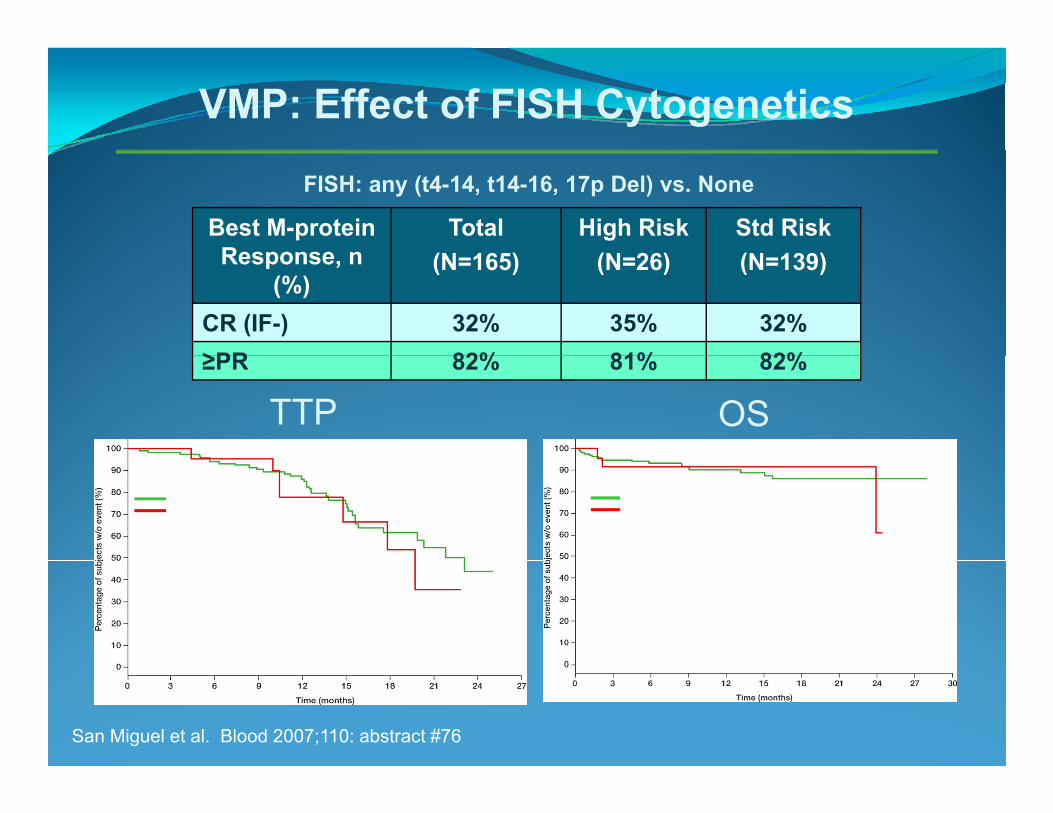
VMP: Effect of FISH Cytogenetics
FISH: any (t4-14, t14-16, 17p Del) vs. None
Best M-protein Response n
Total( 16 )
High Risk( 26)
Std Risk( 139)Response, n
(%)(N=165) (N=26) (N=139)
CR (IF-) 32% 35% 32%≥PR 82% 81% 82%
TTP OS≥PR 82% 81% 82%
VMP standard riskVMP high risk
VMP standard riskVMP high risk
VMP standard risk (N=142): 23.1 months (34 events)VMP high risk (N=26): 19.8 months (7 events)HR = 1.297 (95% CI: 0.55, 3.06)
VMP standard risk (N=142): not reached (16 events)VMP high risk (N=26): not reached (3 events)HR = 1.009 (95% CI: 0.278, 3.663)
San Miguel et al. Blood 2007;110: abstract #76

New Approaches in Elderly Myeloma Patients: Summary
Addition of novel agent to melphalan and prednisone improves outcome
Whether MP followed by novel agent at relapse produces similar or inferior results is uncertain
Toxicity is greaterToxicity is greaterThalidomide regimens require thromboprophylaxisPeripheral neuropathy is a concern
Data needed for risk groupsIn Canada, options include:
T t bt i f di f th lid idTry to obtain funding for thalidomideClinical trial

Management of Elderly Myeloma Patients in Canada: Clinical Trials
NCIC MY11 trial (closed)Melphalan 5 mg/m2 days 1-4Melphalan 5 mg/m days 1-4Lenalidomide 10 mg/days 1-21
O th Bi t h t i l f VOrtho Biotech trial of VMP
Celgene MM020 international trialCelgene MM020 international trialLenalidomide + weekly dex until progressionLenalidomide + weekly dex for 18 monthsMPT

New Approaches before ASCTNew Approaches before ASCT
Background: Patients in CR/nCR/VGPR afterASCT have better PFS and OS
Hypothesis: Achievement of CR/nCR/VGPR before ASCT will translate into improved outcome after ASCT

New Approaches before ASCTpp
Multiple induction regimens containing novel agentsMultiple induction regimens containing novel agents produce high CR/nCR rates (VAD-thal, CTD, VTD)Randomized trials in progressRandomized trials in progress
Thal + Dex vs VAD (MAG)VAD vs Bortezomib + Dex (IFM)( )VTD vs Thal + Dex (Bologna)
Canadian trials“DBd” = Lipo. doxorubicin + bortezomib + dex“CYBOR-D” = cyclophosphamide + bortezomib + dex
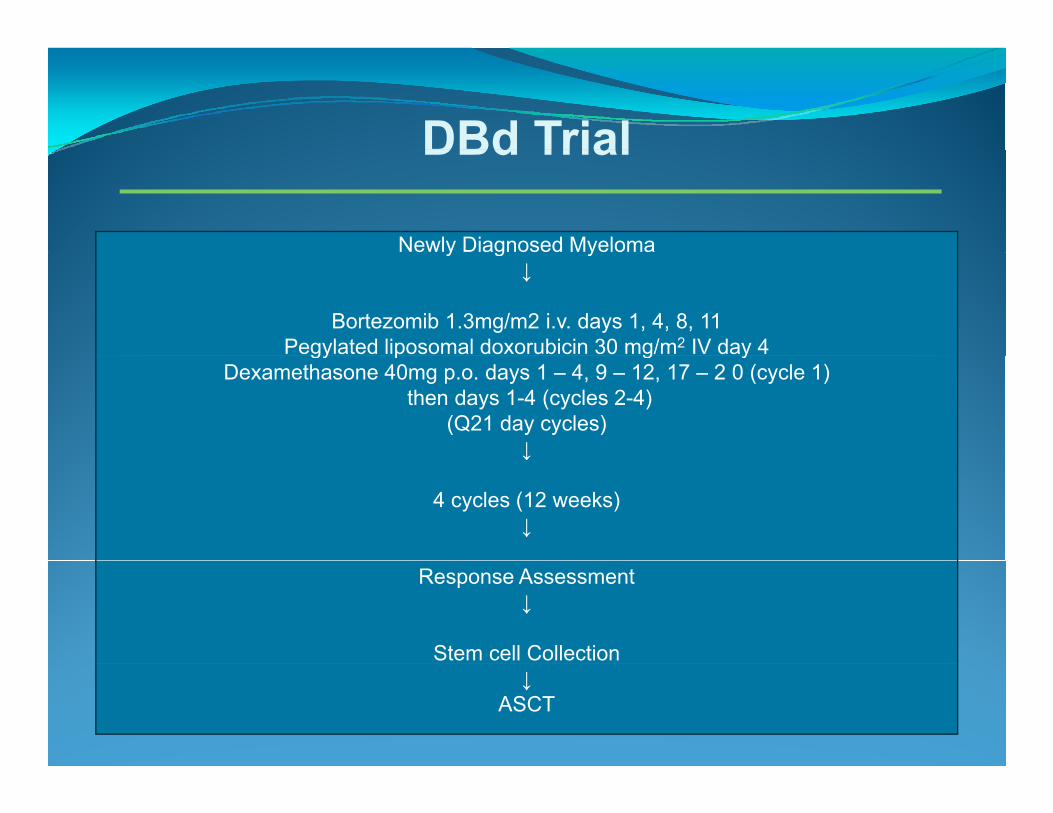
DBd TrialDBd Trial
Newly Diagnosed Myelomay g y↓
Bortezomib 1.3mg/m2 i.v. days 1, 4, 8, 11Pegylated liposomal doxorubicin 30 mg/m2 IV day 4gy p g y
Dexamethasone 40mg p.o. days 1 – 4, 9 – 12, 17 – 2 0 (cycle 1)then days 1-4 (cycles 2-4)
(Q21 day cycles)↓↓
4 cycles (12 weeks)↓
Response Assessment↓
Stem cell Collection↓
ASCT

DBd ResponsesDBd Responses
Responses Response by FISH
Response After After Response t(4;14) Del p53Response After DBd
(N=50)
After ASCT(N=41)
Response t(4;14)(N=4)
Del p53(N=4)
Overall 39(78%) (92.7%)
CR/nCR 11(22%) 12(29 3%)
Overall 4(100%) 3(75%)
CR/ CRCR/nCR 11(22%) 12(29.3%)
PR 28(56%) 26(63.4%)
CR/nCR -- --
PR 4(100%) 3(75%)
Belch A, et al. IMW, 2007

CYBOR D TrialCYBOR-D TrialNewly Diagnosed MyelomaNewly Diagnosed Myeloma
↓Cyclophosphamide 300 mg/m2 p.o. weekly, days 1, 8, 15, 22
Bortezomib 1.3mg/m2 i.v. days 1, 4, 8, 11D th 40 d 1 4 9 12 17 2 0Dexamethasone 40mg p.o. days 1 – 4, 9 – 12, 17 – 2 0
(Q28 day cycles)↓
4 cycles (16 weeks)↓
Response AssessmentResponse Assessment↓
*Stem cell Collection↓
Off Study To Transplant OR Continue Meds for further 8 cycles

CYBOR-D Trial
N= 33 patients to date23 evaluable for toxicity/response after ≥ 1 cycle
Response after Cycle 4CR/nCR 9/14 ( 64%)VGPR 3/14 (21%)y p y
14 have completed 4 cyclesVGPR 3/14 (21%)PR 2/14 (14%)MR 0/14 ( 0%)SD/NR 0/14 ( 0%)
At least nCR in 64% of patientsAt least PR in 100%
• Toxicity (≥ Gr 3 )• Heme 24%, Neutropenia 20%
Hyperglycemia17%• Hyperglycemia17%• Sensory neuropathy 5%• Infection 5%
Trial modified to:Weekly bortezomib 1.5 mg/m2
Weekly dex after cycle 2• Overall incidence of neuropathy 69%
Reeder CB, et al. Blood 2007;110: abstract #3601.
y y

Induction Therapy in “Transplant Uncertain”Induction Therapy in Transplant Uncertain Patients: ECOG IMiD Trials
ECOG: Thalidomide + DexDexamethasone given days 1-4, 9-12 and 17-20 of a 28-day cycle in odd cycles, and days 1-4 in even cyclesyOverall response rate 63% (8% CR), with median TTP 22 months
ECOG E4A03: Rev + Dex versus Rev+ weekly dex
Rajkumar et al. Blood 2006;110 abstract#; Rajkumar et al. Blood 2007;110: abstract#74;

E4A03: Schema for RD vs RdN= 445 pts
RAN @ 4 monthsDOM
Rev + Dexx4 cycles
CR/PR@ 4 monthsPts eligible for SCT proceed to SCT*
IZAT
Less
proceed to SCT
Thal + Rev + Low dose Dex CR/PR/St blT
ION
than PR
Dexx 4 cycles
dose Dexx 4 cycles
CR/PR/Stable
N

E4A03 Trial Results
Response rate with RevD was 82% versus 71% withResponse rate with RevD was 82% versus 71% with RevdBut, more early deaths in RevD group, y g p
Although Dex was reduced for toxicity, it was was not routinely decreased after 4 cycles
Median TTP was around 2 yearsThe results in the small subset of patients who underwent ASCT after 4 cycles were similar to theunderwent ASCT after 4 cycles were similar to the Revd group
However the group that continued Revd was biasedHowever, the group that continued Revd was biasedtowards responding (good-risk patients)

Overall Survival: Primary Therapy beyond 4 Cycles of RD vs RdCycles of RD vs. Rd
93% Rd
82% RD
93% Rd
0 073 (Wil 0 073 (Wil ) 0 569 (l k)p=0.073 (Wilcop=0.073 (Wilcoxon); p=0.569 (log-rank)xon); p=0.569 (log-rank)
Rajkumar V, et al. ASCO 2008, abstract #8504

IMiD Induction Therapy without ASCT
Thal/Dex1 Dex1 RevD2,3 Revd2,3
Overall response
63% 46% 82% 71% → 89%
rateCR rate
8% 3% 4% 2% → 22%
Med TTP 22 4 6 5 25Med TTP(mos)
22.4 6.5 -- 25(Med remission
duration)
Med OS 32 -- 93%Med OS(mos)
-- 32 93%(2 yr)
1Rajkumar V, et al. Blood 2006;108 abstract #795; 2Rajkumar V, et al. Blood 2007;110: abstract #74; 3Rajkumar V, et al. ASCO 2008: abstract #8504

Initial Therapy in “Transplant Uncertain”Initial Therapy in Transplant Uncertain Myeloma Patients
Continuous suppression with IMiD + DexOverall response rates of 65-85%O ti l d f d th t i b t tiOptimal dose of dexamethasone uncertain, but continuous “full dose” likely detrimentalDurability of responses appear to be just under 2 years
Aggressive combinations, without ASCT, not well-studied in Canadain Canada
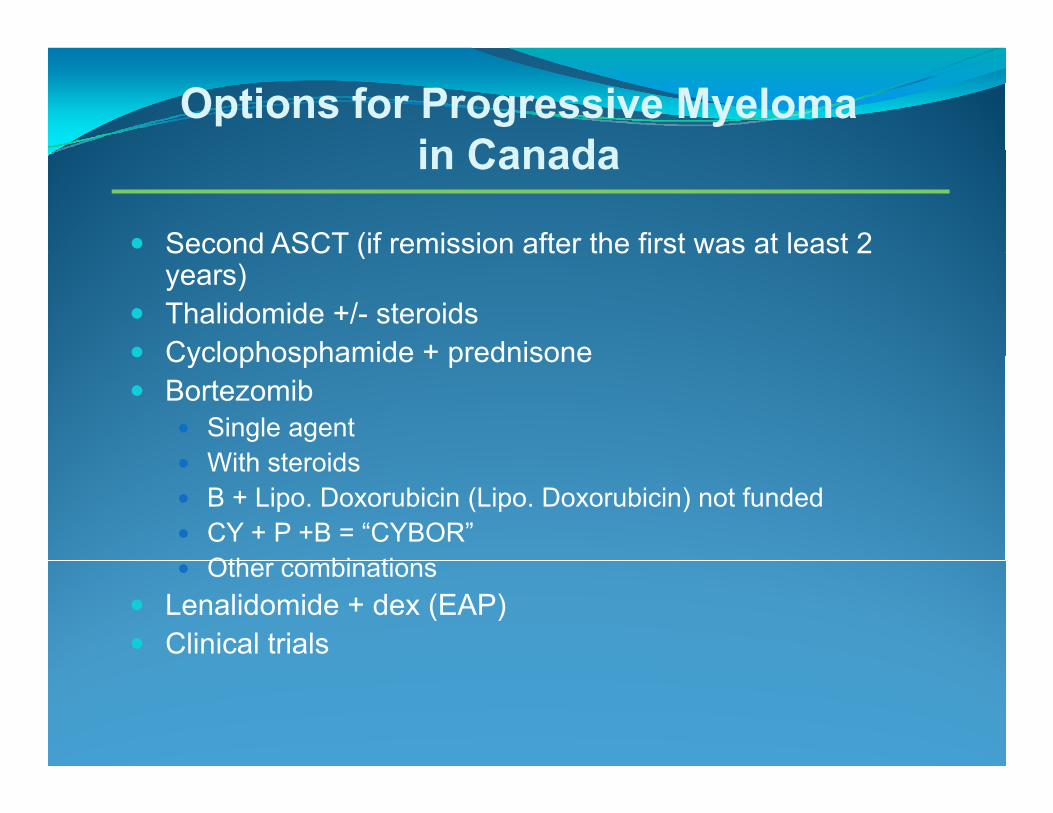
Options for Progressive Myelomain Canadain Canada
Second ASCT (if remission after the first was at least 2Second ASCT (if remission after the first was at least 2 years)Thalidomide +/- steroidsCyclophosphamide + prednisoneCyclophosphamide + prednisoneBortezomib
Single agentWith steroidsWith steroidsB + Lipo. Doxorubicin (Lipo. Doxorubicin) not fundedCY + P +B = “CYBOR”Oth bi tiOther combinations
Lenalidomide + dex (EAP)Clinical trials

Second ASCT for Relapsed MyelomaPrincess Margaret Hospital (N=61)cess a ga e osp a ( 6 )
Median age 56 (35-71) yearsMedian time to relapse after first ASCT 33 mos (10-86)Overall response rate 88% (8% CR)TRM 3%TRM 3%Median PFS from ASCT 15.8 mos, OS 4.2 yearsResults better if PFS after 1st transplant ≥2 years:Post 2nd ASCT Progression Free Survival
Grouped by =< or > 2 yrs PFS post 1st ASCT1.0
Post 2nd ASCT Overall Survival
Grouped by =< or > 2 yrs PFS post 1st ASCT1.0
Surv
ival
.8
.6
.4
.2
=< or > 2 yrs PFS
> 2yrs PFS
Surv
ival
.8
.6
.4
.2
=< or > 2 yrs PFS
> 2yrs PFS
Mikhael et al. Blood 2007;110:abstract #110
PFS post ASCT2 (years)
6543210
Cum
S
0.0
=< 2yrs PFS
OS post ASCT2 (years)
86420
Cum
S
0.0
=< 2yrs PFS

Oral Cyclophosphamide and PrednisoneOral Cyclophosphamide and Prednisone After ASCT at PMH (n = 59)
304050
01020
PR MR SD PD
Median PFS 19 mos; median OS 29 mosPR rate 40%; MR rate 20%
Trieu et al. Mayo ClinProc 2005:80:578-82.
Median PFS 19 mos; median OS 29 mosPR rate 40%; MR rate 20%

“CYBOR-P”W kl B t ib 1 5 / 2 + CY + PWeekly Bortezomib 1.5 mg/m2 + CY + P
N=13Overall RR 85% (CR/nCR rate 54%)
pf s:
0. 75
1. 00
)Only 2 progression events1-year PFS 83% and OS 100%
76 cycles evaluable for toxicity
0. 50
76 cycles evaluable for toxicityGr 4 ↓ ANC 1.3%Gr 4 ↓ pl 2.6%
0. 00
0. 25
Gr 3 ↓ pl 1.3%Gr 1 PN in 7 patients (55%)Shingles in 4 patients
pf sday
0 100 200 300 400 500
Legend: Product -Li mi t Est i mat e Curve Censored Observat i ons
g p
Reece D, et al. JCO,2008 Epub ahead of pressProgression-free survival

Lenalidomide + Dex vs Dex + Placebo in Relapsed MMe apsed
75
100
%)
100MM-00975%) MM-010
25
50
75
Pl b /D
Len/Dex
Patie
nts
(%
25
50
75
Pl b /D
Len/Dex
Patie
nts
(%
Time to progression (months)0 10 20 30
0Placebo/Dex
5 15 25 0 5 10 15 20 250
Placebo/Dex
Time to progression (months)
P
Median time to progression (months)Median time to progression (months)
Len/Len/DexDex Placebo/DexPlacebo/Dex PP--value*value*// //
MMMM--009009 11.111.1 4.74.7 <0.001<0.001
MMMM--010010 11.311.3 4.74.7 <0.001<0.001
*`P-value from log-rank testWeber D, et al. NEJM 2007;357:2133Dimopoulos M, et al. NEJM 2007;357:2123

Myelosuppression with Lenalidamide +/-y ppCorticosteroids: MM 016 Expanded Access Trial at
Princess Margaret Hospital (N=70)
Parameter (%)Response rate 62 4%Response rate
CR/nCRPR
62.4%5.4%57%
G d 3 4 T i itGrade 3-4 ToxicitesNeutropeniaFebrile neutropeniaInfection
49%16%26%
Thrombocytopenia 39%Supportive care needs
Platelet transfusion 41%G-CSF to maintain full dose of lenalidomide 63%
Reece D, et al. Blood 2006;108: abstract #3548, #3550

Lenalidomide Combinations in Relapsed/Refractory MM
AnthracyclinesDVd-R – PLD, vincristine, DEX, lenalidomideRAD – lenalidomide, adriamycin, DEX*, y ,
AlkylatorsRCD – lenalidomide, cyclophosphamide, DEX*CPR cyclophosphamide lenalidomide prednisoneCPR – cyclophosphamide, lenalidomide, prednisone
Novel agentsLenalidomide, bortezomib (+/- DEX)* L lid id if i DEX*Lenalidomide, perifosine, DEX* Lenalidomide, bevacizumab, DEX*
*ASH abstracts 2007

“CPR”: Phase I-II Trial Dose Levels28 d C l28-day Cycle
Dose Level
Cyclophosphamide Lenalidomide PrednisoneLevel
N Median#
Dose (mg/m2)Days 1, 8, 15
DoseDays 1-21
Dose (mg)Q 2 days
cyclesy , , y y
1 3 9 150 15 100
2 3 6 300 25 1002 3 6 300 25 100
3 6 4 300 25 100
3(Expanded)
3 1 300 25 100
Reece, et al. ASH 2008, submitted
DLT not identified; all patients remain on study

FISH Ab liti i M l C llFISH Abnormalities in Myeloma Cells
t(4;14) p53 deletiont(4;14) p53 deletion

t(4;14) Multiple Myeloma
15% of myeloma patientsOften associated with 13q deletionTendency for younger individualsOften IgA lambda subtypeLytic bone lesions less prominentAggressive biology
Beta 2-microglobulin level provides additional prognostic information after tandem ASCT
May respond to therapy but relapses quicklyMay respond to therapy, but relapses quickly
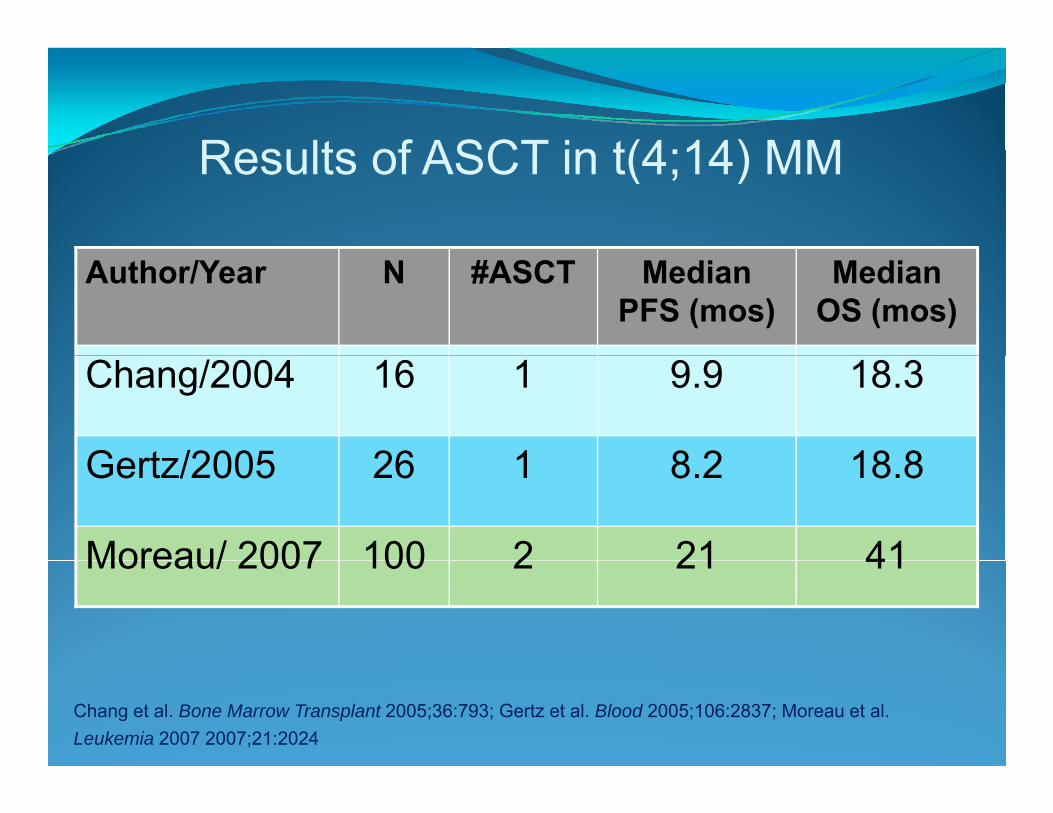
Results of ASCT in t(4;14) MMResults of ASCT in t(4;14) MM
Author/Year N #ASCT Median PFS (mos)
Median OS (mos)
Chang/2004 16 1 9.9 18.3
Gertz/2005 26 1 8 2 18 8Gertz/2005 26 1 8.2 18.8
Moreau/ 2007 100 2 21 41Moreau/ 2007 100 2 21 41
Chang et al. Bone Marrow Transplant 2005;36:793; Gertz et al. Blood 2005;106:2837; Moreau et al. Leukemia 2007 2007;21:2024

Treatment of Progressive t(4;14) MMTreatment of Progressive t(4;14) MMRegimen N Response Median Median g p
rate TTP (mos) OS (mos)Cyclophosphamide + prednisone/MP1
11 0 (63% SD) -- --prednisone/MP1
Thalidomide or dex1 17 41% 4.7 --
Bortezomib +/-steroids2
6 67% 10.5 15.5
1Jaksic W, et al. J Clin Oncol 2003; 23:7069; 2 Chang H, et al. Leuk Res 2007; 31:779-782.
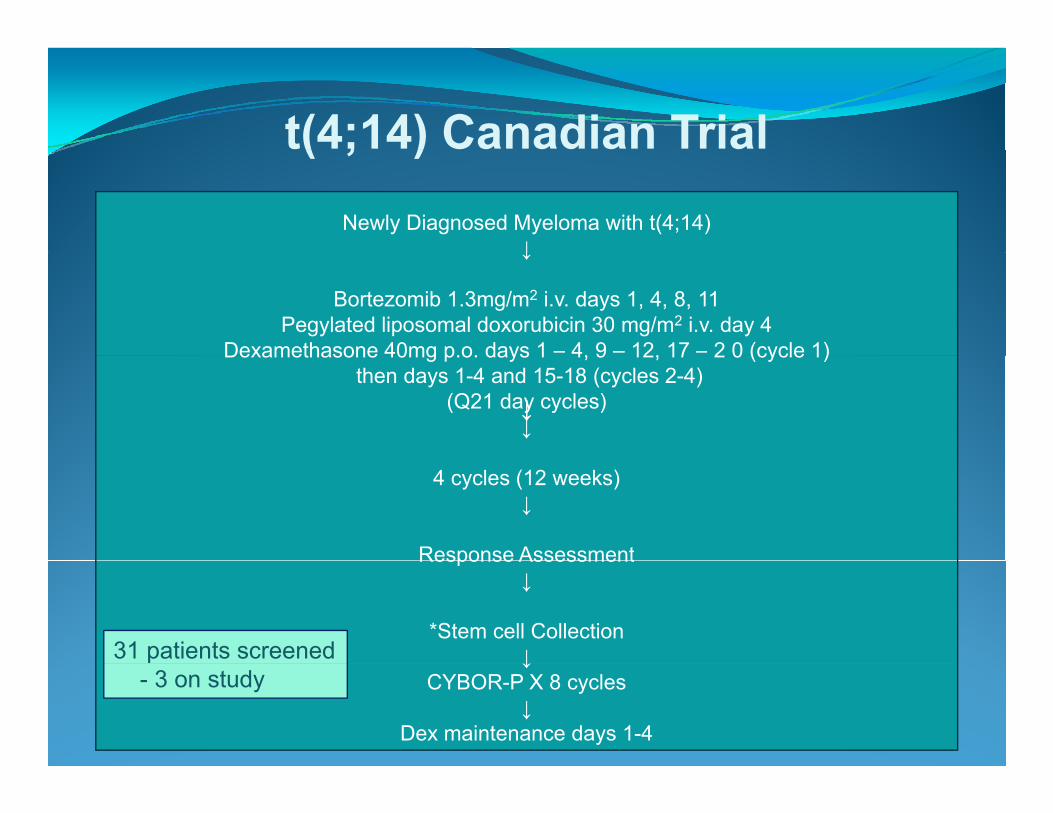
t(4;14) Canadian Trial( ; )Newly Diagnosed Myeloma with t(4;14)
↓↓
Bortezomib 1.3mg/m2 i.v. days 1, 4, 8, 11Pegylated liposomal doxorubicin 30 mg/m2 i.v. day 4
Dexamethasone 40mg p.o. days 1 – 4, 9 – 12, 17 – 2 0 (cycle 1)Dexamethasone 40mg p.o. days 1 4, 9 12, 17 2 0 (cycle 1)then days 1-4 and 15-18 (cycles 2-4)
(Q21 day cycles)↓↓↓
4 cycles (12 weeks)↓
Response AssessmentResponse Assessment↓
*Stem cell Collection↓31 patients screened ↓
CYBOR-P X 8 cycles↓
Dex maintenance days 1-4
p- 3 on study

p53 Deletion Multiple Myeloma
Loss of a tumor suppressor geneCommonly found in cancerNoted in about 10% of myeloma patientsPrognosis with tandem ASCT also affected by beta 2 i l b li l l2-microglobulin levelBest treatment uncertain—novel agents recommendedrecommended

Overall Survival with Len/Dex C di A l i f MM016 (N 120)Canadian Analysis of MM016 (N=120)
t(4;14) p53 deletion
Bahlis et al. ASH 2007, personal communication.

Determinants of Treatment of Relapsed/Refractory Multiple Myeloma
Di l d fDisease - related factorsDuration of benefit of prior therapyDisease biology (e.g. cytogenetics) gy ( g y g )
Patient - related factorsPrior therapyR l i i t/f ilRenal impairment/failureConcomitant medical problems (e.g. peripheral neuropathy, decreased blood counts, diabetes)
Treatment – related factorsTime to responseToxicity profileToxicity profile
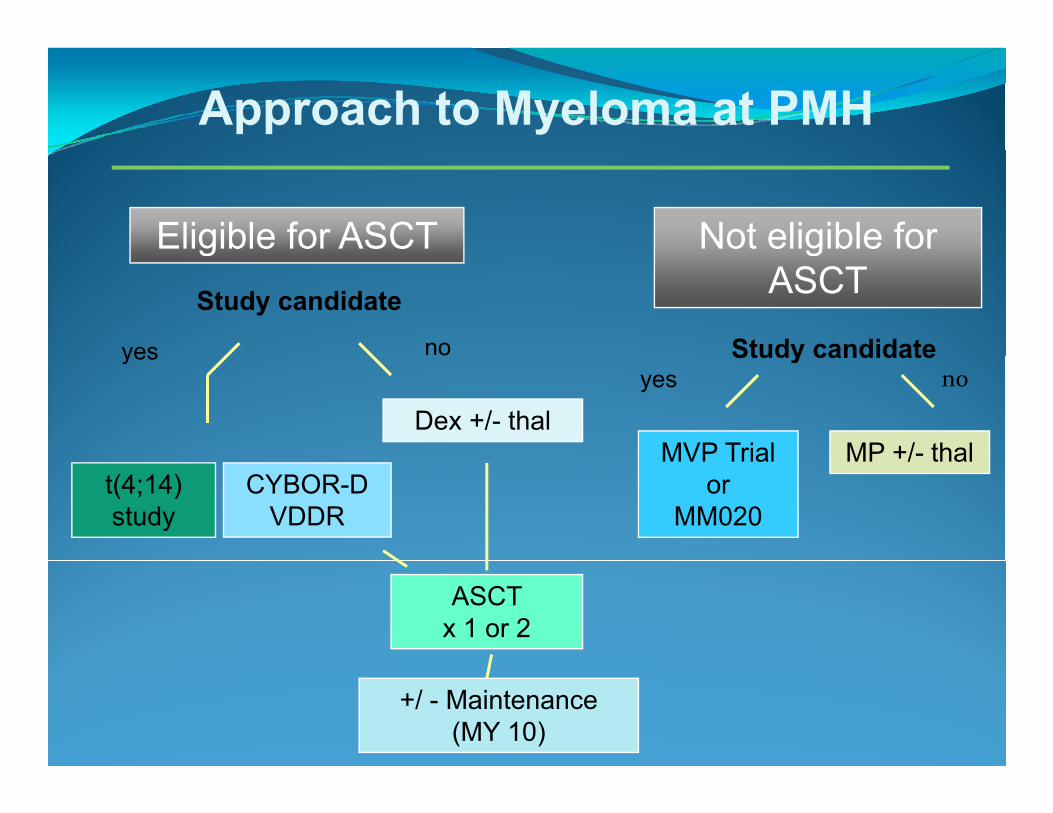
Approach to Myeloma at PMH
Eligible for ASCT Not eligible for gStudy candidate
gASCT
Study candidateyes no
Dex +/- thalMP +/- thal
Study candidateyes o
MVP Trial
noyes
CYBOR-DVDDR
t(4;14) study
MP +/ thalMVP Trialor
MM020
ASCT x 1 or 2
+/ - Maintenance(MY 10)

PMH Approach to Progressive Myelomapp g y
N i ASCTAfter ASCT No prior ASCT
≥ 1 year benefit
Trial CandidateSecond Repeat M+P
≥ 2 year benefity
Trial CandidateSecondASCT
Thalidomide +/- steroidsBortezomib + tipifarnib (MMRC)Bortezomib + Geminex (Mayo)
no yesp
Bortezomib +/- steroids +/- CYCY + P
Lenalidamide + Dex (EAP)CY + P + Lenalidomide (“CPR”)
Carfilzomib (MMRC)(Semaphore PI3K inhibitor [MMRC])
(Pomalidomide [MMRC])(Bortezomib + Vorinistat [MMRC])
(Lenalidamide + HuLuc 60)
Management of Myeloma in 2008 in CanadaSummary/Conclusions
New agents and combinations are available for allNew agents and combinations are available for all age groups and disease settings
Funding limitations are a problemFunding limitations are a problemAccess programs/clinical trials necessary to increase drug availability before funding available
The optimal approach for induction and disease progression has not yet been defined and may be different in biologic subtypesdifferent in biologic subtypesEfforts to match the best therapy with the disease biology desirablebiology desirable

















