31
Dr. Hefziba Green Nephrology & Hypertension Rabin medical center

Dr. Hefziba Green Nephrology & Hypertension
Rabin medical center

A Brief History 27 years old woman. Married + 2 (twins) 2008- Diagnosis of Ulcerative colitis during
pregnancy. Constant elevation of cholestatic liver enzymes.
2/2010 –MRCP – features compatible with PSC
The disease is steroid dependent, multiple flares. Suggested treatments: Remicade, collectomy

Present 12/5/12 – admission after 2 weeks of fatigue, malaise,
nausea, anorexia, arthralgia (ankles) and pre-syncope Diarrhea without change from baseline, 4-5 times a day,
with no blood or mucus. No fever, BP 138/89, SaO2 normal The day before her admission - IV Venofer for the first time
to treat known iron deficiency anemia Current medication:
T. ASACOL 4 G/D T. PURINETHOL(6MP) 75 MG/D T. PREDNISONE 5 MG/D

Lab results (Jan-May 2012) 2/5/12 27/3/12 31/1/12
7300 7000 6400 WBC
10.4 9.8 10.6 Hb
106 110 109 MCV
461,000 391,000 612,000 Plt
12.3 9.2 MPV
17% 17.6% RDW
26% 23% Transferin sat.
13 10 42 Ferritin (ng/ml)
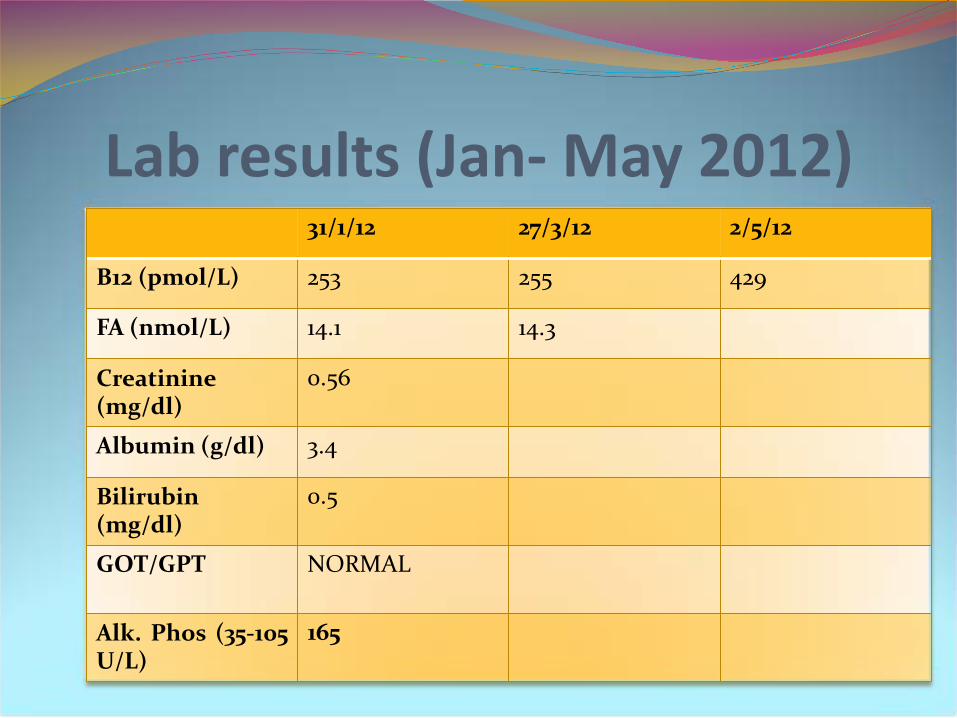
Lab results (Jan- May 2012) 2/5/12 27/3/12 31/1/12
429 255 253 B12 (pmol/L)
14.3 14.1 FA (nmol/L)
0.56 Creatinine (mg/dl)
3.4 Albumin (g/dl)
0.5 Bilirubin (mg/dl)
NORMAL GOT/GPT
165 Alk. Phos (35-105 U/L)
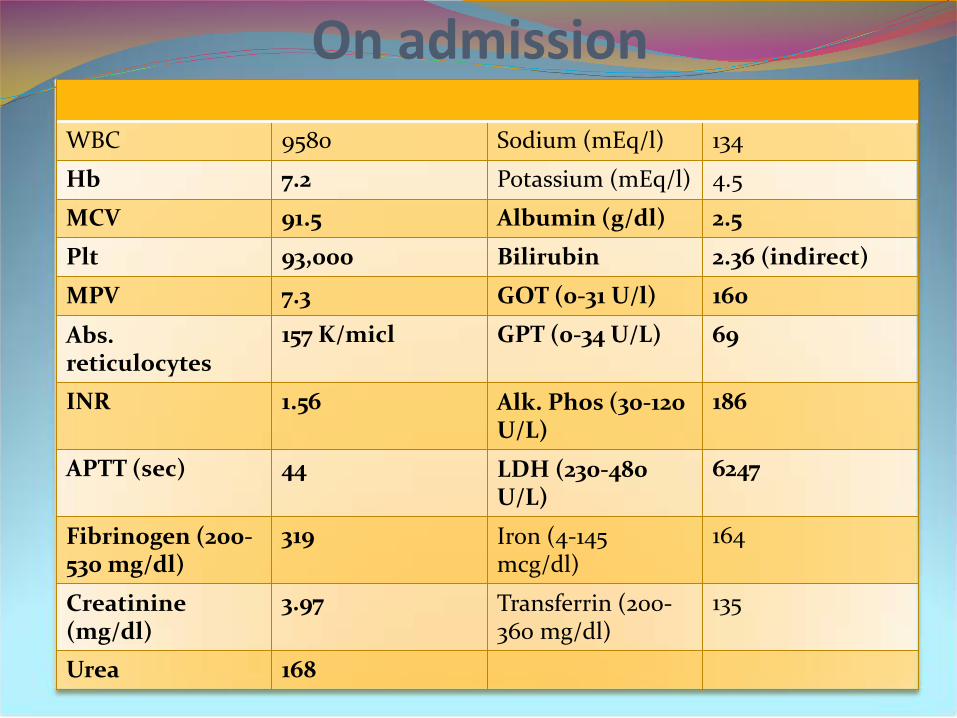
On admission 134 Sodium (mEq/l) 9580 WBC
4.5 Potassium (mEq/l) 7.2 Hb
2.5 Albumin (g/dl) 91.5 MCV
2.36 (indirect) Bilirubin 93,000 Plt
160 GOT (0-31 U/l) 7.3 MPV
69 GPT (0-34 U/L) 157 K/micl Abs. reticulocytes
186 Alk. Phos (30-120 U/L)
1.56 INR
6247 LDH (230-480 U/L)
44 APTT (sec)
164 Iron (4-145 mcg/dl)
319 Fibrinogen (200-530 mg/dl)
135 Transferrin (200-360 mg/dl)
3.97 Creatinine (mg/dl)
168 Urea

Urinalysis : protein 500 mg/dl, erythrocyte casts, few granulr casts
Blood smear: extremely pathologic red cells with target cells, schistocytes, polychromasia, Howell-Jolly bodies
Negative direct Coombs test
Microangiopathic Hemolytic Anemia m/p TTP/HUS
Plasma exchange + IV Hydrocortisone

The first few days Daily plasma exchange
15/5/12 14/5/12 13/5/12 12/5/12
160/100 129/90 122/87 138/89 BP
7.7 8.5 8.1 7.2 Hb
35,000 33,000 42,000 93,000 Plt
3.52 3.77 3.74 3.97 Creatinine (mg/dl)
4173 3732 3376 6247 LDH (U/L)


Some answers Haptoglobin below detection level Negative bHCG Viral serology:
HBsAg - Neg HBsAb>1000 ,HCV – Neg ,HIV -Neg CMV IgG – Pos CMV IgM – Neg EBV-EBNA - Pos
Clotting factors (during PE) Factors V, VII, VIII, IX, X- all within normal values
FACS for the detection of PNH clone CD59-100% ,Monocytes + Granulocytes FLAER -100% ,
Granulocytes CD24-100%
15/5/12 – ADMATS 13 - normal




So, HUS than… 6MP was discontinued in the 2nd admission day
Admission day 4- positive stool test for Clostridium dif. Ag, negative for CD toxin. Started on Flagyl.
Stool cultures - negative
15/5/12 – Mensevax
16-17/5/12 – more results are coming:
ANA- titer 1:80 APLA – Neg Anti MPO – Neg Anti PR3 – Neg RF - Normal SCL-70 - Neg SSA/ SSB – Neg RNP –Neg
C3 – 82.8 mg/dl (90-180) C4 – 7.3 mg/dl (10-40)
Admission day 10 After 9 sessions of PE and high-dose steroids
Clincal evaluation: No change in diarrhea frequency. PCR-CD from blood is
negative- flagyl discontinued after 5 days. She’s hypertensive, diastolic BP>100, anasarca– started
on diuretics and later on calcium channel blockers
Lab results: No change is Hb, Plt., LDH, Creatinine 20/5/12- in 24 hours urine collection proteinuria of 14.5
g/d, same results 2 days later

Biopsy 22/5/12

23-27/5/12- ICU. PC infusion, PE resumed after 48 hours 27/5/12 – Back in internal medicine department
After 12 sessions of PE
22/5/12 for the 1st time LDH<2000 and did not rise between sessions
30/5/12 platelets up to 120,000 without infusions
Creatinine level began to decline, but “got stuck” on 2.6 mg/dl
30/5/12 started on Rafapen


IV ECULIZUMAB
31/5/12


Eculizumab Half life of approximately 11 days following IV
administration. Distributed in the vascular space The inhibition of complement activation at the
level of C5 creates a functional C5 deificiency Blockade of the complement cascade at the C5
level does preserve the early components of complement that are essential for the opsonization of microorganisms and the clearance of immune complexes
Increased risk for Neisseria meningitides
Dramatic response First goes the platelets
146,000 at 31/5 * 160,000 at 1/6 * 309,00 at 4/6
Next come the kidneys
2.42 mg/dl at 4/6 * 2.17 mg/dl at 7/6 * 1.67 mg/dl at 9/6 * 1.56 mg/dl at 12/6
The hemoglobin takes its time getting to 10 mg% only after 3 weeks
LDH is last
1600 at 7/6 * 1112 at 17/6
5/6/12 discharged home

And since then… C3, C4 – normalized and stays within normal range
since 10/6/12 Hb around 12.0, Plt and LDH within normal range,
haptogobin high-normal Creatinine level declined gradually for the next few
weeks, currently around 1.05 mg/dl. No proteinuria BP improving, however still receiving calcium
channels blockers, beta blockers, ACE inhibitors
Slow tapering of steroids, no UC flares up

Anti CFH Ab 2000 AU/ ml

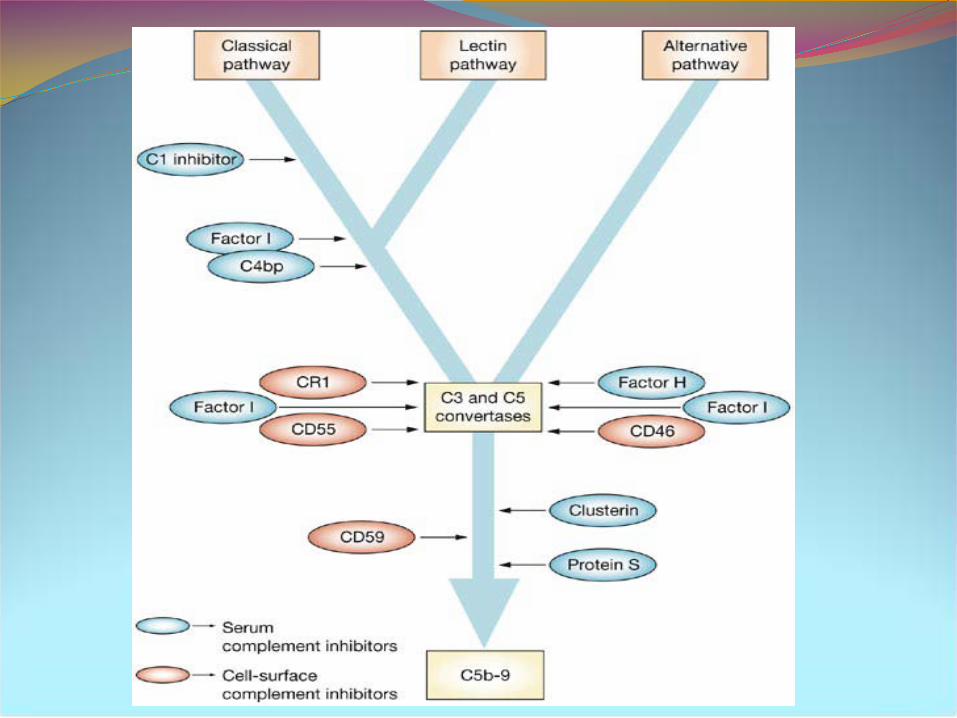
Monitoring complement blockade CH50 assays A useful tool for detecting a deficiency of the
classical pathway by assessing the ability of serum to lyse sheep erythrocytes
All nine components of the classical pathway (C1-C9) are required in order to reach a normal CH50 level
A blockade of C5-9 complex by eculizumab would result in low levels of CH50





















