83
TRATAMIENTO ACTUAL DE LA ESTENOSIS CAROTIDEA Dr. Claudio Cigalini Hospital Privado de Rosario [email protected]

TRATAMIENTO ACTUAL DE LA ESTENOSIS CAROTIDEA
Dr. Claudio Cigalini Hospital Privado de Rosario

• A quién y cuando intervenir?

PACIENTE SINTOMATICO (SINTOMAS HEMISFERICOS U OCULARES)

Riesgo de Stroke luego de un AIT (Pacientes Sintomáticos)
El riesgo de eventos recurrentes es del 10-30% a 30 días

• When revascularization is indicated for patients with TIA or minor, nondisabling stroke, it is reasonable to perform the procedure within 2 weeks of the index event rather than delay surgery if there are no contraindications to early revascularization (Class IIa; Level of Evidence B)

El tratamiento médico no es suficiente, la intervención elegida deberá realizarse rápido, no más alla de las dos semanas

ESTENOSIS CAROTIDEA SINTOMATICA
Ashley M. Wabnitz ET AL. Curr Treat Options Cardio Med (2017) 19: 62

Razonable entre 2 a 7 días!!!

PACIENTE ASINTOMATICO

En todas las directrices actuales las indicaciones de CEA y CAS todavía se basan sólo en los ensayos de CEA versus tratamiento médico en los que los pacientes fueron asignados al azar 12 a 34 años atrás.

Fig. 1. Decreasing trends in the risk of ipsilateral stroke seen in patients
with asymptomatic carotid artery stenosis randomized to medical
therapy in ACAS and ACST. Data obtained from Naylor.30
EL TRATAMIENTO MEDICO CAMBIÓ EL ESCENARIO

RIESGO DE STROKE EN ENFERMEDAD CAROTIDEA ASINTOMATICA


CEA is reasonable “in asymptomatic patients who have more than 70% stenosis of the internal carotid artery if the risk of perioperative stroke, MI [myocardial infarction], and death is low.”(< 3%) IIa, level of evidence B.


(Nicolaides AN y col., Eur J Vasc Surg 2005;30:275-84)
Incidencia de Eventos Hemisféricos Ipsilaterales en pacientes Asintomáticos según la severidad de la estenosis
SEVERIDAD DE LA ESTENOSIS

PROGRESION DE LA ESTENOSIS
Predictors and clinical significance of progression or regression of asymptomatic carotid stenosis
Stavros K. Kakkos, MD, PhD, RVT, Andrew N. Nicolaides, MS, PhD, FRCS, Ioanna Charalambous, Dafydd Thomas, MD, FRCP, Argyrios Giannopoulos, MD, A. Ross Naylor, MD, FRCS, George Geroulakos, MD,
PhD, Anne L. Abbott, MBBS, FRACP, PhD
Ipsilateral cerebrovascular or retinal ischemic (CORI) events P < .001
Ipsilateral hemispheric stroke (P = .050)
ACV ipsilateral a los 8 años fue cero en los pacientes con regresión, el 9% si la estenosis no se modificó y del 16% si hubo progresión (ACV anual promedio del 0%, 1,1% y 2,0%, respectivamente
Journal of Vascular Surgery 2014 59, 956-967

CARACTERISTICAS DE LA PLACA
Stroke. 2015;46:91-97.
Placa ecolúcidas & exceso de riesgo de ACV ipsilateral 2,61 ( 1,47-4,63; P = 0,001)
Pacientes con placas ecolúcidas (Negras) tuvieron un riesgo de ACV a 30 meses de 10% Vs 4,1% (1.6%pa) con placas ecogénicas (blancas)

VOLUMEN DE LA PLACA
J Vasc Surg 2010;52:1486-96
Riesgo de ACV anual 1.0% Riesgo de ACV anual 1.4%
Riesgo de ACV anual 4.6%

ULCERACION DE LA PLACA
• Presencia de placas ulceradas(>3) el riesgo de ACV/Muerte a 3 años (18% Vs 2%)
• Con Microembolia el riesgo de ACV o muerte a 3 años fue 20% vs 2% sin Me

HEMORRAGIA INTRAPLACA
Stroke. 2013;44:3071-3077

Embolización en Doppler TC
Lancet Neurol 2010; 9: 663–71
• Meta análisis • 1144 pactes
• EAC carotidea 70-99% asintomática
• Micro embolia detectada por doppler
Transcraneal
OR 6.34 (2.85 -15.44)

Pacientes con ECA >60% la presencia de IC Silente ipsilateral en TC tienen un RIESGO ANUAL de ACV significativamente aumentado (3.6%pa) que aquellos que no lo tienen (1.0%pa)
Infarto Silente
J Vasc Surg 2009;49:902-9

Reserva Vascular Cerebral
Ante una obstrucción de una carótida interna existe una vasodilatación compensatoria de las arteriolas cerebrales para mantener el flujo sanguíneo, el cual tiene un punto de quiebre, generando una RESERVA VASCULAR CEREBRAL deteriorada o exhausta.
Stroke. 2012;43:2884-2891
OR 4.7
Asintomáticos

Cómo cambia el tratamiento médico la historia natural de la estenosis carotidea?
• Control de la hipertensión
– Cada 10mmHg de caída en la TA disminuye el riesgo de ACV en 33%
• Cesación tabáquica
– Fumadores activos RR 4
– Ex fumadores RR 1.7
*Lawes CM, Bennett DA, Feigin VL, Rodgers A. Blood pressure and stroke: an overview of published reviews. Stroke. 2004;35:776-785. *Wannamethee SG, Shaper AG, Whincup PH, Walker M. Smoking cessation and the risk of stroke in middle-aged men. JAMA. 1995;274:155-160.

Lípidos
• LDL
– El riesgo de stroke disminuye >15% por cada10% de caida en el valor de LDL
• Estatinas
– Disminuyen el riesgo 15-30%
*Bhatt DL, Fox KA, Hacke W, Berger PB, Black HR, Boden WE,et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006;354:1706-1717. *Collaborative overview of randomised trials of antiplatelet therapy--I: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. Antiplatelet Trialists' Collaboration. BMJ. 1994;308:81-106. *Diener HC, Bogousslavsky J, Brass LM, Cimminiello C, Csiba L, Kaste M,et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364:331-337. *Wolff T, Miller T, Ko S. Aspirin for the primary prevention of cardiovascular events: an update of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2009;150:405-410.

• Sin estudios en asintomaticos
• Múltiples estudios del beneficio con DAPT en sintomaticos
• AHA/ASA/USPSTF recomiendan AAS para hombres > 45, mujeres > 55 con >3%
Antiplaquetarios
*Bhatt DL, Fox KA, Hacke W, Berger PB, Black HR, Boden WE,et al. Clopidogrel and aspirin versus aspirin alone for the prevention of atherothrombotic events. N Engl J Med. 2006;354:1706-1717. *Collaborative overview of randomised trials of antiplatelet therapy--I: Prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. Antiplatelet Trialists' Collaboration. BMJ. 1994;308:81-106. *Diener HC, Bogousslavsky J, Brass LM, Cimminiello C, Csiba L, Kaste M,et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364:331-337. *Wolff T, Miller T, Ko S. Aspirin for the primary prevention of cardiovascular events: an update of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2009;150:405-410.

Objetivo: Prevención del ACV
SINTOMATICOS
ASINTOMATICOS
< 6%
< 3%
*Ad Hoc Committee, AHA
Muerte/ACV periprocedimiento*:

• RECOMENDACIONES

SINTOMATICO, 70-99%: EAC IA
SINTOMATICO, 50-69%: EAC IIa
SINTOMATICO, 50-99%, ALTO RIEGO CLINICO O ANATOMICO PARA EAC: AC IIa

SINTOMATICO, RIESGO QUIRURGICO NORMAL: AC ES UNA ALTERNATICA IIb
NO SE RECOMIENDA INTERVENCION EN LESIONES <50% CLASE III NIVEL A

ENDARTERECTOMIA: LESIONES 69-99% CONDICIONES QUE AUMENTEN EL RIESGO DE STROKE LONGEVIDAD > 5 AÑOS RIESGO PERIOPERATORIO < 3%
ANGIOPLASTIA CAROTIDEA: LO MISMO + ALTO RIESGO PARA ENDARTERECTOMIA

ANGIOPLASTIA CAROTIDEA: LESIONES 69-99% CONDICIONES QUE AUMENTEN EN RIESGO DE STROKE LONGEVIDAD > 5 AÑOS RIESGO PERIOPERATORIO < 3% + RIESGO QUIRURGICO NORMAL

• EVIDENCIA

Fig 2. The cumulative incidence of stroke.
Li Y, Yang JJ, Zhu SH, Xu B, Wang L (2017) Long-term efficacy and safety of carotid artery stenting versus endarterectomy: A meta-analysis of randomized controlled trials. PLOS ONE 12(7): e0180804. https://doi.org/10.1371/journal.pone.0180804 http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0180804
Fig 1. The cumulative incidence of the composite outcome of death or stroke.

Sardar, P et al JACC 2017; 69 (18): 2266-75
Death, stroke, MI, or cranial nerve palsy
Stroke
Myocardial Intarction
Eventos periprocedimiento

EVA-3s Trial Endarterectomy versus Stenting in Patients with Symptomatic Severe Carotid Stenosis
(NEJM 2006)
• 20 Hospitales Académicos y 10 no-Académicos de Francia
• La diferencia en complicaciones a 30 días del 2%
• Planeado para randomizar 872 pacientes
• Punto Final Primario: Cualquier muerte o stroke a 30 días
Estudio Randomizado, multicéntrico, de No Inferioridad:
CAS con protección vs. CEA
Pacientes recientemente sintomáticos (120 días)
con estenosis carotídea ≥ 60%.

Eva-3s Trial: Endarterectomy versus Stenting in Patients with Symptomatic Severe Carotid Stenosis (NEJM 2006)
A los Cirujanos se les requería haber realizado 25 CEA en el último año
A los Intervencionistas se les requería una experiencia pequeña: 12 (total)
• 39% de operadores en trainning
• 45% de lo operadores con < 50 Intervenciones
• 16% con más de 50 intervenciones

Eva-3s Trial: Endarterectomy versus Stenting in Patients with Symptomatic Severe Carotid Stenosis (NEJM 2006)
Múltiples dispositivos diferentes utilizados para CAS (5 stents diferentes y 7 sistemas diferentes de protección distal), sin el entrenamiento adecuado (2 casos)
Baja inclusión de pacientes (promedio de pacientes incluídos por centro =1,7 por año)
Solamente el 38% de los pacientes tomaba algún tipo de antiagregante plaquetario después del procedimiento
La utilización de un sistema de protección distal no era obligatoria al comienzo del estudio

Eva-3s Trial: Endarterectomy versus Stenting in Patients with Symptomatic Severe Carotid Stenosis (NEJM 2006)
El estudio fue interrumpido después de randomizar 527 pacientes luego que
se constató un exceso de complicaciones del 5,7% en el grupo Angioplastia

CREST TRIAL

CREST TRIAL

CREST TRIAL

https://www.slideshare.net/DrSatyamRajvanshi/management-of-carotid-artery-stenosis-evidence-and-guidelines

ACT 1 Trial
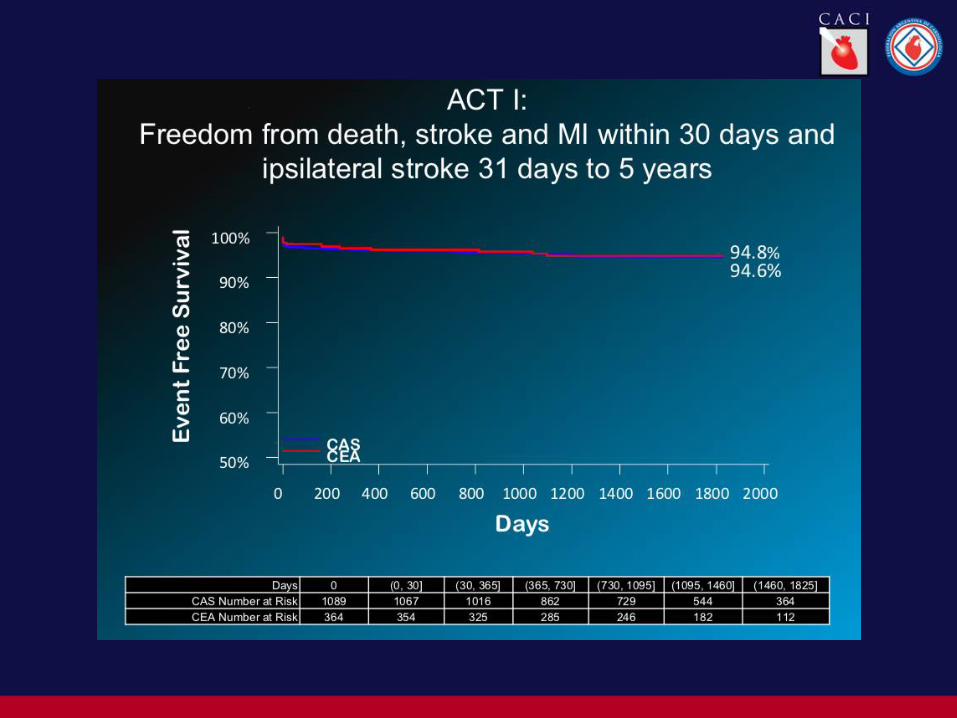


Estudios controlados por FDA
• Para aprobación o vigilancia post aprobación
• Pacientes de alto riesgo
• Uso de EPD en todos los pacientes
• Cerca de 6000 pacientes

Estudios controlados por FDA

• Evaluación Clínica FRCV y comorbilidades:
- edad
- sexo,
- HTA, DLP, DBTTBQ activo
- Cardiopatía isquémica, EPOC, ICC, IRC
Cómo disminuir la incidencia de stroke preiprocedimiento???

Cómo disminuir la incidencia de stroke preiprocedimiento???
Evaluación neurológica independiente (Stroke Team): - Diferencia entre sintomático o asintomático - Identificar situaciones de resolución urgente )ACV in cerescendo o stroke en curso.
- En caso de stroke reciente, diferenciación entre stroke menor y mayor - Interpretación de la TC o RM de cráneo para detectar infartos silentes.

SELECCIÓN DE PACIENTES
Detección de los pacientes con
alto riesgo para Angioplastia
Carotidea

EVALUACION DEL RIESGO
• BAJO RIESGO
- Joven
- Asintomático
- Lesión focal
- Acceso recto
• ALTO RIESGO
- Añoso
- Sintomático
- Lesiones largas
- Acceso tortuoso

CAPTURE 2500
Predictors of Peri-Procedural Outcomes

CAPTURE 2500
Predictors of Peri-Procedural Outcomes

SELECCIÓN DE PACIENTES Evaluación no Invasiva
Ultrasonido
• Cuantificación de la estenosis
• Velocidad de progresión
• Características de la lesión
Las placas ecoluscentes tienen un mayor riesgo embolígeno!!
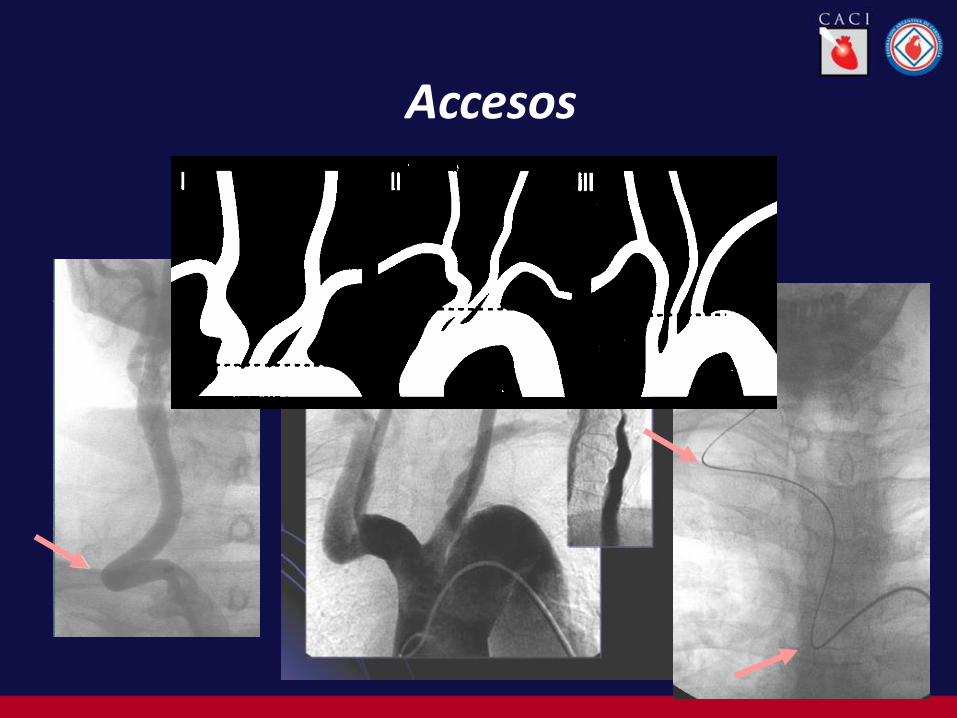
Accesos

Acodaduras y tortuosidades
Glide Wires
Amplatz Wires
90 cm.Shuttle Sheath
5F/125cm Vitek Catheter
Berenstein Catheter
Guiding Catheters
MP
Amplatz
Hockey Stick
Stiff Buddy wire

Ateromatosis y calcificaciones difusas del arco aórtico de la ACC


ACCESO RADIAL

ACCESO DIRECTO EN CAROTIDA COMUN

SELECCIÓN DE MATERIALES

ELECCION STENTS MECHANICAL ASPECTS
• Self expandable
• Low Profile
• Radial Force
• Tracability
• Mesh Size (closed/open cell)
• Foreshortening
• Flexibility
• Adaptability
• Scafoilding and wall coverage
• Tappering
• Nitinol/Steel

Belgian Italian Carotid (BIC) study

Belgian Italian Carotid (BIC) study
2/3 los ACV se producen luego del procedimiento
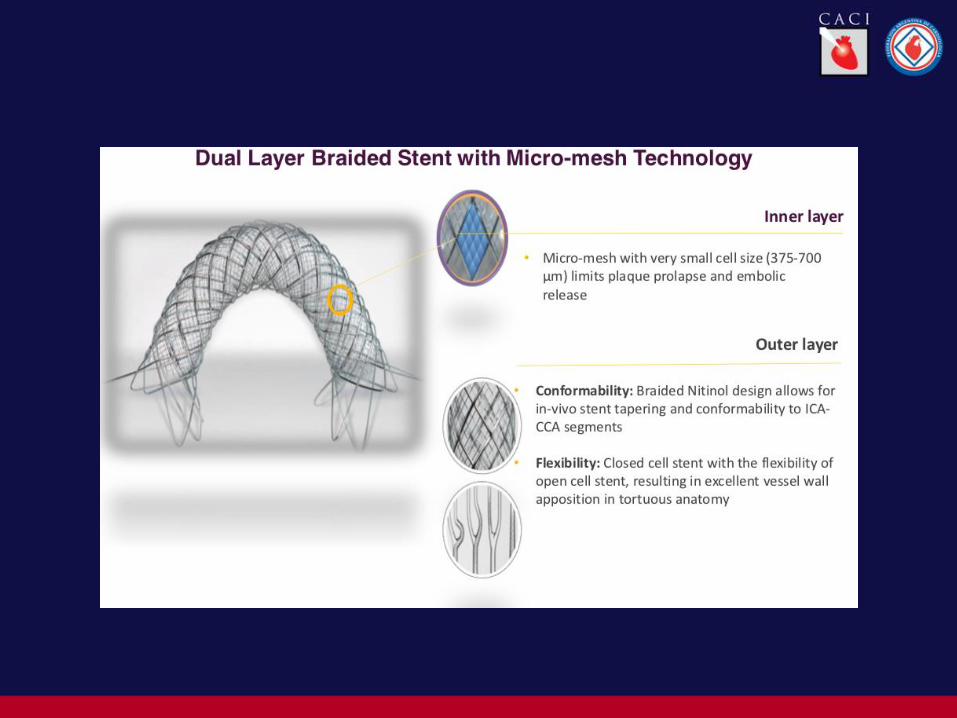



TRIAL CON STENTS MALLADOS

DISTAL OCCLUSION
PercuSurge (Medtronic)
Pros
•Low Profile
•Flexible
Cons
•Less Tolerance in Time
•Contraindicated in isolated Hemisphere
•Without Protection while crossing
PROTECCION CEREBRAL

PROXIMAL OCCLUSION BALLOON
Arteria (Parodi) - MO.MA (Invatec)
Pros:
•Thrombotic Lesions
•With Protection while crossing the lesion
•An alternative for distal tortuosity
Cons
•More complex, prolongs the procedural time
•Similar contrindications ofdistal systems
CEREBRAL PROTECTION

FILTERS PROS
• Cerebral flow is preserved
• Allow contrast injections
• Best Tolarated
• More Friendly
CONS
• More Rigid
• Higher Profile
• Without protection while Crossing
FIXED WIRE Angioguard (Cordis)
Filter Wire (Boston Scientific)
Accunet (Guidant)
Intercedtor (Medtronic AVE)
More rigid
Less torque
Difficult in tortuosities
NEW GENERATION NeuroShield (Mednova, Abbot)
Spider (ev3)
Allow to manipulate an independent
0.014”- wire of choice
CEREBRAL PROTECTION

Early Outcome of Carotid Angioplasty and Stenting With and Without Cerebral Protection Devices
1.80
0.89
0.33
0.56
%
<0.001
0.6
<0.05
<0.001
P value
5.52
0.71
1.10
3.74
%
18
8
3
5
Nº
With CP
140 Any stroke and death
18 Death
28 Major Stroke
94 Minor Stroke
Nº
Without CP
Stroke 2003; 34:813
A systematic review of the literature
(3433 pacientes)


Lesiones con alto riesgo de embolia periprocedimiento
• SÍNTOMAS RECIENTES
• LESION ECOLUCENTE
• TROMBO VISIBLE
• LESION MUY CERRADA
• LESIONES ULCERADAS
• LESIONES MUY LARGAS
• GRAN CARGA DE PLACA

https://www.dropbox.com/s/m1o720qmd0ddyn1/Captura%20de%20pantalla%202018-05-31%2012.21.13.png?dl=0




Efecto del tratamiento médico sobre los resultados
Published online 4 December 2017 in Wiley Online Library (www.bjs.co.uk). DOI: 10.1002/bjs.10717

ENFERMEDAD CAROTIDEA 2018 Claves
Adaptar las indicaciones al actual standard de tratamiento médico actual
Estricta selección en paciente asintomáticos
Detectar síntomas y actuar con celeridad
Evaluación minuciosa pre intervención
Stroke Team (neurólogo, neuroimagenólogo)
En caso de elegír Angioplastia, procedimiento a medida con el objeto de disminuir riesgo embolígeno

MUCHAS GRACIAS!!
Muchas gracias!!!

















