Minilecture. DOTS MANAGEMENT IN TUBERCULOSIS. Zul Dahlan Subdivision Pulmonology Dep artment of Internal Medicine Medical Faculty of Padjadjaran University Hasan Sadikin Hospital , BANDUNG. Female 40 yrs Cough for >3 months 3 x to GP, only presciption No sputum or CXR - PowerPoint PPT Presentation
DOTS MANAGEMENT IN DOTS MANAGEMENT IN TUBERCULOSIS TUBERCULOSIS Zul Dahlan Zul Dahlan Subdivision Pulmonology Subdivision Pulmonology Dep Dep artment of Internal Medicine artment of Internal Medicine Medical Faculty of Padjadjaran Medical Faculty of Padjadjaran University University Hasan Sadikin Hospital , BANDUNG Hasan Sadikin Hospital , BANDUNG Minilecture Minilecture
Transcript
DOTS MANAGEMENT DOTS MANAGEMENT IN TUBERCULOSISIN TUBERCULOSIS
Zul DahlanZul DahlanSubdivision PulmonologySubdivision PulmonologyDepDepartment of Internal Medicine artment of Internal Medicine Medical Faculty of Padjadjaran Medical Faculty of Padjadjaran University University Hasan Sadikin Hospital , BANDUNGHasan Sadikin Hospital , BANDUNG
MinilectureMinilecture
Female 40 yrsFemale 40 yrs Cough for >3 Cough for >3
monthsmonths 3 x to GP, only 3 x to GP, only
presciptionpresciption No sputum or No sputum or
CXRCXR She did CXR on She did CXR on
her initiativeher initiative Her sputum AFB Her sputum AFB
pospos
INTRODUCTIONINTRODUCTION Tuberculosis is an infectious disease that Tuberculosis is an infectious disease that
remain to be a major health problem in the remain to be a major health problem in the world including Indonesia. world including Indonesia.
Indonesia like other countries had adapted Indonesia like other countries had adapted WHO DOTS strategy for national TB control WHO DOTS strategy for national TB control and had succeed in variety of setting.and had succeed in variety of setting.
This presentation will disclose a few aspect This presentation will disclose a few aspect in the implementation of DOTS in the in the implementation of DOTS in the management tuberculosis, in pulmonary management tuberculosis, in pulmonary and extrapulmonary sites.and extrapulmonary sites.
- EASIER TRANSPORTATION BETWEEN COUNTRIES- EASIER TRANSPORTATION BETWEEN COUNTRIES
AFB/ PA/ DNA
EFFORT TO CONTAIN TUBERCULOSIS : - IDENTIFY MYCOBACTERIUM RESISTANCY - ADHERENCE TO TB THERAPY – DOTS METHOD
. Pleura . Pleura : 16,2 %: 16,2 %
. Meningeal . Meningeal : 9,9 %: 9,9 %
. Peritonitis . Peritonitis : 8,3% : 8,3%
. Spondylitis . Spondylitis : 4,0 %: 4,0 %
. Limphadenitis: 2,2 %. Limphadenitis: 2,2 %
. Pericarditis . Pericarditis : 1,0%: 1,0%
. . Coxitis Coxitis : 1.0 %: 1.0 %
. Supracondylus. Supracondylus : 0.7 %: 0.7 %
. Skin. Skin : 0,4 % : 0,4 %
. Sinovitis : 0,3 %
. Hepar : 0,1 %. Renal : 0,1 %
• PULMONARY TB 55 %
TB MANIFESTATION AT HASAN SADIKIN HOSPITAL
• EXTRAPULMONARY TB 45 %
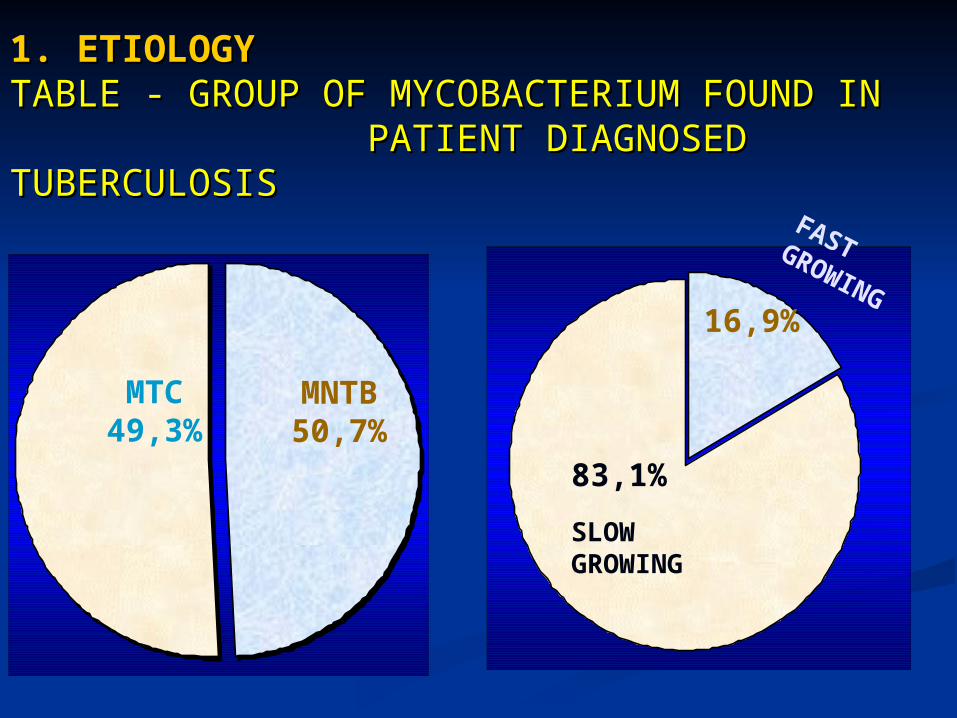
1. ETIOLOGY1. ETIOLOGYTABLE - GROUP OF MYCOBACTERIUM FOUND IN TABLE - GROUP OF MYCOBACTERIUM FOUND IN PATIENT DIAGNOSED TUBERPATIENT DIAGNOSED TUBERCCULOSISULOSIS
83,1%
16,9%
MTC49,3%
MNTB50,7%
SLOW GROWING
FAST GROWING
Table – Frequency Species of Mycobacterium Found in Various Organs
Organ
Lung Pleura Gland Peritoneum Total I.M. NonTuberculosis -MNTB 1. M. gordonae 2. M. alvei 3. M. ratisbonen 4. M. concordense 5. M.mucogenicum 6. M. avium 7. M. fortuitum 8. Uncultured Mycob. 9. M.peregrinum 10. M.septicum 11. M.paratuberculosis Total II. M. Tuberculosis Complex 1. M. africanum 2. M. tuberculosis 3. M. canetti Total
43121111000
14
640
10
31311010110
12
431
8
30000201001
7
1250
17
11001000000
3
000
0
115433322111
36 (50,7%)
22121
35 (49,3%)
Mycobact’rium Species
22. HOST FACTOR. HOST FACTOR
. . GENETIC SENSITIVITY TO TB :GENETIC SENSITIVITY TO TB : - FAMILIAL SYNDROMES : DISSEMINATION POST BCG - FAMILIAL SYNDROMES : DISSEMINATION POST BCG - MENDELIAN SENSITIVITY : IMPAIRMENT OF IFN- MENDELIAN SENSITIVITY : IMPAIRMENT OF IFN FUNCTION FUNCTION
.. INADEQUATE DRUGS DOSAGEINADEQUATE DRUGS DOSAGE
.. COMPLIANCECOMPLIANCE
EFFORT TO CONTAIN TUBERCULOSIS : - IDENTIFY MYCOBACTERIUM RESISTANCY - ADHERENCE TO TB THERAPY –> DOTS METHOD
COMPLIANCECOMPLIANCE
TB Patient frequently did not have their medicine TB Patient frequently did not have their medicine regularly and continuously because of :regularly and continuously because of :
Limited effort because of false understanding : Limited effort because of false understanding :
. Stopping medicine halfway because they are. Stopping medicine halfway because they are
feeling better feeling better TB relapse again TB relapse again
. “Taking the medicine too long “. “Taking the medicine too long “
. “Medicine too much”. “Medicine too much” High cost of therapy High cost of therapy Drug side effect/ untoward effect Drug side effect/ untoward effect
WITH TUBERCULOSIS :WITH TUBERCULOSIS :
- - Treatment is more than treatmentTreatment is more than treatment
- Treatment is prevention of :- Treatment is prevention of :
. further spreading of . further spreading of
infectioninfection
. further process of . further process of
diseasedisease
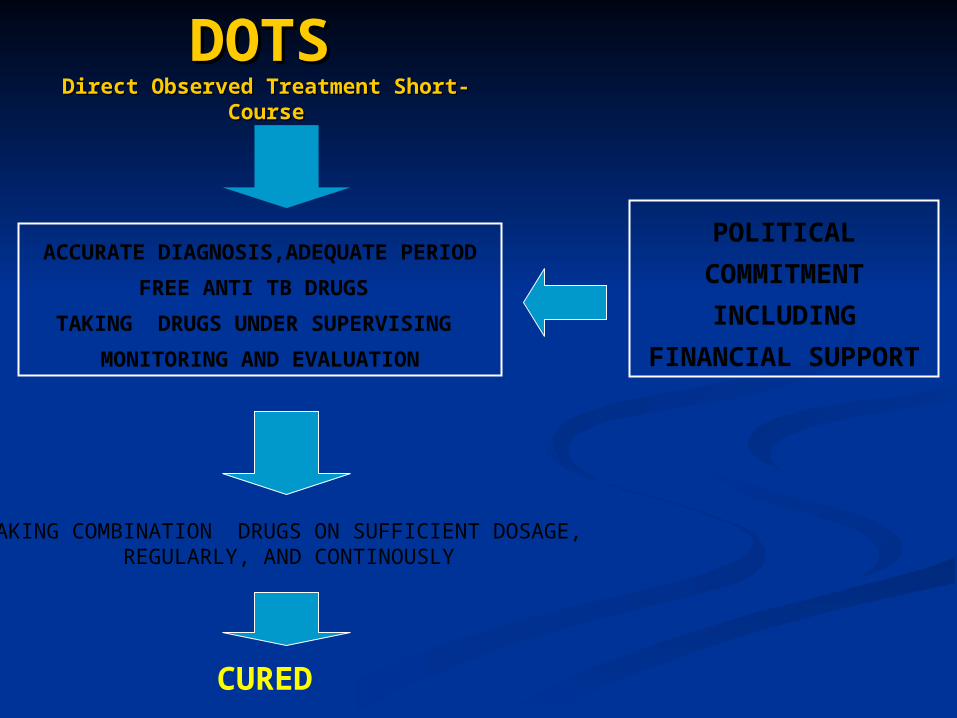
DOTSDOTS
Direct Observed Treatment Short-Direct Observed Treatment Short-CourseCourse
ACCURATE DIAGNOSIS,ADEQUATE PERIOD
FREE ANTI TB DRUGS
TAKING DRUGS UNDER SUPERVISING
MONITORING AND EVALUATION
POLITICAL
COMMITMENT
INCLUDING
FINANCIAL SUPPORT
TAKING COMBINATION DRUGS ON SUFFICIENT DOSAGE, REGULARLY, AND CONTINOUSLY
CURED
BASIC PRINCIPLES OF ANTI BASIC PRINCIPLES OF ANTI TUBERCULOSIS DRUGSTUBERCULOSIS DRUGS
Drug is effective during active multiplication phase Drug is effective during active multiplication phase
of mycobacterium, not in dormant phaseof mycobacterium, not in dormant phase
Use combination of 4 – 5 drugs, for 6 mo. or more Use combination of 4 – 5 drugs, for 6 mo. or more
Use of still effective drug for etiologic Use of still effective drug for etiologic
mycobacteriummycobacterium
Patient has to take the medicine regularly, Patient has to take the medicine regularly,
continuously in adequate dosage and periodcontinuously in adequate dosage and period
CLASSIFICATION TB :CLASSIFICATION TB :
Related to 4 aspects :Related to 4 aspects :
- Organ involved in TB process : lung/ extra-lung - Organ involved in TB process : lung/ extra-lung
- result of sputum examination : AFB (+)/ AFB (-)- result of sputum examination : AFB (+)/ AFB (-)
- Previous history of TB therapy :- Previous history of TB therapy :
. New/ exacerbation, relapse, migration/ drop out, . New/ exacerbation, relapse, migration/ drop out,
failurefailure
- Degree of severity of disease: mild or severe - Degree of severity of disease: mild or severe
DECISION ON CATEGORY OF THERAPY
IMPLEMENTATION OF TB THERAPYIMPLEMENTATION OF TB THERAPY
Aspect–aspect :
Decision on the category of TB therapy
Therapy supervising :
. Healthcare officer, family, friend, etc
Monitoring of sputum ACB, during :
- intensive period
- the end of therapy/ 1 month before the
- follow up of sputum conversion
Monitoring of therapy :
- cured, drop out, not cure
THE CHOICE OF ANTITUBERCULOSIS DRUG THE CHOICE OF ANTITUBERCULOSIS DRUG BASED ON CATEGORIESBASED ON CATEGORIES
Alternative of Combined Drug
CategoryOf therapy
Classification and Type of TB Patient TB
Intensive phase (daily or 3x /
week)
Late Phase
I New case AFB (+)New case AFB (-)Chest x-ray (+) with advanced lung
damage/ severe disease New case of TB Severe extra pulmonary TB case
2 HRZE*2 HRZE
2 HRZE
4 HRZE*4 HR
6 HE
II Patients : relapse failure drop out (after default)
2 HRZES / 1 HRZE*2 HRZES / 1 HRZE
5 H3R3E3*5 HRE
New case TB AFB (-) , Chest x-ray (+), mild disease
2 HRZ*2 HRZ
4 H3R3*6 HE
III Mild new ekstrapulmonary case 2 HRZ 4 HR
IV Chronic case Consultation to specialist for secondary medicine
MULTI DRUG RESISTANCE MULTI DRUG RESISTANCE TBTB
(MDR TB)(MDR TB)
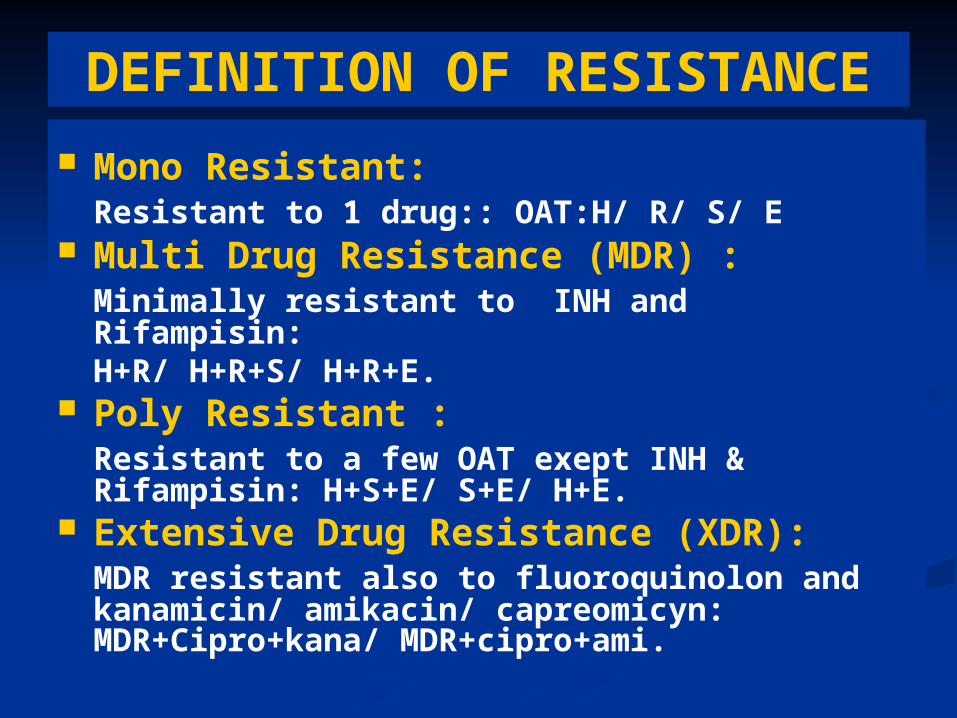
DEFINITION OF RESISTANCE
Mono Resistant:Resistant to 1 drug:: OAT:H/ R/ S/ E
Multi Drug Resistance (MDR) :Minimally resistant to INH and Rifampisin: H+R/ H+R+S/ H+R+E.
Poly Resistant :Resistant to a few OAT exept INH & Rifampisin: H+S+E/ S+E/ H+E.
Extensive Drug Resistance (XDR):MDR resistant also to fluoroquinolon and kanamicin/ amikacin/ capreomicyn:MDR+Cipro+kana/ MDR+cipro+ami.
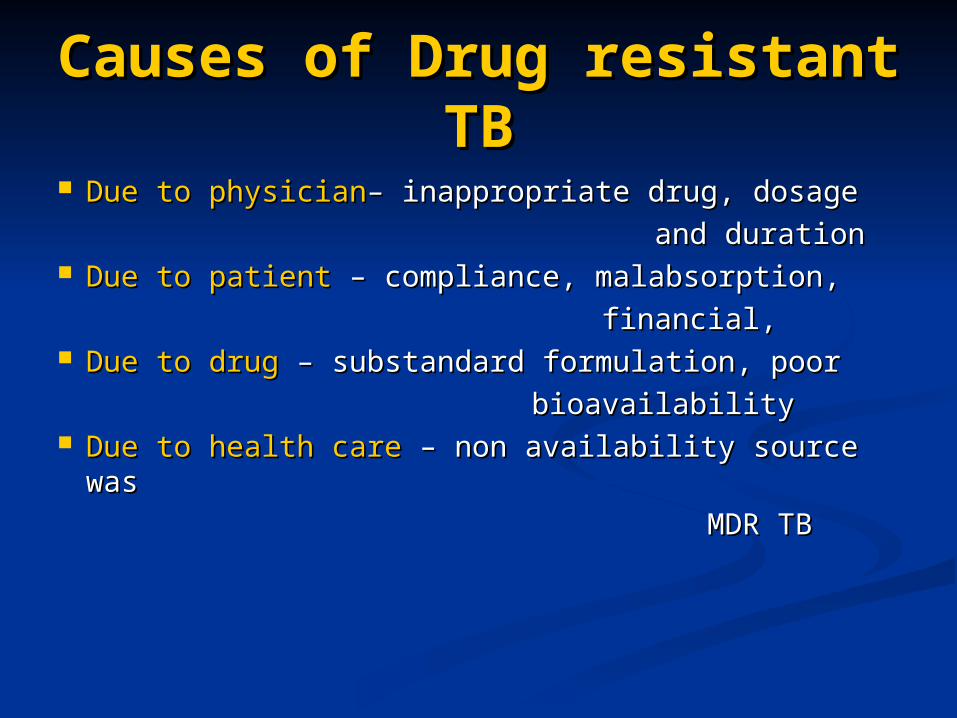
Causes of Drug resistant TBCauses of Drug resistant TB
Due to physicianDue to physician– inappropriate drug, dosage – inappropriate drug, dosage
and durationand duration Due to patientDue to patient – compliance, malabsorption, – compliance, malabsorption,
financial, financial, Due to drugDue to drug – substandard formulation, poor – substandard formulation, poor
bioavailabilitybioavailability Due to health careDue to health care – non availability source was – non availability source was
MDR TB MDR TB
Treatment of Poli/ MDR : More difficult, costly, and more
side effect Individualized :
- “tailor made” - Package
MANAGEMENT OF MDRMANAGEMENT OF MDR
DOTS Plus Strategy Base on :DOTS Plus Strategy Base on : Anamnesis.Anamnesis. Diagnosis berdasarkan Diagnosis berdasarkan laboratorium.laboratorium. Pengobatan berdasarkan Pengobatan berdasarkan laboratorium.laboratorium. Evaluasi pengobatan berdasarkan Evaluasi pengobatan berdasarkan
laboratorium.laboratorium. Evaluasi efek samping, faal hati, faal ginjal, Evaluasi efek samping, faal hati, faal ginjal,
dll berdasarkan dll berdasarkan laboratorium.laboratorium. Lama pengobatan min. 18 bln, dg tahap Lama pengobatan min. 18 bln, dg tahap
intensif 6 bln paduan mengandung OAT intensif 6 bln paduan mengandung OAT suntik.suntik.
Indonesia : Indonesia : 22 High Burden Countries22 High Burden Countries
Indonesia : Indonesia : 22 High Burden Countries22 High Burden Countries1. India
2. China
3. Indonesia4. Bangladesh5. Nigeria6. Pakistan7. South Africa8. Philippines9. Russia10. Ethiopia11. Kenya12. DR Congo13. Viet Nam14. UR Tanzania15. Brazil16. Thailand17. Zimbabwe18. Cambodia19. Myanmar20. Uganda21. Afghanistan22. Mozambique
Indonesia 10%Indonesia 10%Indonesia 10%Indonesia 10%
Bangladesh 4%
China15%
China15%
India30%India30%
Other28%
Philippines 3%
Pakistan 4%
Nigeria 3%
South Africa 2%
Russia 1%
Penyebab kematian terbanyak penyakit infeksi (SKRT 1995)
583.000 kasus baru/tahun, 140.000 kematian /tahun (WHO)
BACKGROUND OF TB PROBLEM IN BACKGROUND OF TB PROBLEM IN DEVELOPING COUNTRIESDEVELOPING COUNTRIES
-Annually there are 1 millions new TB patients
- And TB is responsible for an annual 3 millions death
- 97 % patients located in developing c’ tries 25% can be
avoided
- In Indonesia : TB is third major cause of mortality ( SKRT ‘95)
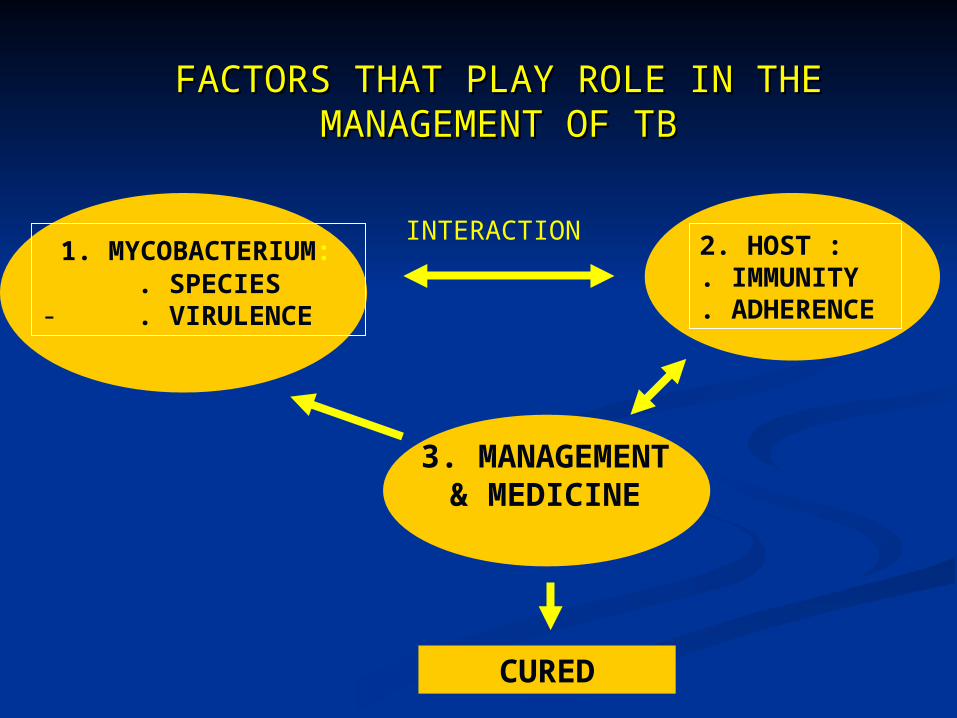
MANAGEMENT OF TB IS BASED ON :-Species of causal mycobacterium - Infected organs- Advanced and progression of diseases
THE STRATEGY IS TO MORBIDITY & MORTALITY
* HIGH MORBIDITY AND MORTALITY RATE
World Health Organization
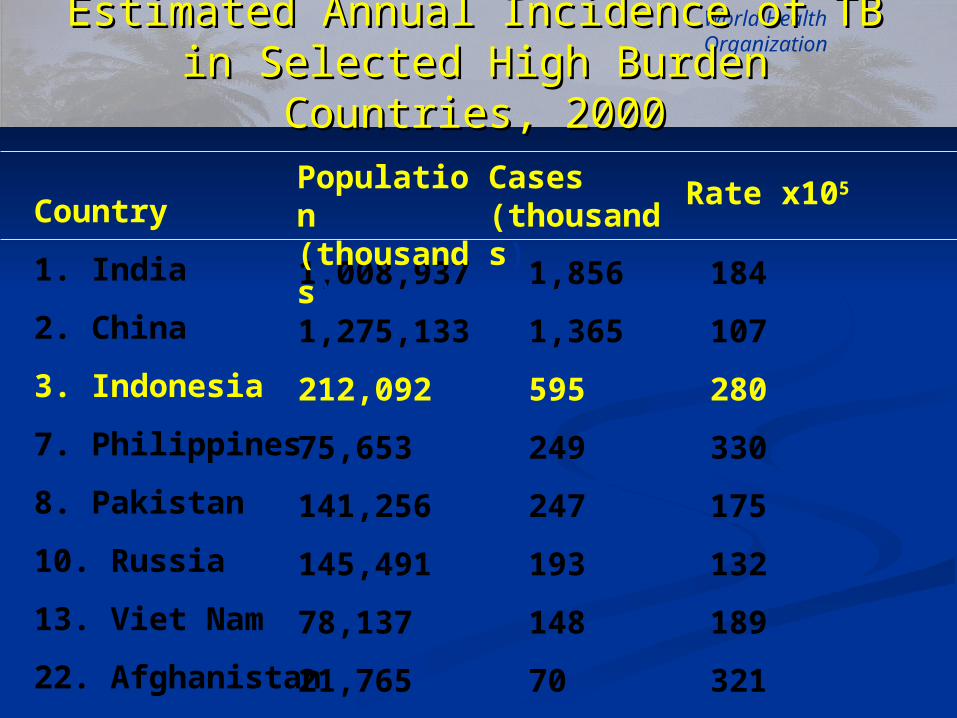
Country
1. India
2. China
3. Indonesia
7. Philippines
8. Pakistan
10. Russia
13. Viet Nam
22. Afghanistan
1,008,937
1,275,133
212,092
75,653
141,256
145,491
78,137
21,765
184
107
280
330
175
132
189
321
1,856
1,365
595
249
247
193
148
70
Population (thousands)
Cases (thousands)
Rate x105
Estimated Annual Incidence of TB in Estimated Annual Incidence of TB in Selected High Burden Countries, 2000Selected High Burden Countries, 2000
BackgroundBackground Indonesian situation :Indonesian situation :
- population : 222,781,000- population : 222,781,000- global rank : 3- global rank : 3- incidence : 239 (239/100,000/year)- incidence : 239 (239/100,000/year)- incidence of new cases : 108 - incidence of new cases : 108
A pessimist sees the difficulty in every opportunity:
an optimist sees the opportunity in every difficulty.
Sir Winston Churchill
Global Strategy to Stop TB 2006-Global Strategy to Stop TB 2006-20152015
1. Pursuing quality DOTS expansion and enhancement1. Pursuing quality DOTS expansion and enhancement• Government commitment with long-term planning and adequate resources Government commitment with long-term planning and adequate resources
to reach targetsto reach targets• Case detection : bacteriology and strengthening of laboratory networkCase detection : bacteriology and strengthening of laboratory network• Standardised treatment, under proper case management conditions Standardised treatment, under proper case management conditions
including DOT and patient supportincluding DOT and patient support• Effective and regular drug supply systemEffective and regular drug supply system• Monitoring system for supervision and evaluation, including impact Monitoring system for supervision and evaluation, including impact
11 Addressing TB/HIV and MDR-TBAddressing TB/HIV and MDR-TB2. 2. Contributing to health system strengtheningContributing to health system strengthening3. 3. Engaging all care providersEngaging all care providers
4. 4. Empowering patients and communitiesEmpowering patients and communities 5. 5. Enabling and promoting researchEnabling and promoting research
Stop TB DepartmentStop TB Department
The new Stop TB Strategy and the The new Stop TB Strategy and the Regional Strategic Plan, 2006-Regional Strategic Plan, 2006-
20152015 Sustaining and enhancing Sustaining and enhancing
DOTS to reach all TB DOTS to reach all TB patients, improve case patients, improve case detection and treatment detection and treatment successsuccess
Establishing interventions Establishing interventions to address TB/HIV and to address TB/HIV and MDR-TBMDR-TB
Forging partnerships, Forging partnerships, including with communities, including with communities, to ensure equitable access to ensure equitable access to international standards of to international standards of TB care for all TB care for all
Contributing to Contributing to strengthening health strengthening health systemssystems
DOTS Success StoryDOTS Success Story DOTS the internationally recommended control DOTS the internationally recommended control
strategy was launched in 1994 strategy was launched in 1994 The DOTS framework has subsequently been The DOTS framework has subsequently been
expanded and implemented in 182 countries. expanded and implemented in 182 countries. DOTS implementation has helped countries to DOTS implementation has helped countries to
improve national TB control programmes (NTPs) improve national TB control programmes (NTPs) and make major progress in TB controland make major progress in TB control
By 2004, more than 20 million patientsBy 2004, more than 20 million patientshad been treated in DOTS programmeshad been treated in DOTS programmesworldwide and more than 16 million of themworldwide and more than 16 million of themhad been cured.had been cured.
HEALTH CENTER INVOLVED IN DOTS< 60 %60 - 80 %81 - 100 %
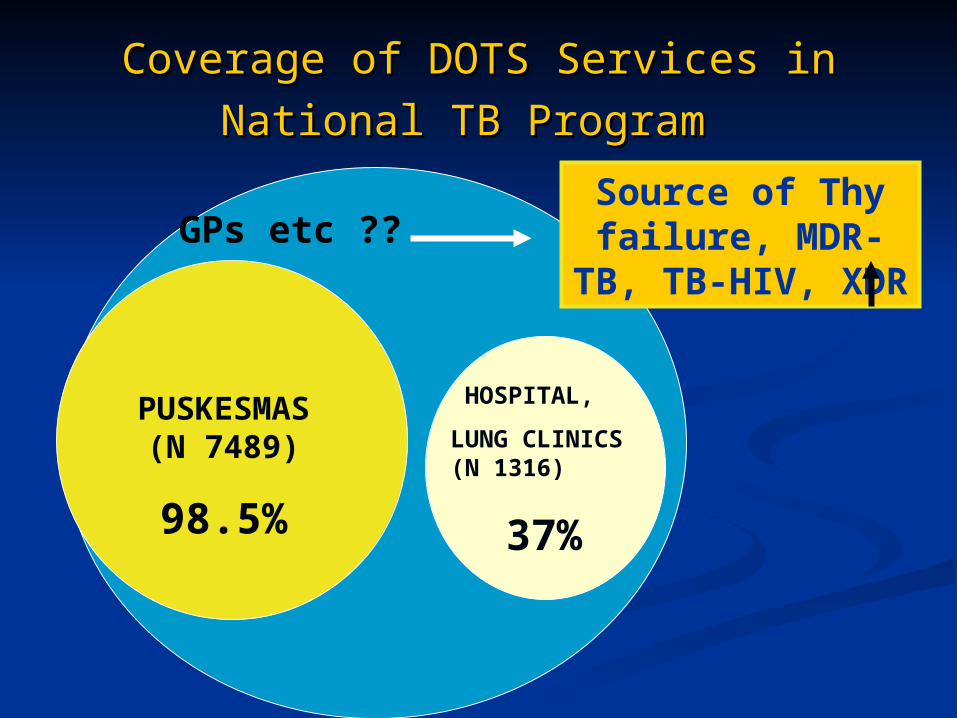
Coverage of DOTS Services in Coverage of DOTS Services in
National TB ProgramNational TB Program
PUSKESMAS (N 7489)
98.5%
HOSPITAL,
LUNG CLINICS (N 1316)
37%
GPs etc ??Source of Thy
failure, MDR-TB, TB-HIV, XDR
The practices of TB care among The practices of TB care among doctors in private sectordoctors in private sector
Over diagnosis and under diagnosisOver diagnosis and under diagnosis Over treatment and under treatmentOver treatment and under treatment Chest X-ray regarded as the most important Chest X-ray regarded as the most important
diagnostic tool diagnostic tool Sputum smear is mostly neglected Sputum smear is mostly neglected Non standard tests gaining popularity (serology, Non standard tests gaining popularity (serology,
PCR etc) PCR etc) Incorrect use of anti TB drugs (regimen, doses, Incorrect use of anti TB drugs (regimen, doses,
duration, compliance)duration, compliance)
Eur Respir J 2006; 28: 687–690
Lead to substandard Lead to substandard care and failurecare and failure
Extension of DOTS Service in Hospital through Hospital DOTS
Extended of working cooperation with LSM with Health Service
DOTS in Work Place Extension of working
cooperation with Medical Proffesion to facilitate DOTS
ISTC & PCTC (Patients’ charter for TB Care)
Involvement of All Health Personnel & health centers
ISTC TB Training Modules 2009
Audience:Audience: all health care practitioners, all health care practitioners, public and privatepublic and private
Scope:Scope: diagnosis, treatment, and public diagnosis, treatment, and public health responsibilities; intended to health responsibilities; intended to complement local and national guidelinescomplement local and national guidelines
Rationale:Rationale: sound sound tuberculosis control requires the effective engagement of all requires the effective engagement of all providers in providing providers in providing high quality care and in and in collaborating with TB control programscollaborating with TB control programs
ISTC: Key PointsISTC: Key Points
ISTC ObjectivesISTC Objectives
The The Standards Standards are intended that all care are intended that all care provider delivered high quality care: provider delivered high quality care:
for patients of all ages, those with sputum for patients of all ages, those with sputum smear (+), sputum smear (-), and extra smear (+), sputum smear (-), and extra pulmonary TBpulmonary TB
TB caused by drug-resistant TB caused by drug-resistant M M tuberculosis tuberculosis complexcomplex
present what should be donepresent what should be done, whereas, , whereas, guidelines describe how the action is to be guidelines describe how the action is to be accomplishedaccomplished
Evidence-based, living documentEvidence-based, living document Developed in tandem withDeveloped in tandem with Patients’ Charter Patients’ Charter
for Tuberculosis Carefor Tuberculosis Care Handbook for Using the International Handbook for Using the International
Standards for Tuberculosis CareStandards for Tuberculosis Care
21 Standards Original Standards were renumbered and
new Standards were written Evidence-based, living document, will require
future revisions as well ISTC Tuberculosis Training Modules and
Facilitator’s Guide were updated and developed to be in agreement with Edition 2 of the ISTC
ISTC TB Training Modules 2009
ISTC Standard 1
All persons with All persons with otherwise otherwise unexplained unexplained productive productive cough lasting two-three weeks or more should should be evaluated for be evaluated for tuberculosistuberculosis
The Indonesian Version of The Indonesian Version of ISTCISTC
ISTC in IndonesiaISTC in IndonesiaIndonesian Standard for Tuberculosis Indonesian Standard for Tuberculosis
ControlControl
Is accepted and being endorsed by Is accepted and being endorsed by several profession organizationseveral profession organization
In socialization phaseIn socialization phase Has been disseminated and implemented Has been disseminated and implemented
in Jakarta, West Java, East Java, and in Jakarta, West Java, East Java, and Central Java as pilot projectCentral Java as pilot project
GoalsGoals
Equitable quality DOTS for all- To standardize the care of TB patients in
variety of different providers - To provide high quality of care- Improve CDR, cure rate- Prevention of MDR- Reduce mortality- Cover co-infection TB/HIV
The first priority is to endorse and implement ISTC among private physicians and hospitals
WORKING TEAM ON PULMONARY & EXTRAPULMONARY TB ERADICATION
PROGRAM
TRAINING DOKTER/PERAWAT/
PARAMEDIS
PULMONARY & EXTRAPULMONARY
TUBERCULOSIS CENTRAL CLINIC
RESPIROLOGY TEAM
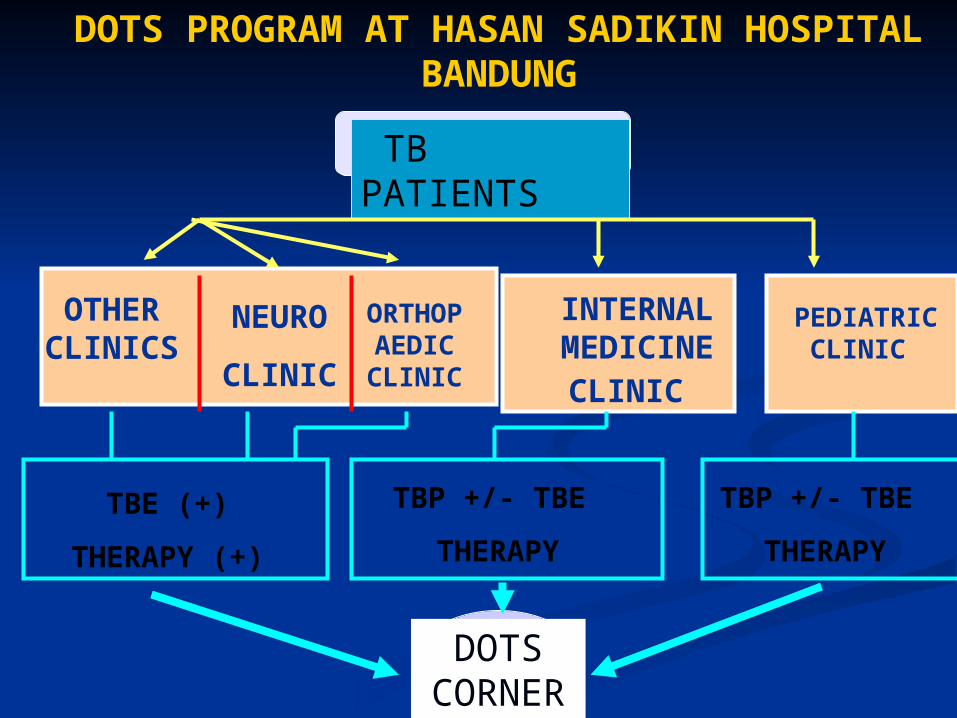
DOTS PROGRAM AT HASAN SADIKIN HOSPITAL BANDUNG
TB PATIENTS
OTHER CLINICS
NEURO
CLINIC
ORTHOPAEDI
C CLINIC
INTERNAL
MEDICINE CLINIC
PEDIATRIC CLINIC
TBE (+)
THERAPY (+)
TBP +/- TBE
THERAPY
TBP +/- TBE
THERAPY
DOTS CORNE
R
SOCIAL WORKER
LABORATORYOFFICER
MEDICALPRACTITIONER
DATA COLLECTINGREPORTING
OFFICER
FARMACY-OFFICER
Conclusion 1Conclusion 11.1. TUBERCULOSIS REMAINS TO BE A MAJOR HEALTH PROBLEM IN TUBERCULOSIS REMAINS TO BE A MAJOR HEALTH PROBLEM IN
INDONESIA WITH A HIGH MORBIDITY AND MORTALITY RATE .INDONESIA WITH A HIGH MORBIDITY AND MORTALITY RATE .
2.2. STRATEGY OF DOTS HAS BEEN PROVEN TO BE AN EFFECTIVE STRATEGY OF DOTS HAS BEEN PROVEN TO BE AN EFFECTIVE METHOD TO ERADICATE UBERCULOSIS. IT MUST BE DONE METHOD TO ERADICATE UBERCULOSIS. IT MUST BE DONE NATIONALLY AND SUPPORTED BY WHOLE COMMUNITY WITH NATIONALLY AND SUPPORTED BY WHOLE COMMUNITY WITH ADEQUATE PERSONNEL, MEDICINE, AND FINANCIAL.ADEQUATE PERSONNEL, MEDICINE, AND FINANCIAL.
3.3. RESISTANT MYCOBACTERIUM TUBERCULOSIS AND OTHER RESISTANT MYCOBACTERIUM TUBERCULOSIS AND OTHER SPECIES MAY HAMPER THE ERADICATION OF TUBERCULOSIS SPECIES MAY HAMPER THE ERADICATION OF TUBERCULOSIS AND MYCOBACTERIOSIS. AND MYCOBACTERIOSIS.
ON THIS CIRCUMSTANCES CONFIRMATION OF ETIOLOGIC AGENT MUST ON THIS CIRCUMSTANCES CONFIRMATION OF ETIOLOGIC AGENT MUST BE DONE WHICH WILL BE HELPFUL IN TREATING THE RESISTANT BE DONE WHICH WILL BE HELPFUL IN TREATING THE RESISTANT SPECIES.SPECIES.
Conclusion 2Conclusion 2 The result of Indonesian National TB The result of Indonesian National TB
Program was encouragingProgram was encouraging However, Puskesmas gave the biggest However, Puskesmas gave the biggest
contribution to successful outcomecontribution to successful outcome The problems lie on Hospitals and Private The problems lie on Hospitals and Private
providersproviders The Implementation of ISTC expected to The Implementation of ISTC expected to
be complimentary to existing DOTS be complimentary to existing DOTS program program
TB EpidemicTB Epidemic
DOTSDOTS
HIV EpidemicHIV Epidemic
Working groups of the Working groups of the Stop TB PartnershipStop TB Partnership












































![Tuberculosis: Laboratory Diagnosis and Dots Strategy ...file.scirp.org/pdf/JTR_2014090311335433.pdf · signs and symptoms of TB are not specific, ... [14]. Therefore, DOTS regimen](https://static.documents.pub/doc/80x56/5a84860c7f8b9a14748b6dcb/tuberculosis-laboratory-diagnosis-and-dots-strategy-filescirporgpdfjtr.jpg)









