52
Don’t Miss Out on NASP’s Fall Conference!
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | linette-carpenter |
| View: | 213 times |
| Download: | 0 times |

Don’t Miss Out on NASP’sFall Conference!

Impact of the Affordable Care Act on Specialty Pharmacy
Moderator:Jim Smeeding, RPh, MPA
Professional AffairsNASP

Impact of the Affordable Care Act on Specialty Pharmacy
Lauren BarnesSenior Vice PresidentAvalere Health, LLC

Coverage Expansion
Medicaid Expansion Exchanges
Payment and Delivery Reforms
Payment Reforms ACOs
Coverage Expansion and Delivery System Reforms Provided in the ACA are Likely to Impact Specialty Pharmacy Business
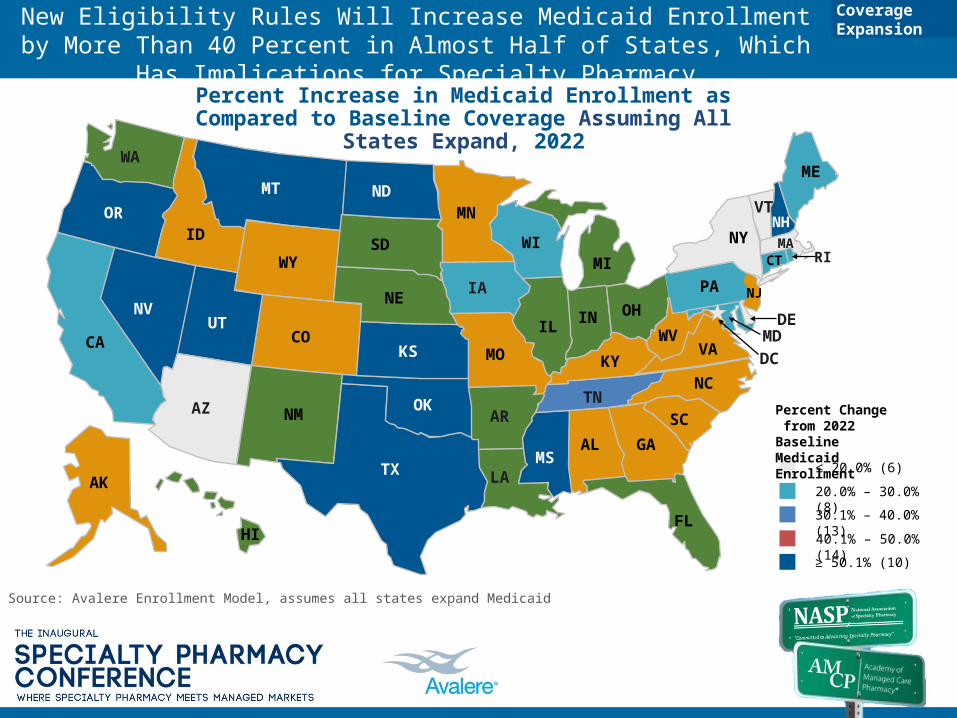
New Eligibility Rules Will Increase Medicaid Enrollment by More Than 40 Percent in Almost Half of States, Which Has Implications for Specialty Pharmacy
WA
OR
NV
ID
MT
WY
COUT
AZ NM
TX
OK
KS
NE
SD
NDMN
IA
MO
AR
LAMS
AL GA
SC
NCTN
IL
WIMI
IN OH
PA
KYVA
FL
CA
NY
VT
ME
NH
MARI
WVDE
MD
NJ
AK
HI
CT
DC
Percent Increase in Medicaid Enrollment as Compared to Baseline Coverage Assuming All States Expand, 2022
40.1% – 50.0% (14)
≥ 50.1% (10)
30.1% – 40.0% (13)
≤ 20.0% (6)
Percent Change from 2022 BaselineMedicaid Enrollment
Source: Avalere Enrollment Model, assumes all states expand Medicaid
20.0% – 30.0% (8)
Coverage Expansion

Specialty Pharmacies Are Expected to Feel Increased Cost Pressure with Reimbursement Changes
Alabama received CMS approval to implement a reimbursement methodology based on AAC in September 2010
Oregon received CMS approval for a similar plan to reimburse pharmacies based on AAC in January 2011
Idaho implemented AAC in September 2011
Louisiana implemented AAC in September 2012
State Medicaid programs have led movement away from AWP to AAC (examples below)
These changes have adjusted ingredients costs and dispensing fees for pharmacies in Medicaid
» Ingredient Cost: Based on survey of invoices, does not include SPPs in survey
» Dispensing Fee: Based on review of the cost of dispensing, typically does not include SPPs
While these new reimbursement formulas are not including SPPs in surveys, they do reimburse SPPs using these metrics.
AAC = Average Acquisition CostAWP = Average Wholesale PriceCMS = Centers for Medicare & Medicaid ServicesSPP = Specialty Pharmacy Provider
Coverage Expansion

Approximately 18 Million Are Expected to Enroll in Subsidized Coverage Through Exchanges, Which May Increase Pressures on Specialty Pharmacy to Control Costs
WA
OR
NV
ID
MT
WY
COUT
AZ NM
TX
OK
KS
NE
SD
NDMN
IA
MO
AR
LAMS
AL GA
SC
NCTN
IL
WIMI
IN OH
PA
KYVA
FL
CA
NY
VT
ME
NH
MARI
WVDE
MD
NJ
AK
HI
CT
DC
Enrollment in Subsidized Coverage, 2022
301,000-450,000 (9)
≥ 451,000 (10)
151,000-300,000 (14)
≤ 150,000 (18)
Enrollment in Subsidized Coverage (2022)
Source: Avalere Enrollment Model, assumes all states expand Medicaid
Coverage Expansion

Upside/Downside Risk
Penalties Only
Nonpayment
Baseline/Performance Period
Medicare Payment and Delivery Reform Programs Will Impact Hospitals Over The Next Ten Years
Source: Centers for Medicare & Medicaid ServicesACO = Accountable Care Organization; VBP=Value-based Purchasing
2008 2009 2011 2013 20172015 20182016
Hospital Inpatient Quality Reporting Program1
ACOs2
Readmission Penalties for Low Performers
20142010 2012
Bundled Payment for Care Improvement
Hospital Acquired Conditions3
Hospital Outpatient Quality Reporting Program1
Hospital VBP4
Private Payers are also engaging in a variety of payment and delivery reform to curb growing costs and encourage value.
Payment and Delivery Reform

Payment Reform Forces Hospitals to Build New Competencies, Which Could Alter Thinking about Drugs
Impact on Health Systems
Reductions in Payment
Changes in Volume/ Access
Increase in Transparency
Transfer of Risk
Aggregate & Capture Data
Work Closely with Physicians
Focus on Costs
Be Responsive to Different Payment Models
Select and Comply with a Core Set of Clinical Guidelines
Hospitals will have to be able to:
© Avalere Health LLCPage 9
Identify Partners Who Can Offer Integrated Solutions
Payment and Delivery Reform
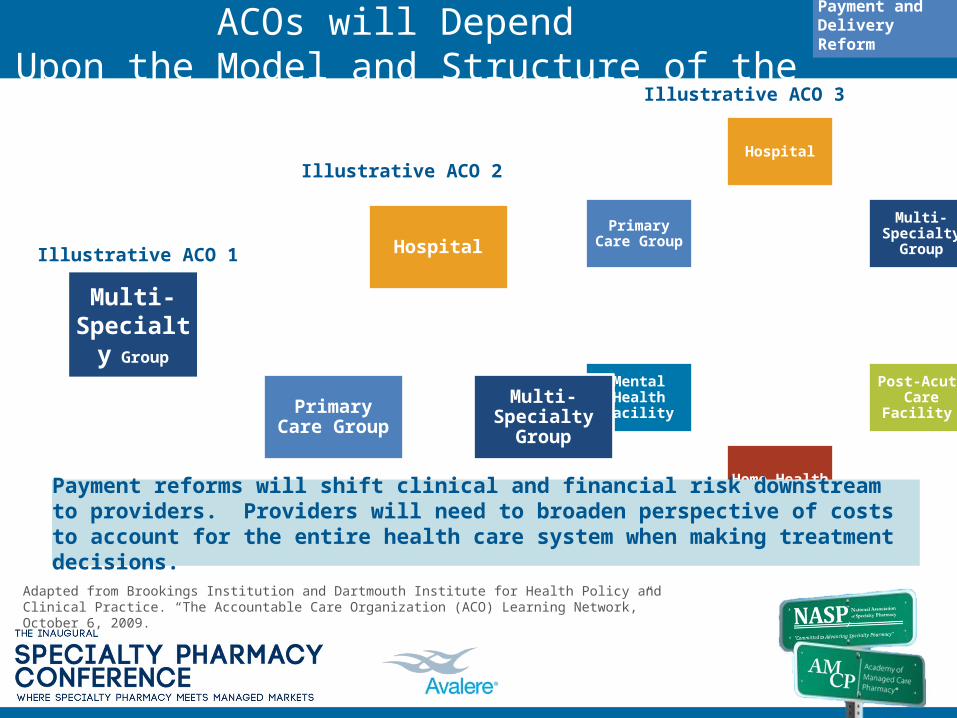
Specialty Pharmacy’s Role within ACOs will Depend Upon the Model and Structure of the ACO
Adapted from Brookings Institution and Dartmouth Institute for Health Policy and Clinical Practice. “The Accountable Care Organization (ACO) Learning Network,” October 6, 2009.
Multi-Specialty
Group
Illustrative ACO 1
Hospital
Multi-Specialty Group
Post-Acute Care Facility
Home Health
Mental Health Facility
Primary Care Group
Illustrative ACO 3
Hospital
Multi-Specialty Group
Primary Care Group
Illustrative ACO 2
Payment reforms will shift clinical and financial risk downstream to providers. Providers will need to broaden perspective of costs to account for the entire health care system when making treatment decisions.
Payment and Delivery Reform
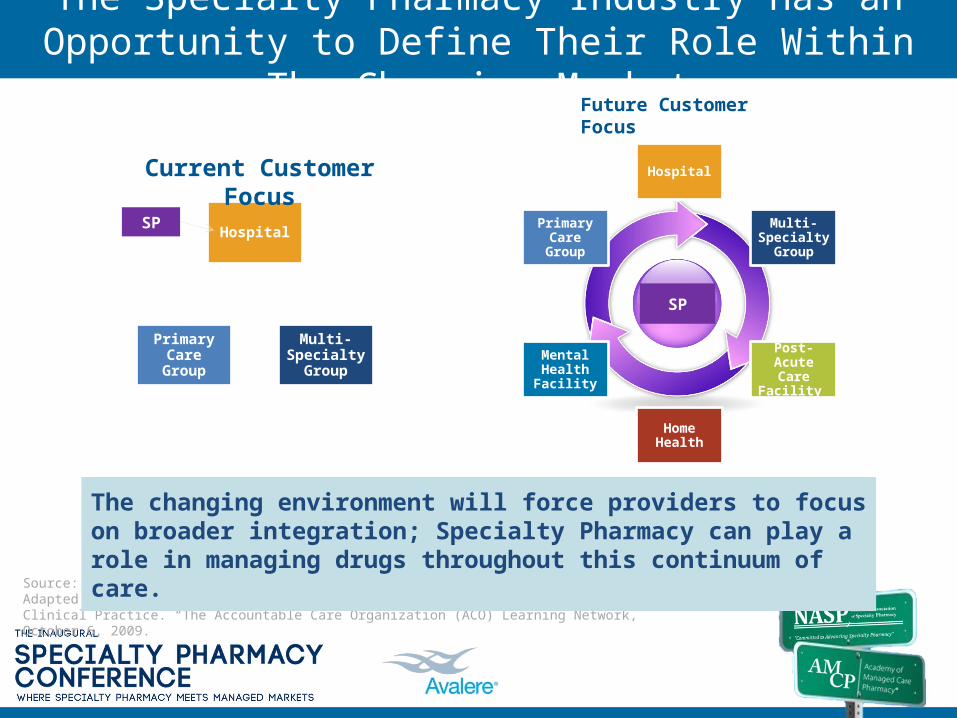
The Specialty Pharmacy Industry Has an Opportunity to Define Their Role Within The Changing Market
Source:Adapted from Brookings Institution and Dartmouth Institute for Health Policy and Clinical Practice. “The Accountable Care Organization (ACO) Learning Network,” October 6, 2009.
Hospital
Multi-Specialty
Group
Post-Acute Care Facility
Home Health
Mental Health Facility
Primary Care Group
Future Customer Focus
Hospital
Multi-Specialty
Group
Primary Care Group
Current Customer Focus
The changing environment will force providers to focus on broader integration; Specialty Pharmacy can play a role in managing drugs throughout this continuum of care.
SP
SP

No Medicare ACOs
AK
HI
CA (23)
AZ (8)
NV (3)
OR(2)
MT(1) MN
(5)
NE(2)
SD
ND
ID(1)
WY(1)
OK(1)
KS(1)
CO (2)
UT(1)
TX (16)
NM (3)
SC (3)
FL (32)
GA (11)
AL(1)
MS (2)
LA(2)
AR(3)
MO(4)
IA (7)
VA(6)
NC (6)TN (7)
IN (9)
KY (7)
IL (8)
MI (9)
WI (7)
PA (3)
NY (18)
WV
VT (2)
ME (4)
RI-2
DE - 1
MD - 9
NJ
MANH
WA(2)
OH(8)
D.C. - 2
Both MSSP and Pioneer ACOs
MSSP ACOs
7
18
NJ -10
Source: CMS Medicare Shared Savings Program website: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/index.html?redirect=/sharedsavingsprogram/Note: MSSP and Pioneer ACOs often serve Medicare beneficiaries in more than one state. Since the numbers embedded in the map capture this, they do not add up to equal the number of ACO entities approved by CMS through January1, 2013.
CT-8
States with Medicare ACOs
Between the Medicare Shared Savings Program and Pioneer ACOs, CMS Has Launched More than 250 ACOs
PR
2
ACOs

Health Systems Across the Country Exhibit Characteristics of ACOs
0AK
HI
CA
AZ
NV
OR
MT
MN
NE
SD
ND
ID
WY
OK
KSCO
UT
TX
NMSC
FL
GAALMS
LA
AR
MO
IA
VA
NCTN
IN
KY
IL
MIWI
PA
NY
WV
VT
ME
RICT
DEMD
NJ
MA
NH
WA
OH
D.C.
5-7
3-4
8-10
2
1
Source: Leavitt Partners Center for ACO Intelligence, “Growth and Dispersion of Accountable Care Organizations,” November 2011.
11+
ACOs
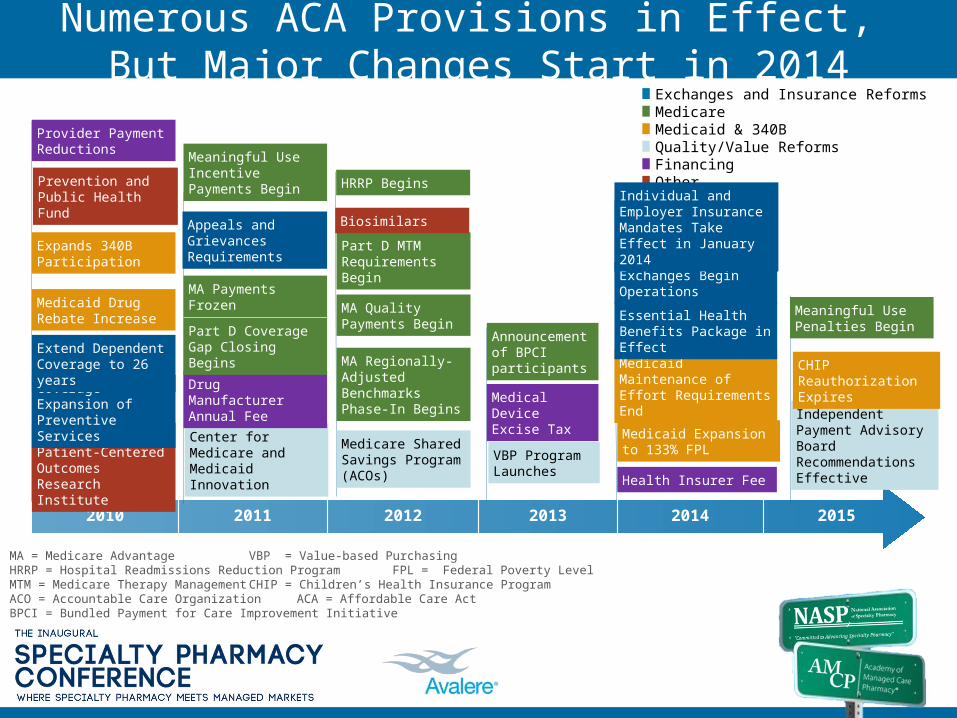
Numerous ACA Provisions in Effect, But Major Changes Start in 2014
2010 2011 2012 2013 2014 2015
MA = Medicare Advantage VBP = Value-based PurchasingHRRP = Hospital Readmissions Reduction Program FPL = Federal Poverty LevelMTM = Medicare Therapy Management CHIP = Children’s Health Insurance ProgramACO = Accountable Care Organization ACA = Affordable Care ActBPCI = Bundled Payment for Care Improvement Initiative
Exchanges and Insurance ReformsMedicareMedicaid & 340BQuality/Value ReformsFinancing Other
VBP Program Launches
Medicaid Maintenance of Effort Requirements End
Center for Medicare and Medicaid Innovation
Medicaid Drug Rebate Increase
Establish Patient-Centered Outcomes Research Institute
Drug Manufacturer Annual Fee
Independent Payment Advisory Board Recommendations Effective
Part D Coverage Gap Closing Begins
Medicaid Expansion to 133% FPL
Expands 340B Participation
Coverage Expansion of Preventive Services
Extend Dependent Coverage to 26 years
MA Payments Frozen
MA Regionally-Adjusted Benchmarks Phase-In Begins
MA Quality Payments Begin Essential Health Benefits
Package in Effect
Medicare Shared Savings Program (ACOs)
Exchanges Begin Operations
Part D MTM Requirements Begin
CHIP Reauthorization Expires
BiosimilarsAppeals and Grievances Requirements
Prevention and Public Health Fund
Medical Device Excise Tax
Health Insurer Fee
Provider Payment Reductions
Individual and Employer Insurance Mandates Take Effect in January 2014
HRRP Begins
Announcement of BPCI participants
Meaningful Use Incentive Payments Begin
Meaningful Use Penalties Begin

Panel Discussion
The intersection of businessstrategy and public policy
Data, Metrics, and Reporting: What Role will Specialty Pharmacy Play?
Brian Nightengale, RPh, PhD President
Xcenda, AmerisourceBergen Consulting Services

Every major aspect of ACA assumes broad access to credible data and sufficient stakeholder collaboration to ensure measurement and reporting

Questions Remain Regarding Impact on SP
• Complex therapeutic areas may offer the best opportunities to demonstrate quality and outcomes
• But, will these low volume, yet expensive specialty therapeutics area be a big focus out of the gate?
– If so, then SPs will likely play an increasingly collaborative role in
• Providing support for complex therapy management within the new coordinated care delivery models
• Providing the necessary data typically required for specialty focused diseases
• Will PCORI’s and other agencies priorities align with the market and/or be relevant to Specialty Pharmacy?
– Currently many initial pilot programs focus on primary care or care delivery• What impact might CER have on the drugs SPs offer to customers?
– Either increasing or limiting access– Changing contracts/rebates with manufacturers of drugs that did not perform well under
CER

Impact on Specialty Pharmacy
March 2009, Amerisource Bergen’s Managed Care Network (MCN™) primary market research
Payer reactions to the statement:“Private payers will use CER data to require enrollees to pay some or all of the additional costs of more expensive drugs, procedures, or technologies for which there is no evidence of superior effectiveness.”
N=43
How much do you agree with this statement?
March 2009 N=41 June 2008 N=68

Questions Remain Regarding Impact on SP
• Stakeholders will need to address care management and quality improvement issues related to small patient populations
– Across specialty therapeutic areas, data needs and reporting requirements differ significantly based on medical complexities
– Is there sufficient data and collaboration to effectively measure?
– Typical “population management” approaches may not apply
• What capital investments will be needed to address the increasing data and reporting demands and who will pay?

Are Credible and Reliable Data Available?
1. EMD Serono. “EMD Serono Specialty Digest, 7th Edition. Managed Care Strategies for Specialty Pharmaceuticals ” (Note: data represented in graphs was collected via an online survey of 93 health plans representing over 115 million lives).
Outcome Measures for Oncology Outcome Measures for Rheumatoid Arthritis

Impact of ACA on Specialty Pharmacy
Dean Erhardt, MBAD2 Pharma Consulting, LLC

D2 Mission Statement
D2 is a Life Sciences consulting firm consisting of accomplished industry personnel who provide hands on expertise in all aspects of channel management.
We provide strategic and tactical commercialization expertise to emerging and existing pharmaceutical,
biotech and specialty organizations focusing on the individuals client’s defined business objectives.
Brief on Healthcare Reform• The good
– In theory fewer uninsured Americans should lead to a lower-cost health care system
– No cap on benefits– No Pre-existing conditions– Kids stay on coverage through age 26– “Free” preventive healthcare
• The Bad– Wrong incentives???
• Patients’ rights advocates have expressed that the model incentivizes providers to save money by cutting corners in treatment
– Increase healthcare costs • 20 M people w/ incomes up to 400% FPL ($92K) to receive subsidies
– Decisions in the hands of unelected bureaucrats– Various cross subsidies (transferring wealth w/o using the tax code)
• Young, healthy pay more to cross subsidize older, sicker• The Ugly?
– Expands power with the IRS – multiple new taxes– 2700 pages of legislation yet to be defined– Approx. 2000 “at the description of the Secretary”

Confidential 25
Specialty Pharmacy Challenges
The other driver of change…
How the FDA pipeline of specialty drugs will impact the existing supply chain?

27Confidential 27 27
The Future of Specialty Pharmacy• Over 600 drugs in the specialty pharmaceutical pipeline
(phase II and phase III)
• Close to 50% of drugs in the pipeline are oral drugs
• Majority of drugs are for treatment of cancer
• Specialty pharmacy today represents about 25% of pharmacy spend but will increase to 40% of total spend by 2015
• Specialty pharmaceuticals will represent top selling drugs by revenue by 2014
Sources www.phrma.org Medco 2011 Drug Trend Report Bartholow M. Top 200 prescription drugs of 2009. Pharmacy Times website. http://www.pharmacytimes.com/issue/pharmacy/2010/May2010/RxFocusTopDrugs-0510.

Supplier:
Wholesaler
Manufacturers
Specialty Distributor
Supplier:
Specialty Distributors
Specialty Pharmacies
Supplier:
Wholesalers
Specialty Distributors
Specialty Pharmacies
Manufacturers
Supplier:
Wholesalers
Specialty Distributors
Distribution Channels for Specialty Products
Source: HDMA Estimated 2011
Key Considerations• How does a specialty pharmacy support patient
initiatives across an ACO?• What are the data requirements necessary to support
reporting ACO initiatives?• How/where does pharma (big/small) fit?

Potential Levers in SP Management
Medical Management
• Referral mgmt• Utilization mgmt• Case management• Disease mgmt• Step therapy• Prior authorization• Retro review
Consumer Engagement
• Awareness campaign• Engagement (Health by
Choice)• Shared decision making• Benefit design• Tiered copays• Preferred networks• Education programs
(wellness)• Transparency – quality
& cost
Network Management
• Renegotiate contracts• Case rates/commodity
pricing• Risk sharing
(capitation, ACO)• Gainsharing• Incentives – reward
achievement of targets• Bundled payments• Site of service
differentials• Transparency• Direct care to Centers
of Excellence

THANK YOU…
How Will Specialty Pharmacy Evolve In A Risk-Sharing Environment?
A Pharmaceutical Industry Colleague Perspective
Jeffrey A. Bourret, MS, RPh, FASHPSenior Director, Medical Affairs
Medical Lead, Specialty & Payer Channel CustomersPfizer Specialty Care
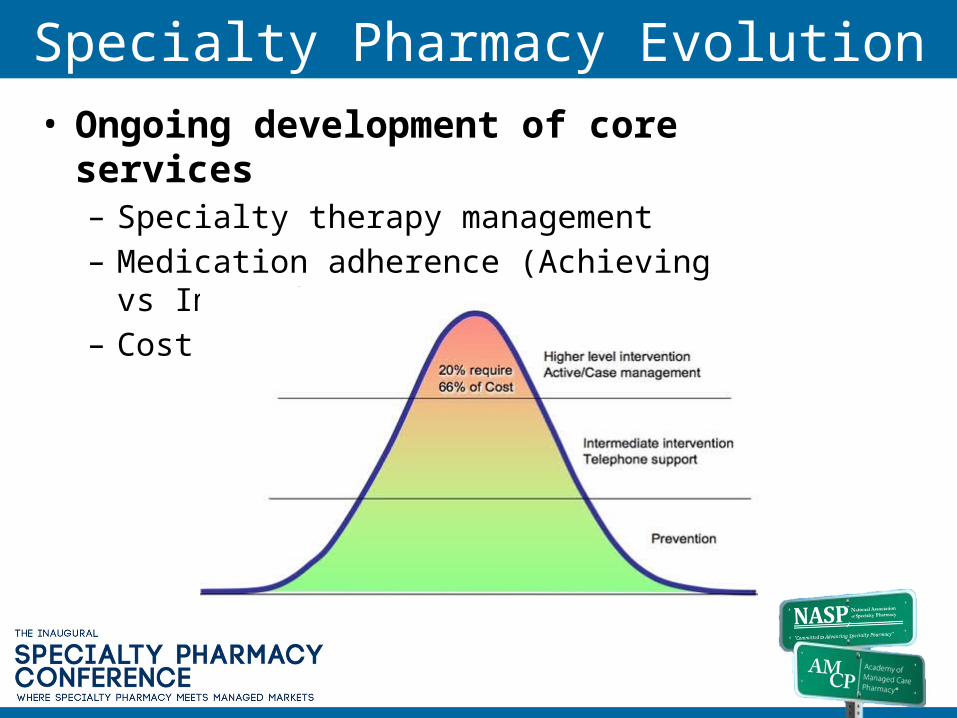
Specialty Pharmacy Evolution• Ongoing development of core services
– Specialty therapy management– Medication adherence (Achieving vs Improving)– Cost management
Development of Enhanced Capabilities1. Specialty therapy management expansion to therapy prescribed
for patient comorbidities for medical conditions targeted by CMS and ACOs
2. Patient behavioral change
3. Health services research on effective strategies and tactics for achieving medication adherence
4. Health outcomes research on impact of adherence on total health care utilization and costs
5. Research on SPP impact on improving quality scores
6. Strategies to enhancing patient care experience
Specialty Pharmacy Evolution: Patient Support
• Specialty Therapy Management– Patient education
– Telephonic adherence support
• Evolution– Expanded role in patient , family and caregiver education
– Certification of patients on appropriate use of medication
– Data capture & integration with medical/pharmacy
– Generation of data on patient outcomes
Medicare Shared Savings Program Final Rule
• Quality measures and reporting– CMS will score 23 quality measures in
calculating the performance standard, spanning four equally weighted domains:
• Patient/caregiver experience (7 measures)• Care coordination/patient safety (6 measures)• Preventive health (8 measures)• At-risk populations (12 measures)
• Specialty pharmacy can potentially impact each core domain & could be called on to play more active role

Finalized Measures Will Target High Impact Conditions
• Diabetes• Heart failure • Coronary artery disease• Ischemic vascular disease• Hypertension• COPD• Tobacco use
• Patient experience• Immunizations• Readmissions• Medication reconciliation• Use of EHRs• Screenings (cancer,
depression, fall risk, weight)
Most high impact conditions targeted by ACOs areco-morbidities for patients with medical conditions
requiring specialty therapy

Comparative Effectiveness Research
Drug Surgery
Device Surgery
Drug Device
Drug A Drug B

An Option Ripe for Specialty Pharmacy Evolution
• Patient education incentives• Medication use certification• Family & caregiver education• Patient self-reported assessments
of disease activity• Patient satisfaction survey• Health outcomes research
Drug (Limited Support) Drug + Enhanced Support

The Best Results Will Come From Effective Collaboration
Patient
DoctorsNurses
Pharmacists
PharmaCompanies
PBM
MCO
Retail Pharmacy
Specialty Pharmacy

Impact of ACA on Specialty Pharmacy
Presented by: Donald C. Balfour, M.D.President and Medical Director
Sharp Rees-Stealy Medical GroupApril 3, 2013

Sharp ACO Collaborations
• Commercial PPO Patients
• Sharp Community Medical Group (“SCMG”)
• Commercial PPO Patients
• SCMG and Sharp Rees-Stealy Medical Group (“SRSMG”)
• Pioneer ACO• Medicare Fee-
for-Service Beneficiaries
• Sharp HealthCare, SCMG, SRSMG

Goal of CMS ACO Program
CMS Shared Savings Program established in the Patient Protection and Affordable Care Act (“PPACA”) with the goal to provide:
1. Better care for individuals
2. Better health for populations
3. Lower growth in Medicare expenditures
Three-Part Aim

Pioneer ACO Footprint
• Began January 1, 2012• Collaboration between Sharp
HealthCare, SCMG and SRSMG– All SRSMG physicians, most SCMG
physicians (includes Graybill), and all Sharp hospitals
• 32,000 aligned beneficiaries– 74% with SCMG– 26% with SRSMG
Sharp HealthCare ACO

What Have We Accomplished?• Created
corporation• Named
leadership team• Developed
subcommittee structure
• Established provider and supplier network• Formed governing body, including consumer advocate
and patient representative

What Have We Learned?• Identified Opportunities
– 63% of 2011 inpatient costs ($78 million) originate from the ED– 51% of total Part A claims costs for 2011 ($123 million) are out-of-
network – Skilled nursing bed days per 1,000 were 2,608 in 2011 compared to a
5% sample of Medicare fee-for-service beneficiaries in San Diego County of 1,842 (42% higher)
• Medicare Advantage patients at 1,439 (81% higher)
– 150 beneficiaries had 5 or more ED visits in 2011 without a corresponding admit (one beneficiary had 53)
– 100 beneficiaries had 5 or more hospital admits in 2011 (one beneficiary had 17)
– 3.5% of beneficiaries generate 21% of Part A paid claims

Aim and Primary Drivers
Best Health, Best Care, Best Experience
Care Delivery Models
Care Coordination
Patient Engagement
Information Technology and Analytics
…………………………………………………………………………
…..
…………………………………………………………………………
…..
Alignment of Incentives

Years One and Two• Providers bill normally and receive standard fee-
for-service paymentsBilling
• Total cost of care for ACO beneficiaries is compared to a benchmark based on historical costs of the aligned population
Comparison
• If total expenses are less than target, and if quality metrics are achieved, a portion of the savings is returned to the ACO
Bonus
• The ACO is responsible for dividing the savings among ACO participantsDistribution
Year Three
• Must achieve quality targets as well as a minimum 2% annual savings in years one and two to receive population-based payments in year three
Payment Option
CMMI’s AIM is that 100% of Pioneer ACOs generate sufficient cost savings and quality
improvements to qualify for population-based payments in year three

Best Health,Best Care,
Best Experience
Don’t Miss Out on NASP’sFall Conference!

















