42
Dorith Shaham, M.D. Department of Radiology Hadassah – Hebrew Uviversity Medical Center

Dorith Shaham, M.D.
Department of RadiologyHadassah –
Hebrew Uviversity
Medical Center

LUNG CANCER
The most common fatal malignancy in the Western
world
Estimated 1.3 million deaths worldwide in 2000
In the US –
222,520 new cases, 157, 300 deaths in 2010
more deaths than breast, prostate, cervix and colon cancer
combined
In Israel – 1,897 new cases and 1,561 deaths in 2008

Lung cancer: Leading cause of death in the Western world
Overall survival: 13%
Virtually no improvement over the last 40 years
Stage I lung cancer: Cure rate of 70%

Overview
CXRs
and their role in lung cancer screening
Prospective RCTs
performed in the 1980’s
Principles of LDCT screening for lung cancer
Results of LDCT trials
I‐ELCAP
Hadassah
NLST
Cost‐effectiveness of LDCT screening for lung cancer
Future of LDCT screening for lung cancer
Research
Clinical

CXR
Inexpensive, readily available
In Hadassah: ≈
6500/month
Lesions =>1 cm are usually detected (smaller lesions if
calcified)
Improve diagnostic accuracy
PA + LAT films
Comparison with old films

1999

CAD: Experimental Results
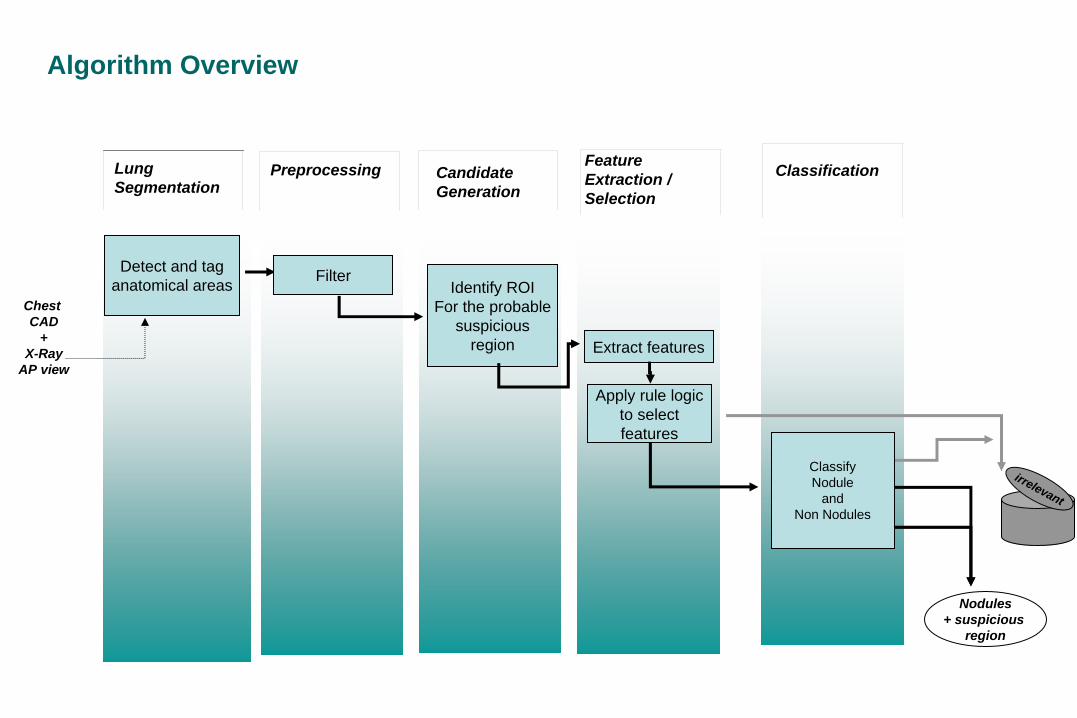
Chest CAD
+X-Ray
AP view
Identify ROIFor the probable
suspiciousregion Extract features
Nodules+ suspicious
region
Feature Extraction /Selection
Candidate Generation
Preprocessing
Algorithm Overview
Classification
Detect and tag anatomical areas
irrelevant
ClassifyNodule
andNon Nodules
Apply rule logic to select features
Lung Segmentation
Filter

53 year-old heavy smoker (37 pack years) with fever, productive cough, left chest pain. CXR 9/5/10: LLL consolidation , loculated left pleural effusion.


Spiculated RUL nodule, 12X9mm
Prospective RCTs on lung cancer screening
Used CXR and sputum cytology
Mayo lung project
Memorial Sloan Kettering Lung Project
Johns Hopkins Lung Project
Czechoslovakian study
Only the Mayo and Czech studies evaluated CXR
No statistically significant difference in mortality in a
population screened by CXR compared to control Fontana et al., Am Rev Respir Dis 1984Melamed et al., Chest 1984Tockman et al., Chest 1986Kubic et al., Cancer 1986

International Early Lung Cancer Action Program (I‐ELCAP)
Initially 2 institutions ; now >50 institutions world‐wide
Investigator team at each institution
Radiologists, pulmonologists, oncologists, thoracic surgeons,
pathologists, epidemiologists and a computer science team
Screening for lung cancer using the same protocol
Share knowledge about lung cancer screening with the
goal of early detection and reducing mortality worldwide

ELCAP:Baseline Findings (started: 1993)
1000 high risk participants underwent baseline LDCT and chest radiograph, and one
annual repeat LDCT.
Age: ≥60, smoking: ≥
10 pack‐years
27 lung cancers diagnosed at baseline
23 (83%) stage I
median diameter: 15 mm
Henschke et al, Lancet 1999; 354:99-105

ELCAP:Baseline Findings (started: 1993)
Of the 23 stage I lung cancers – 19 (83%) were
missed on chest radiographs.
23% had positive result of the initial LDCT
Only one patient who underwent recommended
biopsy had a benign lesion
Henschke et al, Lancet 1999; 354:99-105

ELCAP:Annual repeat findings
Smaller lung cancers
Median diameter: 8 mm
85.7% were stage I
< 3% with positive test result
Henschke
et al, Cancer 2001; 92:153‐159

CT Screening: Baseline & Annual Repeat
Baseline Year 1 Year 2 Year 3 ………..
Prevalence Annual incidence, usually pooled in screening
Screening for lung cancer: The I‐ELCAP approach
Study design
Baseline/ annual repeat screening
Regimen of screening
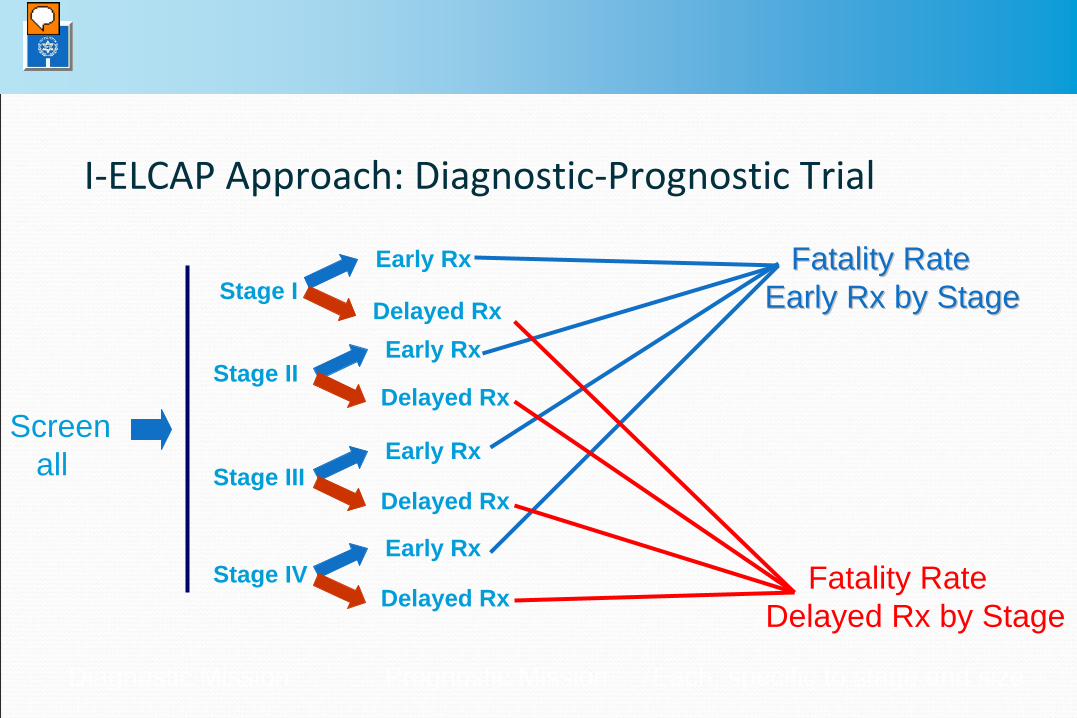
Diagnostic Mission Prognostic Mission Each, specific to stage and size
Stage IEarly Rx
Delayed Rx
Fatality RateFatality RateEarly Rx by StageEarly Rx by Stage
Stage IIEarly Rx
Delayed Rx
Fatality Rate Delayed Rx by Stage
Stage IIIEarly Rx
Delayed Rx
Stage IVEarly Rx
Delayed Rx
Screenall
I‐ELCAP Approach: Diagnostic‐Prognostic Trial

The regimen of screening
Population to be screened (age, smoking history)
Screening positives
Baseline
Annual repeat
Work‐up

Prevalence of malignancy
Dependent on risk profile of participants
Original ELCAP: 60 years of age and older with a smoking
history of 10 pack‐years or more
I‐ELCAP: 40 years of age and older with any smoking history
This needs to be considered when making
recommendations for biopsy

Prevalence of malignancy on baseline low‐dose CT in ELCAP (≥60 yo, ≥
10 pack‐years)
<5 5-9 10-14 15+ Total# people 99 46 9 5 159# malignant 1 11 3 4 19
%malignant 1 24 33 80 12
12% of all participants with nodules had a malignancy

Prevalence of malignancy on baseline low‐dose CT in I‐ELCAP
(≥40 yo, any smoking)
<5 5-9 10-14 15+ Total# people 5344 3221 576 445 9586# malignant 20 118 118 186 442
%malignant 0 4 20 42 5
5% of all participants with nodules had a malignancy

Prognostic significance of nodule type
SolidNonsolidPart‐solid
Prognostic significance of nodule type
Three‐fold malignancy rate in part‐solid nodules
compared to solid/nonsolid nodules
(Henschke et al, AJR Am J Roentgenol. 2002; 178: 1053‐7)

Positive result : Baseline screening
Any solid or part‐solid NCN >
5.0 mm in diameter or any
nonsolid nodule > 8 mm in diameter
Nodules <5 mm: highly unlikely to present with malignancy
during the first “cycle” of screening
(Henschke
et al, Radiology 2004; 231: 164‐8)
Between 12‐15% had a positive test result on baseline
screening at any given institution

Positive result: Annual Repeat
Newly detected or growing non‐calcified nodule
Based on comparison with previous CT
Approximately 6%

Diagnostic work‐up of screening positives
Repeat LDCT
Growth?
Antibiotics followed by CT at 1 month
PET scanning
Biopsy
I-ELCAP protocol available at http://ielcap.org



I‐ELCAP results (N Engl
J Med 2006;355:1763‐71)
31,567 asymptomatic persons at risk for lung cancer screened
using low‐dose CT (1993‐2005)
Stage I lung cancer diagnosed in 412/484 (85%)
10‐year survival in stage I lung cancer
Overall: 88%
Surgical resection in 1 month: 92%

HM‐ELCAP results (started 1998)
Total Enrollment as of Jan 31st, 2011: 1080
56% males, 44% females.
Mean age: 57±12
Mean pack‐years of smoking: 39±27.05
Smoking Hx
Current smokers: 71%
Former smokers: 26%
Never smokers: 3%
Positive studies
Baseline: 12.1%
Annual: 5.4%

HM‐ELCAP results: Detected cancersAnnualBaselineClinical stage
311I
00II
01III
11IV
413Total
Two additional patients discontinued screening and were diagnosed with advanced lung cancer elsewhere

National Lung Screening Trial (NLST) (Started in 2002)
Press release: Nov. 4, 2010
>53,000 current and former heavy smokers, ages 55 to 74
compared the effects of two screening procedures for lung
cancer –
low‐dose helical computed tomography (CT)
standard chest X‐ray
20% fewer lung cancer deaths among trial participants
screened with low‐dose helical CT
Lung cancer deaths in CT‐screened: 354, in CXR screened: 442
(p=0.0041)


Cost effectiveness of LDCT screening in Israel
Screening arm: 842 smokers and past smokers, ≥45 years
screened at Hadassah in 1998‐2004
Usual care arm
Stage distribution and stage‐specific life expectancy ‐
2,906
patients diagnosed in 1994‐2006 (NCI)
Lifetime stage‐specific costs ‐
medical records of 146 patients
diagnosed and treated at Hadassah in 2003‐2004
The analysis took into consideration possible screening
biases such as lead time, overdiagnosis, and self selection

Cost effectiveness of LDCT screening in Israel
The cost per LY or QALY gained by screening was about $20
The results of all the sensitivity checks confirmed the low
cost per LY or per QALY and, in some cases, the dominance of screening
LDCT screening for lung cancer in Israel provides a good
economic value under the common standards of health technology assessments.

Future ResearchImaging
Lowering radiation exposure
Software:
Detection and characterization of nodules
Volumetric measuring

Future Research
Blood/sputum biomarkers
Increased risk
Low OCG (DNA repair enzyme 8‐oxoguanine DNA N‐
glycosylase) activity is associated with increased risk of lung cancer (Paz‐Elizur
et al, J Natl
Cancer Inst 2003; 95:1263‐5)

Is LDCT screening ready for clinical use in Israel?
Effectiveness was confirmed: LDCT screening saves lives!
Cost‐effectiveness in Israel was confirmed
Well‐established protocol prevents unnecessary
interventional work‐up
Radiation exposure – in the same range as mammography

To be determined…
Who should be screened?
Who will pay?
Guidelines for performing and interpreting screening LDCTs
should be prepared and distributed


















